Embed Size (px)
Citation preview

+ MODEL
Journal of Plastic, Reconstructive & Aesthetic Surgery (2014) xx, 1e9
Blood flow through sutured and coupledmicrovascular anastomoses: A comparativecomputational study*
Richard A.J. Wain a,b,c,*, Justin P.M. Whitty b, Milind D. Dalal c,Michael C. Holmes d, Waqar Ahmed e
a Department of Plastic & Reconstructive Surgery, Christie Hospital NHS Foundation Trust,Wilmslow Road, Manchester M20 4BX, UKb School of Computing, Engineering and Physical Sciences, University of Central Lancashire,Fylde Road, Preston, Lancashire PR1 2HE, UKc Department of Plastic & Reconstructive Surgery, Royal Preston Hospital, Lancashire TeachingHospitals NHS Foundation Trust, Sharoe Green Lane, Preston, Lancashire PR2 9HT, UKd Graduate Research School, University of Central Lancashire, Fylde Road, Preston, Lancashire PR12HE, UKe School of Postgraduate Medicine and Dentistry, University of Central Lancashire, Fylde Road,Preston, Lancashire PR1 2HE, UK
Received 1 September 2013; accepted 15 March 2014
KEYWORDSMicrovascular;Anastomosis;Computationalmodelling;Sutured;Coupled;Coupler
* Presentations: This work was preseJune 2013.* Corresponding author. Departmen
Manchester M20 4BX, UK. Tel.: þ44 (0E-mail address: richwain@doctors.
Please cite this article in press as: Wcomputational study, Journal of Plas
http://dx.doi.org/10.1016/j.bjps.2014.01748-6815/ª 2014 British Association of P
Summary This study uses computational fluid dynamics (CFD) to model blood flow throughidealised sutured and coupled arterial anastomoses to investigate the affect of each techniqueon intravascular blood flow.
Local flow phenomena are examined in detail to study characteristics that potentiallyinitiate thrombus formation; for example, changes in velocity profile, wall shear stress(WSS), and shear strain rate (SSR).
Idealised geometries of sutured and coupled anastomoses were created with dimensionsidentical to microvascular suture material and a commercially available coupling device usingCFD software. Vessels were modelled as non-compliant 1 mm diameter ducts, and blood wassimulated as a Newtonian fluid, in keeping with previous studies. All analyses were steady-state and performed on arteries.
The sutured simulation revealed a reduced boundary velocity profile; high WSS; and high SSRat the suture sites. The coupled anastomosis simulation showed a small increase in maximumWSS at the anastomotic region compared to a pristine vessel, however, this was less than half
nted as a podium presentation at the BAPRAS Summer Scientific Meeting, Nottingham, 19th e 21st
t of Plastic & Reconstructive Surgery, Christie Hospital NHS Foundation Trust, Wilmslow Road,) 161 446 3000; fax: þ44 (0) 161 446 3977.org.uk (R.A.J. Wain).
ain RAJ, et al., Blood flow through sutured and coupled microvascular anastomoses: A comparativetic, Reconstructive & Aesthetic Surgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016
3.016lastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved.

2 R.A.J. Wain et al.
+ MODEL
Please cite this article in press as: Wcomputational study, Journal of Plas
that of the sutured model. The coupled vessel displayed an average WSS equivalent to a pris-tine vessel simulation.
Taken together these observations demonstrate a theoretically more thrombogenic profile ina sutured anastomosis when compared to a coupled vessel. Data from simulations on a coupledanastomosis reveal a profile that is nearly equivalent to that of a pristine vessel. Based purelyon the combination of less favourable flow properties shown using these idealised arterialmodels, the sutured method is potentially more thrombogenic than a coupled anastomosis.ª 2014 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Introduction
Microvascular anastomoses are performed for a wide rangeof indications within plastic & reconstructive, head & neck,maxillofacial, and transplant surgery. These include free-tissue transfer for reconstruction of composite defects andvascularised enteral conduits following head and neckcancers; revascularisation of traumatic amputations, im-plantation of transplanted organs, and restoration of vol-ume and contour for autologous breast reconstruction.Over 40 000 people per year are affected by breast cancerin the UK and is the country’s most common cancer.1 In theUSA, over 200 000 women develop invasive breast cancereach year,2 and around 13 000 of these patients undergoreconstruction using autologous free-tissue transfer.3
In the early post operative period, free-flap survival de-pends largely on the arterial supply and venous drainage ofthe anastomosed vessels. The incidence of free-flap failurehas been quoted at approximately 5%, with the majority ofthese due to intravascular thrombus.4 Blood clots have apropensity to formwithin vessels when there is an alterationin blood composition, the vessel wall, or local blood flow.5
Historically vessels have been anastomosed end-to-endusing sutures, which remains the preferred method. How-ever, more recently6 coupling devices have been developedto produce a sutureless anastomosis. These coupling devicesconsist of two polyethylene rings with interlocking stainlesssteel pins to provide intimaeintima contact. Couplers havebeen used in clinical practice for several years and demon-strate venous thrombosis rates approximately equivalent tosutured anastomoses.7 A recent study of 1000 consecutivecoupled anastomoses found thrombosis rates of 0.6%which islower than that stated for standard sutured anastomoses.8
The commercially available coupling device has beendesigned for venous anastomoses and is not recommendedfor arterial coupling. Reasons for avoiding arterial couplingusing this device include thicker and less pliable vesselwalls, which makes placement onto the pins more chal-lenging and often necessitates use of a smaller diametercoupler. This in turn would restrict blood flow and poten-tially lead to thrombosis.8 In 1994 Ahn et al.9 reported a 14%(4/29) intraoperative abandonment rate due restricted flowas a result of these properties, and 3.5% (1/29) vesseltrauma rate in arterial coupled anastomoses.
Despite this, arterial coupling has been successfullyperformed by a few groups both in head & neck surgery,10,11
and for breast reconstruction.12 Also, of the subsequent 24completed arterial coupled anastomoses performed by Ahn
ain RAJ, et al., Blood flow througtic, Reconstructive & Aesthetic S
et al.,9 there were no complications. This demonstrates anaspiration to perform arterial coupling, and as such theneed to investigate whether arterial coupling can be showndefinitively to have flow characteristics comparable to, orbetter than, sutured arterial anastomoses.
Studies into computational modelling of fluid dynamicswithin blood vessels have been carried out in the past13;however these have generally examined flow in cardiacvessels or in larger peripheral vessels. One paper14 hasdiscussed computational modelling of microarterial anas-tomotic techniques with size discrepancy but this did notaddress the effect of sutures on flow. Another studyinvestigated stress values at anastomotic sites, but has notconsidered local fluid dynamics in detail and has also notlooked at the effect of sutures.15 There are no currentstudies that have evaluated flow properties throughmicrovascular coupling devices and sutured anastomoses.
Although low flow and stasis within vessels are risk factorsfor thrombus formation,16 it is known that Shear Strain Rate(SSR) is a more reliable indicator than flow-rate or velocitywhen evaluating coagulation in the presence of flow.17 This isbecause transport phenomena near the surface of vesselsgoverns the SSR and describes the change of flow velocitywith increasing distance from the surface.18 SSR is defined asthe rate of change of strain when a shear stress is applied.
Wall Shear Stress (WSS), which is the tangential force offlowing blood on the endothelial surface, is directly relatedto SSR and has been implicated as a factor leading toatheroma formation within blood vessels.19e22 More impor-tantly for this research, high WSS and SSR have also beenstrongly linked to platelet activation.16,23e25 This is partic-ularly important when considering blood coagulation andthrombosis, as activated platelets adhere to each other toform aggregates, and subsequently thrombus. In addition,shear-induced platelet thrombus formation appears to pro-mote the generation of fibrin through the activity of solublecoagulation factors.26 Excessive generation of fibrin alsoleads to thrombosis. Interestingly, shear-activated plateletsdo not appear to adhere to an intact vessel wall endothe-lium,27 but they do bind tightly to injured endothelium andexposed subendothelium.17 This may be more important insutured anastomoses than in coupled anastomoses as there isa greater chance of exposed thrombogenic subendotheliumin the sutured technique,28 both from the suture sitesthemselves and from the cut vessel ends.
Shen et al.24 and Roth25 demonstrated that a SSR ofgreater than 1000 s�1 causes direct activation of platelets.A recent computational study29 found a positive correlation
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

Blood flow through sutured and coupled microvascular anastomoses 3
+ MODEL
between thrombus accumulation rates and SSR up to6000 s�1. The same study also showed that thrombusgrowth rates were two to four times greater at higher SSRthan for physiological shear rates of less than 400 s�1.29
This study uses CFD to model arterial blood flow throughidealised sutured and coupled anastomoses to investigatethe effect of each technique on intravascular flow. Localflow phenomena are examined in detail around suture andcoupler sites to investigate characteristics that couldpotentially initiate thrombus formation for example:changes in velocity profile, WSS, and SSR.
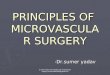
Figure 2 CATIA coupled anastomosis exploded assembly.
Methods
Geometry creation
The coupled anastomosis was created in the ComputerAided Three-Dimensional Interactive Application (CATIA),Computer Aided Design (CAD) program using measurementstaken from a 1 mm GEM Microvascular AnastomoticCoupling (MAC) device under an operating microscope(Figure 1(a and b)). The microvascular anastomosis proce-dure was then replicated using the CAD coupler and com-puter generated vessels of 1 mm diameter and 0.1 mm wallthickness15 (Figure 2), in order to provide an accuraterepresentation of the fluid control volume for evaluation(Figure 3(aec)). This control volume was then transferred
Figure 1 Micrographs of the coupling device (a) plan and (b)side elevation used to construct CATIA model.
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
into the CFD programme ANSYS-CFX for detailed analysis.The anastomosed vessels were of identical diameter,thereby eliminating any potential variance caused by sizediscrepancy. Computational studies of vessels with sizediscrepancy have previously been described.14
Figure 3 Control volume creation (a) section creation, (b)resulting section and (c) symmetric fluid volume for analysis.
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

4 R.A.J. Wain et al.
+ MODEL
The sutured anastomosis was created using Design-Modeler within the ANSYS Workbench software. A series often tori of diameter 0.03 mm (the same as 10-0 Ethilonmicrovascular suture) was formed circumferentially arounda 1 mm vessel to represent the suture material. This ring ofsutures was then subtracted from the vessel to leave thefluid control volume with suture-shaped imprints at corre-sponding locations (Figure 4(a and b)), thereby implyingthat vessel walls are non-compliant i.e. are rigid. Our aimwas to simulate blood flow through each type of anasto-mosis to look for flow properties that may induce thrombusformation. Hence, the simulated vessels exclude thestructural mechanical properties and evaluate only thehaemodynamic properties. It is envisaged that futurestudies will provide a more clinically relevant picture withsimulations accounting for vascular compliance, however,the computational complexity i.e. fluidestructure interac-tion, is beyond this preliminary study.
Figure 4 Sutured modelling process (a) tori ring (b) sub-traction body operation.
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
Boundary conditions
Each model requires accurate boundary conditions toenable appropriate conclusions to be drawn from the ob-tained results. All vascular simulations were carried outusing blood as the working fluid. This was modelled as anincompressible Newtonian fluid with a density of1060 kg m�3 and viscosity of 3.5 mPa s in accordance withcurrent literature.14,30e33 Vessels were given a constantlaminar mass flow rate of 1.045 � 10�4 kg s�1, which wascalculated from the maximum volume flow rate through theright femoral artery of a single 410 g outbred male Wistarrat in the study by Rickard et al.14 This vessel was chosen asit closely matches the mean diameter of an internalmammary artery perforator.14 Again, in keeping with pre-vious studies,14,31,33,34 including an international study onintracerebral blood flow,32 all walls were simulated as rigid,non-compliant structures with non-slip conditions. A sum-mary of all data entered into the simulations can be foundin Table 1.
Simulation and post-processing
Wall velocity (boundary layer velocity) profiles werecreated for each geometry to examine anastomotic flow indetail. The boundary layer velocity streamlines weregenerated from the inlet to better visualise flow patternscaused by the variance in geometry, particularly at the wallin the anastomotic region. As the Reynolds number (Re) waslow in all simulations (Re w 90), turbulence is not present.Hence, a standard laminar solver resident in the ANSYS-CFXsolver was employed for all simulations.
Importantly, as high WSS has been linked to plateletactivation and therefore thrombus formation, WSS and SSRwere also determined for each simulation. Images demon-strating the output of each stage of the post-processingphase are shown in Results.
Table 1 Summary of input data parameters.
Vessel diameter 1 mmVessel section length 5 mmVessel walls Non-compliant, Non-slipFlow regimen Laminar, Steady-stateReynolds number (Re) z90Fluid type Blood (Newtonian)Blood density 1060 kg m�3
Blood viscosity 0.0035 Pa sInlet profile Paraboloid
(fully developed flow)Mass flow rate 1.045 � 10�4 kg s�1
(Calculated from14)Relative pressure 0 PaAdvection scheme High resolution
(ANSYS default)Convergence control 1e100 iterations
(ANSYS default)Convergence criteria
Root Mean Squared (RMS)1 � 104 (ANSYS default)
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

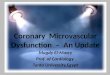
Figure 6 Boundary (wall) velocity streamlines at the couplerinterface.
Blood flow through sutured and coupled microvascular anastomoses 5
+ MODEL
Statistical methods
In order to decipher the relative likelihood of blood clotpropagation as a result of the surgical procedures, the WSSof the sutured and coupled anastomoses should be as closeto that of a natural pristine vessel as possible. Hence, theregions of high WSS within the sutured and coupled modelsindicate the most likely locations for platelet activationand subsequent thrombus formation. It is thereforenecessary to determine whether the WSS values for thesutured technique are significantly greater than those forthe coupled method.
From a statistical analysis viewpoint, this statement canbe expressed as the null (Ho) and scientific (Hs) hypothesisrespectively, thus:
Ho : mðSÞtw
� mðCÞtwZ0
Hs : mðSÞtw
� mðCÞtw
> 0
where mðSÞtw is the inferred population mean WSS of the su-
tured anastomosis and mðCÞtw is the inferred population mean
WSS of the coupled anastomosis. A homoscedastic Student’st-test will be performed at the 99.9% confidence level ontwo samples of data collected from the simulated anasto-motic sites of each technique.
Results
Evaluation of velocity profiles, WSS, and SSR distributionsare addressed in turn for both the sutured and coupledsimulations.
Velocity
The overall velocity profile remains largely uniformthroughout the vessel; however there is altered flow aroundsuture sites in the boundary layer. Blood is seen divergingaround the suture and slowing in velocity (Figure 5). Ve-locity profiles in the coupled simulation show altered flowat the coupler interface (Figure 6), but very similar averageand maximum boundary velocities (Table 2).
Figure 5 Boundary (wall) velocity streamlines around a sin-gle suture.
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
WSS and SSR
Both mean and maximum WSS and SSR are elevated in thesutured model when compared to the coupled simulation.Most importantly, the areas of maximum WSS and SSR areconfined to the suture sites (Figure 7(a and b)) therebyindicating thrombogenic potential. WSS and SSR profiles forthe coupled model demonstrate a regular annular distri-bution of raised WSS and SSR (Figure 8(a and b)). Themaximum WSS and SSR in the coupled anastomosis is lessthan half that seen in the sutured simulation. A directcomparison of the mean and maximum WSS and SSR can beseen in Table 3. It is important to note that the WSS and SSRprofiles for the coupled anastomosis are almost identical tothat of a control pristine vessel.
Statistical results
The results of the t-test are summarised in Table 4. Themean values indicate an overall greater mean WSS for thesutured anastomosis. As the variance of the samples is quitedifferent, it is not appropriate to infer this is true for thewhole population from this analysis alone. However, thetest statistic (t-value) is very high (11.4) in this case, i.e.much greater than the critical value calculated at the 0.1%confidence level of 3.36; which indicates a highly statisti-cally significant result as evidenced by the probability ofthe null hypothesis (p Z 3.83 � 10�13). Incidentally thehomoscedastic assumption was validated via an appropriateFisher’s F-test where the test’s null hypothesis wasretained at the 2% confidence level as shown in Table 5.
Table 2 Mean and maximum boundary velocitycomparison.
Mean boundaryvelocity(�10�3 m s�1)
Maximumboundary velocity(�10�3 m s�1)
Pristine 4.33 � 0.2 6.43 � 0.3Sutured 6.32 � 0.3 9.62 � 0.5Coupled 6.24 � 0.3 9.34 � 0.5
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

Figure 7 Sutured anastomosis (a) WSS distribution around asingle suture (b) SSR distribution.
Figure 8 Coupled anastomosis (a) WSS distribution at thecoupler interface (b) SSR distribution.
6 R.A.J. Wain et al.
+ MODEL
Discussion
Although previous studies have used CFD to evaluate flowwithin blood vessels, none have examined in detail thelocal fluid dynamics around sutured and coupled micro-vascular anastomoses. This study has utilised the commer-cial CFD code ANSYS-CFX to specifically target the localfluid properties at suture sites and the coupler interface,investigating the theoretical potential for intravascularthrombus formation in these two techniques. Based on theassumptionf that higher SSRs are proportional to theamount of platelet activation, this may indicate that thehigher the SSR, the greater proportion of platelets will beactivated, thereby increasing the amount and rate ofthrombus formation. Here the modelling approach pur-posefully neglects vessel wall compliance, mainly to avoidcomplex fluidestructural interaction models, althoughthese techniques are currently being developed.
Clinical evaluation
This study has demonstrated that the flow patterns in su-tured and coupled microvascular anastomoses vary suffi-ciently to produce different physical properties at the
f As platelets become activated and form aggregates, the hy-draulic diameter of the system reduces, thereby increasing pres-sure at the anastomotic site.35 This pressure increase is resolvedinto the shear stress at the walls, which is proportional to the SSR.
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
anastomotic site, and as such have different potential af-fects on coagulation and thrombus formation. Purely basedon the data gathered from the simulations performed, clotformation may be more likely using the sutured techniquerather than the coupler. Anecdotally, the opinion in thesurgical community is that a coupled venous anastomosis isat least as good, if not better than a sutured anastomosis.This is supported by studies demonstrating reduced venousthrombosis rates in comparative series (coupled 1.5% vs.sutured 3.3%7), and very low thrombosis rates (0.6%8) forcoupled anastomoses.
Thrombus formation in hand sutured arterial anasto-moses accounts for approximately 25% of all post operativevessel thrombosis.36 This represents around 1% of all freeflaps36,37 and, whilst this is low, it signifies a large numberof failed free flaps overall. As arterial coupling is notroutine practice, there is little data to evaluate for com-parison with arterial sutured anastomoses. In addition, thestudies that have been performed on arterial couplinginclude relatively low numbers, around 50e100,10e12 whencompared with those carried out on venous coupled anas-tomoses, where 1000 anastomoses were evaluated.8
Consequently, the thrombosis rates in coupled arterialanastomoses range from 0% (0/62)12 to 3.2% (4/124).11 It istherefore difficult to draw firm conclusions from thecurrently available clinical data as to the success of arterialcoupling.
This research has generated raw physical data support-ing the clinical findings of these limited studies: that thecoupled arterial anastomosis is less likely to precipitatethrombus formation. Furthermore, solely on the physical
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

Table 3 Mean and maximum comparison of WSS and SSR.
Mean wallshear stress (Pa)
Maximum wallshear stress (Pa)
Mean shear strainrate (�103 s�1)
Maximum shearstrain rate (�103 s�1)
Pristine 3.50 � 0.17 3.82 � 0.2 0.95 � 0.047 1.10 � 0.055Sutured 4.54 � 0.2 9.91 � 0.5 0.82 � 0.041 2.69 � 0.134Coupled 3.52 � 0.17 4.82 � 0.2 0.85 � 0.042 1.25 � 0.062
Blood flow through sutured and coupled microvascular anastomoses 7
+ MODEL
findings noted it is possible to recommend that, should asutured anastomosis be performed, the smallest possiblenumber of sutures should be placed in order to minimisetheir thrombogenic potential, whilst maintaining a well-sealed anastomosis. This experimental observation sup-ports the view held anecdotally by many microsurgeons.
In addition to the physical flow properties of the suturedanastomosis being potentially more thrombogenic than thatof the coupler; the time taken to perform a sutured anas-tomosis is far greater (22.3 min38) than the coupled tech-nique (5 min39). Based on the combination of adverse flowproperties; a longer operative, and therefore ischaemia,time; and a higher thrombosis rate, the sutured methodcould be depicted as less favourable.
The potential impact of this research lies in the ability totransfer these findings into clinically relevant and appli-cable recommendations. Although the simulations in thisproject have been accurately created under reliable andrealistic physical conditions, the models are idealised andrely on a series of assumptions which may not translatedirectly into clinical practice. These include vessels withnon-compliant walls, and the steady-state nature of bloodflow, and will be addressed in our subsequent work. Thissaid, although the addition of a pulse will make the simu-lations more realistic, the extremes of change in flowthroughout the cardiac cycle would likely cancel each otherout, and may not be significant analytically. In order tofurther validate our current and future computationalsimulations, comparison with suitable animal models maybe beneficial.
It is also worth noting that as this study was intended toexamine flow properties only, the characteristics of arte-riosclerosis have not been incorporated into the models.The complexity of adding plaques with different structuralproperties to that of the vessel wall was outside the scope
Table 4 Statistical analysis of WSS for sutured and coupled sim
Sample size
Sutured 18Coupled 16
Summary
Degrees of freedom 32Test statistics (t-value) 11.43
One-tailed distribution
p-level 3.83 � 10�13
Two-tailed distribution
p-level 7.66 � 10�13
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
of this primary study. In addition to reducing arterial wallcompliance, the hydraulic diameter would also be reducedas a result of the plaques, thereby affecting flow propertieswithin the vessel and at the anastomosis. Arteriosclerosiswould also affect the technical difficulty of applying acoupling device or indeed performing a sutured anasto-mosis. For these reasons, one would usually avoid usingsuch vessels for microvascular anastomoses where possible.
Despite this, it is likely that the fundamental fluid flowsresulting from geometrical differences in the anastomotictechniques will remain largely unchanged. This implies thatas long as there are sutures, or a coupler, at the anasto-motic site, there will be geometrical changes in the lumenof the vessel that can propagate blood clots, irrespective ofthe increased accuracy of the boundary conditions (e.g.compliant walls and pulsatile flow).
Analytical evaluation
The statistical analysis implies strong evidence for rejec-tion of the null hypothesis (Ho) in favour of the scientifichypothesis (Hs), thereby inferring that the values of WSS inthe sutured anastomosis are indeed greater than those ofthe coupled anastomosis. Therefore, initiation of throm-bosis formation is more likely in the sutured anastomotictechnique as there is a 28% increase in the average WSSwhen compared to the coupled method. Incidentally, themaximum WSS seen in the sutured model is 1.5 timesgreater than that in the coupled simulation, when using anatural pristine vessel as a control.
Shear Strain Rates (SSR) were not analysed statisticallyas the SSR is directly proportional to WSS in Newtonianfluids. Hence, the statistical results would reveal the samerelationship.
ulations (p 0.1%).
Mean Variance
8.38 2.073.16 1.42
Hypothesized mean difference 0Pooled variance 1.76
t Critical value (p 0.1%) 3.36
t Critical value (p 0.1%) 3.62
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

Table 5 F test for WSS in sutured and coupled simulations(p 2%).
Coupled Sutured
Sample size 16 18Mean 3.16 8.38Variance 1.42 2.07Standard deviation 1.19 1.43Mean standard error 0.29 0.33
Summary
F 1.44 F Criticalvalue (p 2%)
2.96
p-level 1-tailed 0.23 p-level 2-tailed 0.47H0 (2%)? Accepted
8 R.A.J. Wain et al.
+ MODEL
Conclusion
Data from the coupled simulations reveals a profile that ispotentially less thrombogenic than that of the suturedanastomosis, and that is almost equivalent to that of anatural pristine vessel. This numerical data supports thelimited clinical evidence in favour of arterial coupling.
Funding
This research study was funded by a grant from the Rose-mere Cancer Foundation, Rosemere Cancer Centre, RoyalPreston Hospital, Sharoe Green Lane, Preston, Lancashire,PR2 9HT. The authors have no financial interest to declarein relation to the content or products within this article.Measurements were taken from the following products inorder to produce the computational models:
� 1 mm GEM Microvascular Anastomotic Coupling (MAC)system produced by Synovis Micro Companies Alliance,Inc., 439 Industrial Lane, Birmingham, AL 35211, USA
� 10-0 Ethilon microvascular suture produced by Ethicon,Johnson & Johnson, Main Office, Route 22 West, Som-erville, NJ 08876, USA
Conflicts of interest
None.
Acknowledgements
The authors wish to thank Mr Rory Rickard for his advice oncompiling the manuscript.
References
1. Curo. Breast reconstruction e patient information guide[internet] [cited 26.03.11]. Available from: http://www.bapras.org.uk/guide.asp?idZ358.
2. U.S. breast cancer statistics [internet] [cited 27.10.12].Available from: http://www.breastcancer.org/symptoms/understand_bc/statistics.
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
3. American Society of Plastic Surgeons: report of the 2010 plasticsurgery statistics: reconstructive breast procedures [internet].Available from: http://www.plasticsurgery.org/Documents/news-resources/statistics/2010-statisticss/Patient-Ages/2010-reconstructive-demographics-breast-surgery-statistics.pdf.
4. Kroll SS, Schusterman MA, Reece GP, et al. Choice of flap andincidence of free flap success. Plast Reconstr Surg 1996 Sep;98(3):459e63.
5. Lopez JA, Chen J. Pathophysiology of venous thrombosis.Thromb Res 2009;123(Suppl. 4):S30e4.
6. Ostrup LT, Berggren A. The UNILINK instrument system for fastand safe microvascular anastomosis. Ann Plast Surg 1986 Dec;17(6):521e5.
7. Yap LH, Constantinides J, Butler CE. Venous thrombosis incoupled versus sutured microvascular anastomoses. Ann PlastSurg 2006 Dec;57(6):666e9.
8. Jandali S, Wu LC, Vega SJ, Kovach SJ, Serletti JM. 1000consecutive venous anastomoses using the microvascularanastomotic coupler in breast reconstruction. Plast ReconstrSurg 2010 Mar;125(3):792e8.
9. AhnCY,ShawWW,BernsS,MarkowitzBL.Clinicalexperiencewiththe 3M microvascular coupling anastomotic device in 100 free-tissue transfers. Plast Reconstr Surg 1994 Jun;93(7):1481e4.
10. Ross DA, Chow JY, Shin J, et al. Arterial coupling for micro-vascular free tissue transfer in head and neck reconstruction.Arch Otolaryngol Head Neck Surg 2005 Oct;131(10):891e5.
11. Chernichenko N, Ross DA, Shin J, Chow JY, Sasaki CT, Ariyan S.Arterial coupling for microvascular free tissue transfer. Oto-laryngol Head Neck Surg 2008 May;138(5):614e8.
12. Spector JA, Draper LB, Levine JP, Ahn CY. Routine use ofmicrovascular coupling device for arterial anastomosis inbreast reconstruction. Ann Plast Surg 2006 Apr;56(4):365e8.
13. Migliavacca F, Dubini G. Computational modeling of vascularanastomoses. Biomech Model Mechanobiol 2005 Jun;3(4):235e50.
14. Rickard RF, Meyer C, Hudson DA. Computational modeling ofmicroarterial anastomoses with size discrepancy (small-to-large). J Surg Res 2009 May 1;153(1):1e11.
15. Al-Sukhun J, Lindqvist C, Ashammakhi N, Penttila H. Micro-vascular stress analysis. Part I: simulation of microvascularanastomoses using finite element analysis. Br J Oral MaxillofacSurg 2007 Mar;45(2):130e7.
16. Lowe GDO. Virchow’s triad revisited: abnormal flow. Patho-physiol Haemost Thromb 2003 Dec;33(5e6):455e7.
17. Sakariassen KS, Nievelstein PF, Coller BS, Sixma JJ. The role ofplatelet membrane glycoproteins Ib and IIb-IIIa in plateletadherence to human artery subendothelium. Br J Haematol1986 Aug;63(4):681e91.
18. Ismagilov RF, Stroock AD, Kenis PJA, Whitesides G, Stone HA.Experimental and theoretical scaling laws for transversediffusive broadening in two-phase laminar flows in micro-channels. Appl Phys Lett 2000 Apr 24;76(17):2376e8.
19. Ku DN, Giddens DP, Zarins CK, Glagov S. Pulsatile flow andatherosclerosis in the human carotid bifurcation. Positivecorrelation between plaque location and low oscillating shearstress. Arteriosclerosis 1985 Jun;5(3):293e302.
20. DePaola N, Gimbrone Jr MA, Davies PF, Dewey Jr CF. Vascularendothelium responds to fluid shear stress gradients. Arte-rioscler Thromb 1992 Nov;12(11):1254e7.
21. Shaaban AM, Duerinckx AJ. Wall shear stress and earlyatherosclerosis: a review. AJR Am J Roentgenol 2000 Jun;174(6):1657e65.
22. Caro CG, Cheshire NJ, Watkins N. Preliminary comparativestudy of small amplitude helical and conventional ePTFEarteriovenous shunts in pigs. J R Soc Interface 2005 Jun 22;2(3):261e6.
23. Hathcock JJ. Flow effects on coagulation and thrombosis.Arterioscler Thromb Vasc Biol 2006 Aug;26(8):1729e37.
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016

Blood flow through sutured and coupled microvascular anastomoses 9
+ MODEL
24. Shen F, Kastrup CJ, Liu Y, Ismagilov RF. Threshold response ofinitiation of blood coagulation by tissue factor in patternedmicrofluidic capillaries is controlled by shear rate. ArteriosclerThromb Vasc Biol 2008 Nov;28(11):2035e41.
25. Roth GJ. Developing relationships: arterial platelet adhesion,glycoprotein Ib, and leucine-rich glycoproteins. Blood 1991 Jan1;77(1):5e19.
26. Weiss HJ, Turitto VT, Baumgartner HR. Role of shear rate andplatelets inpromotingfibrin formationon rabbit subendothelium.Studies utilizing patients with quantitative and qualitativeplatelet defects. J Clin Invest 1986 Oct;78(4):1072e82.
27. Grabowski EF. Platelet aggregation in flowing blood at a site ofinjury to an endothelial cell monolayer: quantitation and real-time imaging with the TAB monoclonal antibody. Blood 1990Jan 15;75(2):390e8.
28. Macchiarelli GM, Familiari G, Caggiati A, et al. Arterial repairafter microvascular anastomosis. Cells Tissues Organs 1991;140(1):8e16.
29. Bark Jr DL, Para AN, Ku DN. Correlation of thrombosis growthrate to pathological wall shear rate during platelet accumu-lation. Biotechnol Bioeng 2012 Oct;109(10):2642e50 [Internet][cited 2012 Jul 14]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/22539078.
30. Perktold K, Florian H, Hilbert D. Analysis of pulsatile blood flow:a carotid siphon model. J Biomed Eng 1987 Jan;9(1):46e53.
31. Karmonik C, Bismuth J, Davies MG, Lumsden AB. Computa-tional fluid dynamics as a tool for visualizing hemodynamicflow patterns. Methodist Debakey Cardiovasc J 2009;5(3):26e33.
Please cite this article in press as: Wain RAJ, et al., Blood flow througcomputational study, Journal of Plastic, Reconstructive & Aesthetic S
32. Berti G. @neurIST D23v2-Analysis protocols version 2(internet)[cited 20.04.12]. Available from: http://www.aneurist.org/UserFiles/File/PUBLIC_DELIVERABLES/D23v2_v1.2_final.pdf;2010.
33. Chaniotis AK, Kaiktsis L, Katritsis D, Efstathopoulos E, Pantos I,Marmarellis V. Computational study of pulsatile blood flow inprototype vessel geometries of coronary segments. Phys Med2010;26(3):140e56.
34. Perktold K, Leuprecht A, Prosi M, et al. Fluid dynamics, wallmechanics, and oxygen transfer in peripheral bypass anasto-moses. Ann Biomed Eng 2002 Apr;30(4):447e60.
35. Murray CD. The physiological principle of minimum work: i. thevascular system and the cost of blood volume. Proc Natl AcadSci U S A 1926 Mar;12(3):207e14.
36. Bui DT, Cordeiro PG, Hu Q-Y, Disa JJ, Pusic A, Mehrara BJ. Freeflap reexploration: indications, treatment, and outcomes in1193 free flaps. Plast Reconstr Surg 2007 Jun;119(7):2092e100.
37. Mao C, Yu G, Peng X, Guo C, Huang M. Postoperative vesselthrombosis and its management after free flap transfers inhead and neck region. Zhonghua Er Bi Yan Hou Tou Jing Wai KeZa Zhi 2005 Jun;40(6):415e8.
38. Zeebregts C, Acosta R, Bolander L, van Schilfgaarde R,Jakobsson O. Clinical experience with non-penetratingvascular clips in free-flap reconstructions. Br J Plast Surg2002 Mar;55(2):105e10.
39. Cope C. Technique and clinical experience of the Uni-link/3M(R) microvascular anastomotic coupling device in freeflap surgery [Internet] J Plast Surg 2001;1(1).
h sutured and coupled microvascular anastomoses: A comparativeurgery (2014), http://dx.doi.org/10.1016/j.bjps.2014.03.016