Embed Size (px)
Citation preview

14/10/2013
1
Blood Reflux:
Has your line been slimed?
Accreditation/Disclosure
Accreditation - Provider approved by the California Board of Registered
Nursing, provider number CEP 15005, for 1 contact hour.
Non-endorsement of products - Approval as a provider refers only to this
continuing education activity and does not imply California Board of
Registered Nursing endorsement of any commercial products.
Commercial Support for this activity is provided by Smiths Medical ASD,
Inc.
Conflicts of Interest - Presenter is a full time employee or paid consultant
for Smiths Medical ASD, Inc.
Off-label use of a product for a purpose other than that for which it was
approved by the Food and Drug Administration will not be presented in
this learning activity.
Requirements for Successful
Completion
To earn contact hours for this activity:
� Attend the entire program no partial credit will be awarded
� Complete all required forms
� Return all forms to the program facilitator
� Certificate of Attendance will be provided upon receipt of completed forms
Documentation
� Secured confidential records for this learning activity will be maintained for six (6) years

14/10/2013
2
Objectives
� Describe how blood reflux in vascular access catheters contributes to thrombotic catheter occlusions and bloodstream infections.
� List two quality initiatives to prevent blood reflux complications.
� Identify two strategies for preventing complications created by blood reflux in the vascular access catheter.
Reflux & Bloodstream Infections
“Theoretically, blood reflux into either the IV
catheter or needleless connector increases both the
risk of occlusion and biofilm formation. Both also
increase the risk of Health Care Associated Blood
Stream Infections”.
Infection Control Today August 2010 Vol. 14 No 8, “Choosing the Best Design for Intravenous
Needleless Connector to Prevent HA-BSI” By: William R. Jarvis, MD
Blood Reflux
Uncontrolled backflow of
blood into the catheter
lumen

14/10/2013
3
Blood Reflux
Because the catheter tip is
inside the body and not
visible, we are not always
aware when reflux occurs
Backflow and Biofilm
■ Blood attaches to catheter lumen and begins
coagulation process
■ Blood reflux may cause catheter-associated
venous occlusion and thrombosis
VA
SCU
LAR
PR
ESSU
RE
& IN
FUSIO
N

14/10/2013
4
Dynamics of Vascular Pressure
■ All blood vessels have blood
forced through them by
contraction of the heart muscle
■ This forward flow is often called
vascular pressure and is
measured in units of force such
as mmHg and PSI
Dynamics of Vascular Pressure
■ If vascular pressure becomes higher than infusion
pressure, increased pressure pushes blood into
catheter tip
■ The blood remains in catheter lumen until vascular
pressure drops below pressure of the infusing fluid
Dynamics of Vascular Pressure
Pressure
mm Hg
Example
(rounded pressure values)
Pressure
psi
2 - 20mm Hg Central Venous pressure range 0 - 0.4 psi
10 - 30mm Hg Peripheral Venous pressure range0.2 - 0.6 psi
80-100mm Hg Extravasation risk > 2 psi
75mm HgGravity pressure of fluid 100cm
(39 inches) above cannulation site1.5 psi
36” height above the heart = 1.33 psi overcomes the patients vascular pressure with gravity infusion

14/10/2013
5
TH
RO
MB
OSIS
Type of Thrombotic Occlusions:
• Fibrin sheath thrombus
• Fibrin tail
• Mural thrombus
• Intraluminal thrombus
Hypercoagulability of blood
Vessel Wall Damage
Hemodynamic changes in blood flow
Virchow’s Triad

14/10/2013
6
Blood Coagulation
Acquired
■ Pregnancy
■ Diabetes
■ Trauma or Surgery
■ Cancer
■ Obesity
■ Prolonged immobility
■ Nephrotic Syndrome
■ Dehydration
Genetic
■ Genetic clotting factor
disorders
■ Hemoglobin
deficiencies
Vessel Wall Damage
■ Injuries or trauma
■ Hypertension, chronic inflammation
■ Catheter placement and size
■ Catheter composition
Hemodynamics: Influencing
Factors
■ Syringe connection/ disconnection
■ Syringe plunger rebound
■ IV bag run dry
■ Low infusion rates
■ External pressure from ventilators and other hospital equipment
■ Patient Movement
■ Coughing
■ Crying
■ Sneezing
■ Respiration
■ Vomiting
Mechanical Physiological

14/10/2013
7
TH
RO
MB
OSIS A
ND
INFE
CT
ION
Relationship between
Thrombosis and Infection
“Shortly after insertion, intravascular catheters are
coated with a conditioning film, consisting of fibrin,
plasma proteins, and cellular elements, such as
platelets and red blood cells. Microbes interact with
the conditioning film, resulting in colonization of
the catheter. There is a close association between
thrombosis of central venous catheters and
infection.”
CDC Guidelines for the Prevention of Intravascular Catheter-Related Infection, 2011
What is Biofilm?
■ Bacteria ■ Yeast ■ Algae ■ Fungi
Dynamic ecosystem of microorganisms embedded in a matrix of extracellular polymeric substances (Slimy Matrix)
– Biofilm Bacteria Are 1000X more resistant to antibiotics than free-floating bacteria
– Share and transfer resistance to other organisms
14/10/2013
8
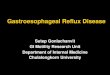
The Five Stages of Biofilm Formation
1. Initial reversible attachment of free swimming micro-organisms to surface
2. Permanent chemical attachment, single layer, bugs begin making slime
3. Early vertical development
4. Multiple towers with channels between, maturing biofilm
5. Mature biofilm with seeding / dispersal of more free swimming micro-organisms
Graphic by Peg Dirckx and David Davies © 2003 Center for Biofilm Engineering Montana State University.
Relationship Between
Thrombosis and Sepsis
“The presence of CRS or significant catheter
colonization was more frequent in patients whose
catheter-related central vein thrombosis was
diagnosed.”
Chest 1998; 114;207-213
Central Vein Catheter-Related Thrombosis in Intensive Care Patients: Incidence, Risk Factors,
and Relationship with Catheter-Related Sepsis.
By: Jean-Francois Timset, MD, PhD
IMP
LICA
TIO
NS
14/10/2013
9
Implications of Occlusion
■ Patient discomfort
■ High risk of DVT
■ Increased risk of embolism
■ Delay in treatment
■ Increased length of stay
■ Nursing time
■ Increase in medication and supply cost
■ Increased risk of infection
Impact of CLABSI
• In the United States, 15 million central vascular
catheter (CVC) days occur in intensive care units
(ICUs) each year
• Outcomes associated with hospital-acquired
CLABSI
• Mortality rate of 12%-25%
• Increased length of hospital stay 6-10 days
• Excess Healthcare cost of $16,550
Morbidity and Mortality Weekly Report, Vital Signs: Central Line–Associated Blood Stream Infections —
United States, March 1, 2011, Vol. 60
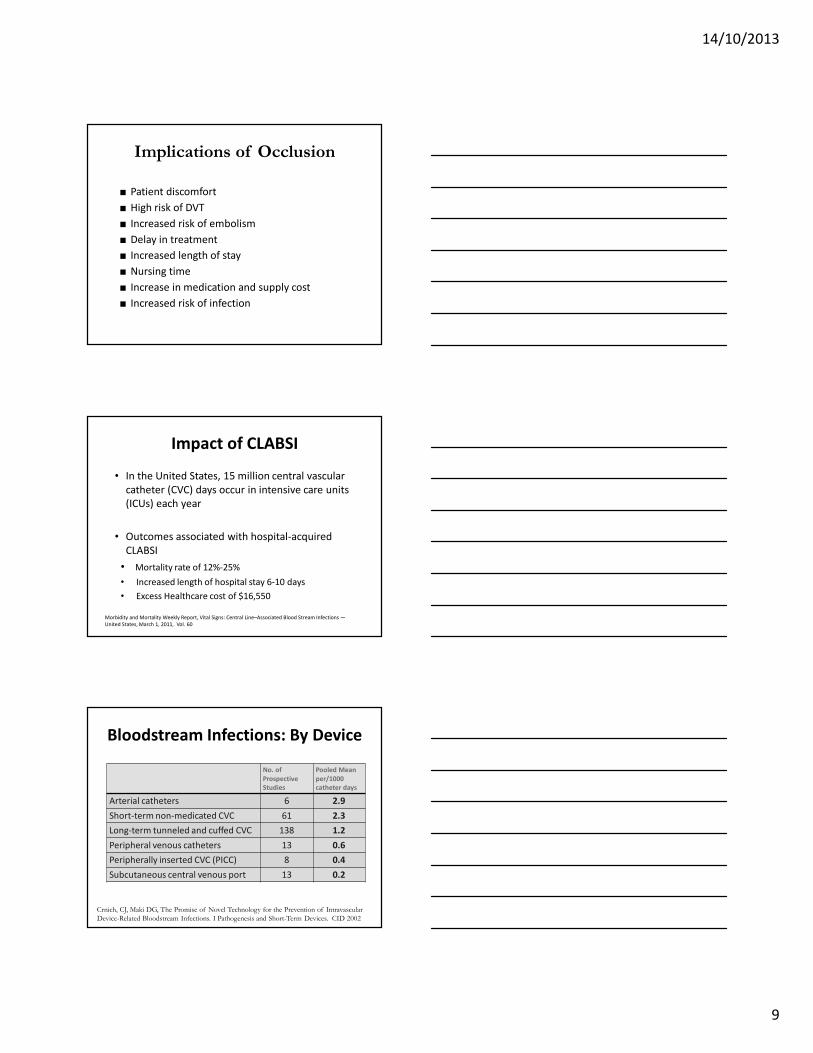
Bloodstream Infections: By Device
No. of
Prospective
Studies
Pooled Mean
per/1000
catheter days
Arterial catheters 6 2.9
Short-term non-medicated CVC 61 2.3
Long-term tunneled and cuffed CVC 138 1.2
Peripheral venous catheters 13 0.6
Peripherally inserted CVC (PICC) 8 0.4
Subcutaneous central venous port 13 0.2
Crnich, CJ, Maki DG, The Promise of Novel Technology for the Prevention of Intravascular Device-Related Bloodstream Infections. I Pathogenesis and Short-Term Devices. CID 2002

14/10/2013
10
PU
SH
FO
R
IMP
RO
VE
ME
NT
CMS Guideline Changes and Impact
on Hospitals:
2005 Deficit Reduction Act’s Hospital-Acquired Conditions (HACs) and Present On Admission (POA) Program
CMS Never Event and Public
Reporting
Central Line Associated Bloodstream
Infections
2011 CMSRequirements
Association for Professionals in Infection Control and Epidemiology, Inc. 3/31/10.

14/10/2013
11
Standards of Evidenced-Based
and Best Practice
■ Infusion Nurses Society – INS
■ Association for Vascular Access – AVA
■ Centers for Disease Control and Prevention - CDC
■ Society for Healthcare Epidemiologist of America - SHEA
■ Manufacture’s Recommendations
Guidelines for Peripheral and
CVCs
Needleless Connectors Add-On/ Administration
Sets
Site and Dressing Changes
CDC
2011
Split septum valve
preferred over
mechanical valve
No more frequently
than 96-hours intervals,
but at least every 7 days
Peripheral catheters :
72-96 hours
SHEA
2008
(CVCs only)
Do not routinely use
positive pressure
needleless connectors
No longer than 96
hours
Non-tunneled CVCs,
change transparent
dressings every 5-7 days
INS
2011
Needleless connectors
shall be Luer-lock
design
Change with site
rotation: up to 96
hours dependent on infusate
When clinically indicated
Peripheral Device Selection
Appropriate catheter should accommodate
patient’s vascular access based on:
■ Prescribed therapy and duration of treatment
■ Vascular integrity and comorbidities
■ Use of smallest gauge size and length
■ Ability and resources to care for the device

14/10/2013
12
Peripheral Site Selection
■ Preferred sites are those found on dorsal
and ventral surfaces of upper extremities
■ Avoid –
� Areas of flexion, bifurcation and valves
� Lateral/ventral surface of the wrist due to
potential nerve damage
� Extremities with lymphedema
� Previously used sites
Central Catheter Placement
Right-sided placement is preferred:
� Results in shorter catheter length
� Catheter lies parallel in the right internal jugular vein resulting in less damage to the intima
� Ideal tip location - lower 1/3 of the superior vena cava
Stabilization
Reduce Mechanical Phlebitis
• Preserve integrity of access device
• Minimize catheter movement at
insertion site
• Prevent catheter dislodgement
14/10/2013
13
Needleless Technology
Negative displacement: Upon syringe
disconnection, blood refluxes into catheter tipAction: clamp BEFORE syringe disconnection
Positive displacement: Upon syringe disconnection,
small amount of fluid pushes out end of catheter
tipAction: clamp AFTER syringe disconnection
Neutral displacement: Designed to minimize blood
reflux into catheter tip upon syringe disconnection Action: clamp BEFORE syringe disconnection
Clamping sequence and fluid displacement
Clamping does NOT
stop all blood reflux potentials
Positive Needleless Connectors
• SHEA – Do not routinely use positive-pressure needleless connectors with mechanical valves
• FDA Alert – Initiated post market surveillance and supports SHEA’s recommendations
• CDC – Split septum valve may be preferred over some mechanical valves
Risk Benefits Education

14/10/2013
14
EX
AM
INE
YO
UR
PR
AC
TIC
E
Are you doing what it takes
to decrease the occurrence of
blood reflux?
Clinical Practice: Policy and
Protocol
Policy must reflect facility specific flush protocol:
■ Proper flush-clamp sequence according to connector being used
■ Proper flush solution, technique, frequency of flush, and volume of flush
■ Treat partial and complete occlusion in central catheters PROMPTLY
Clinical Practice: Needleless
Connectors
• Negative Fluid Replacement Needleless
Connector
Flush Clamp Remove Syringe
• Positive Fluid Replacement Needleless
Connector
Flush Remove Syringe Clamp

14/10/2013
15
Clinical Practice: Data
■ Number of PIV catheters placed■ Number of PIV catheter days■ Mean, Median and Average dwell time
■ Complications:� Phlebitis� Infiltration and Extravasation
� Infection� Air Embolism� Catheter Embolism
� Thrombosis and Occlusion
Education and TrainingOut with the Old in with the New
See One
Do One
Teach One
Hospital Protocols/Policies and
Infection Prevention
■ Hand hygiene and aseptic technique
■ Site care and maintenance
■ Catheter site dressing regimens
■ Assessment for complications
■ Access connector decontamination
■ IV administration set and add-on device
■ Vascular access devices removed when no longer required

14/10/2013
16
SUM
MIN
G IT
UP
Strategies to Prevent Blood
Reflux
� Standards of Best Practice
� Education
� Data – Continuous Quality Improvement
� Technology
Objectives
• Describe how blood reflux in vascular access catheters contributes to thrombotic catheter occlusions and bloodstream infections.
• List two quality initiatives to prevent blood reflux complications.
• Identify two strategies for preventing complications created by blood reflux in the vascular access catheter.

14/10/2013
17
Questions?
Thank you for your attention.
Please complete:
–Evaluation Form
–Sign-in Sheet
–Registration Form