Embed Size (px)
Citation preview

The University of ToledoThe University of Toledo Digital Repository
Theses and Dissertations
2015
Blood flow and oxygenation dynamics as a result ofhuman skeletal muscle stretchingNicholas T. KruseUniversity of Toledo
Follow this and additional works at: http://utdr.utoledo.edu/theses-dissertations
This Dissertation is brought to you for free and open access by The University of Toledo Digital Repository. It has been accepted for inclusion in Thesesand Dissertations by an authorized administrator of The University of Toledo Digital Repository. For more information, please see the repository'sAbout page.
Recommended CitationKruse, Nicholas T., "Blood flow and oxygenation dynamics as a result of human skeletal muscle stretching" (2015). Theses andDissertations. 2064.http://utdr.utoledo.edu/theses-dissertations/2064

i
A Dissertation
entitled
Blood Flow and Oxygenation Dynamics as a Result of Human Skeletal Muscle
Stretching
by
Nicholas T. Kruse
Submitted to the Graduate Faculty as partial fulfillment of the requirements for the
Doctor of Philosophy Degree in
Exercise Science
_________________________________________
Dr. Barry W. Scheuermann, Committee Chair
_________________________________________
Dr. Sophie Lalande, Committee Member
_________________________________________
Dr. Michael Tevald, Committee Member
_________________________________________
Dr. Suzanne Wambold, Committee Member
_________________________________________
Dr. Patricia R. Komuniecki, Dean
College of Graduate Studies
The University of Toledo
May 2015

Copyright 2015, Nicholas T. Kruse
This document is copyrighted material. Under copyright law, no parts of this document
may be reproduced without the expressed permission of the author.

iii
An Abstract of
Blood Flow and Oxygenation Dynamics as a Result of Human Skeletal Muscle
Stretching
by
Nicholas T. Kruse
Submitted to the Graduate Faculty as partial fulfillment of the requirements for the
Doctor in Philosophy Degree in
Exercise Science
The University of Toledo
May 2015
This dissertation examined the effect of skeletal muscle stretching on central and
peripheral cardiovascular responses in humans. Healthy males performed controlled
passive stretching at three different stretching intensities of the plantar flexors on an
isokinetic dynamometer. To determine how stretching effects peripheral cardiovascular
parameters of muscle blood flow and perfusion of the popliteal artery, Doppler
ultrasound velocimetry and imaging techniques were used to determine mean blood flow
(MBF), antegrade blood flow and retrograde blood flow responses while near infrared
spectroscopy (NIRS) was used to measure changes in muscle tissue oxygen extraction
(deoxygenated hemoglobin; [HHb]) and blood volume (total hemoglobin+myoglobin;
(Hbtot). To determine how stretching effects central cardiovascular parameters, heart rate
(HR) was measured using electrocardiography and finger photoplethysmography was
used to measure mean arterial pressure (MAP) simultaneous to peripheral cardiovascular
responses.

iv
During each stretching session a significant elevation in antegrade and retrograde
blood flow were observed, whereas MBF responses were not significantly altered
suggesting that skeletal muscle stretching in humans does not alter blood flow but can
cause a dramatic change in the biphasic nature of the blood flow responses. NIRS-
derived estimates of [HHb] and [Hbtot] were significantly increased, suggesting that
skeletal muscle stretching in humans increases muscle metabolism. Heart rate
significantly rose in a stretch intensity- and time-dependent manner, whereas blood
pressure was not significantly altered, suggesting a role for mechanoreceptive afferent
feedback arising from the musculature to initiate rapid adjustments in blood flow control.
After each stretching session a significant elevation in [Hbtot], MBF and
antegrade blood flow responses were observed in each stretching condition, suggesting
that stretching creates a post-stretch hyperemic response in humans. The retrograde
blood flow responses were significantly decreased following each stretching session and
these responses remained depressed at every time interval measured, suggesting that
stretching in humans creates a lower level of resting myogenic tone and reduced
downstream vascular resistance. These changes were also marked by significant
decreases in MAP in a muscle stretching-extent dependent manner suggesting that: 1)
skeletal muscle stretching in humans (afterward) mediates a baroreflex that serves to
adjust central (HR and BP) parameters back to normal and 2) the magnitude of the stretch
(i.e. higher intensity stretches) appear to dictate this response.
Collectively, the data acquired from this investigation has examined and verified a
critical role for skeletal muscle stretching and cardiovascular responses. Moreover, the
reductions in BP and retrograde blood flow seen after stretching suggests that skeletal

v
muscle stretching in humans reduces myogenic vascular tone which may confer
additional beneficial vascular effects in a post-stretch resting period. Alterations in
NIRS-derived microvascular parameters may reveal a causal role for this phenomenon
which serves to regulate how the upstream conduit artery blood flow profiles manifest.

vi
Table of Contents
Abstract .............................................................................................................................. iii
Table of Contents ............................................................................................................... vi
List of Tables .....................................................................................................................x
List of Figures .................................................................................................................... xi
1 Introduction ..........................................................................................................1
1.1 Stretching overview .....................................................................................2
1.2 Aims and hypotheses ...................................................................................4
2 Literature Review.....................................................................................................8
2.1 Foundational evidence in support for a role in muscle stretch-induced
alterations in energy turnover ..............................................................................................8
2.2 Microcapillary geometry and hemodynamics ............................................11
2.2.1 Muscle fiber stretch........................................................................12
2.3 Measures of near infrared spectroscopy (NIRS) and its implications
toward skeletal muscle stretching in humans.....................................................................14
2.4 Peripheral hemodynamics ..........................................................................17
2.4.1 Biomechanical hemodynamics of blood flow................................18
2.5 Regulation of muscle blood flow ...............................................................21
2.5.1 Local vascular control ....................................................................23
2.5.2 The baroreflex ................................................................................25
2.5.3 The exercise pressor reflex ............................................................29
2.5.4 The mechanoreflex.........................................................................30

vii
2.5.5 Contributions of the muscle mechanoreflex ..................................32
3 Effect of self-administered stretching on NIRS-measured oxygenation dynamics
……………………………………………………………………………………………39
3.1 Introduction ................................................................................................39
3.2 Methods......................................................................................................41
3.2.1 Subjects ..........................................................................................41
3.2.2 Study design ...................................................................................42
3.2.3 Stretch session ................................................................................43
3.2.4 Cycling session ..............................................................................44
3.2.5 Near infrared spectroscopy (NIRS) procedures .............................45
3.2.6 Maximal desaturation procedures ..................................................46
3.2.7 Myoelectrical activity (EMG) ........................................................46
3.2.8 Day-to-day reproducibility.............................................................47
3.2.9 Statistical analysis ..........................................................................47
3.3 Results ........................................................................................................48
3.3.1 Stretch ............................................................................................48
3.3.2 Comparison with cycling session...................................................49
3.4 Discussion ..................................................................................................53
4 Blood flow and oxygenation as a result of skeletal muscle stretching ..................58
4.1 Introduction ................................................................................................58
4.2 Methods......................................................................................................61
4.2.1 Experimental Overview .................................................................61
4.2.2 Subjects ..........................................................................................62

viii
4.2.3 Experimental procedures ...............................................................62
4.3 Muscle Stretching Sessions........................................................................64
4.3.1 Experimental session – CAS ..........................................................64
4.3.2 Experimental session – LIS ...........................................................64
4.3.3 Experimental session – CTS ..........................................................65
4.4 Macrovascular Peripheral Hemodynamic Measurements .........................65
4.4.1 Blood velocity ................................................................................65
4.4.2 Diameter and blood flow ...............................................................66
4.4.3 Shear indices ..................................................................................67
4.4.4 Vascular conductance ....................................................................67
4.5 Microvascular Hemodynamics ..................................................................67
4.5.1 Near Infrared Spectroscopy ...........................................................67
4.6 Central Hemodynamics Measurements .....................................................69
4.6.1 Blood pressure ...............................................................................69
4.6.2 Heart rate ........................................................................................70
4.7 Additional measurements...........................................................................70
4.7.1 Purpose ...........................................................................................70
4.7.2 Muscle activation ...........................................................................70
4.7.2 Breathing pattern ............................................................................71
4.7.3 Torque ............................................................................................72
4.8 Statistical analysis ......................................................................................72
4.9 Results ........................................................................................................72
4.9.1 General results ...............................................................................73

ix
4.9.2 Peripheral hemodynamics during and after stretching...................73
4.9.3 Microvascular hemodynamics during and after stretching ............74
4.9.4 Central hemodynamics during and after stretching .......................75
4.9.5 Passive resistive torque ..................................................................77
4.10 Discussion ..................................................................................................88
4.10.1 Peripheral hemodynamic responses during stretching ...................88
4.10.2 Peripheral hemodynamic responses after stretching ......................90
4.10.3 Microvascular blood volume responses during stretching .............94
4.10.4 Microvascular oxygenation responses during stretching ...............98
4.10.5 Microvascular blood volume responses after stretching ................99
4.10.6 Central hemodynamic responses during stretching. ....................100
4.10.7 Central hemodynamic responses after stretching ........................102
4.10.8 Limitations ...................................................................................104
4.11 Conclusions ..............................................................................................105
5 General conclusions, implications and future directions .....................................107
5.1 Future research directions ........................................................................109
5.2 References ................................................................................................111
A The Heading to Appendix A ................................................................................126

x
List of Tables
4.1 Peripheral biomechanical hemodynamics during stretching .................................78
4.2 Peripheral biomechanical hemodynamics after stretching ....................................79
4.3 Central hemodynamic responses during stretching ...............................................80
4.4 Central hemodynamic responses after stretching ..................................................81

xi
List of Figures
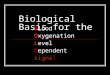
2-1 Capillary arrangement within the framework of skeletal muscle ..........................36
2-2 Blood flow responses at the onset of moderate intensity cycling exercise ............37
2-3 Arterial baroreflex modulation ..............................................................................38
3-1 Muscle deoxygenation changes during a self-administered stretch .......................50
3-2 Muscle deoxygenation comparisons between cycling and stretching ...................51
3-3 Muscle blood volume response between cycling versus stretching.......................52
4-1 Experimental protocol representing three different intensities across time ...........82
4-2 Graph representing CAS versus CTS across time .................................................83
4-3 Popliteal artery blood flow response during stretching .........................................84
4-4 Mean blood flow responses during and after stretching ........................................85
4-5 Microvascular blood volume responses during after stretching ............................86
4-6 Microvascular muscle deoxygenation response during stretching ........................87

1
Chapter 1
Introduction
The intent of this section of the dissertation is to summarize an understanding and
justification of the dissertation studies reported herein, including its aims and structure;
followed by an extensive overview of the interrelationship between the experimental
studies (Chapter 2). The review of literature will therefore, provide a comprehensive
understanding into studies pertaining to the all-encompassing title of this dissertation
entitled: “Blood flow and oxygenation dynamics as a result of human skeletal muscle
stretching.”
To date there is very little human empirical evidence to support the role of
skeletal muscle length dependent alterations in blood flow and the mechanisms that may
regulate these changes. Previous studies have suggested that a relationship exists
between muscle length and both blood flow and vascular conductance (Poole et al., 1997;
Welsh and Segal, 1996; McDaniel et al., 2012), which is likely regulated by the more
commonly documented mechanisms such as: cardiac output modulated by muscle
mechanoreceptor and chemoreceptor afferent feedback (Adreani et al., 1997; Adreani and
Kaufman; 1998; Herr et al., 1999), sympathetic nerve activity (Buckwalter et al., 1997;
Welsh and Segal, 1996), blood flow-induced vasoactive substances and metabolites

2
(Kooijman et al., 2008; Pohl et al., 1986). However, in addition to the more commonly
purported factors, skeletal muscle length-dependent changes in the tortuosity of the
capillary network may also influence blood flow and vascular conductance (Poole et al.,
1997; Segal, 2000), which may subsequently increase microvascular resistance. This
increase in downstream microvascular resistance may also have an impact on the
upstream conduit artery blood flow responses. As such, therein lies an undeniable and
inherent need for a clear interpretation of certain cardiovascular effects as a result of a
specific stretching treatment in humans.
1.1 Stretching overview, implications, structure and justification
Over the last two decades the stretching literature has for the most part, focused
exclusively on the argument of whether stretching effects subsequent exercise
performance and on the identification of the potential mechanisms underpinning such
alterations. For example, recent systemic reviews have suggested that static stretching
prior to a variety of muscular efforts could impair performance (Behm and Chauaouchi,
2011; Kay and Blazevich, 2012; Kallerud and Gleeson, 2013, Simic et al., 2013), such as
maximal eccentric torque (Brandenburg, 2006), concentric torque (Cramer et al., 2005),
maximal strength (Bacurau et al., 2009), peak power output (Cramer et al., 2005), rate of
force development (Kruse et al., 2014), sprinting (Fletcher and Jones, 2004) and jumping
ability (Kruse et al., 2013; Robbins & Scheuermann, 2008); this response has been aptly
referred to as the stretch-induce force deficit (Fowles et al., 2000; Ryan et al., 2008). The
authors to these studies have hypothesized that such an effect may be the result of two
commonly purported mechanisms. The first hypothesis is a reduction in neuromuscular

3
activation (Avela et al., 2004; Cramer et al., 2005; Fowles et al., 2000), such as decreased
motor unit activation and sarcomere shortening velocity. The second hypothesis is the
involvement of a mechanical factor, such as an increase in musculotendinous unit
compliance (Cramer et al., 2007; Herda et al., 2010; Kay & Blazevich, 2008; Mizuno et
al., 2013). Despite the overwhelming propensity to examine neuromuscular and
mechanical related mechanisms associated with stretching, to date, very little research
has explicitly examined the impact of cardiovascular and metabolic responses to human
skeletal muscle stretching.
The basis for a role in cardiovascular and metabolic responses to skeletal muscle
stretching has primarily come from animal studies (Poole et al., 1997; Kindig et al; 1999;
Segal, 2001). However, the idea that a cardiovascular and/or metabolic component
involved in human skeletal muscle stretching has come from the recent work by McCully
(2010) and Nelson and colleagues (2011). Here, authors (Nelson et al., 2011) first
demonstrated that passive stretching for at least 20 min lowered blood glucose values in
individuals with Type 2 diabetes or those at risk for developing Type 2 diabetes. This
finding suggests that a metabolic and/or cardiovascular demand is placed on the skeletal
muscle during muscle stretch. Additionally, muscle stretch in the presence of isometric
muscle contraction appears to induce a significant reduction in muscle oxygenation
(McCully, 2010). Although presently speculative these presumptions need further
clarification. Further, if stretching does indeed cause some sort of metabolic or
cardiovascular perturbation in humans the implications of such findings could be quite
substantial.

4
More research is needed on the human cardiovascular and metabolic response to
stretching because: 1) stretching is a common mode of exercise used by a wide range of
populations ranging from sporting-to-rehabilitative, 2) stretching is considered a low
intensity form of exercise and therefore at risk populations, whose exercise capacity can
be diminished may benefit greatly from a stretching program, especially when exercise is
confined to a smaller muscle mass, and 3) stretching has been shown to augment blood
glucose uptake in at risk populations (Nelson et al., 2011) and therefore, understanding
the mechanisms responsible for muscle length-induced alterations in blood flow are a
critical barrier for the health and fitness practitioner when allocating an effective
stretching intervention.
1.2 Aims and Hypotheses
Purpose
The specific aims of this dissertation are the following:
1) To determine the direct effect that a single bout of skeletal muscle stretching
has on microvascular muscle oxygenation and blood volume dynamics both
during and after passive stretching of the plantar flexors using near infrared
spectroscopy (NIRS) (Study I).
2) To investigate whether different intensities of passive muscle stretch result in
alterations in peripheral hemodynamic responses at the macro- and
microvascular level using NIRS and Doppler ultrasonography (Study II).
Three different intensities of stretching were chosen to determine whether

5
blood flow and perfusion is altered in a stretch-intensity dependent fashion.
The stretching intensities included as part of Study II are as follows:
a. Four minutes of constant angle stretching (CAS) at a relative perceived
moderate intensity. This stretch will serve as the reference session to
the remaining two stretching intensity sessions.
b. Four minutes of constant angle stretching at a low intensity (LIS), as
defined by 80% of the angle found from the reference CAS session.
c. Four minutes of constant torque moderate intensity stretching (CTS) at
the identified angle found from the reference CAS session.
3) To partition the relative contributions of central hemodynamic responses (i.e.
heart rate and blood pressure) that influence blood flow and perfusion during
and after varying intensities of passive stretch.
Hypotheses
The specific hypotheses to this dissertation are the following:
1) That a single bout of stretching for 4 min of the plantar flexors will cause a
significant interaction in microvascular hemodynamics as measured using
NIRS between each stretching condition (CAS vs. LIS vs. CTS) across time
(15 s vs. 60 s vs. 150 s vs. 240 s) corresponding to:
a. A main effect for time such that there will be a significant decrease in
NIRS-derived blood volume across time.

6
b. A main effect for time such that there will be a significant increase in the
relative changes in NIRS-derived muscle deoxygenation patterns over
time.
2) By altering the intensity of a passive stretch on the plantar flexors this will
elicit a significant interaction for popliteal artery conduit blood flow
parameters between conditions (CAS vs. LIS vs. CTS) and across time (15 s
vs. 60 s vs. 150 s vs. 240 s) corresponding to:
a. A main effect for time such that there will be a significant increase in
antegrade and retrograde blood flow and shear rate at each specific time
point.
b. A main effect for condition such that there will be significant changes in
mean blood flow, antegrade and retrograde blood flow and shear rate in an
intensity dependent fashion (CTS > CAS > LIS conditions)
3) By altering the intensity of a passive stretch on the plantar flexors this will
elicit a significant interaction in central hemodynamic parameters of heart rate
and blood pressure between each condition across time point corresponding
to:
a. A main effect for time such that there will be a significant increase in heart
rate and blood pressure at each specific time point
b. A main effect for condition such that there will be a significant change in
HR and BP between each condition in an intensity dependent fashion
(CTS > CAS > LIS)

7
4) A significant increase in blood flow (post-stretch hyperemia) and shear rate
will occur immediately (first 15 s) following stretching:
a. The increase in blood flow after stretching will be the result of significant
increase in antegrade blood flow across each stretching condition.
b. Mean blood flow, shear and vascular conductance will be significantly
increased after stretching in a stretching intensity dependent fashion (CTS
> CAS > LIS).
5) Blood pressure will be significantly decreased after stretching due to:
a. Increased vascular conductance and increase microvascular vasodilation.
6) There will be no significant interaction between stretching conditions across
time for heart rate.

8
Chapter 2
Literature Review
2.1 Foundational evidence in support for a role in muscle stretch-induced
alterations in energy turnover
Conceptually, most people, and perhaps even many physiologist for that matter,
would consider skeletal muscle stretching to be a passive maneuver, whereby the energy
expenditure within the musculature remains unchanged from rest. This notion would
seemingly appear logical from the simple perspective of watching an individual undergo
a passive static stretching maneuver; the task does not look particularly daunting and
perceptually, the individual feels that little effort has been expended. Nevertheless,
research as early as 1932 (Euler and Feng, 1932), has suggested that skeletal muscle
stretching does indeed cause a significant rise in metabolic rate. Thus, the following
paragraphs in this section will argue in favor of the hypothesis that stretching creates
some level of metabolic disturbance.
Early studies applying stretch to animal muscle preparations have shown that
skeletal muscle stretching causes a transient rise in muscle heat production, a direct
measure of energy expenditure or metabolic rate (Ernst, 1963; Euler and Feng, 1932);
this response has since become to be known as the “Feng effect.” Ling and Gerard

9
(1949) determined that the stretch-induced increase in metabolic rate reflects the
additional energy turnover needed to maintain the resting membrane potential at greater
muscle lengths. Harris (1954) further suggested that this effect of stretching was caused
by an increase in the activity of the sodium pump, and that this may have altered the
mechanical efficiency of the myocyte. From these observations it was hypothesized that
if such responses were evident, then an increase in the rate of heat production relative to
muscle length would be increased in a linear fashion. Accordingly, Clinch (1968)
measured the relationship between muscle length and rate of heat production in an
isolated frog sartorious muscle preparation (stretch response). This research model
involved progressively stretching the muscles greater than the resting length, whereby
after each stretch the new length was maintained for 60 s before the muscle was released
back to its resting length. Here, it was found that as muscle preparations were stretched
beyond their physiological lengths there was an appreciable increase in the rate of heat
production, often approaching 3-4 times the basal metabolic rate. These findings are in
agreement with Hill’s previous notion (1952), where he determined that the length at
which the increase in the rate of heat production first occurs approximates the length at
which an element showing normal thermoelasticity (i.e. the coupling between the elastic
field in the structure caused by deformation and the temperature field) first manifests
itself in the passively stretched Sartorius; this element was theorized to derive from the
sarcolemma. Podolsky (1964) then demonstrated that tension (i.e. stretch) becomes
evident at the sarcomere level when sarcomere lengths reached 3.2 μm, and that above
this supposed physiological threshold much of the resting tension arises from the
sarcolemma.

10
The next question that arises is how does how does stretching the muscle lead to
changes in the sarcolemma that result in an appreciable increase in the metabolic rate?
Clinch (1968) theorized that a change in surface energy, or a disorientation of fixed
changes in the membrane might result in a more loose binding of substances, such as
calcium, which is involved in the excitation-contraction coupling process. Furthermore,
it was hypothesized that if stretch were to bring about activation of adenosine
triphosphate (ATP) and active tension development similar to that seen in insect flight
muscle (Jewell & Ruegg, 1966), then the stretch response would be explained as the
metabolic turnover caused by the increased rate of ATP-splitting and its associated
metabolic by product. In support of these theories more recent evidence has provided a
more direct line of evidence where authors have determined further that passively
stretching isolated muscle preparations increases O2 consumption (Barnes, 1987), carbon
dioxide production, glycogen breakdown (Barnes and Worrell, 1985) and lactic acid
production (Barnes, 1987), and decreases phosphocreatine (PCr) concentration (Barnes,
1987).
In summary, the accumulation of early evidence at least with regard to animal
preparations, clearly support the contention that muscle stretch induces an appreciable
increase in metabolic rate. It is therefore possible that, through such metabolic
disturbances, cardiovascular responses are manifested. The following sections will
explore the cardiovascular implications of skeletal muscle stretch within the
microvasculature, with an extended discussion of its implication on microvascular
architecture.

11
2.2 Microcapillary geometry and hemodynamics
The capillary bed is arranged both vertically and horizontally (Figure 2.1) within
skeletal muscle as a complex arrangement of vessels among the connective tissue matrix.
Functionally, this may be represented as a vast “mesh-like" surface of blood vessels that
facilitates blood-tissue exchange of O2, substrates and metabolic by-products as well as
hormones and other bioactive/signaling molecules (Poole et al. 2013). Most of the
capillaries, in situ, are continuously under longitudinal stretch (Learoyd and Taylor,
1966) by tethering to the adjacent connective tissues (i.e. connexin) of the surrounding
myocytes, a property which prevents individual capillaries from collapse. In the event of
sarcomere movement (muscle contraction or muscle lengthening) (Borg & Caulfield,
1980), this will create a kinetic sequence of events moving outward such that the
capillary extension reserve will be altered. This unique characteristic that causes
capillaries to change their architectural arrangement is called tortuosity (Poole et al.,
1989) (Figure 2.1). Unlike conventional wisdom where it is presumed that capillaries are
straight unbranched structures, the work by Poole and others (Mathieu-Costello et al.
1989; Poole et al. 1989) have developed the current perspective that capillaries exhibit
considerable tortuosity (i.e. curving and bending) that changes dynamically as a function
of muscle sarcomere length.
In general, tortuosity is a property of a curve, defined by how twisted it is and
how many turns and bends it has. Tortuosity in the context of capillaries is a
physiological index of the capillary extension reserve, because this mesh-like
arrangement undergoes conformational changes during dynamic muscular movements.
To this end, concentric muscular actions will shorten muscle fibers, causing more

12
twisting and crimping thus, adding to the capillary tortuosity. On the other hand, muscle
lengthening, either by stretching or eccentric muscular contractions, will have the reverse
effect, by elongating capillaries and decreasing tortuosity (Poole et al., 1997). For
purposes of this dissertation, the remaining arguments will be briefly discussed in relation
to muscle lengthening responses, where very little empirical evidence exists in support of
this phenomenon. The next section will therefore discuss dynamic modifications to the
microvasculature within skeletal muscle with careful attention on how stretch impacts
vascular resistance and blood flow dynamics.
2.2.1 Microcapillary geometry and hemodynamics: Muscle fiber stretch. It has been
shown that the lengthening of a muscle using an isolated exteriorized preparation can
significantly alter muscle blood flow at rest (Supinksi et al., 1986; Poole et al., 1997) and
during exercise (Supinski et al., 1986) and that capillary tortuosity (Poole et al., 1997;
Kindig et al; 1999; Segal, 2001) intramuscular pressure (IMP) (Ameredes and
Provenzano, 1997; Kirkebo and Wisnes, 1982) and/or muscle sympathetic nervous
system activity (MSNA) (Welsh and Segal, 1997) can greatly contribute to the regulation
of microvascular blood flow. With regard to muscle stretch, capillaries can display a
substantial variability in length (20-1000 µm) and diameter (~2-8 µm; Mathieu-Costello
et al. 1989; Poole et al. 1989; Nakao and Segal, 1995), a phenomenon which may greatly
change depending on the extent of muscle function. Generally movements that are
defined within a physiological range, that is, within the length that sarcomere binding is
evident in animal preparations, have been shown not to significantly alter blood flow/red
blood flow (RBC) flux through a capillary (Poole et al., 1997; Kindig et al; 1999; Segal,

13
2001). Interestingly, capillary diameter and muscle blood flow do not change in a linear
manner instead; a threshold in the blood flow response initiated by muscle lengthening
becomes evident (Poole et al., 1997). This example has been described by Poole et al.
(1997), where it was demonstrated that the capillary lumen of the rat spinotrapezius
muscle decreased moderately up to sarcomere lengths of ~ 2.9 um, but further
lengthening of the muscle fibers beyond physiological lengths resulted in a steep decline
in luminal diameter resulting in reduced blood flow as great as 40 %. The authors
suggested that as a muscle is extended beyond the physiological range, the physical
lengthening of fibers results in stretching and compression within the vasculature, thereby
altering capillary length, diameter and RBC distribution. It was further suggested that a
moderate increase in sarcomere lengths (up to 2.9 um) may not influence muscle
perfusion, because it reduced capillary tortuosity. Further supporting evidence has shown
that the vessels running parallel to the muscle fibers become longitudinally extended in a
muscle stretching dependent manner (Nakao and Segal., 1995; Poole et al., 1997; Poole
and Mathieu-Costello, 1992) which results in an overall reduction in diameter of that
vessel.
Another plausible explanation for the decrease in microvascular blood flow is that
IMP becomes increased to such an extent that some or all of the blood flow can be
significantly impeded either at the venous and/or arterial level (Ameredes and
Provenzano, 1997; Kirkebo and Wisnes, 1982). Other mechanistic evidence for the
reduction of blood flow during muscle stretch may be attributed to an increased
sympathetic nerve activity initiated by the muscle lengthening (Welsh & Segal, 1997).
Welsh and Segal (1997) concluded that the increase in vascular resistance with muscle

14
lengthening arises primarily from the activation of perivascular sympathetic nerves,
resulting in norepinephrine release and vasoconstriction that is local in nature suggesting
that factors other than muscular pressure and vessel lengthening result in the narrowing
of the vessels. Collectively, these physical and neural alterations increase vascular
resistance, which subsequently disrupts how red blood cells are distributed throughout the
capillary network. Ultimately, these responses decrease muscle blood flow and
oxygenation.
In summary, based on the results of previous animal studies, the dynamic action
of muscle stretching appears to distort the arrangement of capillaries within skeletal
muscle. This alteration reduces vascular conductance and RBC distribution. Further,
these muscle length-dependent alterations in RBC-myocyte flux have formed the
foundation for human experimental research, which until recently, has received very little
attention. Thus, it is likely that when humans stretch their muscles, the initial decrease in
tortuosity increases vascular resistance and reduces blood flow. How this response is
manifested appears to depend on a variety of neural and mechanical mechanisms which,
at present, have not been identified. The next sections, therefore, will discuss indirect
human empirical evidence that support a role for muscle stretch-induced alterations in
muscle blood flow and oxygenation.
2.3 Measures of near infrared spectroscopy (NIRS) and its implications toward
skeletal muscle stretching in humans.
A modicum of human evidence has shed light into muscle length-dependent
changes in cardiovascular and metabolic perturbations involved with stretching. The

15
development of near infrared spectroscopy (NIRS) over twenty years ago has enabled
researchers to delve into the non-invasive assessment of skeletal muscle oxygenation
status as well as blood volume within the microvasculature over a range of muscular
movements. For instance, Miura and colleagues (2004) found that regional differences
between the distal end and proximal end of gastrocnemius medialis (GM) and vastus
lateralis during isometric contractions amount to noticeably different markers of blood
volume and oxygenation as determined by NIRS. Additionally, McCully (2010) found
that when skeletal muscle was passively stretched in combination with intermittent
isometric contractions of the distal ends of gastrocnemius medialis and vastus lateralis
muscle groups, a corresponding reduction in muscle oxygenation was observed, which
often approached levels comparable to complete muscle ischemia. These results
however, were not evident when the NIRS sensor was placed over the proximal portion
of these same muscle groups, thus adding to previous knowledge that a dynamic
heterogeneity exists with regard to muscle oxygenation dynamics in humans and that
such changes appear greatly to depend on the extent of muscle function and muscle
length. Otsuki and colleagues (2011) provided additional support, as these authors
demonstrated that individuals with extensive stretch training (i.e. ballet trained dancers)
could extend their muscles (tibialis anterior) without excessive reductions in muscle-
blood volume and muscle oxygenation (derived from the NIRS signal) at the same
relative but at an absolute greater muscle-stretching level than a control group. The
conflicting finding between McCully’s (2010) investigation and Otsuki et al (2011) is
likely due to several notable factors. The first is that McCully’s investigation
incorporated intermittent contractions to the stretch protocol. Thus, the extent that the

16
muscle contractions contributed to the decrease in muscle oxygenation versus the change
in muscle length during the intense passive stretch of the plantar flexors is not known.
Indeed, isometric contractions as low as 25 % and 35 % of an individual’s maximal
voluntary contraction (MVC) have been reported to cause marked reductions in NIRS-
derived measures of blood volume and oxygenation within skeletal muscle tissue
(DeRuiter et al., 2007), possibly as a result of increased IMP (Poole et al., 1997).
Another factor that may have resulted in the conflicting findings is the fact that the
tibialis anterior muscle used in Otsuki et al’s (2011) study is not considered a highly
pennated muscle in comparison to gastrocnemius muscle from the previous study
(McCully, 2010). This notion is supported by the well-known fact that IMP is greatest in
muscle demonstrating the highest degree of curvature (i.e. pennation) than longer slender
muscles (i.e. tibialis anterior) (Sejerstad et al., 1984; Naamani et al., 1995; Muramatsu et
al., 2002). Accordingly, the increase in IMP was likely greater during passive muscle
stretch in McCully’s investigation because of a higher degree of pennation, which may
have created a greater shift in blood volume subsequent to an overall reduction in muscle
oxygenation.
In conclusion, these findings in humans coupled with previous animal evidence
suggest that skeletal muscle stretching can cause a dramatic microcirculatory response
capable of altering blood flow and the relationship between O2 availability and O2
utilization. Therefore, if microvascular oxygenation dynamics and blood volume are
altered in a muscle-length dependent manner in humans, it is plausible to assume that a
large hydrostatic gradient becomes evident between the microvasculature and larger
upstream feed conduit arteries such that vascular conductance and blood flow is altered

17
within this specific vasculature. The next sections will address basic hemodynamic
parameters of the conduit arterial system and how such modifications may lead to
alterations in blood flow.
2.4 Peripheral hemodynamics
The velocity of flow through a large conduit artery can be reliably assessed using
Doppler ultrasonography and is calculated based on the principle of propagation of
ultrasound waves directed into the tissue which are reflected by the erythrocytes passing
through the vessel (Gill, 1979). To this extent, Doppler ultrasound allows for continuous
imaging of the artery and the red blood cells travelling through it in combination with
either a pulsed or continuous wave Doppler velocity signal. The underlying principle of
the Doppler ultrasound technique is that a frequency shift occurs when a sound beam is
reflected from a moving source (i.e. erythrocytes) back to the probe. The probe then
interprets the temporal responses from the Doppler frequency waves, which are then
interpreted as antegrade (forward direction) and retrograde (backward direction) blood
velocity oscillations on the computer screen. The combination of vessel diameter and
mean blood velocity profiles enable the researcher to directly determine muscle blood
flow and shear stress responses within the conduit artery. Blood flow therefore, can be
calculated by multiplying mean blood velocity (cm·s−1
) by the cross-sectional area of the
artery (cm2) then multiplying by 60 to represent values as milliliters per minute
(ml·min−1
). To account for the physical stimulus placed on the endothelium, shear rate
can also be calculated using the following equation: shear rate (s–1
) = (4 x mean blood
flow)/πr3 (Silber et al. 2005), where r represents the radius of the vessel. Since these

18
measurements are greatly dictated by several biomechanical hemodynamic variables
within the conduit arterial system, the next section will provide for a basic understanding
of these principles and their overall importance to blood flow regulation and control.
2.4.1 Peripheral hemodynamics: Biomechanical hemodynamics of blood flow
regulation. Blood flow traveling throughout the circulatory tree is dictated by several
important biomechanical and hydraulic factors. These biomechanical stimuli directly
affect the luminal endothelium which, in return, directly impact vascular function. There
are three primary biomechanical stimuli that the vascular endothelium is exposed to:
shear stress, identified as the drag frictional force generated by blood flowing through the
vessel; circumferential stretch, highlighted as the pulsatile blood flow acting against the
vessel walls in all direction; and hydrostatic pressure gradient, which is the compressive
forces generated during cardiac cycles (Davies, 1995). In this regard, the basic hydraulic
principles that influence hemodynamics should be addressed.
Hemodynamics can be defined as the science of the relationship between blood
flow, pressure, and hydraulic resistance. The rate of blood flow through a cylindrical
tube is determined by a pressure gradient as defined by the pressure drop over a given
length (ΔP/Δℓ). Typically length (Δℓ) does not change whereas pressure (ΔP) undergoes
the largest changes. A prime example of a significant pressure gradient in the arterial tree
is across the arterioles, where a precipitous fall in pressure can occur by as much a 40
mmHg. This rapid fall in pressure across the arterioles demonstrates that this is the major
site of resistance in the vascular tree. Vascular resistance (R), or the impedance of blood
flow therefore, can be expressed as the relationship between the blood pressure gradient

19
(P1-P2) and blood flow, R = (P1-P2)/Q. On the other hand the relative ease of blood flow
through a vessel is termed vascular conductance (VC), where the variables of the previous
equation can be switched to be represented in the equation:
VC = Q/MAP
where MAP is mean arterial pressure, which represents the average pressures on both the
arterial and venous side of systemic circulation.
If the length of a vessel is assumed to be constant, the pressure gradient between
two points in the circulatory system becomes the primary factor influencing blood flow
control. Accordingly, Darcy’s law states that steady state flow (Q), is linearly related to
the pressure difference between two points in a tube, as highlighted in the equation
below:
Q = K(P1 – P2) = (P1 – P2)/ R
where K is the hydraulic conductance between two points, R is hydraulic resistance, and
P1-P2 is the difference in pressures between two points. This equation can then be
applied to a practical human model of circulation, which is highlighted as:
Q = (MAP – CVP)/ TPR

20
where, Q represents cardiac output, CVP is central venous pressure, and TPR is the total
peripheral resistance. Because Darcy’s equation only addresses one of the three
fundamental forms of mechanical energy (pressure) additional information must be
addressed in order to fully represent the precise hemodynamic changes of the circulatory
system. Daniel Bernoulli addressed some of these issues, as he was further able to
describe the forces in a moving fluid; Bernoulli’s principle states, that the flow between
two points (A and B) in a steady state is proportional to the difference in the mechanical
energy of the fluid between those two points. The Bernoulli principle therefore, is able to
calculate that the mechanical energy is the summation of pressure energy, potential
energy, and kinetic energy which is highlighted by the equation:
ME = P + ρgh + v2/2
where ME is the mechanical energy, P is the pressure energy, (acceleration/deceleration
of fluid), ρgh is the gravitational potential energy (ρ is the density of the fluid, g is the
gravitational acceleration = 9.8 m·s-2
). Bernoulli’s principle however, only applies to
steady state laminar flow, which is opposed to the pulsatile flow that occurs as a series of
fluid-like layers in human circulation. Laminar flow thus, only applies to the molecules
(i.e. erythrocytes) immediately adjacent to the vessel wall, which move at a slower rate
than those in the middle. This movement creates multiple layers, termed lamina, which
create a parabolic velocity profile where velocity (v) is equal to one-half the maximum
velocity at the center of the vessel. Further, the sliding motion of one lamina over
another may be termed shear, which leaves a thin layer of plasma next to the vessel wall

21
called the marginal layer; this motion is functionally important in augmenting blood flow
through the conduit arteries. The velocity of one lamina sliding past another lamina is
termed shear rate (s-1
) and produces a mechanical stimulus called shear stress (τ, N·m-2
).
In this context shear force acts to accelerate and decelerate the lamina generating a
pulsatile blood flow profile (Davies, 1995). Additionally, because blood viscosity, for
the most part, behaves as a Newtonian fluid in the human body where the blood viscosity
in larger conduit arteries generally remain constant, coinciding with the fact that the
length of the vessel does not change, it becomes apparent that the control of blood flow is
primarily dictated by pressure and resistance, as described by the Poiseuille’s equation.
Jean Leonard Marie Poiseuille was a 19th
century French physician who discovered that
flow through a tube is directly proportional with the differences in pressure and to the
fourth power of the tube radius, while the length and fluid viscosity is inversely
proportional as highlighted by the equation:
Q = ∆Pπr4/8ℓη
where Q is flow rate (cm3/sec), ∆P is the difference in pressure between two vessels
(dynes/cm2), r is the radius of the tube (cm), ℓ is the length of the tube (cm), and η is the
viscosity of the fluid in poise (dyne sec/cm2). This equation has formed the foundation
for the basis of biomechanical hemodynamic principles of blood flow regulation for over
100 years.
2.5 Regulation of muscle blood flow

22
As previously stated in prior sections of this literature review, muscle stretch
appears to initiate a sympathetic mediated response which is controlled via modulation of
the autonomic nervous system. Therefore, a muscle length induced autonomic nervous
system response is partially responsible for central cardiovascular control of blood flow.
Indeed, it is well understood that autonomic modulation of the cardiovascular system,
during transitional exercise functions to closely match the delivery of blood flow (and
oxygen) to meet the metabolic demands of the working muscle (Murphy et al., 2011).
Some of the potential mechanisms that occur early on in the transition period from rest-to
steady state exercise include central command, the exercise pressor reflex (EPR),
metabolic control (i.e. functional sympatholysis), and the muscle pump (Boushel, 2003;
Delp & Laughlin, 1998; Saltin et al., 1998).
The initial rapid increase in muscle blood flow, also named the phase I response,
occurs approximately within 10 s of initiation of exercise, whereas phase II, occurs more
slowly, with an exponential increase towards a new steady state if the intensity of
exercise is in the moderate intensity domain (Shoemaker & Hughson, 1999; Rådegran &
Saltin, 1998) (Figure 2.2). One confounding issue to the initial rapid increase in blood
flow (phase I) is whether this is due to a feed-forward mechanism through inherent
mechanical changes to the vasculature (i.e. the muscle pump), local vascular control or by
autonomic feedback mechanisms such as the mechanoreflex and metaboreflex. Despite
the muscle pump offering a reasonable explanation towards the initial rise in blood flow
at the onset of exercise, direct evidence for this action in humans is lacking since the
required instrumentation needed to measure this effect would disrupt the internal
structure of the vessels (Laughlin & Schrage, 1999; Tschakovsky, 2004; Tschakovsky et

23
al., 2004). Furthermore, the metaboreflex cannot account for the rapid rise in blood flow,
because this response is delayed (at least ~ 20 s), and therefore is believed to be the
primary control mechanism during the secondary phase (phase II) of blood flow (Skinner,
Jr. & Powell, Jr., 1967; Skinner, Jr. & Costin, 1970; Haddy & Scott, 1968; Proctor &
Duling, 1982). Therefore, local vascular control mechanisms or an exercise pressor
reflex-induced response dominated by the mechanoreflex seems like a plausible
explanation for the initial rise in blood flow at the onset of exercise. The following
sections will highlight a basic understanding toward local vascular control mechanisms
and the EPR.
2.5.1 Regulation of blood flow: Local vascular control. The adaptions of blood flow
during the rest to work transition represent an ongoing and major challenge to
homeostasis (Shoemaker and Hughson, 1996). In general increased blood flow, and
hence O2 delivery to the muscle will increase in proportion to work and metabolic
demand placed by that muscle. This term that is referred to as active hyperemia. One
prominent feature of active hyperemia is that dramatic increases in vascular conductance
(i.e., decreased vascular resistance) are mediated by relaxation of vascular smooth muscle
in resistance arteries and arterioles supplying the skeletal muscle (Armstrong et al., 1987;
Rowell, 1993). In recent years, investigations have demonstrated in humans (Rogers et
al., 2006; Saunders and Tschakovsky, 2004; Tschakovsky et al., 2004) and in animal
models (Hamann et al., 2004; VanTeeffelen and Segal, 2006) that the resistance vessels
can dilate immediately after the first contraction at exercise onset. The mechanisms
responsible for rapid vasodilation are presently unclear but a few notable mechanisms

24
may be responsible. Firstly, Van Teefelen and Segal (2006) presented evidence for
acetylcholine-mediated spillover from motor end plates as the mechanism for rapid
vasodilation at the onset of contraction however; other investigators have presented
evidence that opposes this (Dyke et al., 1998; Naik et al., 1999). Tschakovsky and
colleagues (2004) have proposed that mechanical distortion of resistance vessels with
contraction directly affect smooth muscle tone, which may reflect a myogenic reflex with
decreased transmural pressure during contraction (Mohrman and Sparks, 1974). Clifford
et al (2006) also confirmed a mechanical distortion effect in isolated vessels and further
proposed that an intact endothelium is needed to elicit this response. To this end,
Hamman et al (2004) have suggested endothelial release of vasodilator substances occurs
with cell distortion. Furthermore, these responses are not just activated at the immediate
onset of muscle contraction but also with further increases in contraction intensity
(Saunders and Tschakovsky, 2004) as well as contraction velocity (Rogers et al., 2006).
This active hyperemic response is well maintained, at least when using a human forearm
exercise model.
As exercise continues beyond 7-10s, and if the exercise is above the ventilatory
threshold, byproducts of anaerobic metabolism accumulate in exercising skeletal muscle
and blunts the normal ability of sympathetic nerves to cause vasoconstriction, a
phenomenon termed ‘functional sympatholysis’ (Remensnyder et al., 1962; Buckwalter
& Clifford, 2001). Several factors are purported to potentially contribute to the
attenuated vasoconstrictor effects to sympathetic activation during exercise which include
the following: α-adrenergic receptor subtype (Anderson & Faber, 1991; Buckwalter et al.
2001; Wray et al. 2004), nitric oxide (Thomas & Victor, 1998; Dinenno & Joyner, 2003),

25
prostaglandins (Crecelius et al. 2011; Markwald et al. 2011), ATP (Kirby et al. 2008;
Crecelius et al. 2011) and ATPsensitive K+ channels (Thomas et al. 1997; Keller et al.
2004). Functional sympatholysis also appear to be affected by muscle fiber type such
that the response may preferentially occur largely in glycolytic type II motor units as
compared to oxidative type I motor units (Thomas et al. 1994; Horiuchi et al., 2012). In
the only human study to address whether muscle fiber type differences contribute to
functional sympatholysis, Horiuchi et al (2014) examined NIRS-derived oxygenation
over the triceps surae muscle groups across varying levels of exercise intensity. The
authors measured simultaneous muscle oxygenation responses by placing near infrared
sensors over gastrocnemius medialis (higher proportion of type II muscle fibers) and
soleus muscles (higher proportion of type I muscle fibers) during acute sympatho-
excitation testing, which involved the cold pressor test. Collectively, the authors found
that muscle groups composed mainly of glycolytic type II fibers (gastrocnemius medialis
muscle) are more sensitive to functional sympatholysis, particularly at lower intensities of
exercise. These findings lend further insight into the dependence of local blood flow
redistribution on the recruitment patterns of muscle fiber type as well as exercise
intensity (Laughlin and Armstrong, 1982; Kouzak et al., 2003).
2.5.2 Regulation of muscle blood flow: The baroreflex. During the transition from rest
to exercise or during incremental increases in work intensity, arterial baroreceptors
originating in the carotid arteries and aorta play a pivotal role in the rapid reflex
adjustments of blood pressure and heart rate, which ultimately regulate blood flow
(Fadel, 2008; Joyner, 2006). The carotid and aortic baroreflexes consist of

26
unencapsulated free nerve endings located at the medial–adventitial border of arteries in
the carotid sinus bifurcation and aortic arch (Fadel, 2008, Sheehan et al., 1941). These
mechanoreceptors function on a negative feedback control system such that when arterial
blood pressure (BP) becomes elevated, the baroreceptors are stretched, and this
deformation causes an increase in afferent neuronal firing that result in a reflex-mediated
increase in parasympathetic nerve activity and decrease in sympathetic nerve activity.
On the other hand, if arterial BP becomes suddenly decreased, little stretch is imposed on
the baroreceptors. This results in a decrease in afferent firing on the baroreceptors,
resulting in a decrease in parasympathetic nerve activity and an increase in sympathetic
nerve activity (Fadel, 2008). Collectively, these neural feedback adjustments in
baroreceptor function have a profound impact on heart rate (HR) and vascular tone in an
effort to maintain or return MAP to its normal value (Figure 2.3).
To assess contributions of the baroreflex to hypertensive and hypotensive stimuli,
many studies incorporate the variable pressure neck chamber using either neck suction or
neck pressure as a means to assess the magnitude of this response (Figure 2.3). The
appealing aspect of this procedure is that: 1) it is non-invasive, 2) is non-pharmacologic,
3) the rate, timing and duration of the pressure stimulus can be precisely controlled, and
4) it can be applied under a variety of experimental conditions (Fadel, 2008). The neck
chamber functions to alter the transmural pressure acting on the carotid sinus, thereby
altering parasympathetic or sympathetic nervous system tone, depending on the nature of
the stimulus. For example an increase in pressure within the neck chamber causes a
decrease in carotid sinus transmural pressure. This compresses the carotid baroreceptors,
which then exposes them to a hypotensive stimulus thereby evoking reflex-mediated

27
increases in heart rate and blood pressure. Conversely, neck suction stimulates the
carotid baroreceptors and administers a hypertensive condition which creates a reflex-
mediated decrease in heart rate and blood pressure.
The first convincing evidence showing the importance of vascular responses to
the arterial baroreflex control of blood pressure at rest came from the work of Ernsting
and Parry (1957) who used the application of neck suction to stimulate the carotid
baroreceptors. Later on, Bevegard and Shepherd (1966), using the variable pressure neck
chamber, became the first to observe in man a preserved baroreflex control during
exercise. These authors demonstrated a clear contribution to the understanding that
alterations in vascular resistance control baroreceptor-mediated changes in blood
pressure. Potts et al (1993) then became the first authors to directly assess in humans,
that the baroreflex is reset during exercise to functionally operate around the prevailing
BP elicited by the exercise workload. This resetting of the baroreceptors has also been
confirmed by several other recent investigations (Norton et al., 1999; Ogoh et al., 2003;
Papelier et al., 1994).
Baroreceptors can respond to alterations in mean arterial pressure (MAP) by
affecting three primary physiological variables as highlighted in the equation:
MAP = (HR x SV)/TVC
where MAP is mean arterial pressure, HR is heart rate, SV is stroke volume and TVC is
total vascular conductance. When partitioning which physiological variables are
important in baroreflex-mediated changes in MAP, current evidence has purported a role

28
for HR and TVC as being the primary means by which the carotid baroreceptors respond
to acute changes in carotid sinus transumural pressure (Ogoh et al., 2002). However,
because the baroreflex transiently occurs on a beat-by-beat basis, HR has been shown to
be modulated early in the baroreflex (i.e. first 3-4s) after neck suction or neck pressure,
and this response appears to be related to changes in cardiac vagal tone derived from
parasympathetic modulation (Fadel et al., 2003; Keller et al., 2004; Ogoh et al., 2003;
Potts et al., 1993). Furthermore, TVC appears to be important at a later time interval
during neck suction or neck pressure (4-10 s), as MAP become elevated. Specifically,
peak changes in HR appear to be solely responsible (SV is unaltered) for the initial
reflex-mediated changes in MAP (i.e. 3-4 s) when MAP only changes minimally (i.e. 2-3
mmHg) however; alterations in TVC predominate over the HR changes in cardiac output
at a later time point (4-10 s) because MAP changes more dramatically (10-15 mmHg)
than HR mediated-responses. Therefore, it can be concluded that the capacity of the
carotid baroreceptors to regulate MAP depends critically on their ability to alter TVC
both at rest and during exercise (Fadel, 2008).
In summary, the baroreflex is a neural feedback mechanism that is reset to a
higher or lower operating point around the prevailing alterations in BP during transitions
from rest-to-exercise, and serves to regulate blood flow through changes in central and/or
peripheral hemodynamic parameters. Alterations in SV do not contribute primarily to the
maintenance of arterial blood pressure by the carotid baroreceptors, and therefore, any
reflex-induced changes in cardiac output must come from reflex-mediated changes in
HR. However, baroreflex changes in MAP are primarily dictated by changes in vascular
conductance at both rest and exercise. The two major neural mechanisms that are

29
primarily involved in regulating this response have been proposed to be as a result of
central command and the EPR (Rowell and O’Leary, 1990). As such the following
sections will focus exclusively on the EPR namely, mechanoreceptive afferents, as this is
one of the primary focal points of the dissertation studies reported herein.
2.5.3 Regulation of muscle blood flow: The exercise pressor reflex. The concept that a
neural reflex arising from contracting skeletal muscle capable of increasing ventilatory
and cardiovascular responses has come from the seminal work by Alam and Smirk
(1937). Here, the authors employed rhythmic calf muscle exercise simultaneous to
inflation cuffs wrapped around the thigh inflated to supra-systolic blood pressure to
occlude local systemic circulation. This occlusion was maintained after the exercise
protocol in order to trap metabolites produced during exercise within the active muscles.
It was reported that blood pressure increased during exercise and fell slightly at the end
of exercise but was maintained above resting levels for as long as occlusion was
sustained. Since blood pressure remained elevated at a time when no exercise was being
performed but local occlusion continued, it was concluded that a reflex originating from
the previously active muscles was maintaining the elevated blood pressure. It was argued
by these authors that this would serve to increase the blood supply to the muscles where
metabolic waste products were trapped but needed to be removed.
More recent support has come from experiments in which healthy humans were
given paralytic agents intravenously or paralyzed patients were asked to attempt exercise
(Freyschuss, 1970; Victor et al., 1989). These studies showed that when individuals
attempted to exercise during temporary paralysis, an evoked pressor and muscle

30
sympathetic efferent response were at best only 50% of those evoked by exercise when
subjects were not paralyzed. These results were interpreted with the assumption that
during paralysis the subjects’ ability to generate central command remained intact. Other
empirical evidence in support for the hypothesis that a muscle reflex contributes to the
cardiovascular response to exercise has come from experiments in which humans were
given epidural injections of lidocaine. The purpose of these experiments was to allow
muscles to exercise while sensory feedback from these muscles was attenuated via the
lidocaine. In these experiments, the pressor and cardioaccelerator responses to both static
and dynamic exercise were attenuated, and the post-exercise pressor response due to
circulatory occlusion ischemia was abolished (Fernandes et al., 1990; Freund et al., 1979;
Mitchell et al., 1989). Collectively, in these foundation studies, which observed a blunted
pressor and cardioaccelerator response during exercise, this has become known as the
exercise pressor reflex (EPR) (Iellamo et al., 1999; Drew et al., 2008; Gladwell et al.,
2005).
2.5.4 Regulation of muscle blood flow: The mechanoreflex. The EPR can be defined as
a sequence of cardiovascular responses evoked by contraction of skeletal muscle and
consists of increases in MAP, HR, and cyclical breathing (Mitchell et al., 1983). A
continuous neural feedback from working limb muscles is well-known to be primarily
dictated by group III and IV muscle afferents – this response helps to maintain an
appropriate HR and pressor response to exercise (Amann et al. 2010) which subsequently
helps to control skeletal muscle blood flow (Alam & Smirk, 1937; O’Leary & Sheriff,
1995). These thinly myelinated (i.e., Type III) and unmyelinated (i.e., Type IV) afferents

31
are either sensitive to mechanical or chemical stimuli, although both afferents may
display polymodal properties meaning that, Type III receptors can be augmented in the
presence of metabolic stimuli (Kaufman et al., 1983).
In general, Type III afferents have been classified as being predominantly
mechanically sensitive and occurs when contraction or stretch distorts the receptive fields
of the afferents. These “mechano-sensitive” receptors are also known as
mechanoreceptors (Mense & Stahnke, 1983; Kaufman & Forster, 1996). Broadly, a
mechanoreceptor is a highly specific receptor that responds to mechanical stimuli, such
as pressure or stretch (Mense & Stahnke, 1983; Kaufman & Forster, 1996). Functionally,
it is well established that mechanoreceptive muscle afferents contribute to a significant
proportion of the drive controlling the cardiovascular system during exercise (Adreani et
al., 1997; Adreani and Kaufman, 1998; Drew et al., 2008; Gladwell and Coote, 2002;
Gladwell et al., 2005) and its response is more rapid (2-5 s) to cardiovascular control than
Type IV muscle afferents (5-20 s) (Brooks, Fahey and Baldwin 4th
ed., pg. 300).
Therefore, the centrally mediated blood flow response at the onset of exercise is
suggested to be related, at least partially, to stretch and pressure sensitive
mechanoreceptor afferents rather than metaboreceptor afferents.
In conclusion, the mechanoreflex is an autonomic mediated reflex involved in the
EPR which acts rapidly to regulate blood flow (phase I) via increased heart rate and
blood pressure at the onset of muscular movement. In the following section empirical
evidence is provided on the origins of the EPR with extended implications toward how
the mechanoreflex exerts a critical function in cardiovascular control at the onset of
exercise.

32
2.5.5 Regulation of muscle blood flow: Contributions of the muscle mechanoreflex.
One challenge when describing specific neural activation mechanisms involved with
human-muscle length dependent changes in blood flow and perfusion is separating
central command efferent input from peripheral muscle ergoreceptor afferent activation
from the EPR (metaboreceptors versus mechanoreceptors). As such, one classic method
to selectively activate the mechanoreceptors and the group III afferent-mediated
mechanoreflex independent of central motor unit activation (central command) and the
group IV mediated metaboreceptors is to employ passive stretch (Gladwell and Coote,
2002). Passive stretch has been shown to be capable of exclusively activating the
mechanoreflex because this response is believed not to initiate any muscle contractile
metabolite accumulation, which would confound the influence of mechanoreceptor
modulation, since the metaboreflex would also be activated.
When muscle mechanoreceptors are stimulated in isolation in an animal model,
using muscle stretch, they have been shown to produce a decrease in cardiac vagal
activity and an increase in cardiac and renal sympathetic nerve activity and blood
pressure (Stebbins et al. 1988; Matsukawa et al. 1994; Wilson et al. 1994; Murata &
Matsukawa, 2001). Likewise, the muscle mechanoreflex can be studied in humans via
passive stretch of the human triceps surae muscle group as a reductionist approach to
assess specific cardiovascular contributions (i.e. HR versus BP) associated with the EPR
(Baum et al., 1995; Drew et al., 2008, Gladwell & Coote, Gladwell et al., 2005; 2002;
Fisher et al., 2005; Ives et al., 2013). Unlike animal studies where research has
consistently reported that passive muscle lengthening stimulates autonomic

33
cardiovascular responses that serve to adjust blood flow control (Stebbins et al. 1988;
Matsukawa et al. 1994; Wilson et al. 1994; Murata & Matsukawa, 2001), human studies
on the cardiovascular responses to passive muscle stretch have been found to be
somewhat equivocal.
For example, it has been demonstrated in humans that passive stretch is capable of
raising HR and/or BP above baseline values (Gladwell and Coote, 2002; Fisher et al.,
2005; Gladwell et al., 2005), and that mechanoreceptors could only be attributed to this
response because voluntary muscle activation was not employed and thus by-products of
anaerobic metabolism did not contribute to metaboreceptor afferents. Specifically,
Gladwell and Coote (2002) first demonstrated a role for small muscle mechanoreceptors
in the cardiovascular response by employing a novel passive stretch of triceps surae
muscle group in the resting human. Here, the authors demonstrated that sustained
passive stretch of the triceps surae for 1 min, caused a significant increase in HR (5 ± 3
beat·min-1
) with no significant change in BP. In support of these findings Gladwell et al
(2005) further demonstrated in humans that selective activation of mechanoreceptive
afferents by passive calf muscle stretch decreased vagal tone and caused significant
increases in HR, by vagal inhibition. Fisher and colleagues (2005) investigated whether
the cardiovascular response to a standard muscle stretch was altered by varying the
metabolic conditions within the muscle by manipulating the circulation using the post-
exercise circulatory occlusion method under varying circumstances. By maintaining
circulatory occlusion following static exercise these authors (Fisher et al. 2005) were able
to successfully grade the level of muscle metaboreflex activation (Alam & Smirk, 1937;
Rowell et al., 1976). In accordance, their findings found that the HR and BP responses to

34
calf muscle stretch, in man, are unaffected by the level of concurrent metaboreflex
activation in that same muscle group. Collectively, in explanation to such findings, it is
possible that stretch stimulates a mechanically sensitive afferent population of nerves
whose response is unaffected, i.e. not sensitive, by the metabolic conditions within the
muscle.
Although not truly considered a stretch protocol, more recent evidence (Trinity et
al., 2010) has demonstrated that the central hemodynamic response to passive limb (knee)
movement is significantly blunted with pharmacological blockade of group III and IV
afferent nerve fibers, revealing that a significant portion of this response is mediated by
afferent signals. Additional evidence using a passive knee extension model (Gonzalez-
Alonso et al., 2008; Hellston et al., 2008; Parker et al., 2007; Radegran and Saltin, 1998;
Trinity et al., 2010; Wray et al., 2005), in the absence of local metabolic perturbation has
revealed that passive movement is capable of selectively mediating mechanoreflex
induced elevations in femoral artery blood flow. Other related evidence however, does
not support the role for mechanoreflex mediated changes in in HR, BP and muscle blood
flow. For example, Baum et al (1995) demonstrated a progressive blood pressure
increase but no HR change during sustained calf stretch for 1 min. McDaniel et al (2012)
further demonstrated that slow changes (passive extension and flexion of the knee joint)
in muscle length in humans elicited an increase in femoral blood flow by ~ 90% as knee
joint angle increased from 100º to 180º, whereas central parameters of cardiac output,
mean arterial pressure, stroke volume and HR did not change. It was concluded that the
muscle-length alteration in muscle blood flow was most likely the result from peripheral

35
factors, such as changes in capillary tortuosity and decreased diameter associated with
changes in muscle geometry and length and not the mechanoreflex.
In conclusion, there is substantial evidence in support that the EPR and muscle
mechanoreceptor afferents play a significant role in the early rise in skeletal muscle blood
flow. Whether this response is primarily controlled by central (HR and/or BP) or
peripheral (conduit artery and microvasculature) mediated mechanisms remains a
question of debate. Further research using a reductionist approach is therefore warranted
in order to determine the precise mechanism(s) responsible for the regulation of muscle
blood flow in humans.

36
Figure 2-1. Skeletal muscle capillary arrangement within the framework of skeletal
muscle. The tortuous arrangement of capillaries can play a substantial role in dictating
how red blood cells (RBC) – myocyte gas exchange occurs during varying levels of
muscle lengthening or shortening. Figure modified from Poole et al., 1989.

37
Figure 2-2. Phase I and phase II blood flow responses at the onset of moderate intensity
cycling exercise below the gas exchange threshold.

38
Figure 2-3. Arterial baroreflex modulation during neck pressure (NP) and neck suction
(NS). In response to NP, reduced firing of the baroreceptors sends a signal to the
medullary center of the brain to reduce parasympathetic nervous system activity. This
subsequently increases heart rate (HR), stroke volume (SV) and mean arterial pressure
(MAP). The opposite of this response occurs during NS. Figure modified from Fadel,
2008.

39
Chapter 3
Effect of self-administered stretching on NIRS-
measured oxygenation dynamics
3.1 Introduction
Stretching routines are an integral part of fitness and are applied in sport,
recreational and clinical environments (Gajdosik et al., 2007; Magnusson et al. 1996;
Morse et al., 2008). Despite the widespread use of many different stretching modalities,
limited knowledge exists regarding their mechanisms and efficacy. For example, passive
static stretching has been shown to lower blood glucose values in individuals with Type 2
diabetes or those at risk for developing Type 2 diabetes (Nelson et al., 2011), and
researchers have hypothesized that muscle-stretch creates some level of microvascular
and/or metabolic disturbance capable of causing such alterations. Nevertheless, the role
of microvascular and/or metabolic-related adaptations involved in human skeletal muscle
stretching has not been extensively examined. Further, if stretching is going to be
implemented in at risk populations, its mechanisms of microvascular efficacy must first
be identified.
The majority of the supporting mechanistic evidence for a role in skeletal muscle
length-dependent changes in microvascular dynamics has come from animal models
(Kindig & Poole, 1999; Nakao & Segal, 1995; Poole et al., 1997). Because capillaries in

40
skeletal muscle are retained open by collagenous struts (i.e. connexin) that affix the
capillary wall to the surrounding myocytes, lengthening of sarcomeres (Borg &
Caulfield, 1980) will create a kinetic sequence of events moving outward such that the
capillary extension reserve will cause compression and reduced vessel diameter (e.g.
tortuosity, Poole et al., 1997). This, in return, alters vascular resistance and subsequently
alters blood flow. This notion was observed by Poole et al. (1997) where capillary
tortuosity decreased with increases in sarcomere lengths up to a physiological range of
2.6 µm. As the sarcomere was further lengthened beyond its physiological properties
(e.g. 3.3 µm), the mean capillary diameter became reduced and resulted in blood flow
decreasing by approximately 40%. Therefore, it is possible that through human skeletal
muscle stretching some level of vascular resistance is induced, which may disturb
microvascular and metabolic adaptations, although the magnitude of this effect is largely
undefined in humans.
The application of near infrared spectroscopy (NIRS) to the site of interest
provides for a non-invasive assessment of functional insights with regard to skeletal
muscle microcirculation and oxygenation in humans (Boushel et al., 2001). This
technique uses the absorption characteristics of NIRS-derived light directed into the
microvasculature (arterioles, capillaries and venules) to determine the concentration
changes of oxygenated and deoxygenated hemoglobin/myoglobin ([HHb]) (Pereira et al.,
2007). In this regard, investigating the relative changes of [HHb] during a stretching
intervention would be of considerable practical importance, since this measure reflects a
similar time course of the microvascular partial pressure of oxygen (PO2) changes, and
thus the local balance between O2 availability and O2 utilization (Boushel et al., 2001).

41
Furthermore, there is an inherent need to identify transitional dynamics of muscle blood
volume as reflected by the concentration changes in O2 bound by hemoglobin ([Hbtot])
both during and after stretching (Pereira et al., 2007). This is particularly important
because it has been previously shown that after exercise elevations in glucose uptake and
glycogen repletion follows a similar time-course as that of skeletal muscle blood flow
(Ivy, 1991).
The present investigation aimed to determine, through the use of NIRS, the effect
that a single bout of muscle stretching of the plantar flexors has on changes in
oxygenation and blood volume. Based on the results of previous studies, it was
hypothesized that a single bout of stretching of the plantar flexors would cause a
significant decrease in [Hbtot], as an index of muscle-blood volume, parallel to a
significant increase in the relative changes in [HHb].
3.2 Methods
3.2.1 Subjects. Nine healthy individuals (7 males and 2 females) (mean age ± SD =
25.1 ± 3.7 years; body mass = 69.8 ± 13.1 kg; height = 172.5 ± 8.8 cm) volunteered to
participate in this three day investigation. Prior to the start of all testing, subjects read
and signed an informed consent form and completed a health status questionnaire
approved by the local Ethics Committee of the University of Toledo. Subjects were
excluded if they had a family history of blood clotting disorders or had previous
orthopedic related injuries. Three men and one woman reported performing in > 2.5 h
week of aerobic (running and cycling) exercise, 1-2 h week of resistance training and < 1
h week of stretching exercises, while the remaining four men and one woman reported 1-

42
3 h week of resistance training and 1-3 h week of recreational sports and no stretching.
As such, these subjects might be deemed best classified as healthy, recreationally
fitactive men and women. The subjects refrained from vigorous exercise and alcohol
consumption for 24 h, and caffeine ingestion for 6 h prior to testing.
3.2.2 Study design. The study was a randomized within subject design and involved
three sessions. The first session was a familiarization and orientation session in which
subjects became accustomed to the equipment and then performed a ramp cycling (25
W·min-1
) test to volitional exhaustion. The two experimental sessions were a stretch
session or cycling only session, which were randomized. To investigate the relative
change of microvascular muscle blood volume and oxygenation, near infrared
spectroscopy (NIRS) was employed to the region of interest, which was over the medial
head of gastrocnemius (GM). In this regard, NIRS provides continuous, noninvasive
monitoring of the absolute concentration changes of deoxygenated-Hb ([HHb]) and total-
Hb (Hbtot = O2Hb + deoxy-Hb) as an index of muscle-blood volume during stretching,
and thus reflects the relationship between local muscle O2 delivery and muscle O2
utilization at the site of O2 exchange within the region of NIRS interest (Pereira et al.,
2007). Measures of [HHb] and [Hbtot] were assessed in a baseline condition of 5 minutes
before the warm-up and then followed by a single bout of stretching of GM of the left
leg. Simultaneously, NIRS measures were assessed during stretching at timing interval
assessments of 30 s, 60 s, 90 s, 120 s and 240 s (total duration = 4 min). Upon
completion of the stretch, participants rested in a chair while NIRS measures were
continuously monitored at 1, 5 and 10 min.

43
3.2.3 Stretch session. Prior to the stretch session a standardized warm-up was
conducted. This involved participants cycling on a cycle ergometer (Monark, 823E) at
60 rpm with 1 kg resistance for 5 min. A 5 min rest followed the warm-up where the
subject rested his/her leg on a padded table approximately at the level of the heart.
Subjects then performed a single bout of stretching of the left plantar flexors on a
stretching device (Medi-dyne, Pro Stretch Original®). The stretch device is a
semicircular rigid plastic structure with a reinforced heel cup to prevent slipping during
stretching procedures. Subjects applied a slow continuous stretch by tilting back on the
stretch device while simultaneously keeping their left leg straight. Subjects applied their
own resistance for the stretch, with the instruction to stretch the muscles to the point of
discomfort (Behm et al., 2011; Behm & Kibele, 2007; Power et al. 2004). Thus, the
stretch may be defined as a self-administered stretch (SAS) (Behm et al., 2011). Each
subject verbally announced the point of discomfort to the technician, and this time was
marked down for future data analyses. Verbal feedback was continuously given
throughout the stretching maneuver in order to make sure that a continuous amount of
pressure was placed across the ankle joint during the entirety of the stretch. The duration
of the SAS was 4 min. This duration was determined based on pilot work from our
laboratory where it was observed that the response to which the NIRS-derived [HHb]
signal plateaus during SAS between 3 - 4 min (see Figure 1). During stretching, NIRS
measures of [HHb] and [Hbtot] each were assessed at 30 s, 60 s, 90 s, 120 s and 240 s.
During recovery the leg was rested on a padded table, approximately at the level of the

44
heart, and the knee bent slightly to minimize any resting tension on GM that may have
interfered with NIRS signal during the recovery.
3.2.4 Cycling session. A session involving high intensity cycling was also conducted
for this investigation. Currently there is no available knowledge to compare the
microvascular trauma that appears to occur during stretching with another common mode
of exercise. Therefore, comparing maximally attained values of [HHb] between high
intensity cycling and SAS would provide for a better understanding regarding the
magnitude effect of stretching and the metabolic responses. Furthermore, it is well known
that when cycling at high intensity workloads the ankle joint torque exerted by the plantar
flexors on the pedal crank more closely resembles moderate intensity exercise (~ 60 % of
MVC) (Driss & Vandewalle, 2013). Therefore, all comparison data reported herein are
assumed that a moderate intensity on the GM during cycling conditions is being
compared to the SAS condition. The cycling session consisted of a 5 min standardized
warm-up then followed by a 5 min rest, which was consistent with methods from the SAS
session. The subject then performed 4 min cycling at 85 % of the individual’s maximal
workload, which was obtained from the ramp protocol test in the preliminary testing
session. Only, NIRS measures of [HHb] were assessed in a baseline condition of 5 min
and its maximal value attained during the last 10 s of cycling. After cycling, subjects
rested in a chair with feet elevated on a padded table approximately at the level of the
heart and NIRS measures of [Hbtot] were measured at 1, 5 and 10 min in order to compare
the blood volume/blood flow interaction to the stretching condition.

45
3.2.5 Near infrared spectroscopy (NIRS) procedures. The
deoxyhemoglobin/myoglobin signal in the present study was determined using a
frequency-domain multi-distance NIRS system (OxiplexTS, ISS, Champaign, IL, USA)
during each intervention. This device operates at two wavelengths (690 nm and 820 nm)
with light source-detector separation distances of 2.0, 2.5, 3.0 and 3.5 cm for each
wavelength. The difference in the tissue absorbency between 820 nm, which reflects the
oxy-Hb signal and 690 nm, which reflects the deoxy-Hb signal, indicates the balance
between the delivery and removal of O2 at the capillary level (Pereira et al., 2007).
Additionally, the sum of these absorbencies provides an index of the relative
concentration change in total-Hb ([Hbtot]), which is considered to reflect total blood
volume (Pereira et al., 2007). Changes in [Hbtot] are exclusively related to blood volume
changes under the photon path however, they can be considered as an indirect measure of
local blood flow changes (Cardinale et al., 2007). The NIRS probe was placed
longitudinally over the distal belly of GM. The site was measured as 1/3 the distance
between medial condyle of the tibia and medial malleolus. The NIRS probe was held in
place by Velcro strapping, and then reinforced with additional elastic taping. An opaque
vinyl cloth was placed over the probe and additional elastic taping was used to prevent
any extraneous light from interfering with the NIRS signal. The sampling rate was set at
2 Hz. The NIRS probe was calibrated before each session according to manufacturer’s
recommended guidelines using a calibration block with known absorption and scattering
coefficients.

46
3.2.6 Maximal desaturation procedures. After each experimental intervention subjects
underwent a maximal relative physiological desaturation of oxygen at the site of GM
with NIRS measurement. This was conducted for normalization of the oxygenation
response when comparing it to the experimental stretching protocol or control. This
procedure takes ~ 5 min to achieve a plateau in the deoxy-Hb response. The left thigh of
the subject was occluded by inflating a pneumatic cuff (Hokanson, Bellevue, WA)
around the proximal portion of the thigh to ~ 300 mmHg. Complete deoxygenation was
confirmed by the plateau in [HHb] (i.e. the most maximal value during the last 10 s
occlusion phase). The pre-occluded baseline value was determined as the average during
5 min of resting phase. The baseline value was defined as 0 % and the maximum value
during ischemia was defined as 100 %, and the peak NIRS measures of [HHb] during
SAS and cycling were calculated relative to these values.
3.2.7 Myoelectrical activity (EMG). Myoelectrical activity was determined on four
randomly chosen subjects during a maximal voluntary isometric contraction (MVC) and
during SAS. Much of the literature measuring myoelectrical activity has consistently
reported negligible artifact during a stretching intervention (Magnusson et al., 1998).
Therefore, we used four randomly chosen subjects merely to verify pre-existing studies’
results to our study design that myoelectrical activity remained below the critical
threshold value during SAS. The MVC was performed prior to initiating the
experimental stretch session. The MVC was performed on an isokinetic dynamometer
(Biodex System 2, Biodex Medical Systems, Inc. Shirley, NY, USA) with the knee kept
straight by Velcro strapping. The ankle was aligned to the rotational axis of the

47
dynamometer. The best of three MVCs interspersed with a 5 min rest was used as 100 %
myoelectrical activity. To verify that muscle activation level remained negligible during
stretching, a 10 % cut-off from the MVC value was set, and is consistent with previous
methods (Trajano et al., 2014). An electromyography (EMG) electrode was placed just
proximal (~ 2 cm) to the attachment of the NIRS device on the GM of the four randomly
chosen subjects. The bipolar electrode configuration was set at a 1000 Hz analog-digital
(A-D) conversion rate (bandwidth 10 to 500 Hz) using the Bagnoli-8 Main Unit EMG
system (DelSys, Inc., MA, USA). The EMG data were simultaneously recorded using
LabChart (PowerLab System, ADInstruments, Model ML795, Castle Hill, Australia).
The skin under the electrodes was shaved, lightly abraded with sand paper and cleaned
with alcohol. These techniques reduced the inter-electrode resistance below 5 kΩ.
3.2.8 Day-to-day reproducibility. In four subjects, intraclass correlation coefficients
(ICC) were used to ensure day-to-day reproducibility of the dependent variables. This
was covered over three different testing days and separated by at least 24 h. A 95 %
confidence interval for the mean differences were used to assess whether test and retest
results differed significantly at the P < 0.05 level. An ICC > 0.80 was considered as
minimal acceptable reliability.
3.2.9 Statistical analysis. To assess the time course changes of the stretching
intervention on the dependent variables ([HHb] and [Hbtot]) during stretching a 1
(session) x 6 (timing – baseline at rest + 5 time points during stretch or cycling) repeated
measures (RM) analysis of variance (ANOVA) was run to determine any treatment effect

48
for the independent variable (SAS). To determine if a post-stretch hyperemia was present
after stretching, the time course of changes in [Hbtot] was analyzed using a 1 (session) x 3
(timing – baseline from rest + 3 time points after stretch or cycling) RM ANOVA. If a
significant interaction was found, separate t tests were run with Bonferroni post-hoc
procedures applied to identify where the differences were. When sphericity was violated,
Greenhouse-Geisser corrections were made.
To identify the difference in maximal [HHb] values during stretching versus
cycling conditions an independent t test was run. To identify post-condition measures of
[Hbtot] at 1, 5 and 10 minutes between stretching and cycling conditions similar t tests
were run.
All data were analyzed using Statistical Package for the Social Sciences (SPSS)
version 21.0 (Windows 2007, Chicago, IL). Data are reported as mean ± SD with the
alpha level set at P < 0.05.
3.3 Results
Day-to-day reliability for [HHb] and [Hbtot] were considered acceptable and
ranged from 0.98 for [HHb] and 0.97 for [Hbtot] values. It was also confirmed that
myoelectrical activity was negligible because the EMGs on the GM were detected below
10% of each of the four individual’s MVC during SAS.
3.3.1 Stretch. Repeated measures ANOVA revealed a significant interaction for [HHb]
during SAS. Comparison analysis for [HHb] (Figure 3.1) revealed a significant increase
from baseline at 60 s (P = 0.012, + 33.6 ± 6.7 %), 90 s (P = 0.011, + 36.1 ± 8.2 %), 120 s

49
(P = 0.009, + 41.5 ± 8.6 %) and 240 s (P = 0.013, + 43.8 %). No significant difference (P
> 0.05) was detected between baseline versus 30 s. Additional comparison analysis for
[HHb] revealed a significant increase from 30 s at 60 s (P = 0.008, + 20.6 ± 5.5 %), 90 s
(P = 0.006, + 23.6 ± 5.6 %), 120 s (P = 0.005, + 24.1 ± 6.4 %) and 240 s (P = 0.01, + 28.8
± 6.9 %) respectively (Figure 3.1). No significant interaction (P > 0.05) was detected for
[Hbtot] during SAS.
Repeated measures ANOVA revealed a significant interaction for [Hbtot] after
SAS (P = 0.02). Post-hoc analyses revealed a significant difference from baseline at 1
minute (P = 0.02, 8.8 ± 7.1 %), 5 minutes (P = 0.03, 7.8 ± 6.7 %) and 10 minutes (P =
0.03, 7.2 ± 6.8 %) after SAS.
3.3.2 Comparison with cycling session. Between conditions analysis revealed no
significant (P > 0.05) difference for peak values of [HHb] during SAS versus cycling
conditions (Figure 3.2). Additionally, there was no significant (P > 0.05) difference at
any point for [Hbtot] after stretching versus cycling respectively (Figure 3.3).

50
Figure 3-1. Graph representing muscle deoxygenation ([HHb]) changes at each specific
timing interval during a self-administered stretch. (*) Significantly different (P < 0.05)
than baseline. (¥) Significantly different (P < 0.05) than 30 s.

51
Figure 3-2. Graph representing muscle deoxygenation ([HHb]) responses between
cycling versus stretching conditions. No significant difference (P > 0.05) was found for
peak [HHb] values between conditions.

52
Figure 3-3. Graph representing muscle blood volume ([Hbtot]) postcondition response
between cycling versus stretching. No significant difference (P > 0.05) was found at time
interval.

53
3.4 Discussion
Little is known about the muscle-length dependent changes in blood volume and
oxygen dynamics in humans. Identifying this relationship in humans could offer
important mechanistic evidence to explain a number of physiological responses to
stretching. The novel findings of this investigation were that: 1) during SAS a transient
increase in [HHb] was observed, but [Hbtot] was not significantly impeded; 2) muscle
blood volume as indicated by [Hbtot] was significantly increased at every time interval
after SAS, thus providing novel evidence for a “stretch-induced hyperemia” effect; and 3)
peak microvascular muscle oxygen consumption as indicated by [HHb] during SAS and
moderate intensity cycling of the plantar flexors are similar.
Changes in [Hbtot] reflect blood volume changes, which can be considered as an
indirect measure of local blood flow changes (Cardinale et al., 2007) through muscle
vasodilation and overall conductance of that vessel (Pereira et al., 2006). Contrary to our
hypothesis, findings of the study indicate that SAS of the plantar flexors elicited no
significant decrease in [Hbtot] values. This hypothesis was based in part on the findings
from animal studies where it has previously been reported that a significant decrease in
muscle blood flow occurs when sarcomere length are increased beyond physiological
range (Kindig & Poole, 1999; Poole et al., 1997). However, passively stretched muscle
in vivo may be different when comparing it with animal preparations because: 1) there is
an anesthesia effect which reduces perceptions of pain, and 2) the degree of muscle
lengthening may not be in the physiological range when tendon insertions are cut, since
muscle lengthening in situ is limited by ligaments and joints. In accordance, our findings

54
do not support previous animal evidence, as no significant effect was found for [Hbtot]
during SAS of the human plantar flexors.
A unique finding of the present investigation was that a significant effect for
[HHb] was evident between 60 s - 240 s during SAS. Prior work by McCully (2010)
measured NIRS-derived oxygenation of the plantar flexors during a passive stretch
protocol in combination with intermittent isometric contractions. Thus, the extent to
which the muscle contractions contributed to the decrease in muscle oxygenation versus
the change in muscle length during the intense passive stretch of the plantar flexors was
not known. Indeed, isometric contractions as low as 25 % and 35 % of an individual’s
MVC have been reported to cause marked reductions in NIRS-derived measures of blood
volume and oxygenation within skeletal muscle tissue (DeRuiter et al., 2007), possibly as
a result of increased intramuscular pressure (Poole et al., 1997). Therefore, to eliminate
any confounding effect that isometric contraction may have as a result of stretching, a
single sustained stretch without the application of isometric contractions was employed in
the present study. We also confirmed that negligible muscular activity occurred during
our stretching intervention, because myoelectrical artifact from the EMG signal (data not
shown) on the muscle did not exhibit any appreciable EMG activity (< 10 % MVC).
Moreover, evidence from isolated muscle preparations suggest that despite a lack of
sarcolemma depolarization or cross bridge cycling (i.e. myoelectrical activity), a
passively stretched muscle can increase muscle oxygen consumption and heat production
(Barnes, 1987, Feng, 1932), increase carbon dioxide production (Eddy & Downs, 1967),
increase glycogen breakdown (Barnes & Worrel, 1985), increase glucose uptake
(Chamber et al., 2009) and increase phosphocreatine (PCr) breakdown (Barnes & Worrel,

55
1985). Hence, based on the above findings and findings of the present investigation, it
might otherwise be interpreted that human skeletal muscle stretching alone or in
combination with intermittent isometric contractions can cause a mismatching of O2
availability and O2 utilization of similar magnitude, thus decreasing muscle energy
provisions, such as PCr, which are thought to reflect transitional changes in [HHb]
derived from the NIRS signal (Boushel et al., 2001).
Further novel findings of the present investigation were that a significant increase
in [Hbtot] was observed at every time interval (1, 5 and 10 min) after SAS relative to
baseline values, suggesting that a single bout of stretching alone can induce a “post-
stretch hyperemia” effect. Exercise studies have used post-exercise hyperemia as a
marker to indicate insufficient O2 delivery at the end of dynamic exercise (Harper et al.,
2009), and this effect manifests from the release of local vasoactive metabolites (such as
K+ and H
+) and/or endothelial factors (MacDonald et al., 2001). As such, this adaptive
phase allows for a more coordinated distribution of blood flow to metabolically active
sites. Furthermore, it has also been shown that skeletal muscle hypoxia (reduced O2)
and/or passive stretch can increase glucose transport and translocation of glucose
transporters (Cartee et al., 1991, Iwata et al., 2007). Additional evidence reveals that
following exercise, elevations in glucose uptake and glycogen repletion follow a similar
time-course as that of skeletal muscle blood flow (Ivy, 1991). Due to the fact that [Hbtot]
was significantly increased after stretching in the present study coupled with the finding
that [Hbtot] was not significantly different between stretching versus cycling at any time
point (Figure 5), these findings are suggestive that some degree of hypoxia occurred
during stretching which may have augmented the blood volume/blood flow response.

56
Although this is speculative, it is possible that a stretch-induced hyperemia functions to
enhance glucose delivery within human skeletal muscle. This could explain why recent
evidence (Nelson et al., 2011) found significant increases in glucose uptake in diabetic
individuals after an acute bout of stretching.
Additional important findings of the present study were that no significant effect
for [HHb] values was observed between SAS and moderate intensity cycling. This
finding suggests that a single bout of moderate intensity cycling and stretching to a point
of discomfort at the GM level reflect a dynamic metabolic consistency, at least with
regard to O2 availability and O2 utilization. It might be somewhat difficult to interpret
this finding however; a few notable factors might offer an explanation. Firstly, it might
be speculated that stretching increases metabolic rate because significant changes in
[HHb] values were observed in the present study. However, there was no indication that
SAS increased myoelectrical activity as measured with surface EMG in the current
investigation. This finding is in accordance with prior work, as most studies involving
asymptomatic subjects who are slowly and passively stretched into end range positions,
do not demonstrate significant activation of stretched muscles (Magnusson, 1998).
Nevertheless, animal experiments have observed that despite a lack of sarcolemma
depolarization or cross bridge cycling (i.e. EMG activity), a passively stretched muscle
can indeed be metabolically active (Barnes, 1987; Feng, 1932). Therefore, it might be
suggested that instead of muscular work contributing to stretch-induced alterations in
[HHb], the mechanical distortion of the microvasculature during stretching may disturb
calcium homeostasis (Armstrong et al., 1993), such that a negative effect on the

57
synergistic interaction between the calcium-release ryanodine receptor and voltage-
sensitive dihydropyridine receptors becomes temporarily impaired (Balog, 2010).
Another possibility for the changes in [HHb] during stretching is that the changes
in the path-length of light (NIRS) with stretch might alter oxygenation results (McCully,
2010). However, as the path-length changed due to the lengthening of the sarcomere, the
change in absorption characteristics would be expected to occur very rapidly, on the same
time course as the initiation of the stretch maneuver. In the current investigation, a slow
stretch of the plantar flexors was employed, and this effect was not seen in the data.
In summary, our results indicate that a single self-administered stretch of the
human plantar flexors between 60 – 240 s can cause a substantial microcirculatory
disturbance. Furthermore, stretching of the plantar flexors for at least 240 s is capable of
improving blood flow to that muscle, as indicated by a significant rise in NIRS derived
Hbtot. Of clinical importance, stretching appears to be particularly relevant to those
individuals who may have a limited work capacity to perform the intended goal of a
rehabilitation program, as stretching is considered a low intensity form of exercise.

58
Chapter 4
Blood flow and oxygenation as a result of skeletal
muscle stretching in humans.
4.1 Introduction
Over the last several decades stretching studies have, for the most part, focused
exclusively on whether stretching improves range of motion about a joint and/or whether
stretch training can mitigate the age-related increases in musculotendinous stiffness
which may serve to improve upon activities of daily living (Gajdosik, 2001; Gajdosik et
al., 2007, Knudson et al., 2000, Shrier, 2004; Decoster et al., 2005; Nakamura et al.,
2012). Little attention however, has focused on the potential impact of skeletal muscle
stretching on cardiovascular function in humans. For example, most of the available
research examining the impact of muscle stretching on cardiovascular responses has
come exclusively from isolated animal preparations (Kindig & Poole, 2001; Mathieu-
Costello, 1987; Poole et al., 1997; Segal, 2000). Thus, it is difficult to infer a direct cause
and effect relationship on the mechanisms that effect vascular hemodynamics as a result
of skeletal muscle stretching in humans. Given that skeletal muscle stretching is
considered as a low intensity form of exercise, it is important to characterize the
mechanisms responsible for muscle length-induced alterations in cardiovascular function
in humans to most efficiently and safely prescribe stretching exercise.

59
On the basis of previous animal evidence, it has been shown that the lengthening
of a muscle within physiological ranges, using an isolated exteriorized preparation, can
significantly alter muscle blood flow (Poole et al., 1997; Kindig & Poole, 2001; Nakao &
Segal, 1995; Segal, 2001), and that increases in capillary tortuosity (Poole et al., 1997;
Kindig et al; 1999; Segal, 2001), intramuscular pressure (IMP) (Ameredes and
Provenzano, 1997; Kirkebo and Wisnes, 1982), muscle sympathetic nervous system
activity (MSNA) (Welsh and Segal, 1997) and muscle mechanoreceptor afferent feed
back (McDaniel et al., 2012) can greatly contribute to these alterations of microvascular
blood flow. One particular aspect of muscle stretch on capillary blood flood kinetics is
that capillary diameter and muscle blood flow are not altered in a linear manner; instead,
a threshold in the blood flow response initiated by muscle lengthening becomes evident
(Poole et al., 1997). As the muscle is lengthened or stretched, the capillaries are pulled
into a straight configuration (tortuosity decreases) until a mean sarcomere length of ~ 2.2
µm however, this may not alter blood flow (Poole et al., 1997). Further muscle length
increases within the physiological range (~ 3.3 µm) will stretch the capillaries in the
longitudinal direction along the axis of the sarcomere (Ellis et al., 1990; Poole and
Mathieu-Costello, 1992). Consequently, mean capillary diameter will become reduced,
vascular resistance to be increased and blood flow to be significantly impeded by as
much as 40% (Poole et al., 1997). Thus, there appears to be a threshold, at least with
regard to microvascular blood flow in animals, that is dependent on the intensity of
muscle stretch and that multiple mechanisms are the result of these alterations in the
microvascular resistance. How these physiological responses occur during muscle
stretching in humans, presently remains unclear.

60
Since muscle lengthening, at least seen exclusively in animal preparations, results
in alterations in microvascular resistance and subsequent blood flow through this
network, it might be assumed that similar responses occur in the microvasculature in
humans. Furthermore, regulation of blood flow in the larger feeder “upstream” conduit
arteries may become significantly altered as result of increases in “downstream”
microvascular resistance. This presumption is based on the well-known fact that
previous evidence (Thijsen et al., 2009; Casey et al., 2012; Schreuder et al., 2014) has
demonstrated that artificial conditions that elevate downstream vascular resistance (i.e.
cuff occlusion) provoke large increases in upstream conduit artery retrograde blood flow.
Retrograde blood flow is defined as the resistance to blood flow and therefore, significant
increases in retrograde may decrease net mean blood flow of the conduit artery (Thijsen
et al., 2009). Therefore, it is possible that increasing microvascular resistance via muscle
stretch in humans, may create large increases in retrograde blood flow which may
subsequently create a significant impediment on mean blood flow within the conduit
artery in a stretch intensity dependent fashion.
In an effort to address this issue – whether a threshold exists between the level of
muscle lengthening and peripheral hemodynamic responses in humans, the primary
purpose of this investigation was to measure local arterial blood flow responses before,
during and after varying intensities of muscle stretch. We hypothesized that the higher
stretch intensities would create a larger conduit artery retrograde blood flow response and
accordingly, this would create a significant decreases in mean blood flow through the
muscle in an intensity dependent manner. In order to elucidate the potential mechanisms
associated with changes in conduit artery blood flow the second purpose of this

61
investigation was to measure tissue oxygenation and systemic cardiovascular responses
before, during and after varying intensities of muscle stretch.
4.2 Methods
4.2.1 Experimental Overview. This investigation used a randomized, within-subject
design to evaluate the effectiveness of three different stretching intensities on peripheral
and central cardiovascular parameters. Participants reported to the laboratory on four
separate occasions. The first session consisted of a preliminary testing and informative
session which consisted of the following: 1) filling out an activity and questionnaire
form, 2) obtaining anthropometric measures, 3) familiarization to the equipment and the
experimental protocol (Figure 4-1), 4) familiarization with the stretch intensities to be
performed and 5) three maximal voluntary isometric contractions (MVICs) were
performed. During the remaining sessions, each subject performed one of three
stretching conditions (described in detail below) which consisted of varying intensities of
stretch separated by at least 48 h of recovery and included the following: 1) constant
angle moderate intensity stretch (CAS), constant angle low intensity stretch (LIS) and
constant torque moderate intensity stretch (CTS). Each stretching session was similar in
design. Following 15 min of rest in a prone position, a stretch was performed for 4 min
followed by 10 min of recovery in the same position (Figure 4-1). Measures of central
(HR, BP), peripheral conduit artery (popliteal artery diameter and flow), and
microvascular (blood volume and oxygenation) were the key variables measured in this
investigation.

62
4.2.2 Subjects. Twelve healthy males (age 28.2 ± 4.7 yr, height 173.1 ± 2.6 cm, body
mass 67.2 ± 8.7 kg) volunteered to participate in the present investigation. All were
habitually physically active but none were specifically flexibility trained per health and
fitness activity questionnaire. Females were excluded because: 1) hormonal influences
during different phases of the menstrual cycle may augment muscle tendon unit (MTU)
stiffness (Morse, 2011), 2) females in general, exhibit a less stiff MTU as compared to
males (Morse, 2011) and 3) females have an attenuated mechanoreflex, and rely more on
local vasodilation than males (Casey et al., 2014; Ives et al., 2013). Participants received
complete written and verbal details of the experimental procedures and potential risks
involved before signing an informed consent form approved by the University of Toledo
Institutional Review Board and in accordance with the Declaration of Helsinki. All
testing sessions were performed in a thermoneutral environment (22º C) and subjects
refrained from exercise 24 h and caffeine and alcohol consumption12 h prior to data
collection.
4.2.3 Experimental procedures. Upon arrival to the laboratory participants were
instructed to lie prone for at least 15 min on a padded table with head piece to support the
head. During this time, subjects were equipped with electrocardiogram (ECG) (in the
standard lead II position) electrodes, electromyography (EMG) (DelSys, Inc., MA, USA)
electrodes and blood pressure was monitored via finger photoplethysmography (CNAP™
Monitor500, CNSystems, Graz, Austria). In addition, the subject’s right foot was placed
in a footplate attached to an isokinetic dynamometer (Biodex, Shirley, NY, USA). The
ankle joint was carefully aligned to the axis of rotation of the dynamometer and then

63
secured in place with a heel support and straps to minimize foot displacement during
passive stretching. The position of the heel and foot was adjusted to same height prior to
stretching to ensure the same point of rotation for each subject. This positioning elicited
a knee joint angle held constant throughout each testing session at 160º flexion. Prior to
each experimental stretch session, maximum triceps surae extension was accomplished
by brief passive dorsiflexion of the foot to an angle just before moderate discomfort upon
which, the ankle was returned to baseline or 110º dorsiflexion (20º into plantar flexion).
We choose 110º dorsiflexion because this is a point were no resting passive tension is
created on the dynamometer as assessed from the passive torque signal. After a 1 min
baseline, the foot was passively stretched on the dynamometer at a rate of 10º/s into
dorsiflexion to the predetermined stretch intensity, which was then programmed into the
dynamometer. Beat-by-beat hemodynamic parameters of heart rate (HR), blood pressure
(BP), Doppler ultrasound estimates of popliteal artery blood flow and NIRS derived
estimates of microvascular deoxygenated forms of hemogblobin (Hb) and myoglobin
([HHb]), considered as a surrogate of microvascular oxygen (O2) extraction (Delorey et
al., 2003; Grassi et al., 2003), and the sum total of O2Hb and HHb, considered as
estimates of microvascular blood volume concentration ([Hbtot]), were continuously
measured and averaged as follows: 1) during baseline (rest) in a period of 30 s preceding
the passive stretch, 2) during the first 15 s upon initiation of stretch, 3) during the last 15
s of each of time interval of 60 s, 150 s, and 240 s during passive stretch for 4 min. After
4 min of passive static stretch, the footplate was rotated back to resting position (110º
dorsiflexion) and hemodynamic variables were continuously measured and recorded as

64
follows: 1) during the first 15 s after the stretch was released and 2) during the last 15 s of
each time interval at 1, 5 and 10 min after stretch (Figure 4.1).
4.3 Muscle Stretching Sessions
4.3.1 Experimental session – CAS. The CAS session served as the reference session for
ankle joint angle and torque measurements in experimental testing sessions 2 and 3,
which were randomly assigned (LIS or CTS). With the subject fully relaxed, a 1 min
baseline period was followed by 4 min of a sustained constant angle passive stretch. In
brief, the isokinetic dynamometer passively stretched the plantar flexor by rotating the
footplate into dorsiflexion, which was according to the predetermined maximal range of
dorsiflexion. Maximal dorsiflexion was identified by each subject as a point just before
the feeling of moderate discomfort, and is consistent with the approaches used in
previous research (Behm & Kibele, 2007; Kruse and Scheuermann, 2014). Descriptively,
this point of discomfort was explained by the technician to each subject as “a feeling of
discomfort as if you were to perform an over-hang calf stretch over a step.”
4.3.2 Experimental session – LIS. For the LIS session, a 1 min baseline period was
followed by a constant angle passive stretch of gastrocnemius medialis muscle by
rotating the footplate to 80 % of the predetermined end ROM from the angle acquired
from Session 1, and holding for 4 min. We chose this intensity because based on
preliminary work from our laboratory this is the point just before subjects felt “slight
discomfort.”

65
4.3.3 Experimental session – CTS. Due to the phenomenon of viscoelastic creep where
the musculotendinous unit “creeps” below its initial passive torque level during the
duration of a constant angle stretch, the angle of the plantar flexors was adjusted
continuously during the CTS session so that a continuous amount of pressure was held
constant on the plantar flexors across the duration of the stretch (Figure 4.2). The
subject’s ankle was passively dorsiflexed to the “point of mild discomfort,” which was
based off the subject’s angle from reference session 1. Rather than holding the angle
constant during the entirety of the stretch, continuous torque adjustments were applied by
the dynamometer so that the starting torque was equal to the finishing torque (Figure 4.2).
4.4 Macrovascular Peripheral Hemodynamic Measurements
4.4.1 Blood velocity. Prior to Doppler blood velocity measurement a longitudinal B-
mode image of the popliteal artery was required to determine the diameter of the vessel,
which was measured using a 7 MHz echo Doppler ultrasound probe (z.one ultra,
ZONARE Medical Systems Inc., Mountain View, Calif., USA) at 4-5 cm depth. All
images were acquired proximal to the branching of the tibial artery at the position that
produced the best quality image. Once a good quality image was obtained the site of the
probe was marked on the skin with ink for repeatable and consistent measurements.
Instantaneous blood velocity (cm/s) in the right popliteal artery was continuously
measured using a Doppler ultrasound velocimetry system (NEUROVISION™ model
500-M, Multigon Industries, New York, USA) operating in continuous mode. This
device has been shown to produce reliable and accurate measurements over the popliteal
artery at rest and dynamic exercise in a prone horizontal position (CV%: 7.5 ± 5.4%;

66
ICC: 0.84) (Villar & Hughson, 2013). The flat ultrasound probe was held in place over
the popliteal artery embedded at a 45° angle of insonation relative to the skin.
Ultrasound settings were recorded for each individual and used during subsequent test
days to keep consistent for each participant.
4.4.2 Diameter and blood flow. In pilot studies, we measured popliteal artery diameter
in five subjects before, during and after passive stretch. Consistent with previous results
from our lab and others (MacDonald et al., 2001; Gonzales et al., 2007; Thompson et al.,
2008) using dynamic exercise protocols, we found no significant increase in popliteal
artery diameter during or after a single 4 min stretch (CAS) of the plantar flexors relative
to baseline. Thus, resting popliteal artery diameter for each subject was used to calculate
blood flow at rest, during stretch and after stretch. The popliteal artery of the right leg
was insonated at 60° ~ 2-8 cm above popliteal crease in the popliteal fossa at the back of
the knee, where it could be optimally visualized. The sample volume was maximized
according to vessel size and centered, which was verified by real-time ultrasound
visualization of the vessel. Ultrasound images were taken as the average of three separate
measurements during diastole at the end of the 15 min rest period (baseline) and at the
end of muscle stretch during a 15 s period. The mean of these measurements was then
used to calculate an average cross-sectional area (CSA = πr2) of the artery, where r is the
radius of the artery. Assuming the popliteal artery is cylindrical, the blood flow was
calculated as the time average mean velocity multiplied by the cross sectional area of the
vessel to obtain relevant blood flows (popliteal artery blood flow (ml/min) = blood
velocity (cm/s) x CSA x 60).

67
4.4.3 Shear indices. Shear rate was calculated for mean blood velocity and its
antegrade and retrograde components using the following equation: shear rate (s–1
) = (4 x
Vm)/D (Silber et al. 2005), where Vm is blood velocity (cm/s) and D is the diameter of
the vessel (cm). Antegrade shear rate represents forward flow through the popliteal
artery, whereas retrograde shear rate results from the resistance to flow. The
representative of bidirectional flow from these parameters can collectively be captured as
the dimensionless measure known as the oscillatory shear index, which is calculated
using the following equation: | retrograde shear rate |/(antegrade shear rate + | retrograde
shear rate |) (Moore et al. 1994).
4.4.4 Vascular conductance (VC). The relative ease of blood flow through a conduit
artery can be measured as VC and is described by the equation: VC = Blood flow/mean
arterial pressure (MAP).
4.5 Microvascular Hemodynamics
4.5.1 Near Infrared Spectroscopy (NIRS). To determine microvascular perfusion and
hemodynamic responses, NIRS-derived changes in tissue concentrations of HHb ([HHb])
were measured over the distal aspect of gastrocnemius medialis with a frequency-domain,
phase-modulation NIR spectrophotometer (ISS Oximeter model 96208, Champaign,
Illinois, USA), which is in accordance with previously described methods from our
laboratory (Kruse & Scheuermann, 2014). In brief, the spectrophotometer uses intensity
modulated light at a frequency of 110 MHz to measure light attenuation caused by tissue

68
absorption and scattering. Laser diode sources emit light at two wavelengths, 750 nm,
corresponding to the high spectral HbO2 absorption peak, and 830 nm, to the high
spectral HHb absorption peak and one detector fiber bundle (source-detector distance 2.0-
3.5 cm). In this study, to minimize light scattering due to changes in water and blood
volume in the tissue we measured light attenuation at a wavelength of 830 nm. The
[HHb] can be considered as a proxy for microvascular O2 extraction (Delorey et al.,
2003; Grassi et al., 2003) independent by changes in blood volume under the NIRS probe
(Ferreira et al., 2005; Grassi et al., 2003; Maehara et al., 1997). Thus, the NIRS derived
[HHb] signal can provide unique, noninvasive insight into the control mechanisms
governing the relationship between O2 delivery and O2 utilization at the site of interest
during muscle stretch. Furthermore, the sum of the two variables (O2Hb + HHb) is
related to changes in the total Hb volume in the muscle region of interest (Grassi et al.,
2003). Day-to-day reliability for this device on microvascular responses was considered
to be acceptable (ICC = 0.98 for [HHb] and 0.97 for [Hbtot]) as based on prior work from
our laboratory (Kruse and Scheuermann, 2014).
The NIRS probe was held in place by Velcro strapping, and then reinforced with
additional elastic taping. An opaque vinyl cloth was placed over the probe and additional
elastic taping was used to prevent any extraneous light from interfering with the NIR
signal. The sampling rate was set at 2 Hz and 15 sec averages, which were time aligned
to macro- and central cardiovascular responses during each specific time interval during
and after stretching.
To normalize the data to individual maximal physiological changes each subject
underwent a maximal physiological desaturation of oxygen (HHb) at the site of

69
gastrocnemius medialis using a pneumatic cuff (D.E. Hokanson, Bellevue, Wash., USA)
placed proximal to the NIRS sensor and inflated to ~ 300 mmHg for ~ 5min, or until
complete deoxygenation was confirmed by the plateau in the muscle [HHb] response (i.e.
the most maximal value during the last 10 s occlusion phase). The pre-occluded baseline
value was determined as the average during 5 min of resting phase. The baseline value
was defined as 0 % and the maximum value during ischemia was defined as 100 %. The
NIRS measures of [HHb] during each stretching session were calculated as the relative
percent concentration change of these values (% ∆[HHb]).
4.6 Central Hemodynamics Measurements
4.6.1 Blood pressure. To address whether central cardiovascular parameters influence
the blood flow/blood volume response as a result of different intensities of muscle
lengthening, the present study measured, on a beat-by-beat basis heart rate (HR) and (BP)
blood pressure responses. Mean arterial pressure was non-invasively monitored with an
automated finger cuff on a beat-by-beat basis (CNAP™ Monitor500, CNSystems, Graz,
Austria). This device has been shown to produce clinically acceptable agreement in
subjects lying in the prone position when compared against values obtained from the
intra-arterial canula method (Dewhirst et al., 2013). The monitoring finger cuffs were
placed around the middle-two fingers of the left hand and supported at the heart level.
From the arterial blood pressure waveform, MAP was calculated from the systolic blood
pressure (SBP) and diastolic blood pressure (DBP) using the standard equation, MAP =
DBP + ⅓ (SBP – DBP). For each subject, MAP, SBP and DBP were averaged over 15s

70
intervals and time aligned with the central and peripheral hemodynamic measurements
for comparison.
4.6.2 Heart rate. Heart rate was measured using a standard three lead ECG, placed at
specified landmarks on the dorsal side of the subject’s torso according to the
manufacturer guidelines. For each subject, HR was averaged over 15s intervals and time
aligned with the central and peripheral hemodynamic measurements for comparison.
4.7 Additional measurements
4.7.1 Purpose. Our purpose was to determine peripheral conduit artery, central and
microvascular responses to controlled passive stretching. To ensure that muscle
activation and breathing patterns (i.e. sinus arrhythmia) did not confound our result,
EMG and cyclical respiratory breathes were monitored throughout the stretch maneuvers.
4.7.2 Muscle activation. EMG was recorded on gastrocnemius lateralis of the right leg
during the MVIC and during stretch sessions to verify that myoelectrical activity
remained below the critical threshold value during stretching. EMG activity greater than
10% (measured as the root mean square [RMS] in millivolts [mV]) of MVIC was
considered significant enough that it would confound the result, and is consistent with
previous methods from our laboratory (Kruse et al., 2014) and others (Trajano et al.,
2014). The bipolar electrode configuration was set at a 1000 Hz analog-digital (A-D)
conversion (bandwidth 10 to 500 Hz) and then smoothed using a 50 ms RMS window
using the Bagnoli-8 Main Unit EMG system (DelSys, Inc., MA, USA) and LabChart 7.0

71
(PowerLab 16SP, ADInstruments, CO, USA). Prior to electrode placement, the skin was
shaved, abraded, and cleaned with alcohol to ensure an interelectrode resistance value
below 5 kΩ. Movement artefacts were minimized by taping the electrodes wires to the
skin.
4.7.2 Breathing pattern. In an effort to prevent vagal induced changes in breathing by
the sinus arrhythmia from contributing to changes in HR responses during and after
stretch maneuvers, the respiratory cycle as well as the rate and depth of breathing was
assessed using a metronome and respiratory belt (UFI Model 1132 Pneumotrace II™,
CA, USA) that was placed around the chest. The Pneumotrace is a piezo-electric
respiration transducer that generates a linear signal in response to changes in thoracic
circumference associated with respiration. Pilot work determined that the best placement
of this band to eliminate excessive artifact was over the middle-to-lower torso such that
the elastic strain gauge was visible on back-side. Respiratory rate was standardized for
each subject, which meant that subjects set a breathing rate that they found to be most
comfortable on the first testing; this rate of breathing was controlled via audible beats
from a metronome. Subjects were asked to maintain the same respiratory pattern for each
of the remaining testing sessions. A 10% cut-off from the depth of oscillatory breathing
values (measured as the RMS in mVs) relative to baseline was set as the threshold to
identify whether cyclical breathing remained negligible during each stretch maneuver at
each pertinent time interval.

72
4.7.3 Torque. Ankle plantar flexor passive torque, angle and speed of rotation were
monitored using an isokinetic dynamometer (Biodex Medical Systems, Shirley, NY,
USA). All outputs underwent A-D conversion and recorded using LabChart 7.0
(PowerLab 16SP, ADInstruments, CO, USA).
4.8 Statistical analysis
All data were analyzed using Statistical Package for the Social Sciences (SPSS)
version 21.0 (IBM, Chicago, IL). A Shapiro-Wilk test was used to confirm normal
distribution and a Mauchley test of sphericity to verify homogeneity of variance.
Furthermore, day-to-day reliability for popliteal conduit artery mean blood flow
responses was determined in a subset of 5 subjects at rest and during stretching using an
intraclass correlation coefficient (ICC) and a coefficient of variation (CV) (Hopkins,
2000). Initially, a three-way ANOVA with repeated measures was conducted to analyze
the interaction effect of exercise condition (CAS vs. LIS vs. CTS) and time during stretch
(15s vs. 60s vs. 150s vs. 240s) and after stretching (15s vs. 60s vs. 1min vs. 5min vs.
10min). If significant differences were detected, Tukey’s post hoc procedures were
applied for pairwise comparisons to identify condition differences over time in blood
flow, NIRS, vascular conductance, shear rate, heart rate, blood pressure and passive
torque responses as a result of stretching. When sphericity was violated, Greenhouse-
Geisser corrections were made. Statistical significance was set at p < 0.05.
4.9 Results

73
4.9.1 General results. Day-to-day reliability for popliteal conduit artery mean blood
flow responses in a subset of 5 subjects at rest and during stretching were: Rest: CV =
9.7% and ICC = 0.84; Stretch: CV = 9.1% and ICC = 0.86. EMG and cyclical breathing
patterns were remained below the 10% threshold during on- and off-transitions from
stretch, and thus were not considered sources of contamination. Acquisition of high-
quality imaging was achieved for a majority of the participants; however, ultrasound
images for one participant were noisy and had too much artifact (border detection was not
clearly visible across all sessions at baseline). In accordance with software quality
control recommendations, these images were excluded from the analysis. Therefore,
results are presented for n = 11.
4.9.2 Peripheral hemodynamic responses during and after stretching. Prior to passive
stretch, no significant (P > 0.05) difference was present in any of the cardiovascular
(peripheral, microvascular and central) variables measured at rest (baseline).
Results for antegrade, retrograde and mean blood flow through the popliteal artery
are shown in Figures 4-3 and 4-4. The analysis revealed that there was a significant
interaction on antegrade (P = 0.03) and retrograde (P = 0.03) blood flow during stretch.
Additionally, there was a main effect of time for antegrade (P = 0.02) and retrograde
blood flow (P = 0.03) respectively. Post-hoc analyses revealed that, during stretch, the
antegrade and retrograde blood flow immediately increased and remained elevated in
each condition for 4 min (Figure 4-3). The parallel increases in antegrade and retrograde
blood flow resulted in no net change (P > 0.05) in mean blood flow (MBF) during
stretch. After stretch, however, there was a significant (P < 0.01) interaction for MBF.

74
Additionally, there was a main effect for time (P = 0.01) and condition (P = 0.01) for
MBF. Specifically, MBF increased in all groups immediately (post 15 s, P < 0.01),
indicating a post-stretch hyperemia. MBF remained elevated at post 60s for CAS (P =
0.01) and CTS (P = 0.02), but returned to baseline by 60s for LIS (P > 0.05). After
stretch, MBF was significantly higher (post 15 s, P < 0.001) in CTS than CAS and LIS
conditions respectively.
Table 4.1 illustrates shear indices over time during passive stretch. As with
antegrade and retrograde blood flow responses, shear rate and oscillatory shear index
followed a similar time course change showing an immediately increase (P < 0.05)
followed by a sustained elevation during 4 min of stretch. Mean shear rate remained
unchanged (P > 0.05). Since MBF and MAP responses did not change during stretching,
no changes (P > 0.05) in vascular conductance were observed at any time interval.
Table 4.2 illustrates shear indices over time after stretching. After stretching,
antegrade shear rate, mean shear rate and oscillatory shear index showed a similar time
course change as that of blood flow respectively. Vascular conductance immediately
increased (post 15 s, P < 0.05) after stretching in each condition. Vascular conductance
remained elevated at post 60 s for CTS, but returned to baseline by 60 s for CAS and LIS
(P > 0.05) respectively.
4.9.3 Microvascular hemodynamic responses during and after stretching. Results for
microvascular blood volume concentration ([Hbtot]) through the gastrocnemius medialis
muscle is shown in Figure 4-5. The analysis revealed that there was a significant
interaction on [Hbtot], during stretch (P < 0.03). Additionally, there was a main effect of

75
time (P < 0.01) for [Hbtot] respectively. Post hoc analyses revealed that, during stretch,
the [Hbtot] increased in CAS and LIS conditions at 60 s (P = 0.02), 150 s (P = 0.03) and
240 s (P = 0.03) whereas CTS did not significantly (P > 0.05) change respectively.
Further analyses revealed that there was a significant interaction on [Hbtot] after
stretching. Additionally, there was a main effect of time (P < 0.01) and condition (P =
0.01) for [Hbtot] respectively. Specifically, [Hbtot] increased in all groups immediately
(post 15 s, P < 0.01) and remained elevated (P < 0.05) in each condition at every time
point. Furthermore, the immediate (post 15s) “overshoot” response was intensity
dependent such that CTS and CAS conditions were significantly (P < 0.05) higher than
LIS respectively.
Figure 4-6 represent the change in percent concentration in muscle deoxygenation
(% ∆[HHb]) during stretching among each condition. The analysis revealed a significant
interaction for [HHb] during stretch (P = 0.04). Additionally, there was a main effect of
time (P < 0.01) and condition (P < 0.01) for % ∆[HHb] respectively. Post hoc analyses
revealed that during stretch, % ∆[HHb] transiently increased (P < 0.05) over time in all
conditions, however, LIS plateaued by 150 s, whereas CAS and CTS continued to
increase such that there was a stretch intensity dependent increase at 150 s and 240 s
between conditions respectively. Furthermore, CAS and CTS conditions elicited a
significantly (P < 0.01) greater % ∆[HHb] response at 150s and 240s as compared to LIS.
4.9.4 Central hemodynamic responses during and after stretching. Results for central
hemodynamics during stretch are shown in Table 4.3. The analysis revealed that there
was a significant interaction (P < 0.001) on HR during stretch. Additionally, there was a

76
main effect of time for HR. During CAS, HR immediately increased (P < 0.001) (+ 5 ± 3
bpm) and remained elevated (P < 0.001) for 60 s (+ 4 ± 4 bpm) before returning to
baseline values by 150 s. During LIS, HR immediately increased (P < 0.001) (+ 4 ± 4
bpm) but returned to baseline values by 60 s. During CTS, HR immediately increased (P
< 0.001) (+ 6 ± 4 bpm) and remained elevated (P < 0.001) for each time interval (60 s = +
5 ± 6 bpm; 150 s = + 5 ± 5 bpm; 240 s = + 5 ± 5 bpm) during 4 min of stretch. During
stretch, there was no interaction or main effect (P > 0.05) in SBP, DBP and MAP
parameters in any condition respectively (Table 4.3).
Results for central hemodynamics after stretch are shown in Table 4.4. The
analysis revealed that there was a significant interaction (P < 0.001) on HR after stretch.
Additionally, there was a main effect of time for HR. After stretching, HR immediately
increased (P < 0.01) in the CAS condition (+ 5.5 ± 3.8 bpm) and returned to baseline by
60 s. After stretching, HR remained significantly elevated (P < 0.01) immediately
following stretching in the CTS condition (+ 4.8 ± 4.3 bpm) and returned to baseline by
60 s. There was no change (P > 0.05) in HR following the LIS condition. After
stretching there was no interaction (P > 0.05) for SBP (Table 4.4). However, there was
significant (P < 0.01) interaction for DBP after stretch. Additionally, there was a main
effect for time for DBP. Specifically, in the CAS and CTS conditions, DBP was
decreased (P < 0.05) at every time interval after stretching (Table 4.4). Collectively, this
resulted in MAP being decreased (main effect for time, P < 0.05) in CAS and CTS
conditions at every time interval. The LIS condition did not exhibit any significant
change (P > 0.05) in DBP and MAP parameters, suggesting that higher intensity
stretching yielded a post-stretch hypotensive response.

77
4.9.5 Passive resistive torque. Figure 4.2 represents a raw data tracing of passive
resistive torque across time in CAS condition. Passive torque was similar (P > 0.05)
between CAS (38.4 ± 4.5 ft/lbs) and CTS (37.8 ± 5.9 ft/lbs) conditions at the onset of
stretch but was significantly (P < 0.001) higher than LIS condition (20.4 ± 11.9 ft/lbs).
CAS demonstrated a 41.4 ± 7.7% (P < 0. 001) decrease in torque across time (38.4 ± 4.5
vs. 22.6 ± 4.1). LIS demonstrated a 35.8 ± 6.2% (P < 0.001) decrease in torque across
time respectively (20.4 ± 4.9 ft/lbs vs. 11.9 ± 3.2 ft/lbs). There was no change (P > 0.05)
in torque across time in the CTS condition.

78
Tab
le 4.1
Perip
heral b
iom
echan
ical hem
od
ynam
ics befo
re, durin
g an
d after stretch
ing. V
alues are m
eans ±
SD
. *
Sig
nifican
tly d
ifferent fro
m b
aseline.

79
Tab
le 4.2
Perip
heral b
iom
echan
ical hem
od
ynam
ics befo
re, durin
g an
d after stretch
ing. V
alues are m
eans ±
SD
. *
Sig
nifican
tly d
ifferent fro
m b
aseline.

80
Tab
le 4.3
Cen
tral hem
od
ynam
ic responses d
urin
g stretch
ing. V
alues are m
eans ±
SD
. * S
ignifican
tly d
ifferent fro
m b
aselin
e.

81
Tab
le 4.4
Cen
tral hem
od
ynam
ic responses after stretch
ing. V
alues are m
eans ±
SD
. * S
ignifican
tly d
ifferent fro
m b
aseline.

82
Figure 4-1. Experimental protocol representing three different intensities across time.
CAS = constant angle stretching at moderate intensity; LIS = constant angle stretching at
80 % from reference (CAS) session; CTS = constant torque stretching at moderate
intensity stretching from reference session (CAS).

83
Figure 4-2. Figure representing constant angle moderate intensity stretching (CAS)
versus constant torque moderate intensity stretching (CTS). Note. The viscoelastic creep
phenomenon during CAS decreases passive resistive torque across time, whereas CTS
maintains passive resistive torque via continuous adjustments made by the dynamometer.

84
Fig
ure 4
-3. P
opliteal artery
blo
od flo
w resp
onse d
urin
g stretch
ing. V
alues are m
eans ±
SD
. There w
as a main
effect for tim
e (P <
0.0
5) . *
Sig
nifican
tly d
ifferent th
an b
aseline. P
< 0
.05.

85
Figure 4-4 Popliteal artery mean blood flow responses before, during and after
stretching. Values are means ± SD. There was a main effect for time (P < 0.05) and
condition (P < 0.05). * Significantly different from baseline in CAS, LIS and CTS; #
CTS is significantly different than CAS and LIS. P < 0.05.

86
Figure 4-5. Microvascular blood volume responses before, during after stretching.
Values are means ± SD. There was a main effect for time (P < 0.01) and condition (P <
0.05). * Significantly different from baseline in CAS and LIS. # Significantly different
in CAS vs LIS and CTS vs LIS. † Significantly different from baseline in CAS, LIS and
CTS. P < 0.05.

87
Figure 4-6. Microvascular muscle deoxygenation response before and during stretching.
Values are means ± SD. There was a main effect for time (P < 0.01) and condition (P <
0.01). * Significantly different from baseline in CAS, LIS and CTS. † Significantly
different from CAS and LIS condition. P < 0.05.

88
4.10 Discussion
To our knowledge, this is the first study to simultaneously examine muscle blood
flow and oxygenation-deoxygenation responses during and after stretching in humans.
The novel findings of the present study indicate that skeletal muscle stretching of the
plantar flexors in humans: 1) does not decrease conduit artery blood flow or
microvascular blood volume during stretching; however, the magnitude of antegrade and
retrograde blood flow/shear profiles are altered, 2) causes an acute post-stretch hyperemic
response at the macro- and microvascular level that is intensity dependent, 3) decreases
systemic blood pressure (afterward), and 4) reduces resting retrograde blood flow and
shear stress after stretch. Collectively, these results show that skeletal muscle stretching
in humans can be a substantial cardiovascular event. Moreover, the reductions in DBP,
retrograde blood flow and shear responses seen after stretching suggests that skeletal
muscle stretching in humans reduces myogenic vascular tone which may confer
additional beneficial vascular effects in a post-stretch resting period.
4.10.1 Peripheral hemodynamic responses during stretching. In the present study, we
hypothesized that skeletal muscle stretching would alter the oscillatory pattern (antegrade
vs. retrograde) of the upstream conduit artery blood flow. This hypothesis was based in
part on recent evidence demonstrating in artificial conditions (e.g. cuff occlusion) that
elevate downstream vascular resistance result in a corresponding increase in upstream
retrograde blood flow simultaneous to a decrease in mean blood flow and shear responses
(Padilla et al., 2010; Thijsen et al., 2009; Schreuder et al., 2014). During stretching in
each condition of the present study, the retrograde blood flow and shear profiles

89
increased significantly; however, the antegrade component increased in a similar fashion.
This resulted in no net change in mean blood flow and shear parameters. Somewhat
surprisingly there was no difference in the magnitude change of the oscillatory blood
flow and shear parameters between conditions. Previous evidence using cuff occlusion
(Thijsen et al., 2009; Schreuder et al., 2014) to artificially increase retrograde flow has
shown that the magnitude change in retrograde flow appears to play a predominating
factor in the overall net mean blood responses. As the level of downstream vascular
resistance increases as a result of increased cuff occlusion (Thijsen et al., 2009; Totosy et
al., 2014), the level of the upstream conduit artery retrograde flow increases simultaneous
to an overall decrease in net mean flow. However, in some instances (Schreuder et al.,
2014; Totosy et al., 2014) there is a significant rise in antegrade flow which can offset the
rise in retrograde flow, amounting to no net change in mean blood flow. Accordingly,
the present study found a similar response as previous authors (Schreuder et al., 2014;
Totosy et al., 2014) who used cuff occlusion.
At present it is somewhat difficult to interpret the present study findings and how
it may affect the vasculature. Shear stress is a potent stimulus for vascular endothelial
remodeling which, depending on the nature of oscillatory patterns can create either a
negative of positive effect on the vasculature (Cunningham and Gottlieb, 2005). Recent
evidence has demonstrated that changes in the contribution of nitric oxide (Padilla et al.,
2011) and alpha-adrenergic sympathetic nervous system (Casey et al., 2012) to vascular
tone contribute considerably to the magnitude change of retrograde shear rate during
downstream resistive conditions. Furthermore, augmented oscillatory shear and
retrograde shear resulting from increases in downstream vascular resistance (i.e. cuff

90
occlusion) reduce endothelial function via the flow mediated dilation technique in
humans in a dose-dependent manner (Thijssen et al., 2009). This test is considered a very
good estimate of endothelial nitric oxide dependent function (Thijssen et al., 2011).
Schreuder and colleagues (2014) further proposed that changes in vasoactive substance
may contribute to the development of endothelial dysfunction during prolonged exposure
to potentially harmful oscillatory shear patterns (e.g. retrograde shear) as a result of
downstream vascular resistance. Conversely, elevations in antegrade and overall mean
shear rate manifest to improve flow-mediated dilation (Tinken et al., 2009), and this
response is purported to induce an anti-atherogenic state on the vasculature at rest.
Totosy and colleagues (2014) suggested that since anterograde shear rate is considered to
be atheroprotective (Wang et al., 2013), acute increases in anterograde shear rate in the
presence of increased retrograde shear rate may confer additional cardio-protective
effects. Therefore, although an increase in retrograde was observed in the present study,
it is possible that the parallel increase in antegrade may offset any negative effect such
that there is no adverse effect on the endothelium. Even more this effect could serve as
an important mediator capable of improving vascular endothelial function. Future
research is therefore warranted to examine the impact of acute and chronic exposure to
levels of elevated retrograde and antegrade shear rate under physiological resistive
conditions (i.e. skeletal muscle stretching) to better understand the importance of shear
patterns in the development of endothelial function.
4.10.2 Peripheral hemodynamic responses after stretching. To our knowledge this is the
first investigation that has directly examined blood flow responses to skeletal muscle

91
stretching in humans. In the immediate off-transient (first 15 s) from stretching each
condition exhibited an overshoot in mean blood flow, shear and vascular conductance,
the magnitude of which, was intensity dependent. Furthermore, although mean blood
flow and shear responses began to decline shortly thereafter, these responses were still
elevated at 60s before returning to baseline for the remainder of the post-stretch rest
period. Currently there is no available evidence to compare to the present study findings
however; recent investigators (Groot et al., 2013; McDaniel et al., 2010; Trinity et al.,
2012; Wray et al., 2005; Mortenson et al., 2012) examining hemodynamic changes to
passive limb movement might offer some comparable measures. For instance, in the
present study the higher intensities of stretch resulted in an immediate (first 15s)
hyperemic response that was ~ 2.5 (in CAS) and ~ 3.2 (in CTS) times greater than
baseline, whereas LIS resulted in values that were ~ 1.4 times greater than baseline. This
is compared to previous evidence using passive limb movement of the thigh (Trinity et
al., 2012; Groot et al., 2013) demonstrating a hyperemic response ~ 1.3 times greater than
baseline in a similar (supine) position. Interestingly, though, the response nearly doubled
when passive limb movement was conducted in the upright position. We interpret our
results by suggestion that the intensity of LIS was similar to the intensity imposed on the
limbs during dynamic passive limb movement in the previous passive limb movement
studies, because similar acute hyperemic responses occurred. Furthermore, by increasing
the stretch intensity (i.e. from LIS to CAS and/or CTS) a more robust hyperemic response
occurs relative to passive limb movement. The differences in hyperemic responses as a
result of stretching and passive limb movement are likely demarcated by the dynamic
nature of the passive movement, which is a muscle pump-induced driven hyperemic

92
event versus the isometric nature of static stretching, which its hyperemic response is
explained by factors other than the muscle pump (see below discussion).
Another mechanism to explain the hyperemia seen after stretching may be related
to the mechanical compression of the musculature during passive stretch which would
then create a large hydrostatic pressure gradient between the microvasculature and its
upstream conduit artery. This circumstance may be illustrated as a form of active or
reactive hyperemia. In the case of reactive hyperemia a pneumatic blood pressure cuff is
wrapped around a limb and inflated to occlude some or all of blood flow thus, creating an
artificial level of downstream vascular resistance. As blood flow is impeded byproducts
of anaerobic metabolism become elevated simultaneous to an increase in hydrostatic
pressure. This two-fold effect essentially creates a large vasodilatation which, upon
release of compression, a large hyperemic response ensues – this response is dictated by
the length of time under occlusion, which is consistent with the notion that higher
accumulation of metabolites by ischemic tissue creates a larger and longer reactive
hyperemic response (Clifford et al., 2010). Therefore, based on the results of the present
investigation it is possible that through skeletal muscle stretching in humans, the
magnitude of the post-stretch hyperemic stimulus may be explained by the length of time
that the “metabolic stimulus” is spent in stretch as well as the intensity of stretch.
Unfortunately, this presumption, that a “metabolic signal” is involved in stretching, may
not explain the entire hyperemic response after stretching. Recent unpublished findings
from our laboratory have determined that a single stretch for 5 s is equally capable of
creating an immediate hyperemic response when compared to 4 min of stretch. These
preliminary findings are suggestive that a “mechanical” factor, namely an increased

93
hydrostatic gradient as a result of muscle stretch, most notably explains the immediate
hyperemic response. However, this response was only evident for 15 s before returning
to baseline by 60s which is opposite to present study findings demonstrating that mean
blood flow was still elevated at 60s after 4 min of stretching. Therefore, the adaptations
to a post-stretch hyperemic responses to skeletal muscle stretching in humans has a two-
fold effect: 1) that the initial overshoot in blood flow in the immediate off-transient is
likely due to a large hydrostatic gradient (mechanical hypothesis) which likely peaks
within a few cardiac cycles upon the release of stretch and 2) that the elevation in mean
blood flow for up to 60s after more prolonged stretching (4 min) is suggestive of
insufficient oxygenation (metabolic hypothesis) and therefore, is seen as an increase in
O2 delivery or blood flow.
Perhaps the most intriguing finding of the present investigation was that
retrograde blood flow and shear responses were attenuated following each stretching
sessions and these responses remained depressed at every time interval measured. The
reason for the decreases in retrograde may be the result of several notable mechanisms.
Firstly, muscle sympathetic nerve activity is known to be significantly attenuated after
stretching (Cui et al., 2006; Welsh and Segal, 1997), and this mechanism may have
allowed for arteriolar vasodilation to persist which may have resulted in the significant
elevation in blood volume responses. Indeed, our finding that [Hbtot] was elevated after
stretch provides an indirect indication that there was some level of arteriolar vasodilation
and reduced microvascular resistance after stretching. This reduced downstream vascular
resistance would then dampen the oscillatory nature of the upstream shear responses thus,
resulting in a reduction in retrograde parameters.

94
Lastly, central parameters of HR and BP may have played a factor in the
alteration in blood flow and shear patterns after stretching. In the present study HR was
significantly increased immediately after CAS and CTS conditions. However, the
increase in HR likely cannot explain the entire hyperemic response after stretching, as it
(in the CAS and CTS conditions) returned to baseline by 60s, whereas blood flow,
vascular conductance and shear responses were still significantly elevated at 60s
respectively. Furthermore, the reduced BP responses likely offset any central (HR)
mediated increase in blood flow after stretching.
4.10.3 Microvascular blood volume responses during stretching. Changes in [Hbtot]
reflect blood volume changes, which can be considered as an indirect measure of local
blood flow changes (Cardinale et al., 2007) through muscle vasodilation and overall
conductance of that vessel (Pereira et al., 2006). In the present study, [Hbtot] slowly
increased during constant angle stretching conditions (CAS and LIS) whereas CTS
remained unchanged. Previous evidence from animal studies has reported that muscle
blood flow decreases when sarcomere length is increased beyond physiological values
(Poole et al., 1997; Kindig & Poole, 1999). These findings in animals have led to the
current perspective that skeletal muscle stretching causes a transient reduction in blood
flow in humans (Sands et al., 2013). However, contrary to previous animal evidence the
findings of the present study suggest that skeletal muscle stretching in humans does not
decrease microvascular blood flow. Moreover the direct assessment of blood flow via
ultrasound Doppler at the conduit popliteal artery in the present study confirms our

95
microvascular results because mean blood flow did not decrease (or increase) during each
stretching condition.
At present we cannot fully explain the discrepancies in present study finding to
other animal research. One reason may be due to the fact that NIRS does not directly
measure microcapillary blood flow kinetics; rather, this method provides an indirect
assessment of blood flow changes at the site of interest (Cardinale et al., 2007). Another
possible reason is that stretching of an isolated animal preparation results in a different
physiological environment, which may allow for the muscle to be stretched beyond the
limitations that can be imposed in humans. Capillaries are tethered to the adjacent
connective tissue matrix, which are connected to myofibrils. When the sarcomeres are
lengthened this will also cause the capillaries to be extended. This kinetic sequence of
events (i.e. skeletal muscle-to-capillary) causes the tortuous arrangement of microvessels
to be increased in such a way that the luminal diameters become temporary reduced
(Poole & Mathieu-Costello, 1992; Nakao & Segal; 1995). Such reductions in luminal
diameter and subsequent blood flow may be dictated by the level of the intensity of the
stretch. Indeed this notion was described by Poole et al (1997), where authors found a
biphasic pattern with regard to capillary blood flow kinetics and muscle lengthening such
that initial lengthening of a sarcomere within physiological values (i.e. 2.7 µm) resulted
in no appreciable changes in blood flow, but when the sarcomere was further lengthened
beyond physiological ranges (i.e. 3.3 µm), a dramatic decrease in blood flow ensued.
Thus, the level of the intensity of muscle stretch may dictate how red blood cells are
perfused in the microcapillary bed, which may be represented as alterations in blood
volume distribution, as seen in the present study. Based on this information and the

96
present study findings it might be suggested that skeletal muscle stretching in humans
cannot reach a lengthening threshold and therefore, does alter microcapillary blood
volume.
Intramuscular pressure was not measured in this study; however, the
disproportionate findings in [Hbtot] between different intensities of stretch (constant angle
versus constant torque) raise the possibility that IMP may play a causal role in altering
the microvasculature and its blood volume distribution during stretch. The initial work
by McCully (2010), who first found that stretching in humans creates a transient
reduction in muscle oxygenation using NIRS, suggested that higher IMP may reduce
muscle blood flow by occluding blood vessels (i.e. arterioles and venules) due to a
shearing effect, especially at the distal portion (where our NIRS probe was positioned) of
muscles where greater pennation angles (i.e. gastrocnemius medialis, vastus lateralis) and
IMPs are seen (Sejerstad et al., 1984; Naamani et al., 1995; Miura et al., 2004). There is
credible evidence to support this hypothesis, as it is well known that IMP can be
increased to such an extent that some or all of the blood flow can be significantly
impeded at the microvascular level during isometric contractions (Ameredes and
Provenzano, 1997; Sejersted et al., 1984; Kirkebo and Wisnes, 1982) and static stretching
positions (Davis et al., 2003; Jenkyn et al., 2002) potentially as result of compressive
forces. These compressive forces during stretching may cause some level of venous
and/or or arterial congestion to occur resulting in alterations of blood volume. Thus, the
intensity and duration of muscle stretching may play a critical factor for compressive
forces to act upon the arterial or venous end of microcirculation. This would then alter

97
how blood volume is distributed within the microvasculature, as evidenced in the present
study.
Of further important note, the viscoelastic creep phenomenon may have played an
important role in how compressive forces control blood flow as a result of stretch. As
previously mentioned viscoelastic creep can cause a transient reduction in passive torque
during the time course of a constant angle stretch. Due to the fact that passive torque
declined by as much as 35 – 40 % during constant angle stretching sessions in the present
study, the dramatic decrease in passive resistance may have resulted in similar reductions
in IMP which may have allowed for some arterial inflow to occur while venous
congestion was maintained. This could explain the small but significant elevations in
[Hbtot] seen after 60 s during CAS and LIS conditions. Alternatively, the consistent
passive torque applied during the CTS session may have created a level of arteriolar
congestion which may have reduced the ability for the [Hbtot] signal to increase.
Lastly, it should be noted that the NIRS sensor used in the present study is only
capable of penetrating to a tissue depth of ~ 2 cm. Indeed, IMP can be significantly
increased at greater muscle tissue depths (Davis et al., 2003; Jenkyn et al., 2002) which
may create for larger changes in microvasculature blood volume displacement.
Nevertheless, we were able to find small but significant changes in blood volume in the
presents study and therefore, it is likely that greater differences in blood volume would be
observed at greater muscle tissue depths. Taken together, or findings suggest that the
mechanical event of stretching over a broad range of muscle lengths in humans increases
microvascular resistance via changes in NIRS-blood volume, and that these alterations
may be the result of venous and/or arterial congestion.

98
4.10.4 Microvascular oxygenation responses during stretching. The NIRS-derived HHb
signal can be considered to represent the relative matching between O2 delivery and O2
utilization at the site of interest and hence, skeletal muscle oxygen consumption
irrespective of blood volume changes (Pereira et al., 2007). In the present study, the %
∆[HHb] dramatically increased in all stretching conditions. Furthermore, these changes
became intensity dependent meaning that, the higher stretch intensities elicited greater
elevations in O2 extraction. These findings extend previous findings from our laboratory
(Kruse and Scheuermann, 2014) and others (McCully, 2010; Otsuki et al., 2011)
indicating that skeletal muscle stretching in humans can increase microvascular metabolic
(i.e. increased HHb) demand.
The mechanisms for the alterations in muscle oxygenation patterns seen in the
present study and others (McCully, 2010; Otsuki et al., 2011) currently remain unknown.
As previously suggested, IMP could be increased to such an extent that some level of
venous and/or arterial congestion occurs. Indeed, the differences in [Hbtot] values
provide an indirect line of evidence to support this notion since the different stretching
intensities elicited different changes in blood volume. Therefore, the inability to augment
venous outflow during stretching within the microvasculature will alter the balance
between arterial inflow versus venous outflow – this will then create a relative mismatch
between O2 delivery and O2 utilization which subsequently, results in the elevation of %
∆ [HHb], as seen in the present study.
It is also possible that skeletal muscle stretching causes an increase in metabolic
rate. For example, there is convincing evidence from animal experiments observing that

99
despite a lack of sarcolemma depolarization or cross-bridge cycling, a passively stretched
muscle can be metabolically active, as observed through increases in oxygen
consumption and heat production (Feng, 1932; Barnes, 1987), carbon dioxide production
(Eddy & Downs, 1921), glycogen utilization (Barnes & Worrell, 1985), blood glucose
uptake (Chambers et al., 2009) and phosphocreatine (PCr) breakdown (Barnes & Worrell,
1985). Therefore, whether skeletal muscle stretching in humans increases metabolic rate
or whether some level of mechanically induced venous/arterial congestion contributes to
the associated increases in oxygen extraction of the present study remain unclear. Taken
together our results indicate that skeletal muscle stretching in humans can substantially
decrease muscle oxygenation and that this result is presumed to manifest from
mechanical and/or a metabolic factors.
4.10.5 Microvascular blood volume ([Hbtot]) responses after stretching. Consistent with
previous findings from our laboratory (Kruse and Scheuermann, 2014), [Hbtot] was
elevated after stretching however, by providing a closer time domain analysis (15s) after
stretching, this enabled us to capture the immediate off-transient nature of blood volume
within the microvasculature. As such we found an immediate overshoot followed by
steady decline in blood volume, but this still remained above baseline for up 10 min after
stretching. Furthermore, these responses were intensity dependent, as the two higher
intensities of muscle stretching (CAS and CTS) exhibited the greatest overshoot
immediately (Post-15s) after the stretch as compared to LIS condition.
At present, there is no clear interpretation for our study findings however, the
hypothesis that skeletal muscle stretching in humans increases metabolism may fit well

100
when understanding the primary mechanism responsible for the sustained elevation in
microvascular blood volume after stretching. Along these lines, in the present study, we
found that skeletal muscle stretching creates a significant rise in muscle oxygen
extraction (i.e. % ∆HHb]), thus leading to the assumption that stretching increases muscle
metabolism. Furthermore, there is substantial evidence to show, at least in animals, that
skeletal muscle stretching increases muscle metabolism (Chamber et al., 2009; Barnes,
1987; Barnes and Worrel, 1985; Feng, 1932) and that increased levels of local vasoactive
metabolites, such as K+ and H
+ and/or endothelial factors (MacDonald et al., 2001) by
ischemic tissue can create large reactive hyperemic responses (Clifford et al., 2010).
Therefore, it is possible that the sustained microvascular post-stretch hyperemic
responses may be associated with release of local vasoactive metabolites during
stretching which allows for a more coordinated distribution of blood flow to deliver more
blood flow to metabolically active sites. In summary, our findings provide supporting
evidence for a post-stretch hyperemia at the microvascular level and that this response
may be a marker to indicate a change in O2 delivery and O2 utilization during stretching.
4.10.6 Central hemodynamic responses during stretching. During stretching, HR
immediately (15 s) increased in each condition whereas the length of time that HR
remained elevated depended on the level of intensity of the stretch. For example, in the
constant angle stretching conditions, HR returned to baseline by 60 s (LIS) and 150 s
(CAS), whereas CTS showed a similar but sustained increase in HR throughout the
entirety of the stretch. The reasons for the differences in HR responses remain unclear;
however, the roles of stretch/tension mechanoreceptors are well understood to play a

101
critical factor in HR responses, especially at the onset of stretch or exercise (McCloskey
and Mitchell, 1972; Gladwell and Coote, 2002). Gladwell and Coote (2002)
demonstrated a potential role for stretch sensitive mechanoreceptors at the onset of
muscle stretch in humans by finding a significant increase in HR (5 ± 3 bpm) during 60 s
of constant angle stretching of the triceps surae muscle group. Our findings add credence
to these previous findings as we found similar increases in HR (~ 5-6 bpm) during each
stretch condition examined. In addition, by extending the time interval for the stretch
beyond 60 s, we were able to determine the time course changes in HR responses during
varying levels of muscle stretch.
The disparate findings in HR over time in each condition also raise the possibility
that viscoelastic creep could have played a role in the activation of mechanoreceptors
initiated by muscle stretching. For example, both constant angle stretching sessions
(CAS and LIS) resulted in a 35 - 40 % reduction in passive torque across 4 min of
stretching. During this time frame HR was not sustained above resting baseline levels for
the entire length of the stretch duration. However in the CTS session, where the passive
torque was consistently held at a moderate intensity during the entirety of the stretch, HR
was increased at every time interval. By placing the tension “constant” on the plantar
flexors it is possible that the stretch/tension sensitive mechanoreceptors during CTS were
continuously activated during 4 min of stretching which may have caused HR responses
to be similarly increased.
On the basis of the known discharge characteristics of mechanoreceptive afferent
fibers (Adreani and Kaufman, 1998, Kaufman et al., 1984), it is conceivable that some
fibers may have adapted to the stretch stimulus during such stretch periods (Drew et al.,

102
2008). This would tend to reduce the level of afferent feedback which would then serve
to decrease HR back to baseline. However, since an increase in HR was observed at
every time interval during the CTS condition, the results of the present study suggests
that this adaption did not occur. If there was a reduction in mechanoreceptor afferent
activity due to a conditioning affect, then a coinciding decrease in HR would be expected
during the CTS condition. From another perspective, HR may have been elevated due to
the polymodal properties that mechanoreceptive afferents are known to possess (Adreani
and Kaufman, 1998). Indeed reactivation of the mechanoreceptive afferents has been
demonstrated after their initial burst of firing due to a “metabolite sensitization” and
consequently restoring their modulatory input (Cui et al., 2008; Drew et al., 2008;
Adreani and Kaufman, 1998). In the present study, we found a transient elevation in %
∆[HHb], a finding which would indicate that byproducts of anaerobic metabolism
accumulated during stretch. However, as % ∆[HHb] progressively increased, HR fell
back to baseline, at least in the constant angle stretching sessions. Therefore, based on
the present study findings and assuming that mechanoreceptive afferents are the
predominating factor in initiating HR responses, it can be concluded that any metabolic
accumulation during stretching does not play a significant role in mediating HR
responses rather; it might be assumed that a critical tension must be applied, and held, to
provoke a mechanoreceptive mediated increase in HR responses during muscle stretch in
humans.
4.10.7 Central hemodynamic responses after stretching. Following stretching in the
CAS condition HR immediately increased and returned to baseline by 60 s while DBP

103
and MAP pressure immediately decreased and remained decreased for the remainder of
the post-stretch time period. The primary reason for this response appears likely due to
the baroreflex. The baroreflex is a well-known phenomenon governed by changes tin
HR, BP and total vascular conductance. Typically, changes in HR occur on a beat-to-
beat basis with the greatest change occurring early in the recovery period (from exercise
or cuff occlusion) whereas total vascular conductance plays a larger role in mediating a
baroreflex at a later time point (i.e. ~ 8-10 s) (Raven et al., 2006; Fadel, 2008).
Therefore, the large increase in vascular conductance immediately following (first 15 s)
CAS in the present study, likely caused a temporary drop in total peripheral resistance as
highlighted by decreases in DBP and MAP (Table 4.2) which then initiated a baroreflex
mediated increase in HR to sustain blood flow and perfusion. These findings are also
supported by the non-significant findings in BP during the LIS condition where vascular
conductance in the immediate off-transit from stretching reached only ~ 20 % of what the
CTS and CAS responses elicited. The lower magnitude in vascular conductance likely
was not sufficient to cause a significant drop in total peripheral resistance to such an
extent that would trigger a baroreflex response. Furthermore, the LIS condition confirms
that the HR increases after stretching in the CAS condition is not likely explained by a
“startle reflex,” as no changes in HR were evident in this condition. Nevertheless, we
carefully checked cyclical breathing patterns in order to eliminate any ventilation induced
influence in hemodynamic changes as a result of the on- and off-stretch transitions.
Therefore, based on the above evidence a baroreflex mediated increase in HR driven by
the magnitude change in vascular conductance, at least during higher intensity stretching

104
(i.e. CAS and CTS), is the most likely candidate to explain central hemodynamic
responses after stretch.
4.10.8 Limitations. The present study is not without a few limitations. Firstly, the
results of the present study can only be extrapolated to healthy young males. However,
due to the low intensity nature of skeletal muscle stretching it would be relatively easy to
incorporate this stretching protocol in a variety of other populations. Thus, future
research is warranted in other population that may possess differences in blood flow
distribution (i.e. females, aging and disease populations) to assess the impact of passive
stretch on hemodynamic responses. In the present study we could not employ a
quantitatively consistent stretching intensity for the reference session (CAS) because it is
not possible to “maximize” passive torque. Instead, the passive torque on the plantar
flexors was to a point that was perceived as “moderate discomfort” for each subject.
Clearly this intensity can be subjective between subjects which may explain the large
standard deviations in hemodynamic responses. Nevertheless, the hemodynamic
responses were consistent within and between subjects which allowed for statistical
significances to persist. Furthermore, the diameter of the popliteal artery was unchanged
during or after a single 4 min stretch (CAS) of the plantar flexors relative to baseline,
thus adding further credibility to the significance of our findings. In the present study an
anticipatory response or startle reflex may have confounded the HR responses during the
on- and off-transitions from stretch; however, we made every precautionary measure to
eliminate this. For example the rate of rotation on the Biodex was 10º/s, which is slow
enough to eliminate the stretch reflex. Furthermore, to avoid a startle reflex and active

105
resistance to the passive movement as well as an anticipatory response, subjects were not
informed of exactly when the stretch would initiate but only made aware at a random
time point within a 60 s window prior to the onset of stretch. Additionally, there is
convincing research demonstrating that despite the presence of arousal as presented by
increases in ventilatory responses during passive limb movement, this phenomenon does
not play a significant role in altering central or peripheral hemodynamic responses
(Venturelli et al., 2012). Lastly, stretching of the gastrocnemius medialis muscle is
presumed to be the predominant muscle eliciting the cardiovascular responses. Indeed, as
an agonist muscle is being stretched its antagonist muscle group is simultaneously
shortening. Thus, the shortening of tibialis anterior muscle, which its blood flow is also a
fed by the popliteal artery, may contribute to some discrepancies in hemodynamic
responses. However, we do not know of a vessel that does not feed an agonist/antagonist
muscle pair.
4.11 Conclusions
The data acquired from this investigation has examined and verified a critical role
for skeletal muscle stretching on cardiovascular responses. Regardless of intensity, when
the muscle is passively stretched mean blood flow and shear responses do not change;
however, the antegrade and retrograde blood flow and shear responses are dramatically
altered. Central hemodynamic increases in HR during varying levels of stretch may be
related to mechanoreceptor afferent feedback arising from the musculature and these
responses appear to have a stretch/tension threshold initiating these HR responses. Upon
release of the stretch a large hyperemic response ensues and this response is dependent on

106
the intensity of the stretch. Although we are not able to differentiate a specific
mechanism to explain the hyperemic response, it can be assumed that alterations in
NIRS-derived microvascular parameters, which reveal patterns of downstream vascular
resistance, regulate how the upstream conduit artery blood flow/shear profiles are
manifested. Lastly, stretching at a higher intensity decreases BP and retrograde responses
(afterward), a finding that may suggest that skeletal muscle stretching in humans results
in a lower level of myogenic tone at rest. Collectively, these findings are interpreted to
suggest that higher stretching intensities (CAS and CTS) elicit the most favorable
cardiovascular adaptations, especially after a stretching session.

107
Chapter 5
General conclusions, implications and future directions
One common assumption regarding skeletal muscle stretching in humans is that,
when done statically, it can create a transient reduction in blood flow and muscle
oxygenation. Yet, these assumptions are based on no current empirical evidence
examining the cardiovascular responses to stretching in humans and, at best, these
presumptions have been made exclusively in animal investigations. Thus, the purpose of
this dissertation was to translate the available animal evidence into a practical human
model by directly examining whether skeletal muscle stretching in humans does indeed
create cardiovascular alterations. Such findings could pave the path toward the
incorporation of alternative therapeutic strategies in counteracting a variety of disease
states including but are not limited to, individuals with peripheral arterial disease, pre-
and post- diabetics and disuse muscular dystrophy. Stretching is considered as a low
intensity form of exercise and fitness and therefore, if beneficial cardiovascular effects
can be derived as result of stretching, this treatment could be effectively incorporated into
virtually every type of clinical and rehabilitation setting.
In first study (Chapter 3) of this dissertation we investigated skeletal muscle
stretching in humans and its effect on NIRS-derived measures in oxygenation and blood

108
volume parameters. In this study it was demonstrated that a single bout of stretching on
the plantar flexors resulted in: 1) a transient increase in muscle oxygen consumption but
microvascular blood volume from the NIRS signal was not significantly impeded, and 2)
a significant increase in muscle blood volume after stretching, thus providing novel
evidence for a “post-stretch hyperemia.” This is the first study to exclusively
demonstrate in humans that skeletal muscle stretching without the use of intermittent
isometric contraction can decreases muscular oxygenation in a dose response time-
dependent manner. Furthermore, this is the first time in humans that an increase in
microvascular blood volume was found after stretching, a finding that may otherwise
imply that skeletal muscle stretching in humans creates a significant hyperemic event.
In the second study (Chapter 4) of this dissertation we extended our previous
study’s findings (Study I) by directly assessing blood flow parameters at the conduit
artery level using ultrasound Doppler while simultaneously examining NIRS-derived
muscle oxygenation and blood volume parameters of the microvasculature during 4 min
of plantar flexor stretching. We further examined how central hemodynamic parameters
of heart rate and blood pressure could play an important role in controlling these
peripheral responses at the macro and microvascular level. By employing three different
stretching intensities we were able to specifically examine how physiological levels of
downstream microvascular resistance may control the oscillatory nature of blood flow
and shear responses. To this end we demonstrated that skeletal muscle stretching in
humans: 1) does not decrease macro or microvascular blood flow as previous animal
evidence has found however; the biphasic nature of PA conduit blood flow/shear profiles
(retrograde vs. antegrade) are altered, 2) causes an acute post-stretch hyperemic response

109
at the macro and microvascular level that is intensity dependent, 3) decreases systemic
blood pressure (afterward), and 4) reduces resting retrograde blood flow and shear stress
after stretch. Collectively, the work in this dissertation has enhanced current knowledge
regarding skeletal muscle stretching and changes in cardiovascular outcomes. The
implications for these findings seem quite substantial and future research is needed to
fully elucidate the potential mechanisms involved with stretching and its cardiovascular
outcomes.
5.1 Future research directions
Our discovery that stretching can have a profound impact on elevating blood flow
and altering the oscillatory nature of these responses could have important clinical
implications, especially when examining its effect on the vascular endothelium. Because
we did not directly assess the impact of blood flow and shear indices on endothelial
function within the present dissertation the next question that future research should
address is: Does passive stretch enhance endothelium-dependent vasodilation,
contributing to increased skeletal muscle blood flow? There are at least two directions to
approach this question which can be based on the knowledge gained from the present
dissertation findings as well as previous animal evidence. Due to the robust hyperemic
response seen when the stretch is released, it might be suggested that multiple cycles of
ischemia followed by reperfusion as a result of stretch might serve to directly impact the
vascular endothelium. Indeed it is well known that when the vascular endothelium is
consistently exposed to high shear stress over a prolonged period of time,
mechanotransduction signaling alters smooth muscle function which subsequently causes

110
vasodilation. Therefore, it is possible that a long term stretching program, which creates
consistent elevations in shear stress, may directly alter vascular remodeling and
consequently vascular function. On the other hand, it is possible that skeletal muscle
stretch directly impacts the microvasculature by altering (i.e. decreasing) the tortuous
arrangement of the microcapillary bed which may serve to reduce downstream vascular
resistance. This presumption is met by the well-known fact that increased capillary
tortuosity increases vascular resistance (Hughes et al., 2007). Therefore, to potentially
alter the tortuous arrangement of the capillary bed in humans another approach would be
to employ a program of daily ankle dorsiflexion stretching/splinting for 10-30 min daily
for several weeks. In doing so this might serve to chronically decrease tortuosity,
decrease microvascular resistance and decrease myogenic tone. This could then improve
endothelium-dependent vasodilation of the conduit artery thereby providing direct
evidence in support that stretch training is viable means to improve the vasculature.

111
5.2 References
Adreani CM, Hill JM, Kaufman MP (1997). Responses of group III and IV muscle
afferents to dynamic exercise. J Appl Physiol 82, 1811–1817.
Adreani CM & Kaufman MP (1998). Effect of arterial occlusion on responses of
group III and IV afferents to dynamic exercise. J Appl Physiol 84, 1827–1833.
Alam M & Smirk FH (1938). Observations in man on a pulse-accelerating reflex
from the voluntary muscles of the legs. J Physiol 92, 167–177.
Alam M & Smirk FH (1937). Observations in man upon a blood pressure raising
reflex arising from the voluntary muscles. J Physiol 89, 372–383.
Ameredes BT & Provenzano MA (1997). Regional intramuscular pressure
development and fatigue in the canine gastrocnemius muscle in situ. J Appl Physiol
83, 1867–1876.
Amann M &Dempsey JA (2008). Locomotor muscle fatigue modifies central motor
drive in healthy humans and imposes a limitation to exercise performance. J Physiol
586, 161–173
Anderson KM & Faber JE (1991). Differential sensitivity of arteriolar α1- and α2-
adrenoceptor constriction to metabolic inhibition during rat skeletal muscle
contraction. Circ Res 69, 178–184.
Armstrong, RB, MD, Delp, EF, Goljan, and MH Laughlin (1987). Distribution of
blood flow in muscles of miniature swine during exercise. J Appl Physiol 62, 1285–
1298.
Armstrong RB, Duan C, Delp MD, Hayes DA, Glenn GM, Allen GD (1993).
Elevations in rat soleus muscle [Ca2] with passive stretch. J Appl Physiol 74, 2990-
2997.
Avela J, Kyrolainen H, Komi PV (1999). Altered reflex sensitivity after repeated and
prolonged passive muscle stretching. J Appl Physiol 86, 1283-1291.
Bakker W, Eringa EC, Sipkema P, van Hinsbergh VW (2009). Endothelial
dysfunction and diabetes: roles of hyperglycemia, impaired insulin signaling and
obesity. Cell Tissue Res 1, 165-89.
Balog EM (2010). Excitation-contraction coupling and minor triadic proteins in low-
frequency fatigue. Exerc Sport Sci Rev 38, 135–142.
Baum K, Selle K, Leyk D, Essfeld D (1995). Comparison of blood pressure and heart
rate responses to isometric exercise and passive muscle stretch in humans Eur J Appl
Physiol 70, 240–245.

112
Barnes WS (1987). Respiration and lactate production in isolated frog skeletal
muscle: effects of passive stretch. Comp Biochem Physiol 86, 229-232.
Barnes WS & Worrel GA (1985). Glycogen utilization in isolated frog muscle: an
effect of passive mechanical stretch. Comp Biochem Physiol 81, 243-256.
Behm DG, Chaouachi A (2011) A review of the acute effects of static and dynamic
stretching on performance. Eur J Appl Physiol 111(11):2633–2651
Behm DG, Kibele A (2007). Effects of differing intensities of static stretching on
jump performance. Eur J Appl Physiol 101, 587–594.
Bevegard BS & Shepherd JT (1966). Circulatory effects of stimulating the carotid
arterial stretch receptors in man at rest and during exercise. J Clin Invest 45, 132–42.
Borg TK & Caulfield JB (1980). Morphology of connective tissue in skeletal muscle.
Tissue Cell 12, 197–207.
Boushel R (1998). Metabolic control of muscle blood flow during exercise in
humans. Can J Appl Physiol 28, 754–773.
Brooks GA, Fahey TD, Baldwin KM (2005). Exercise Physiology: Human
Bioenergetics And It's Aplication. New York, McGraw-Hill 4th
Ed.
Buckwalter JB & Clifford PS (2001). The paradox of sympathetic vasoconstriction in
exercising skeletal muscle. Exerc Sport Sci Rev 29, 159–163.
Buckwalter JB, Mueller PJ, Clifford PS (1997). Autonomic control of skeletal muscle
vasodilation during exercise. J Appl Physiol 83, 2037–2042.
Cardinale M, Ferrari M, Quaresima V (2007). Gastrocnemius medialis and vastus
lateralis oxygenation during whole-body vibration exercise. Med Sci Sports Exerc 39,
694–700.
Cartee GD, Douen AG, Ramlal T, Klip A, Holloszy, JO (1991). Stimulation of
glucose transport in skeletal muscle by hypoxia. J Appl Physiol 70, 1593-1600.
Casey DP, Padilla J, Joyner MJ (2012). α-adrenergic vasoconstriction contributes to
the age-related increase in conduit artery retrograde and oscillatory shear.
Hypertension 60, 1016-22.
Casey DP, Shepherd JR, Joyner MJ (2014). Sex and vasodilator responses to hypoxia
at rest and during exercise. J Appl Physiol 116, 927-36.
Chambers MA, Moylan JS, Smith JD, Goodyear LJ, & Reid MB (2009). Stretch-
stimulated glucose uptake in skeletal muscle is mediated by reactive oxygen species
and p38 MAP-kinase. J Physiol 587, 3363-3373.

113
Cicchetti DV (1994). Guidelines, criteria, and rules of thumb for evaluating normed
and standardized assessment instruments in psychology. Psychological Assessment 6,
284–290.
Clifford PS, Jasperse JL, Shoemaker JK (2010). Limb position affects magnitude of
reactive hyperemia. FASEB J 24, 804.12.
Clifford PS, Kluess HA, Hamann JJ, Buckwalter JB, and Jasperse JL (2006).
Mechanical compression elicits vasodilatation in skeletal muscle feed arteries. J
Physiol 572, 561–567.
Clinch, NF. (1968). On the increase in rate of heat production caused by stretch in
frog’s skeletal muscle. J. Physiol 196, 397-414.
Cramer JT, Housh TJ, Weir JP, Johnson GO, Coburn JW, Beck, TW (2005) The
acute effects of static stretching on peak torque, mean power output,
electromyography, and mechanomyography. Eur J Appl Physiol 93(5–6):530–539.
Crecelius AR, Kirby BS, Richards JC, Garcia LJ, Voyles WF, Larson DG, Luckasen
GJ & Dinenno FA (2011). Mechanisms of ATP-mediated vasodilation in humans:
modest role for nitric oxide and vasodilating prostaglandins. Am J Physiol Heart Circ
Physiol 301, H1302–H1310.
Cui J, Blaha C, Moradkhan R, Gray KS, Sinoway LI (2006). Muscle sympathetic
nerve activity responses to dynamic passive muscle stretch in humans. J Physiol 15,
576(Pt 2), 625-34.
Cui J, Mascarenhas V, Moradkhan R, Blaha C, Sinoway LI (2008). Effects of muscle
metabolites on responses of muscle sympathetic nerve activity to mechanoreceptor(s)
stimulation in healthy humans. Am J Physiol Regul Integr Comp Physiol 294, R458-
66.
Cunningham KS, Gotlieb AI (2005). The role of shear stress in the pathogenesis of
atherosclerosis. Lab Invest 85, 9-23.
Davies PF (1995). Flow-mediated endothelial mechanotransduction. Physiol Rev 75,
519-60.
Davis J, Kaufman KR, Lieber RL (2003). Correlation between active and passive
isometric force and intramuscular pressure in the isolated rabbit tibialis anterior
muscle. J Biomech 36, 505-12.
Decoster LC, Cleland J, Altieri C, Russell, P (2005). The effects of hamstring
stretching on range of motion: a systematic literature review. J Ortho Sport Physical
Ther 35, 377-387.

114
Delorey DS, Kowalchuk JM, Paterson DH (2003). The relationship between O2
uptake kinetics and muscle deoxygenation during moderate-intensity exercise. J Appl
Physiol 95, 113–120.
Delp MD, Laughlin MH (1998). Regulation of skeletal muscle perfusion during
exercise. Acta Physiol Scand 162, 411–419.
De-Ruiter CJ Goudsmit FA Van-Tricht JA De-Haan A (2007). The isometric torque
at which knee-extensor muscle reoxygenation stops. Med Sci Sports Exerc 3, 443-
452.
Dewhirst E, Corridore M, Klamar J, Beebe A, Rice J, Barry N, Tobias JD (2013).
Accuracy of the CNAP monitor, a noninvasive continuous blood pressure device, in
providing beat-to-beat blood pressure readings in the prone position. J Clin Anesth
25, 309-13.
Dinenno FA & Joyner MJ (2003). Blunted sympathetic vasoconstriction in
contracting skeletal muscle of healthy humans: is nitric oxide obligatory? J Physiol
553, 281–292.
Downs ME, Hackney KJ, Martin D, Caine TL, Cunningham D, O'Connor DP, Ploutz-
Snyder LL (2014). Acute vascular and cardiovascular responses to blood flow-
restricted exercise. Med Sci Sports Exerc 46, 1489-97.
Drew RC, Bell MPD, White MJ (2008). Modulation of spontaneous baroreflex
control of heart rate and indexes of vagal tone by passive calf muscle stretch during
graded metaboreflex activation in humans. J Appl Physiol 104, 716-723.
Driss T, Vandewalle H (2013). The Measurement of Maximal (Anaerobic) Power
Output on a Cycle Ergometer: A Critical Review. BioMed Res Inter 1-40.
Dyke CK, Dietz NM, Lennon RL, Warner DO, and Joyner MJ (1998). Forearm blood
flow responses to handgripping after local neuromuscular blockade. J Appl Physiol
84, 754–758.
Eddy NB, Downs AW (1921). Extensibility of muscle: the production of carbon
dioxide by a muscle when it is made to support a weight. Amer J Physiol 56, 188-
195.
Ellis CG, Mathieu-Costello O, Potter RF, MacDonald IC, Groom AC (1990). Effect
of sarcomere length on total capillary length in skeletal muscle: In vivo evidence for
longitudinal stretching of capillaries. Microvasc Res 40, 63–72.
Ernst E. (1963). Biophysics of the Striated Muscle, 2nd edn., pp. 239-241. Budapest:
Hungarian Academy of Sciences.
Ernsting J, Parry DJ (1957). Some observations of the effects of stimulating the
stretch receptors in the carotid artery in man. J Physiol 137, 454P–6P.

115
Fadel PJ (2008). Arterial baroreflex control of the peripheral vasculature in humans:
rest and exercise. Med Sci Sports Exerc 40, 2055-62.
Fadel PJ, Keller DM, Watanabe H, Raven PD, Thomas GD (2004). Noninvasive
assessment of sympathetic vasoconstriction in human and rodent skeletal muscle
using near-infrared spectroscopy and Doppler ultrasound. J Appl Phyisol 96, 1323–
1330.
Fadel PJ, Ogoh S, Keller DM, Raven PB (2003). Recent insights into carotid
baroreflex function in humans using the variable pressure neck chamber. Exp Physiol
88, 671-80.
Feng TP (1932) The effect of length on the resting metabolism of muscle. J Physiol
(Lond) 74, 441–454.
Ferreira LF, Harper AJ, Townsend DK, Lutjemeier BJ, Barstow TJ (2005). Kinetics
of estimated muscle capillary blood flow during recovery from exercise. Exp Physiol
90, 715–726.
Fisher JP, Bell MPD, White MJ (2005). Cardiovascular responses to human calf
muscle stretch during varying levels of muscle metaboreflex activation. Exp Physiol
90, 773–781.
Freyschuss, U. (1970). Cardiovascular adjustment of somatomotor activation. Acta
Physiologica Scandinavica 342, suppl. 1, 1–63.
Fowles JR, Sale DG, MacDougall JD (2000). Reduced strength after passive stretch
of the human plantar flexors. J Appl Physiol 90, 1179-88.
Gajdosik RL (2003). Passive extensibility of skeletal muscle: review of the literature
with clinical implications. Clin Biomech 16, 87-101.
Gajdosik RL, Allred JD, Gabbert HL, Sonsteng BA (2007). A stretching program
increases the dynamic passive length and passive resistive properties of the calf
muscle-tendon unit of unconditioned younger women. Eur J Appl Physiol 99, 449-54.
Gill RW (1979). Pulsed Doppler with B-mode imaging for quantitative blood flow
measurement. Ultrasound Med Biol 5, 223–35.
Gladwell VF & Coote JH (2002). Heart rate at the onset of muscle contraction and
during passive muscle stretch in humans: a role for mechanoreceptors. J Physiol 540,
1095–1102.
Gladwell VF, Fletcher J, Patel N, Elvidge LJ, Lloyd D, Chowdhary S, Coote JH
(2005). The influence of small fibre muscle mechanoreceptors on the cardiac vagus in
humans. J Physiol 567, 713–721.

116
Gonzalez-Alonso J, Mortensen SP, Jeppesen TD, Ali L, Barker H, Damsgaard R,
Secher NH, Dawson EA & Dufour SP (2008). Haemodynamic responses to exercise,
ATP infusion and thigh compression in humans: insight into the role of muscle
mechanisms on cardiovascular function. J Physiol 586, 2405–2417.
Gonzales JU, Thompson BC, Thistlethwaite JR, Harper AJ, Scheuermann BW
(2013). Forearm blood flow follows work rate during submaximal dynamic forearm
exercise independent of sex. J Appl Physiol 103, 1950-7.
Grassi B, Pogliaghi S, Rampichini S. et al (2003). Muscle oxygenation and
pulmonary gas exchange kinetics during cycling exercise on-transitions in humans. J
Appl Physiol 95, 149–158.
Groot HJ, Trinity JD, Layec G, Rossman MJ, Ives SJ, Richardson RS (2013).
Perfusion pressure and movement-induced hyperemia: evidence of limited vascular
function and vasodilatory reserve with age. Am J Physiol Heart Circ Physiol 304,
H610-9.
Haddy FJ & Scott JB. (1968). Metabolically linked vasoactive chemicals in local
regulation of blood flow. Physiol Rev 48, 688-707.
Hamann JJ, Buckwalter JB, and Clifford PS (2004). Vasodilatation is obligatory for
contraction-induced hyperaemia in canine skeletal muscle. J Physiol 557, 1013–1020.
Harper AJ, Ferreira LF, Lutjemeier BJ, Townsend DK, Barstow TJ (2008). Matching
of blood flow to metabolic rate during recovery from moderate exercise in humans.
Exp Physiol 10, 1118-25.
Harris EJ (1954). An effect of stretch upon the sodium output from frog muscle. J.
Physiol. 124, 242-247.
Hellsten Y, Rufener N, Nielsen JJ, Hoier B, Krustrup P & Bangsbo J (2008). Passive
leg movement enhances interstitial VEGF protein, endothelial cell proliferation, and
NOS mRNA content in human skeletal muscle. Am J Physiol Regulatory Integrative
Comp Physiol 294, R975–982.
Herr MD, Imadojemu V, Kunselman AR, Sinoway LI (1999). Characteristics of the
muscle mechanoreflex during quadriceps contractions in humans. J Appl Physiol 86,
767–772.
Hopkins WG. Measures of reliability in sports medicine and science (2000). Sports
Med 30, 1–15.
Horiuchi M, Fadel PJ, Ogoh S (2014). Differential effect of sympathetic activation on
tissue oxygenation in gastrocnemius and soleus muscles during exercise in humans.
Exp Physiol 99, 348-58.

117
Hughes S, Gardiner T, Baxter L, Chan-Ling T (2007). Changes in pericytes and
smooth muscle cells in the kitten model of retinopathy of prematurity: implications
for plus disease. Invest Ophthalmol Vis Sci 48, 1368-79.
Iellamo F, Pizzinelli P, Massaro M, Raimondi G, Peruzzi G, Legramante JM (1999).
Muscle metaboreflex contribution to sinus node regulation during static exercise:
insights from spectral analysis of heart rate variability. Circulation 100(1), 27-32.
Iida H, Kurano M, Takano H, Kubota N, Morita T, Meguro K, Sato Y, Abe T,
Yamazaki Y, Uno K, Takenaka K, Hirose K, Nakajima T (2007). Hemodynamic and
neurohumoral responses to the restriction of femoral blood flow by KAATSU in
healthy subjects. Eur J Appl Physiol 100, 275–285.
Iwata M, Hayakawa K, Murakami T, Naruse K, Kawakami K, Inoue-Miyazu M, et al.
Uniaxial cyclic stretch stimulated glucose transport is mediated by a Ca-dependent
mechanism in cultured skeletal muscle cells (2007). Pathobiology: J
Immunopathology Molecular Cell Biology 74, 159–168.
Ives SJ, McDaniel J, Witman MA, Richardson RS (2013). Passive limb movement:
evidence of mechanoreflex sex specificity. Am J Physiol Heart Circ Physiol 304,
H154-61.
Ivy JL. Muscle glycogen synthesis before and after exercise (1991). Sports Med 11:
6- 19.
Jenkyn TR, Koopman B, Huijing P, Lieber RL, Kaufman KR (2002). Finite element
model of intramuscular pressure during isometric contraction of skeletal muscle. Phys
Med Biol 47, 4043-61.
Johnson MA, Polgar J, Weightman D & Appleton D (1973). Data on the distribution
of fibre types in thirty-six human muscles. An autopsy study. J Neurol Sci 18, 111–
129.
Joyner MJ (2006). Baroreceptor function during exercise: resetting the record. Exp
Physiol 91, 27–36.
Jewell BR. & Ruegg JC (1966). Oscillatory contractions of insect fibrillar muscle
after glycerol extraction. Proc. R. Soc. B 164, 428-459.
Kallerud H and Gleeson N. Effects of stretching on performances involving stretch
shortening cycles. Sports Medicine 43: 733-750, 2013.
Kaufman M, Forster H. Reflexes controlling circulatory, ventilator and airway
responses to exercise. In: Handbook of Physiology. Exercise: Regulation and
Integration of Multiple Systems. Bethesda, MD: Am. Physiol. Soc., 1996, sect. 12,
chapt. 10, p. 381–447.

118
Kaufman MP, Rybicki KJ, Waldrop TG, Ordway GA (1984). Effect of ischemia on
responses of group III and IV afferents to contraction. J Appl Physiol 57, 644-650.
Kaufman MP, Longhurst JC, Rybicki KJ, Wallach JH, Mitchell JH (1983). Effects of
static muscular contraction on impulse activity of groups III and IV afferents in cats. J
Appl Physiol 55, 105–112.
Kay AD and Blazevich AJ (2012). Effect of acute static stretch on maximal muscle
performance: a systematic review. Med Sci Sport Exerc 44, 154-164.
Kay AD and Blazevich AJ (2009). Moderate-duration static stretch reduces active and
passive plantar flexor moment but not Achilles tendon stiffness or active muscle
length. J Appl Physiol 106: 1249-1256.
Keller DM, Ogoh S, Greene S, Olivencia-Yurvati A, Raven PB (2004). Inhibition of
KATP channel activity augments baroreflex-mediated vasoconstriction in exercising
human skeletal muscle. J Physiol 561, 273–282.
Kirby BS, Voyles WF, Carlson RE, Dinenno FA (2008). Graded sympathetic effect
of exogenous ATP on postjunctional α-adrenergic vasoconstriction in the human
forearm: implications for vascular control in contracting muscle. J Physiol 586, 4305–
4316.
Kirkebo A, Wisnes A (1982). Regional tissue fluid pressure in rat calf muscle during
sustained contraction or stretch. Acta Physiol Scand 114, 551–556.
Kindig CA, Poole DC (2001). Sarcomere length-induced alterations of capillary
hemodynamics in rat spinotrapezius muscle: vasoactive vs passive control. Microvasc
Res 61, 64-74.
Kindig CA, Musch TI, Basaraba RJ, Poole DC (1999). Impaired capillary
hemodynamics in skeletal muscle of rats in chronic heart failure. J Appl Physiol 87,
652–60.
Kouzaki M, Shinohara M, Masani K, Tachi M, Kanehisa H, Fukunaga T (2003).
Local blood circulation among knee extensor synergists in relation to alternate muscle
activity during low-level sustained contraction. J Appl Physiol 95, 49–56.
Knudson D, Magnusson P, McHugh M (2000). Current issues in flexibility fitness.
President’s Council on Physical Fitness and Sports Research Digest 3, 1-8.
Kooijman M, Thijssen DH, de Groot PC, Bleeker MW, van Kuppevelt HJ, Green DJ,
Rongen GA, Smits P, Hopman MT (2008). Flow-mediated dilatation in the
superficial femoral artery is nitric oxide mediated in humans. J Physiol 586, 1137–
1145.

119
Kruse NK, Barr MW, Gilders RM, Kushnick MJ, Rana SR (2013). Using a practical
approach for determining the most effective stretching stretching in female NCAA
division I volleyball players. J Strength Cond Res 27, 3060-7.
Kruse, NK, Scheuermann, BW (2014). Effect of self-administered stretching on
NIRS-measured oxygenation dynamics. Clin Physiol Funct Imaging. In press.
Laughlin MH & Armstrong RB (1982). Muscular blood flow distribution patterns as
a function of running speed in rats. Am J Physiol Heart Circ Physiol 243,H296–
H306.
Learoyd BM & Taylor MG (1966). Alterations with age in the viscoelastic properties
of human arterial walls. Circ Res 18, 278–292.
Ling G & Gerard RW. (1949). The influence of stretch on the membrane potential of
the striated muscle fibre. J Cell Comp Physiol 34, 397-405.
MacDonald MJ, Naylor HL, Tschakovsky ME, Hughson RL (2001). Peripheral
circulatory factors limit rate of increase in muscle O2 uptake at the onset of heavy
exercise. J Appl Physiol 90, 83–89.
Maehara K, Riley M, Galassetti P, Barstow TJ & Wasserman K (1997). Effect of
hypoxia and carbon monoxide on muscle oxygenation during exercise. Am J Respir
Crit Care Med 155, 229–235.
Magnusson SP, Simonsen EB, Dyhre-Poulsen P, et al (1996). Viscoelastic stress
relaxation during static stretch in human skeletal muscle in the absence of EMG
activity. Scand J Med Sci Sports 6, 323–328.
Mathieu-Costello O, Hoppeler H, Weibel ER (1989). Capillary tortuosity in skeletal
muscles of mammals depends on muscle contraction. J Appl Physiol 66, 1436–1442.
Mathieu-Costello O (1987). Capillary tortuosity and degree of contraction or
extension of skeletal muscles. Microvasc Res 33, 98–117.
McCloskey DI, Mitchell JH (1972). Reflex cardiovascular and respiratory responses
originating in exercising muscle. J Physiol 224, 173–186
McCully KK (2010). The influence of passive stretch on muscle oxygen saturation.
Adv Exp Med Biol 662, 317-322.
McDaniel J, Ives SJ, Richardson RS. Human muscle length-dependent changes in
blood flow. J Appl Physiol 112: 560 –565, 2012.
McNair PJ, Dombroski EW, Hewson DJ, Stanley SN (2001). Stretching at the ankle
joint: viscoelastic responses to holds and continuous passive motion. Med Sci Sports
Exerc 354–358.

120
Miles SC, Chun-Chung C, Hsin-Fu L, Hunter SD, Dhindsa M, et al. (2013) Arterial
blood pressure and cardiovascular responses to yoga practice. Altern Ther Health
Med 19, 38-45.
Miura H, McCully K, Nioka S, and Chance B. (2004) Relationship between muscle
architectural features and oxygenation status determined by near infrared device. Eur
J Appl Physiol 91, 273–278.
Mitchell JH, Kaufman MP, Iwamoto GA (1983). The exercise pressor reflex: its
cardiovascular effects, afferent mechanisms, and central pathways. Annu Rev Physiol
45, 229 –242.
Moore JE, Xu C, Glagov S, Zarins CK, Ku DN (1994). Fluid wall shear stress
measurements in a model of the human abdominal aorta: oscillatory behavior and
relationship to atherosclerosis. Atherosclerosis 110, 225–240.
Morse CI (2011). Gender differences in the passive stiffness of the human
gastrocnemius muscle during stretch. Eur J Appl Physiol 111, 2149–2154.
Morse CI, Degens H, Seynnes OR, Maganaris CN, Jones DA (2008). The acute effect
of stretching on the passive stiffness of the human gastrocnemius muscle tendon unit.
J Physiol 586, 97–106.
Mortensen SP, Mørkeberg J, Thaning P, Hellsten Y, Saltin B (2012). Two weeks of
muscle immobilization impairs functional sympatholysis but increases exercise
hyperemia and the vasodilatory responsiveness to infused ATP. Am J Physiol Heart
Circ Physiol 302, H2074–H2082.
Muramatsu T, Muraoka T, Kawakami Y, et al. In vivo determination of fascicle
curvature in contracting skeletal muscles (2002). J Appl Physiol 92, 129-34
Miyachi M (2013) Effects of resistance training on arterial stiffness: a metaanalysis.
Br J Sports Med 47, 393-396.
Markwald RR, Kirby BS, Crecelius AR, Carlson RE, Voyles WF, Dinenno FA
(2011). Combined inhibition of nitric oxide and vasodilating prostaglandins abolishes
forearm vasodilatation to systemic hypoxia in healthy humans. J Physiol 589, 1979–
1990.
Mohrman DE and Sparks HV (1974). Myogenic hyperemia following brief tetanus of
canine skeletal muscle. Am J Physiol 227, 531–535.
Murphy MN, Mizuno M, Mitchell JH, Smith SA (2011). Cardiovascular regulation
by skeletal muscle reflexes in health and disease. Am J Physiol Heart Circ Physiol
301, H1191-204.
Naamani R, Hussain SN, Magder S (1995). The mechanical effects of contractions on
blood flow to the muscle. Eur J Appl Physiol Occup Physiol 71, 102–112.

121
Nakamura M, Ikezoe T, Takeno Y, Ichihashi N (2012). Effects of a 4-week static
stretch training program on passive stiffness of human gastrocnemius muscle-tendon
unit in vivo. Eur J Appl Physiol 112, 2749-55.
Naik JS, Valic Z, Buckwalter JB, Clifford PS (1999). Rapid vasodilation in response
to a brief tetanic muscle contraction. J Appl Physiol 87, 1741–1746.
Nakao M & Segal SS (1995). Muscle length alters geometry of arterioles and venules
in hamster retractor. Am J Physiol 268(1 Pt 2), H336-44.
Nelson AG, Kokkonen J, Arnall DA (2011). Twenty minutes of passive stretching
lowers glucose levels in an at-risk population: an experimental study. J Physiother 57,
173-8.
Norton KH, Boushel R, Strange S, Saltin B, Raven PB (1999). Resetting of the
carotid arterial baroreflex during dynamic exercise in humans. J Appl Physiol 87,
332–8.
Ogoh S, Fadel PJ, Nissen P, et al (2003). Baroreflex-mediated changes in cardiac
output and vascular conductance in response to alterations in carotid sinus pressure
during exercise in humans. J Physiol 550, 317–24.
Otsuki A, Fujita E, Ikegawa S, Kuno-Mizumura M (2011). Muscle oxygenation and
fascicle length during passive muscle stretching in ballet-trained subjects. Int J Sports
Med 32, 496-502.
Padilla J, Simmons GH, Fadel PJ, Laughlin MH, Joyner MJ, Casey DP (2010).
Impact of aging on conduit artery retrograde and oscillatory shear at rest and during
exercise: role of nitric oxide. Hypertension 57, 484-9.
Papelier Y, Escourrou P, Gauthier JP, Rowell LB (1994). Carotid baroreflex control
of blood pressure and heart rate in men during dynamic exercise. J Appl Physiol 77,
502-506.
Parker BA, Smithmyer SL, Pelberg JA, Mishkin AD, Proctor DN (2008). Sex-
specific influence of aging on exercising leg blood flow. J Appl Physiol 104, 655–
664.
Pereira MI, Gomes PS, Bhambhani YN (2007). A brief review of the use of near
infrared spectroscopy with particular interest in resistance exercise. Sports Med 37,
615-24.
Podolsky R (1964). The maximum sarcomere length for contraction of isolated
myofibrils. J. Physiol 170, 110-123.
Pohl U, Holtz J, Busse R, Bassenge E (1986). Crucial role of endothelium in the
vasodilator response to increased flow in vivo. Hypertension 8, 37–44.

122
Poole DC, Copp SW, Ferguson SK, Musch TI (2013). Skeletal muscle capillary
function: contemporary observations and novel hypotheses. Exp Physiol 98, 1645-58.
Poole DC, Musch TI, & Kindig, CA (1997). In vivo microvascular structural and
functional consequences of muscle length changes. Am J Physiol. 272(5 Pt 2),
H2107–H2114.
Poole DC, Mathieu-Costello O (1992). Capillary and fiber geometry in rat diaphragm
perfusion fixed in situ at different sarcomere lengths. J Appl Physiol 73, 151-9.
Poole DC, Mathieu-Costello O & West JB (1989). Capillary tortuosity in rat soleus
muscle is not affected by endurance training. Am J Physiol Heart Circ Physiol 256,
H1110–H1116
Potts JT, Shi XR, Raven PB (1993). Carotid baroreflex responsiveness during
dynamic exercise in humans. Am J Physiol Heart Circ Physiol 265, H1928–H1938.
Proctor KG & Duling BR. (1982). Adenosine and free-flow functional hyperemia in
striated muscle. Am.J Physiol 242, H688-H697.
Radegran G & Saltin B (1999). Nitric oxide in the regulation of vasomotor tone in
human skeletal muscle. Am J Physiol Heart Circ Physiol 276, H1951–1960.
Raven PB, Fadel PJ, Ogoh S (2006). Arterial baroreflex resetting during exercise: a
current perspective. Exp Physiol 91, 37-49.
Remensnyder JP, Mitchell JH, Sarnoff SJ (1962). Functional sympatholysis during
muscular activity. Observations on influence of carotid sinus on oxygen uptake. Circ
Res 11, 370-80.
Renzi CP, Tanaka H, Sugawara J (2010). Effects of leg blood flow restriction during
walking on cardiovascular function. Med Sci Sports Exerc 42, 726-32.
Robbins JW, Scheuermann BW (2008). Varying amounts of acute static stretching
and its effect on vertical jump performance. J Strength Cond Res 22, 781-6.
Rowell, LB. Human Cardiovascular Control. New York: Oxford University Press,
1993, pp. 255–301.
Rowell LB and O'Leary DS (1990). Reflex control of the circulation during exercise;
chemoreflexes and mechanoreflexes. J Appl Physiol 69, 407-418.
Ryan ED, Beck TW, Herda TJ, Hull HR, Hartman MJ, Stout JR, et al (2008). Do
practical durations of stretching alter muscle strength? A dose-response study. Med
Sci Sports Exerc 40, 1529-37.

123
Saunders NR & Tschakovsky ME (2004). Evidence for a rapid vasodilatory
contribution to immediate hyperemia in rest-to-mild and mild-to-moderate forearm
exercise transitions in humans. J Appl Physiol 97, 1143–1151.
Saltin B, Radegran G, Koskolou MD, Roach RC (1998). Skeletal muscle blood flow
in humans and its regulation during exercise. Acta Physiol Scand 162, 421–436.
Sands WA, McNeal JR, Murray SR, Ramsey MW, Sato K, Mizuguchi S, Stone MH.
Stretching and Its Effects on Recovery: A Review (2013). Strength Cond J 35, 30–
36.
Schreuder THA, Green DJ, Hopman MT, Thijssen DH (2014). Acute impact of
retrograde shear rate on brachial and superficial femoral artery flow-mediated dilation
in humans. Physiol Report 2, 1–8
Seals DR, Desouza CA, Donato AJ, Tanaka H (2008). Habitual exercise and arterial
aging. J Appl Physiol 105, 1323-1332.
Segal SS (2000). Integration of blood flow control to skeletal muscle: key role of
feed arteries. Acta Physiol Scand 168, 511-8.
Sejersted OM, Hargens AR, Kardel KR, Blom P, Jensen O, and Hermansen L (1984).
Intramuscular fluid pressure during isometric contraction of human skeletal muscle. J
Appl Physiol 56, 287–295.
Sheehan D, Mulholland JH, Safiroff B (1941). Surgical anatomy of the carotid sinus
nerve. Anat Rec 80, 431–42.
Shoemaker JK & Hughson RL (1999). Adaptation of blood flow during the rest to
work transition in humans. Med Sci Sports Exerc 31, 1019–1026.
Shrier, I (2004). Does stretching improve performance? A systematic and clinical
review of the literature. Clin J Sport Med 14, 256-273.
Silber HA, Ouyang P, Bluemke DA, Gupta SN, Foo TK, Lima JA (2005). A novel
method for assessing arterial endothelial function using phase contrast magnetic
resonance imaging: vasoconstriction during reduced shear. J Cardiovasc Magn Reson
7, 615-21.
Simic L, Sarabon N, and Markovic G (2011). Does pre-exercise static stretching
inhibit maximal muscular performance? A meta-analytical review. Scand J Med Sci
Sport 23, 131-148.
Stebbins CL, Brown B, Levin D, and Longhurst JC (1988). Reflex effect of skeletal
muscle mechanoreceptor stimulation on the cardiovascular system. J Appl Physiol 65,
1539 –1547.

124
Supinski GS, Bark H, Guanciale A, Kelsen SG (1986). Effect of alterations in muscle
fiber length on diaphragm blood flow. J Appl Physiol 60, 1789-96.
Takano H, Morita T, Iida H, Asada K, Kato M, Uno K, Hirose K, Matsumoto A,
Takenaka K, Hirata Y, Eto F, Nagai R, Sato Y, Nakajima T (2005). Hemodynamic
and hormonal responses to a short-term low-intensity resistance exercise with the
reduction of muscle blood flow. Eur J Appl Physiol 95, 65-73.
Tanaka S, Sugiura T, Yamashita S, Dohi Y, Kimura G, Ohte N (2014). Differential
response of central blood pressure to isometric and isotonic exercises. Sci Rep 4,
5439.
Thijssen DH, Dawson EA, Tinken TM, Cable NT, Green DJ (2009) Retrograde flow
and shear rate acutely impair endothelial function in humans. Hypertension 53, 986–
992. 11.
Thijssen DH, Black MA, Pyke KE, Padilla J, Atkinson G, et al. (2011). Assessment
of flow-mediated dilation in humans: a methodological and physiological guideline.
Am J Physiol Heart Circ Physiol 300, H2–12.
Tinken TM, Thijssen DH, Hopkins N, Black MA, Dawson EA, et al. (2009) Impact
of shear rate modulation on vascular function in humans. Hypertension 54, 278–285.
Thomas GD, Hansen J, Victor RG (1997). ATP-sensitive potassium channels mediate
contraction-induced attenuation of sympathetic vasoconstriction in rat skeletal
muscle. J Clin Invest 99, 2602–2609.
Thomas GD & Victor RG (1998). Nitric oxide mediates contraction-induced
attenuation of sympathetic vasoconstriction in rat skeletal muscle. J Physiol 506,
817–826.
Thomas GD, Hansen J & Victor RG (1994). Inhibition of α2-adrenergic
vasoconstriction during contraction of glycolytic, not oxidative, rat hindlimb muscle.
Am J Physiol Heart Circ Physiol 266, H920–H929.
Thompson BC, Fadia T, Pincivero DM, Scheuermann BW (2007). Forearm blood
flow responses to fatiguing isometric contractions in women and men. Am J Physiol
Heart Circ Physiol. 93, H805-12.
Totosy de Zepetnek JO, Jermey TL, MacDonald MJ (2014). Superficial Femoral
Artery Endothelial Responses to a Short-Term Altered Shear Rate Intervention in
Healthy Men. PLoS One 21, 9(11).
Trajano GS, Nosaka K, Seitz L, Blazevich AJ (2014). Intermittent stretch reduces
force and central drive more than continuous stretch. Med Sci Sports Exerc 5, 902-10
Trappe SW, Trappe TA, Lee GA & Costill DL (2001). Calf muscle strength in
humans. Int J Sports Med 22, 186–191.

125
Trinity JD, Amann M, McDaniel J, Fjeldstad AS, Barrett-O'Keefe Z, Runnels S,
Morgan DE, Wray DW, Richardson RS (2010). Limb movement-induced hyperemia
has a central hemodynamic component: evidence from a neural blockade study. Am J
Physiol Heart Circ Physiol 299, H1693-700.
Tschakovsky ME, Rogers AM, Pyke KE, Saunders NR, Glenn N, Lee SJ,
Weissgerber T, and Dwyer EM (2004). Immediate exercise hyperemia in humans is
contraction intensity dependent: evidence for rapid vasodilation. J Appl Physiol 96:
639–644.
VanTeeffelen JW & Segal SS (2006). Rapid dilation of arterioles with single
contraction of hamster skeletal muscle. Am J Physiol Heart Circ Physiol 290, H119–
H127.
Venturelli M, Amann M, McDaniel J, Trinity JD, Fjeldstad AS, Richardson RS
(2012). Central and peripheral hemodynamic responses to passive limb movement:
the role of arousal. Am J Physiol Heart Circ Physiol 302, H333-9.
Victor, RG, Pryor, SL, Secher, NH, Mitchell, JH (1989). Effects of partial
neuromuscular blockade on sympathetic nerve responses to static exercise in humans.
Circ Res 65, 468–476.
Villar R, Hughson RL. Repeatability of popliteal blood flow and lower limb vascular
conductance at rest and exercise during body tilt using Doppler ultrasound (2013).
Physiol Meas 34, 291-306.
Welsh DG & Segal SS (1997). Coactivation of resistance vessels and muscle fibers
with acetylcholine release from motor nerves. Am J Physiol 273(1 Pt 2), H156-63.
Welsh DG & Segal SS (1996). Muscle length directs sympathetic nerve activity and
vasomotor tone in resistance vessels of hamster retractor. Circ Res 79, 551–559.
Wilson LB, Wall PT, Pawelczyk JA, Matsukawa K (1994). Cardiorespiratory and
phrenic nerve responses to graded muscle stretch in anesthetized cats. Respir Physiol
98, 251–266.
Wray DW, Fadel PJ, Smith ML, Raven P & Sander M (2004). Inhibition of α-
adrenergic vasoconstriction in exercising human thigh muscles. J Physiol 555, 545–
563.
Wray DW, Donato AJ, Uberoi A, Merlone JP, Richardson RS (2005). Onset exercise
hyperaemia in humans: partitioning the contributors. J Physiol 565, 1053–1060.
Yamamoto K, Kawano H, Gando Y, Iemitsu M, Murakami H, et al. (2009) Poor trunk
flexibility is associated with arterial stiffening. Am J Physiol Heart Circ Physiol 297,
314-318.

126
Appendix A
Subject Information and Consent form
Time Course Changes in Muscle Oxygenation, Neuromuscular Activity and Force after
Passive Stretching.
Principal Investigator: Barry W. Scheuermann, Ph.D.
Other Staff (identified by role): Nick Kruse, MS (Co-investigator)
Shinichiro Sugiura, MS (Graduate Student Research
Assistant)
Trent Cayot, BS, (Graduate Student Research
Assistant)
Erin Garmyn, BS (Graduate Student Research
Assistant)
Chris Silette, BS (Graduate Student Research
Assistant)
Contact Phone number(s): (419) 530-2692 Office
(419) 530-2058 Lab
What you should know about this research study:
We give you this consent/authorization form so that you may read about the
purpose, risks, and benefits of this research study. All information in this
form will be communicated to you verbally by the research staff as well.
Routine clinical care is based upon the best-known treatment and is
provided with the main goal of helping the individual patient. The main
goal of research studies is to gain knowledge that may help future patients.
We cannot promise that this research will benefit you. Just like routine
care, this research can have side effects that can be serious or minor.
You have the right to refuse to take part in this research, or agree to take
part now and change your mind later.

127
If you decide to take part in this research or not, or if you decide to take part
now but change your mind later, your decision will not affect your routine
care.
Please review this form carefully. Ask any questions before you make a
decision about whether or not you want to take part in this research. If you
decide to take part in this research, you may ask any additional questions at
any time.
Your participation in this research is voluntary.
PURPOSE (WHY THIS RESEARCH IS BEING DONE)
You are being asked to take part in a research study that will measure how your skeletal
muscles respond to static stretching. Static stretching involves moving a limb such as
your arm or leg to a position and then holding that position to improve your flexibility.
This is a very common approach used by elite and recreational athletes. A greater
understanding of the time course by which your skeletal muscles respond to static
stretching may provide important information and add further merit to the use of
stretching in both therapeutic and exercise performance programs.
You were selected as someone who may want to take part in this study because you
indicated an interest in this study by contacting either Dr. Barry Scheuermann or Nick
Kruse and you meet the criteria outlined below. This study will include 20 participants
recruited from the University of Toledo and surrounding community.
To participate in this study, you must be between 18-45 years of age and be free of any
known cardiovascular, pulmonary, or metabolic disease as determined by a medical
history questionnaire (Appendix A). If you do not meet these criteria, we appreciate your
willingness to volunteer but unfortunately, you will not be able to participate in this
study.
DESCRIPTION OF THE RESEARCH PROCEDURES AND DURATION OF
YOUR INVOLVEMENT
If you decide to take part in this study, you will be asked to visit the Cardiopulmonary
and Metabolism Research (room HH 1407) laboratory in the Department of Kinesiology
located on the main campus of the University of Toledo in the Health and Human
Services Building. All testing will take place at this location. You will be asked to visit
the Cardiopulmonary and Metabolism Research Laboratory on 4 separate occasions.
Each session will last approximately 1 hour.
Study Visits
First Visit: (orientation and familiarization)
The first visit will be a familiarization and orientation to the following three
experimental sessions. During the first visit you will be asked to read and sign

128
this informed consent form, which explains all of the tests and procedures of the
research study. You will be able to ask the investigators any questions regarding
the research study prior to signing the informed consent form.
After you sign the informed consent form, you will be asked to complete a
medical history questionnaire and an activity level questionnaire.
Standard measurements of height, weight, thigh girth (circumference), thigh
skinfold measurements, and resting blood pressure will also be recorded.
If you meet all inclusion criteria, you will then be oriented to the following
procedures and equipment used in this study:
o Muscle function test (MFT): The maximal strength of your calf muscles will
be evaluated using an isokinetic dynamometer involving a maximal voluntary
isometric contraction (MVIC) of your calf muscles. An isokinetic
dynamometer is equipment that has a chair attached to an adjustable strength
machine and computer control unit. This device allows us to measure how
much force or strength that you are able to generate when you contract your
muscles with a maximal effort. The leg that we will test in this research study
is your dominant leg (the leg that you would use to kick a ball). You will be
asked to sit on the isokinetic dynamometer and perform 2 sets of 4 repetitions
of leg exercise using a light- to-moderate amount of weight or resistance as a
warm-up. During the exercise you will have a strap wrapped around your
ankle as well as a Velcro belt around you hips. Following the warm-up, you
will be asked to contract your leg muscles as hard as you can (MVIC) and
exert a maximal effort for 5 seconds. You will be asked to repeat this
maximal effort a total of 3 times but you will be provided with a 7 minute rest
period between each attempt.
o Near infrared spectroscopy (NIRS) will be used to measure local changes in
muscle oxygenation and blood flow during and after experimental stretch
protocols. Near infrared spectroscopy (NIRS) is a non-invasive method used
to measure relative changes in oxygen saturation and blood volume.
o Electromyography (EMG); The amount of muscle that you use during mucle
contractions and stretching activities will be measured using surface EMG
methods. Surface EMG is non-invasive way of measuring the small amount
of electrical activity (neural activity) that your muscles generate during
acitivity
Preparation Steps for NIRS and EMG:
o In order to accurately measure muscle NIRS and EMG a small area of your
skin will be shaved, abraded, and cleaned before a small plastic sensor and
adhesive electrode is placed on the surface of your skin over your calf muscles
(also called your gastrocnemius muscle). To measure muscle oxygenation, a
small plastic sensor will also be placed on the surface of your skin and secured
in place using Velcro straps. EMG assessment will involve placing an
adhesive pad over surface of the skin overlying the muscles just below the

129
NIRS sensor. A small wire connects the adhesive pad to an electronic device
that is able to record the small electrical signals generated by muscles when
they contract.
Visits Two to Four: (Experimental Sessions)
You will be randomly assigned to each experimental sessions (session 2-4), and
each testing session will last ~1h. You will be required to refrain from strenuous
exercise for at least 24 h and caffeine 2 h prior to entering the laboratory each
morning between 7-9 am.
Just prior to the stretch protocol a preliminary muscle function test (MFT) (as
described above) will be conducted.
Afterward, either a control (CON), static stretch only (SS), or warm-up with SS
(WSS) session will be completed for a total duration of 12 minutes. Upon
completion, you will perform the MFT, which will involve contracting your calf
muscles involving a series of MVICs at timing interval assessments of 1, 5 and 15
minutes post-stretch.
The following is a brief description of each intervention you will perform:
o Control: During the control (CON) session, you will be equipped with a near
infrared sensor (NIRS) and EMG electrode over the surface of the skin in line
with the location of the medial gastrocnemius (MG). Specifically, the NIRS
source detector will be placed on the proximal portion of the MG while the
EMG electrode will be place on the distal belly portion of the MG. No
stretching will occur during this session. Instead, after resting in a seat for 12
minutes, you will complete the MFT. During the MFT your leg will be kept
fully extended and strapped into this position with a Velcro strap to minimize
limb movement during MVICs. Muscle oxygenation (NIRS) and muscle
activity (surface EMG) will be continually assessed during a series of three
MVCs at each specific time (1 vs. 5 vs. 15 min).
o Static stretch: For the SS only session you will perform 3 sets of 3 minute
static stretches with 1 minute rest of your calf muscle on the isokinetic
dynamometer while NIRS and EMG is continuously recorded. The
dynamometer is a machine that can be adjusted based on the amount of force
that you push against it with your foot. You will place your foot on a plate
and you move your foot to stretch in your calf muscle. The machine will be
manually stopped by the investigator by your verbal command when the
stretch is at a point of “moderate discomfort.” At this point the clock will start
and your first 3 minute SS will begin. After the first SS, your foot will be
released from the stretch and allowed to rest passively for 1 minute. The
stretch-rest protocol will be repeated 2 more times for a total duration of 12
minutes. After the third SS you will be asked to perform three MVICs at
timing intervals of 1, 5, and 15 minutes after the last stretch.

130
o Warm-up with static stretch: For the warm-up with static stretch (WSS)
intervention all preparations involving the isokinetic dynamometer will apply
for this session. Once your foot is secured to the plate you will begin 2 warm-
up sets for 3 minutes each performing light (15% of initial pre-test MVIC).
To warm-up, you will be asked to move your foot through a complete range of
motion by pushing your toes toward the floor as far as you can and then
pulling your toes up as far as you can. Each set will be accompanied by a 1
minute rest. On the third 3 minute set, instead of pushing your toes towards
the floor, your foot will be positioned so that your calf muscle is stretched to a
point of “moderate discomfort” based on verbal cues by you. At this point the
stretch will be held for 3 minutes. After the WSS intervention (totaling 12
minutes), you will then perform three MVICs at timing intervals of 1, 5, and
15 minutes after the last stretch.
o Maximal physiological oxygen desaturation: After each experimental protocol
(visit 2-4) you will undergo a maximal desaturation trial using a blood
pressure cuff placed around your thigh. The cuff will be inflated to 250 mm
Hg for 5 minutes and NIRS will be used to measure the change in oxygen
used by your muscle during this time. This procedure is performed so that we
can compare your results across each of the visits 2 to 4.
RISKS AND DISCOMFORTS YOU MAY EXPERIENCE IF YOU TAKE PART
IN THIS RESEARCH
Immediate risks may include muscle cramping, strain, or soreness during the exercise,
especially following the muscle function test.
You may also experience numbness, tingling sensation, or bruising in the lower
extremities during the duration of the blood flow restriction conditions (while the blood
pressure cuffs are inflated). Numbness and tingling sensations will stop immediately
upon the release of the pressure in the blood pressure cuffs. There is a small potential
risk that a venous clot may develop during the blood flow restriction period but this risk
will be minimized by indicating on the medical history questionnaire if you have any
hereditary conditions that may cause your blood to clot easily. There exists a low, but
unknown, risk of developing chronic venous insufficiency (difficulties with blood flow
out of the leg) and/or deep vein thrombosis (blood clot within the leg) in the lower
extremities in the future following blood flow restriction exercise. This risk will be
minimized by indicating on the medical history questionnaire if you have any hereditary
conditions that may cause your blood to clot easily.
There are no known risks and/or discomfort associated with measuring oxygen delivery
using near-infrared spectroscopy (NIRS) techniques or with measuring electrical activity
of the muscles using electromyography (EMG).

131
POSSIBLE BENEFIT TO YOU IF YOU DECIDE TO TAKE PART IN THIS
RESEARCH
There is no direct benefit from participating in this study to the participants. Students
from the Department of Kinesiology that participate in this study will be exposed to
current research topics and techniques.
COST TO YOU FOR TAKING PART IN THIS STUDY
There are no costs associated with participating in this study.
PAYMENT OR OTHER COMPENSATION TO YOU FOR TAKING PART IN
THIS RESEARCH
If you decide to take part in this research you will not receive any payment or
compensation for participating in this research nor will you be given “extra credit” in any
academic courses that you are enrolled.
ALTERNATIVE(S) TO TAKING PART IN THIS RESEARCH
No alternative procedures or treatments will be made available since this research does
not incorporate any procedures or treatments that affect the subject.
CONFIDENTIALITY - (USE AND DISCLOSURE OF YOUR PROTECTED
HEALTH INFORMATION)
The researchers will make every effort to prevent anyone who is not on the research team
from knowing that you provided this information, or what that information is. The
consent forms with signatures will be kept separate from responses, which will not
include names and which will be presented to others only when combined with other
responses. The Medical History Questionnaire with signatures will be kept separate from
the consent form and other responses which will not include names. Although we will
make every effort to protect your confidentiality, there is a low risk that this might be
breached.
IN THE EVENT OF A RESEARCH-RELATED INJURY
In the event of injury resulting from your taking part in this study, treatment can be
obtained at a health care facility of your choice. You should understand that the costs of
such treatment will be your responsibility. Financial compensation is not available
through The University of Toledo or The University of Toledo Medical Center. By
signing this form you are not giving up any of your legal rights as a research participant.
In the event of a study-related injury, you may contact Dr. Barry Scheuermann any time
of the day or night at 567-288-9732.
VOLUNTARY PARTICIPATION
Taking part in this study is voluntary. You may refuse to participate or discontinue
participation at any time without penalty or a loss of benefits to which you are otherwise
entitled. If you decide not to participate or to discontinue participation, your decision
will not affect your future relations with the University of Toledo or The University of
Toledo Medical Center.

132
NEW FINDINGS
You will be notified of new information that might change your decision to be in this
study if any becomes available.

133
OFFER TO ANSWER QUESTIONS
Before you sign this form, please ask any questions on any aspect of this study that is unclear to you. You may take
as much time as necessary to think it over. If you have questions regarding the research at any time before, during or
after the study, you may contact Dr. Barry Scheuermann (419-530-2692) or Nick Kruse
If you have questions beyond those answered by the research team or your rights as a research subject or research-
related injuries, please feel free to contact the Chairperson of the University of Toledo Biomedical Institutional
Review Board at 419-383-6796.
SIGNATURE SECTION (Please read carefully)
YOU ARE MAKING A DECISION WHETHER OR NOT TO PARTICIPATE IN THIS RESEARCH
STUDY. YOUR SIGNATURE INDICATES THAT YOU HAVE READ THE INFORMATION PROVIDED
ABOVE, YOU HAVE HAD ALL YOUR QUESTIONS ANSWERED, AND YOU HAVE DECIDED TO
TAKE PART IN THIS RESEARCH.
BY SIGNING THIS DOCUMENT YOU AUTHORIZE US TO USE OR DISCLOSE YOUR PROTECTED
HEALTH INFORMATION AS DESCRIBED IN THIS FORM.
The date you sign this document to enroll in this study, that is, today’s date, MUST fall between the dates indicated
on the approval stamp affixed to the bottom of each page. These dates indicate that this form is valid when you enroll
in the study but do not reflect how long you may participate in the study. Each page of this Consent/Authorization
Form is stamped to indicate the form’s validity as approved by the UT Biomedical Institutional Review Board (IRB).
Name of Subject (please print) Signature of Subject or
Person Authorized to Consent
Date
a.m.
Relationship to the Subject (Healthcare Power of Attorney authority or Legal Guardian) Time p.m.
Name of Person Obtaining Consent (please
print)
Signature of Person Obtaining Consent Date
Name of Witness to Consent Process (when
required by ICH Guidelines)
(please print)
Signature of Witness to Consent Process
(when required by ICH Guidelines)
Date