Embed Size (px)
Citation preview

BLOOD TRANSFUSIONBLOOD TRANSFUSION
Suprhamanyam EvaliSuprhamanyam Evali

QUIZQUIZ What is your blood What is your blood
group? group? How How common is it in this common is it in this room?room? is it the same is it the same as the world population?as the world population?
RECESSIVE but most common??
ANSWER: it is the ancestral form. The A and B mutations appeared in the last 20,000 years and haven't spread through the population yet.

TOPICSTOPICS
Blood ComponentsBlood Components Pre-transfusion TestingPre-transfusion Testing Transfusion ReactionsTransfusion Reactions

1665 — 11665 — 1stst Documented DocumentedAnimal-to-Animal Transfusion Animal-to-Animal Transfusion
Dog-to-dog Dog-to-dog transfusion transfusion by Richard by Richard Lower.Lower.
From Petz and Swisher’s Clinical Practice of Transfusion Medicine, 2nd ed., 1989.

1667—11667—1stst Documented DocumentedAnimal-to-Human TransfusionAnimal-to-Human Transfusion
Jean Baptiste Jean Baptiste Denis infuses Denis infuses 15-year-old 15-year-old boy with boy with lamb’s blood.lamb’s blood.
From Zmijewski’s Immunohematology.

1818—11818—1stst Documented DocumentedHuman-to-Human TransfusionHuman-to-Human Transfusion
Following a 150-year Following a 150-year transfusion hiatus, transfusion hiatus, James Blundell James Blundell transfuses patient with transfuses patient with blood from a human blood from a human donor. donor.
From Petz and Swisher’s Clinical Practice of Transfusion Medicine, 2nd ed., 1989.

1800’s—All Manner of Blood 1800’s—All Manner of Blood Collection Devices UtilizedCollection Devices Utilized
(You think present-(You think present-day donor centers day donor centers sometimes face sometimes face challenges in challenges in recruiting repeat recruiting repeat blood donors?)blood donors?)
From Petz and Swisher’s Clinical Practice of Transfusion Medicine, 2nd ed., 1989.

1900—1900—ABH Blood Group System ID’dABH Blood Group System ID’d
Karl Landsteiner Karl Landsteiner discovers ABH system discovers ABH system when he types when he types individuals as (what we individuals as (what we now call) group A, group now call) group A, group B, and group O. In 1902, B, and group O. In 1902, his proteges identify a his proteges identify a group AB individual for group AB individual for the first time.the first time.
From Transfusion, Vol. 1, p. 2 (1961)

The Discovery of Many OtherThe Discovery of Many OtherRed Cell Antigens FollowedRed Cell Antigens Followed
Rh (C, c, D, E, e, …)Rh (C, c, D, E, e, …) Kell (K, k, …)Kell (K, k, …) Kidd (JkKidd (Jkaa, Jk, Jkbb, …), …) Duffy (FyDuffy (Fyaa, Fy, Fybb, …), …) MNSs, … MNSs, … Lewis (LeLewis (Leaa, Le, Lebb)) … … … … … …

How We Make Blood ComponentsHow We Make Blood ComponentsCollection ProcessCollection Process(1) (1) Via Whole Blood DonationVia Whole Blood Donation: : Whole blood is collected from Whole blood is collected from healthy blood donors into sterile healthy blood donors into sterile blood bags that contain blood bags that contain anticoagulant-preservative.anticoagulant-preservative.
(2) (2) Via ApheresisVia Apheresis: Machines with : Machines with internal centrifuges separate a donor’s internal centrifuges separate a donor’s blood into individual components (e.g., blood into individual components (e.g., platelets, plasma, RBCs, etc.). The platelets, plasma, RBCs, etc.). The desired components are retained, desired components are retained, while the remainder is returned to the while the remainder is returned to the donor.donor.
TAKE ALL
TAKE WHAT YOU WANT

Blood productsBlood products
Whole bloodWhole blood CellularCellular
PRBCsPRBCs PlateletsPlatelets
PlasmaPlasma FFPFFP CryoprecipitateCryoprecipitate Other proteinsOther proteins

Blood Component Preparation“A little goes a long way”
Slow centrifuge
Fast centrifuge
450ml
180-200ml
50-70ml
10-15ml
200-250ml
You may donate every 56 days
The plasma from your donation is replaced within about 24 hours. Red cells need about four to six weeks for complete replacement. That’s why at least eight weeks are required between whole blood donations

Blood component Blood component

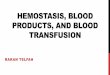
Whole Blood Separation
Typical values of the density of blood plasma and blood cells are 1025 kg/m^3 and 1125 kg/m^3, respectively."

Differential CentrifugationDifferential CentrifugationFirst CentrifugationFirst Centrifugation
Whole Blood Main Bag
Satellite Bag 1
Satellite Bag 2
RBC’sPlatelet-rich Plasma
First
Closed System

Differential CentrifugationDifferential CentrifugationSecond CentrifugationSecond Centrifugation
Platelet-rich Plasma
RBC’s PlateletConcentrate
RBC’s
Plasma
Second


Collection of Blood ProductsCollection of Blood Products
Apheresis Apheresis (TAKE WHAT U WANT-RETURN WHAT U DON’T)(TAKE WHAT U WANT-RETURN WHAT U DON’T)
Plateletpheresis- may donate up to 24x/yearPlateletpheresis- may donate up to 24x/year Leukapheresis-granulocytes donor given Leukapheresis-granulocytes donor given
dexamethasone? G-CSF?dexamethasone? G-CSF? ErythrocytapheresisErythrocytapheresis may donate every 16 weeks may donate every 16 weeks PlasmapheresisPlasmapheresis Stem Cell collectionStem Cell collection


Blood productsBlood products
Cellular ComponentsCellular Components:: RRed blood cellsed blood cells
- - LeukocyteLeukocyte--reduced reduced RBCsRBCs p purifiedurified
- W- Washed ashed RBCsRBCs plasmal plasmaless RBCess RBC
- Irradiated RBCs- Irradiated RBCs smash the DNA of WBC to smash the DNA of WBC to prevent GVHDprevent GVHD
PlateletsPlatelets - - Whole blood derivedWhole blood derived platelets platelets
- S- Single-donor platelets ingle-donor platelets (Apheresis Platelets)(Apheresis Platelets) GGranulocyteranulocytess

Blood productsBlood products
Acellular ComponentsAcellular Components::
FFresh-frozen plasma (FFP)resh-frozen plasma (FFP), Thawed plasma, Thawed plasma CryoprecipitateCryoprecipitate FFactor concentrates (VIII, IX)actor concentrates (VIII, IX) AlbuminAlbumin

Blood Component Manufacture from Whole Blood Component Manufacture from Whole BloodBlood
RBCsRBCs
Platelet-Rich Platelet-Rich PlasmaPlasma
+
or
Centrifuge
(higher g forces)
Freeze
Fresh Frozen Plasma (FFP)or
“Plasma Frozen with 24 hours”
Plasma
Platelets
+
• Leukoreduce• Possibly irradiate• Other

Blood Component Manufacture from Blood Component Manufacture from Whole BloodWhole Blood
FreshFrozenPlasma(FFP)
Cryo-Reduced Plasma
Cryoprecipitate
+•Thaw (4° C)
•Centrifuge

Using the “Leftovers” WiselyUsing the “Leftovers” Wisely
Plasma DerivativesPlasma Derivatives AlbuminAlbumin Factor VIIIFactor VIII Immune globulinImmune globulin etc. etc.
Sent for
further processing
Plasma
Plasma
(of any kind)
(of any kind)

Over 400 red cell antigens describedOver 400 red cell antigens described Each antigen is defined by a specific Each antigen is defined by a specific
antibody antibody Antigens are divided into blood group Antigens are divided into blood group
systems > 25 systemssystems > 25 systems
The most important blood group The most important blood group system system ABO!ABO!

IncompatibilitiesIncompatibilities
ABOABO RhRh Lewis (oligosaccharide)Lewis (oligosaccharide) KellKell DuffyDuffy KiddKidd MNSsUMNSsU I/I (carbohydrate)I/I (carbohydrate)



ABO System
The ABO system is defined by the presence of A, B., H (0) antigens (sugars) on surface of red cells
Determined by allelic genes A, B, O, and Hh
Genes code for specific glycosyltransferases that add sugars to oligosaccharide chains
H substance is the precursor on which A and B antigens are built
O gene is a silent allele which does not encode a functional enzyme - the structure of H substance is not altered

Precursor Substance
H antigen
A antigen B antigen
(Hh gene)(Se gene)
(B gene)(A gene)

ABO Antigen System

H antigen only = Blood group O



COMPATIBLECOMPATIBLE
Patient'sPatient'sABO ABO GroupGroup
AntigenAntigenon Red on Red CellsCells
Antibody Antibody in in SerumSerum
WholeWholeBloodBlood
Red Blood Red Blood CellsCells PlasmaPlasma
OO No A or BNo A or B Anti-A Anti-A Anti-BAnti-B OO OO
OOAABBABAB
AA AA Anti-BAnti-B AAAAOO
AAABAB
BB BB Anti-AAnti-A BBBBOO
BBABAB
ABAB A and BA and B NoneNone ABAB
ABABAABBOO
ABAB

RBC CompatibilityRBC Compatibility

Plasma CompatibilityPlasma Compatibility

The Rh or Rhesus blood system is the second most important The Rh or Rhesus blood system is the second most important system. system.
The major antigen in this system is The major antigen in this system is DD
Rh positive ( D+) 85%Rh positive ( D+) 85% Rh negative ( D-) 15%Rh negative ( D-) 15%
DD Ag is highly immunogenic Ag is highly immunogenic
Antibodies are "unexpected" and are immune - they result Antibodies are "unexpected" and are immune - they result from previous transfusion or pregnancy from previous transfusion or pregnancy
The Rhesus System

Rh factor blood grouping systemRh factor blood grouping system
Many people also have a so called Rh factor Many people also have a so called Rh factor on the red blood cell's surface. on the red blood cell's surface.
This is also an antigen and those who have it This is also an antigen and those who have it are called Rh+. are called Rh+.
Those who haven't are called Rh-.Those who haven't are called Rh-. A person with Rh- blood does not have Rh A person with Rh- blood does not have Rh
antibodies naturally in the blood plasma (as antibodies naturally in the blood plasma (as one can have A or B antibodies, for instance). one can have A or B antibodies, for instance).

Cont.Cont.
But a person with Rh- blood can But a person with Rh- blood can developdevelop Rh antibodies in the Rh antibodies in the blood plasma if he or she receives blood from a person with blood plasma if he or she receives blood from a person with Rh+ blood, whose Rh antigens can trigger the production of Rh+ blood, whose Rh antigens can trigger the production of Rh antibodies. Rh antibodies.
A person with Rh+ blood can receive blood from a person A person with Rh+ blood can receive blood from a person
with Rh- blood without any problems.with Rh- blood without any problems.


Rh COMPATIBILITY Rh COMPATIBILITY
Rh Positive PatientRh Positive Patient Rh Negative Patient Rh Negative Patient
Rh positive or Rh positive or Rh negative Components Rh negative Components Only Rh negative ComponentsOnly Rh negative Components

WHAT IS AN ANTIGLOBULIN TEST ?
The antiglobulin test is either "direct" or "indirect". The "direct antiglobulin test“or DAT is often called the “__________".

DIRECT ANTIGLOBULIN TEST
In a “direct” antiglobulin test (DAT), red cells are taken from the patient, extensively washed and then "directly" tested with anti IgG or anti complement. Agglutination indicates a positive test.
A DAT evaluates whether a patient’s red cells are coated in vivo with IgG or complement.

.. Direct Antiglobulin Test

USE OF THE DAT:USE OF THE DAT: Diagnosis of:Diagnosis of:
Haemolytic Disease of the Newborn (HDN)Haemolytic Disease of the Newborn (HDN)
Autoimmune Haemolytic Anaemia (AIHA)Autoimmune Haemolytic Anaemia (AIHA)
Drug related HaemolysisDrug related Haemolysis
Haemolytic Transfusion ReactionHaemolytic Transfusion Reaction

INDIRECT ANTIGLOBULIN TEST
Detects in vitro sensitization
Plasma added to “screening” red cells
If antibodies to red cell antigens are present, the antibodies will coat the red cells
Anti IgG added and agglutination will occur

Plasma with antibodies and reagent red cells
Sensitization Anti IgG

USE OF THE IAT:USE OF THE IAT:
Detection of unexpected Detection of unexpected antibodies antibodies
Phenotyping or detection of red Phenotyping or detection of red cell antigenscell antigens
CrossmatchingCrossmatching


conclusionconclusion


HOW TO FIGURE IT OUTHOW TO FIGURE IT OUT

RECOMMENDATIONRECOMMENDATION

RH COMMENTSRH COMMENTS

COMPATIBLECOMPATIBLE
Patient'sPatient'sABO ABO GroupGroup
AntigenAntigenon Red on Red CellsCells
Antibody Antibody in in SerumSerum
WholeWholeBloodBlood
Red Blood Red Blood CellsCells PlasmaPlasma
OO No A or BNo A or B Anti-A Anti-A Anti-BAnti-B OO OO
OOAABBABAB
AA AA Anti-BAnti-B AAAAOO
AAABAB
BB BB Anti-AAnti-A BBBBOO
BBABAB
ABAB A and BA and B NoneNone ABAB
ABABAABBOO
ABAB

Pre-Transfusion TestingPre-Transfusion Testing
ABO/Rh type – 5 minutesABO/Rh type – 5 minutes Antibody screen – 25 minutesAntibody screen – 25 minutes Antibody identification – 1 hour or much moreAntibody identification – 1 hour or much more

TestingTesting
ABOABO RhRh RBC Antibody ScreenRBC Antibody Screen Infectious DiseasesInfectious Diseases
SyphilisSyphilis HBsAgHBsAg Anti-HIV-1/2Anti-HIV-1/2 Anti-HBcAnti-HBc

TestingTesting Infectious Diseases (cont.)Infectious Diseases (cont.)
Anti-HTLV-I/IIAnti-HTLV-I/II Anti-HCVAnti-HCV HIV Nucleic acid testing (NAT)HIV Nucleic acid testing (NAT) HBV NATHBV NAT HCV NATHCV NAT WNV NATWNV NAT T. cruzi T. cruzi antibody (Chagas’ Disease)antibody (Chagas’ Disease) (On some units) Anti-CMV(On some units) Anti-CMV Future ??? Parvovirus B19, malaria, etc.Future ??? Parvovirus B19, malaria, etc.

• HIV:HIV: 1 in 2,135,000 units 1 in 2,135,000 units• HBV:HBV: 1 in 205,000-to-488,000 units 1 in 205,000-to-488,000 units • HCV:HCV: 1 in 1,935,000 units 1 in 1,935,000 units• HTLV-I/II:HTLV-I/II: 1 in 514,000-2,993,000 units 1 in 514,000-2,993,000 units• CMV:CMV: << 1: 100 (when leukoreduced or CMV- << 1: 100 (when leukoreduced or CMV-
negative blood used)negative blood used)• WNV:WNV: ? (region-specific; very low) ? (region-specific; very low)• vCJD:vCJD: ? (risk very, very low—even in U.K.) ? (risk very, very low—even in U.K.)
“Infectious Risks of Blood Transfusion.” Blood Bulletin (America’s Blood Centers). December 2001.
Infectious Transfusion RisksInfectious Transfusion Risks

Time required for unitsTime required for units
Uncrossmatched Group O-neg RBCs - < 5 Uncrossmatched Group O-neg RBCs - < 5 minutesminutes
Uncrossmatched type specific RBCs – ~ 15 Uncrossmatched type specific RBCs – ~ 15 minutesminutes
Crossmatched RBCs – 30-45 minutesCrossmatched RBCs – 30-45 minutes Full ABO type, screen & crossmatch – 1 hourFull ABO type, screen & crossmatch – 1 hour Patient with multiple alloantibodies – may take Patient with multiple alloantibodies – may take
many hours!many hours! FFP – 30-45 minutes for thawingFFP – 30-45 minutes for thawing Cryo – 15 minutes for thawingCryo – 15 minutes for thawing

Whole BloodWhole Blood
StorageStorage 44° for up to 35 days° for up to 35 days
IndicationsIndications Massive Blood Loss/Trauma/Exchange TransfusionMassive Blood Loss/Trauma/Exchange Transfusion
ConsiderationsConsiderations Use filter as platelets and coagulation factors will not be Use filter as platelets and coagulation factors will not be
active after 3-5 daysactive after 3-5 days Donor and recipient must be ABO identical Donor and recipient must be ABO identical

RBC ConcentrateRBC Concentrate
StorageStorage 44° for up to 42 days, can be frozen° for up to 42 days, can be frozen
IndicationsIndications Many indications—ie anemia, hypoxia, etc.Many indications—ie anemia, hypoxia, etc.
ConsiderationsConsiderations Recipient must not have antibodies to donor RBC’s (note: Recipient must not have antibodies to donor RBC’s (note:
patients can develop antibodies over time)patients can develop antibodies over time) Usual dose 10 cc/kg (will increase Hgb by 2.5 gm/dl)Usual dose 10 cc/kg (will increase Hgb by 2.5 gm/dl) Usually transfuse over 2-4 hours (slower for chronic Usually transfuse over 2-4 hours (slower for chronic
anemiaanemia

PlateletsPlatelets
StorageStorage Up to 5 days at 20-24Up to 5 days at 20-24°°
IndicationsIndications Thrombocytopenia, Plt <15,000Thrombocytopenia, Plt <15,000 Bleeding and Plt <50,000Bleeding and Plt <50,000 Invasive procedure and Plt <50,000Invasive procedure and Plt <50,000
ConsiderationsConsiderations Contain Leukocytes and cytokinesContain Leukocytes and cytokines 1 unit/10 kg of body weight increases Plt count by 50,0001 unit/10 kg of body weight increases Plt count by 50,000 Donor and Recipient must be ABO identicalDonor and Recipient must be ABO identical

Plasma and FFPPlasma and FFP Contents—Coagulation Factors (1 unit/ml)Contents—Coagulation Factors (1 unit/ml) StorageStorage
FFP--12 months at –18 degrees or colderFFP--12 months at –18 degrees or colder IndicationsIndications
Coagulation Factor deficiency, fibrinogen replacement, DIC, liver Coagulation Factor deficiency, fibrinogen replacement, DIC, liver disease, exchange transfusion, massive transfusiondisease, exchange transfusion, massive transfusion
ConsiderationsConsiderations Plasma should be recipient RBC ABO compatiblePlasma should be recipient RBC ABO compatible In children, should also be In children, should also be Rh compatibleRh compatible Account for time to thawAccount for time to thaw Usual dose is 20 cc/kg to raise coagulation factors approx 20%Usual dose is 20 cc/kg to raise coagulation factors approx 20%

CryoprecipitateCryoprecipitate DescriptionDescription
Precipitate formed/collected when FFP is thawed at 4Precipitate formed/collected when FFP is thawed at 4°° StorageStorage
After collection, refrozen and stored up to 1 year at -18After collection, refrozen and stored up to 1 year at -18°° IndicationIndication
Fibrinogen deficiency or dysfibrinogenemiaFibrinogen deficiency or dysfibrinogenemia vonWillebrands DiseasevonWillebrands Disease Factor VIII or XIII deficiencyFactor VIII or XIII deficiency DIC (not used alone)DIC (not used alone)
ConsiderationsConsiderations ABO compatible preferred (but not limiting)ABO compatible preferred (but not limiting) Usual dose is 1 unit/5-10 kg of recipient body weightUsual dose is 1 unit/5-10 kg of recipient body weight

Granulocyte TransfusionsGranulocyte Transfusions
Prepared at the time for immediate transfusion (no Prepared at the time for immediate transfusion (no storage available)storage available)
Indications – severe neutropenia assoc with infection Indications – severe neutropenia assoc with infection that has failed antibiotic therapy, that has failed antibiotic therapy, andand recovery of BM recovery of BM is expectedis expected
Donor is given G-CSF and steroids or HetastarchDonor is given G-CSF and steroids or Hetastarch ComplicationsComplications
Severe allergic reactionsSevere allergic reactions Can irradiate granulocytes for GVHD preventionCan irradiate granulocytes for GVHD prevention

Leukocyte Reduction FiltersLeukocyte Reduction Filters
Used for prevention of transfusion reactionsUsed for prevention of transfusion reactions Filter used with RBC’s, Platelets, FFP, Filter used with RBC’s, Platelets, FFP,
CryoprecipitateCryoprecipitate Other plasma proteins (albumin, colloid expanders, Other plasma proteins (albumin, colloid expanders,
factors, etc.) do not need filters—NEVER use filters factors, etc.) do not need filters—NEVER use filters with stem cell/bone marrow infusionswith stem cell/bone marrow infusions
May reduce RBC’s by 5-10%May reduce RBC’s by 5-10% Does not prevent Graft Verses Host Disease (GVHD)Does not prevent Graft Verses Host Disease (GVHD)

Transfusion ComplicationsTransfusion Complications
Acute Transfusion Reactions (ATR’s)Acute Transfusion Reactions (ATR’s) Chronic Transfusion ReactionsChronic Transfusion Reactions Transfusion related infectionsTransfusion related infections

Acute Transfusion ReactionsAcute Transfusion Reactions
Hemolytic Reactions (AHTR)Hemolytic Reactions (AHTR) Febrile Reactions (FNHTR)Febrile Reactions (FNHTR) Allergic ReactionsAllergic Reactions TRALITRALI Coagulopathy with Massive transfusionsCoagulopathy with Massive transfusions BacteremiaBacteremia Fluid overloadFluid overload

Frequency of Transfusion ReactionsFrequency of Transfusion Reactions
Adverse EffectAdverse Effect FrequencyFrequency CommentsComments
Acute Hemolytic RxnAcute Hemolytic Rxn 1 in 25,0001 in 25,000 Red cells onlyRed cells only
Anaphylactic hypotensiveAnaphylactic hypotensive 1 in 150,0001 in 150,000 Including IgAIncluding IgA
Febrile NonhemolyticFebrile Nonhemolytic 1 in 2001 in 200 CommonCommon
AllergicAllergic 1 in 1,0001 in 1,000 CommonCommon
Delayed HemolyticDelayed Hemolytic 1 in 2,5001 in 2,500 Red cells onlyRed cells only
RBC alloimmunizationRBC alloimmunization 1 in 1001 in 100 Red cells onlyRed cells only
WBC/Plt WBC/Plt alloimmunizationalloimmunization
1 in 101 in 10 WBC and Plt onlyWBC and Plt only

Acute Hemolytic Transfusion Acute Hemolytic Transfusion Reactions (AHTR)Reactions (AHTR)
Immune and non immune hemolysisImmune and non immune hemolysis Occurs when incompatible RBC’s are transfused into a Occurs when incompatible RBC’s are transfused into a
recipient who has pre-formed antibodies (usually ABO or Rh)recipient who has pre-formed antibodies (usually ABO or Rh) Antibodies activate the complement system, causing Antibodies activate the complement system, causing
intravascular hemolysisintravascular hemolysis Symptoms occur within minutes of starting the transfusionSymptoms occur within minutes of starting the transfusion This hemolytic reaction can occur with as little as 1-2 cc of This hemolytic reaction can occur with as little as 1-2 cc of
RBC’sRBC’s Labeling error is most common problemLabeling error is most common problem Can be fatalCan be fatal

Symptoms of AHTRSymptoms of AHTR
High fever/chillsHigh fever/chills HypotensionHypotension Back/abdominal painBack/abdominal pain OliguriaOliguria DyspneaDyspnea Dark urineDark urine PallorPallor

What to do?What to do?If an AHTR occursIf an AHTR occurs
STOP TRANSFUSIONSTOP TRANSFUSION ABC’sABC’s Maintain IV access and run IVF (NS or LR)Maintain IV access and run IVF (NS or LR) Monitor and maintain BP/pulseMonitor and maintain BP/pulse Obtain blood and urine for transfusion reaction Obtain blood and urine for transfusion reaction
workupworkup Send remaining blood back to Blood BankSend remaining blood back to Blood Bank

Labs found with AHTRLabs found with AHTR
HemoglobinemiaHemoglobinemia HemoglobinuriaHemoglobinuria Positive DATPositive DAT HyperbilirubinemiaHyperbilirubinemia Abnormal DIC panelAbnormal DIC panel

Monitoring in AHTRMonitoring in AHTR
Monitor patient clinical status and vital signsMonitor patient clinical status and vital signs Monitor renal status (BUN, creatinine)Monitor renal status (BUN, creatinine) Monitor coagulation status (DIC panel– Monitor coagulation status (DIC panel–
PT/PTT, fibrinogen, D-dimer/FDP, Plt, PT/PTT, fibrinogen, D-dimer/FDP, Plt, Antithrombin-III)Antithrombin-III)
Monitor for signs of hemolysis (LDH, bili, Monitor for signs of hemolysis (LDH, bili, haptoglobin)haptoglobin)

Febrile Nonhemolytic Transfusion Febrile Nonhemolytic Transfusion Reactions (FNHTR)Reactions (FNHTR)
Definition--Rise in patient temperature >1Definition--Rise in patient temperature >1°C °C (associated with transfusion without other fever (associated with transfusion without other fever precipitating factors)precipitating factors)
Occurs with approx 1% of PRBC transfusions and Occurs with approx 1% of PRBC transfusions and approx 20% of Plt transfusionsapprox 20% of Plt transfusions
FNHTR caused by alloantibodies directed against FNHTR caused by alloantibodies directed against HLA antigensHLA antigens
Need to evaluate for AHTR and infectionNeed to evaluate for AHTR and infection

What to do?What to do?If an FNHTR occursIf an FNHTR occurs
STOP TRANSFUSIONSTOP TRANSFUSION Use of AntipyreticsUse of Antipyretics Use of Corticosteroids for severe reactionsUse of Corticosteroids for severe reactions Use of Narcotics for shaking chillsUse of Narcotics for shaking chills Future considerationsFuture considerations
May prevent reaction with leukocyte filterMay prevent reaction with leukocyte filter Use single donor plateletsUse single donor platelets Use fresh plateletsUse fresh platelets Washed RBC’s or plateletsWashed RBC’s or platelets

Washed Blood ProductsWashed Blood Products
PRBC’s or platelets washed with salinePRBC’s or platelets washed with saline Removes all but traces of plasma (>98%)Removes all but traces of plasma (>98%) Indicated to prevent recurrent or severe reactionsIndicated to prevent recurrent or severe reactions Washed RBC’s must be used within 24 hoursWashed RBC’s must be used within 24 hours RBC dose may be decreased by 10-20% by washingRBC dose may be decreased by 10-20% by washing Does not prevent GVHDDoes not prevent GVHD

Allergic Nonhemolytic Transfusion Allergic Nonhemolytic Transfusion ReactionsReactions
EtiologyEtiology May be due to plasma proteins or blood May be due to plasma proteins or blood
preservative/anticoagulantpreservative/anticoagulant Best characterized with IgA given to an IgA deficient Best characterized with IgA given to an IgA deficient
patients with anti-IgA antibodies patients with anti-IgA antibodies Presents with urticaria and wheezingPresents with urticaria and wheezing TreatmentTreatment
Mild reactions—Can be continued after BenadrylMild reactions—Can be continued after Benadryl Severe reactions—Must STOP transfusion and may require Severe reactions—Must STOP transfusion and may require
steroids or epinephrinesteroids or epinephrine Prevention—Premedication (Antihistamines)Prevention—Premedication (Antihistamines)

TRALITRALITransfusion Related Acute Lung InjuryTransfusion Related Acute Lung Injury
Clinical syndrome similar to ARDSClinical syndrome similar to ARDS Occurs 1-6 hours after receiving plasma-containing Occurs 1-6 hours after receiving plasma-containing
blood productsblood products ANTIBODY HYPOTHESIS & NEUTROPHIL ANTIBODY HYPOTHESIS & NEUTROPHIL
PRIMING (magnet) HYPOTHESISPRIMING (magnet) HYPOTHESIS Caused by WBC antibodies present in donor blood Caused by WBC antibodies present in donor blood
that result in pulmonary leukostasisthat result in pulmonary leukostasispulmonary pulmonary edemaedema
Treatment is supportiveTreatment is supportive High mortalityHigh mortality

Massive TransfusionsMassive Transfusions
Coagulopathy may occur after transfusion of Coagulopathy may occur after transfusion of massive amounts of blood (trauma/surgery)massive amounts of blood (trauma/surgery)
Coagulopathy is caused by failure to replace Coagulopathy is caused by failure to replace plasmaplasma
See electrolyte abnormalitiesSee electrolyte abnormalities Due to citrate binding of CalciumDue to citrate binding of Calcium

Bacterial ContaminationBacterial Contamination
More common and more severe with platelet More common and more severe with platelet transfusion (platelets are stored at room transfusion (platelets are stored at room temperature)temperature)
OrganismsOrganisms Platelets—Gram (+) organisms, ie Staph/StrepPlatelets—Gram (+) organisms, ie Staph/Strep RBC’s—Yersinia, enterobacterRBC’s—Yersinia, enterobacter
Risk increases as blood products age (use fresh Risk increases as blood products age (use fresh products for immunocompromised)products for immunocompromised)

Chronic Transfusion ReactionsChronic Transfusion Reactions
AlloimmunizationAlloimmunization Transfusion Associated Graft Verses Host Transfusion Associated Graft Verses Host
Disease (GVHD)Disease (GVHD) Iron OverloadIron Overload Transfusion Transmitted InfectionTransfusion Transmitted Infection

AlloimmunizationAlloimmunization
Can occur with erythrocytes or plateletsCan occur with erythrocytes or platelets ErythrocytesErythrocytes
Antigen disparity of minor antigens (Kell, Duffy, Kidd)Antigen disparity of minor antigens (Kell, Duffy, Kidd) Minor antigens D, K, E seen in Sickle patientsMinor antigens D, K, E seen in Sickle patients
PlateletsPlatelets Usually due to HLA antigensUsually due to HLA antigens May reduce alloimmunization by leukoreduction (since May reduce alloimmunization by leukoreduction (since
WBC’s present the HLA antigens)WBC’s present the HLA antigens)

Transfusion Associated GVHDTransfusion Associated GVHD
Mainly seen in infantsMainly seen in infants Etiology—Results from engraftment of donor Etiology—Results from engraftment of donor
lymphocytes of an immunocompetent donor lymphocytes of an immunocompetent donor into an immunocompromised hostinto an immunocompromised host
Symptoms—Diarrhea, skin rash, pancytopeniaSymptoms—Diarrhea, skin rash, pancytopenia Usually fatal—no treatmentUsually fatal—no treatment Prevention—Irradiation of donor cellsPrevention—Irradiation of donor cells

Transfusion Associated Transfusion Associated InfectionsInfections
Hepatitis CHepatitis C Hepatitis BHepatitis B HIVHIV CMVCMV
CMV can be diminished by leukoreduction, which CMV can be diminished by leukoreduction, which is indicated for immunocompromised patientsis indicated for immunocompromised patients