Embed Size (px)
Citation preview

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Chapter 4 Hemorrhage and Shock

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Introduction to Hemorrhage and Shock
Hemorrhage
Shock
Topics

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Introduction to Hemorrhage and Shock
Hemorrhage– Abnormal internal or external loss of
blood
Homeostasis– Tendency of the body to maintain a
steady and normal internal environment
Shock– INADEQUATE TISSUE PERFUSION– Transition between homeostasis and
death

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage
Circulatory System
Hemorrhage Classification
Clotting
Factors Affecting Clotting
Hemorrhage Control
Stages of Hemorrhage
Hemorrhage Assessment
Hemorrhage Management

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiac Anatomy

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Heart
Cardiac Cycle – The repetitive pumping action that
produces pressure changes that circulate blood throughout the body
Cardiac Output – The total amount of blood separately
pumped by each ventricle per minute, usually expressed in liters per minute

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiac Output
Normal cardiac output = 5 to 6 liters per minute (LPM). Can increase up to 30 LPM in times of stress or exercise.Determined by multiplying the heart rate by the volume of blood ejected by each ventricle during each beat (stroke volume).CO is influenced by:– Strength of contraction– Rate of contraction– Amount of venous return available to the
ventricle (preload)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Circulatory System (1 of 4)
Heart– Autonomic nervous system
Parasympathetic nervous systemSlows rate
Mediated by vagus nerve
Sympathetic nervous systemIncreases rate
Cardiac plexus

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Circulatory System (2 of 4)
Key TermsStroke VolumePreloadVentricular FillingStarling’s Law of the heartAfterload (End Diastolic Pressure or EDP)Cardiac Output– SV x HR– 5 liters/minute
Fick Principle

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Arteries– Tunica Adventitia– Tunica Media– Tunica Intima
ArterioleCapillary: 7% of total blood volumeVenuleVein– Constriction returns 20% (1 liter) of blood to
active circulation
} 64% of blood volume
} 13% of blood volume
Circulatory System (3 of 4)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Circulatory System (4 of 4)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
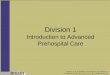
Cardiac Physiology
Vena Cavaand
SystemicVeins
Aortaand
SystemicArteries
SystemicCapillaries
PulmonaryArteries
LUNGS
PulmonaryVeins
RightAtrium
RightVentricle
LeftAtrium
LeftVentricle

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Circulation (1 of 2)
Systolic Pressure– Strength and volume of cardiac output
Diastolic Pressure– More indicative of the state of constriction
of the arterioles
Mean Arterial Pressure– 1/3 pulse pressure added to the diastolic
pressure– Tissue perfusion pressure

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Circulation (2 of 2)
Vascular Control– Increased sympathetic tone results in
increased vasoconstriction.
Microcirculation– Blood flow in the arterioles, capillaries,
and venules.– Sphincter functioning.
Most organ tissue requires blood flow 5 to 20% of the time.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiac Physiology (1 of 2)
Oxygen Supply– The myocardium receives its blood/oxygen supply
during the diastole phase of contraction. The blood flows from the aorta through the two coronaries into the relaxed myocardium.
Oxygen Demand– 90% of the O2 demand, or work, of the heart is
performed during the isovolumetric phase of contraction. In this phase, NO blood flows from the heart into the aorta, until the pressure in the heart is greater than the end diastolic pressure (EDP).

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiac Physiology (2 of 2)
Releases a polypeptide called atrial natriuretic peptide (ANP)
Works antagonistically to renin-angiotensin
Four Effects– Promotes Na+ and water loss at the kidneys– Inhibits renin release and ADH, aldosterone
secretion– Suppresses thirst– Blocks action of angiotensin II and
norepinephrine

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Negative Feedback
Important negative feedback mechanisms in maintaining tissue perfusion are the:– Baroreceptor reflexes– Central nervous system ischemia
responses– Hormonal mechanisms– Reabsorption of tissue fluids

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiovascular System Regulation (1 of 3)
PNS and SNS always act in balance
Baroreceptors: monitor BP
Chemoreceptors
Hormone regulation
Reabsorption of tissue fluids

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiovascular System Regulation (2 of 3)
Parasympathetic Nervous System
Decrease – Heart rate– Strength of contractions– Blood pressure
Increase– Digestive system– Kidneys

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Cardiovascular System Regulation (3 of 3)
Sympathetic Nervous SystemIncrease– Body activity– Heart rate– Strength of contractions– Vascular constriction
Bowel and digestive visceraDecreased urine production
– Respirations– Bronchodilation
Increases skeletal muscle perfusion

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Baroreceptor Reflexes (1 of 5)
High in the neck, each carotid artery divides into external and internal carotid arteries.– At the bifurcation, the wall of the artery is thin
and contains many vine-like nerve endings.
The small portion of the artery is the carotid sinus.– Nerve endings in this area are sensitive to
stretch or distortion.Serve as pressure receptors or baroreceptors.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Baroreceptor Reflexes (2 of 5)
Similar area found in the arch of the aorta.– Serves as a second important baroreceptor
Large arteries, large veins, and the wall of the myocardium also contain less important baroreceptors.Baroreceptor reflexes help maintain blood pressure by two negative feedback mechanisms:– By lowering blood pressure in response to
increased arterial pressure– By increasing blood pressure in response to
decreased arterial pressure

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Baroreceptor Reflexes (3 of 5)
Normal blood pressure partially stretches the arterial walls so that baroreceptors produce a constant, low-frequency stimulation.
Impulses from the baroreceptors inhibit the vasoconstrictor center of the medulla and excite the vagal center when blood pressure increases.– Results in vasodilation in the peripheral circulatory
system and a decrease in the heart rate and force of contraction.
Combined effect is a decrease in arterial pressure.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Baroreceptor Reflexes (4 of 5)
Baroreceptors adapt in 1 to 3 days to whatever pressure level they are exposed. Therefore, they do not change the average blood pressure on a long-term basis. This adaptation is common in people who have chronic hypertension.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Baroreceptor Reflexes (5 of 5)
When baroreceptor stimulation ceases due to a fall in arterial pressure, several cardiovascular responses are evoked:– Vagal stimulation is reduced and sympathetic
response is increased.– The increase in sympathetic impulses results in
increased peripheral resistance and an increase in heart rate and stroke volume.
Sympathetic discharges also produce generalized arteriolar vasoconstriction, which decreases the container size.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
The vasoconstriction in peripheral vascular beds results in the
characteristic pale, cold skin of patients suffering from hypovolemic shock.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Chemoreceptor Reflexes
Chemoreceptors– Monitor level of CO2 in CSF
– Monitor level of O2 in blood

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Chemoreceptor Physiology
Low arterial pressure leads to hypoxemia and/or acidosis.Hypoxemia/acidosis stimulate peripheral chemoreceptor cells within the carotid and aortic bodies.– These bodies have an abundant blood supply.
When oxygen or pH decreases, these cells stimulate the vasomotor center of the medulla.– The rate and depth of ventilation are also
increased to help eliminate excess carbon dioxide and maintain acid-base balance.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (1 of 7)
Catecholamines– Epinephrine– Norepinephrine– Actions
Alpha 1
Alpha 2
Beta 1
Beta 2

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (2 of 7)
Alpha 1– Vasoconstriction– Increased
peripheral vascular resistance
– Increased preload
Alpha 2– Regulates release
of NE
Beta 1– Positive inotropy– Positive
chronotropy– Positive
dromotropy
Beta 2– Bronchodilation– Smooth muscle
dilation in bowel

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (3 of 7)
Antidiuretic Hormone (ADH)– AKA: Arginine Vasopressin (AVP)– Released
Posterior pituitary
Drop in BP or increase in serum osmolarity
– ActionIncrease in peripheral vascular resistance
Increase water retention by kidneys
Decrease urine output
Splenic vasoconstriction200 mL of free blood to circulation

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (4 of 7)
Angiotensin II– Released
Primary chemical from kidneys
Lowered BP and decreased perfusion
– ActionConverted from renin into angiotensin I
Modified in lungs to angiotensin II
20-minute process
Potent systemic vasoconstrictor
1-hour duration
Causes release of ADH, aldosterone, and epinephrine

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (5 of 7)
Aldosterone– Release
Adrenal cortex
Stimulated by angiotensin II
– ActionMaintain kidney ion balance
Retention of sodium and water
Reduce insensible fluid loss

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (6 of 7)
Glucagon– Release
Alpha cells of pancreas
Triggered by epinephrine
– ActionCauses liver and skeletal muscles to convert glycogen into glucose
Gluconeogenesis

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CV System and Hormone Regulation (7 of 7)
Insulin– Release
Beta cells of pancreas
– ActionFacilitates transport of glucose across cell membrane
Erythropoietin– Release
Kidneys
Hypoperfusion or hypoxia
– ActionIncreases production and maturation of RBCs in the bone marrow

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Reabsorption of Tissue Fluids (1 of 2)
Arterial hypotension, arteriolar constriction, and reduced venous pressure during hypovolemia lower the blood pressure in the capillaries (hydrostatic pressure).
The decrease promotes reabsorption of interstitial fluid into the vascular compartment.– Considerable quantities of fluid may be drawn
into the circulation during hemorrhage.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Reabsorption of Tissue Fluids (2 of 2)
Approximately 0.25 mL/min/kg of body weight (1 L/hr in the adult male) can be autotransfused from the interstitial spaces after acute blood loss.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Vasculature
Lined with smooth muscle.
All vessels larger than capillaries have layers of tissues (tunicae).
Maintains blood flow by changes in pressure and peripheral vascular resistance.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Vascular Pressure Gradients
Fluid flows through a tube in response to pressure gradients between the two ends of the tube.
It is not the absolute pressure in the tube that determines flow, but the difference in pressure between the two ends.
In humans, the two ends are the aorta and the vena cava.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
VasculatureMeasurements of pressure in the vascular system:– Systemic pressure
(left‑sided pressure) and
– Pulmonic pressure (right‑sided pressure)
Systemic pressure, like pulmonic pressure, has two phases: systolic and diastolic.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Diastolic Blood Pressure
Diastolic blood pressure is a reflection of peripheral vascular resistance.– Pulse pressure is the difference between
these two pressures.– Pressure is greatest at its origin (the heart)
and least at its terminating point (the venae cavae).
– This pressure gradient changes significantly at the arteriole because of peripheral vascular resistance.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Peripheral Vascular Resistance (Afterload)
The total resistance against which blood must be pumped.It is essentially a measure of friction between the vessel walls and fluid, and between the molecules within the fluid itself (viscosity).– Both oppose flow.
When resistance to flow increases, blood pressure must increase for the flow to remain constant.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Starling’s Law of the Heart
When the rate at which blood flows into the heart from the veins (venous return) changes, the heart automatically adjusts its output to match inflow. The more blood the heart receives the more it pumps…
Increased end diastolic volume increases contractility. Increases stroke volume.
– Increases cardiac output. Starling curves at any end-diastolic volume.Increased sympathetic input increases stroke volume. Decreased sympathetic input decreases stroke volume.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Resistance to Blood Flow Increases with…
Increased fluid viscosity
Increased vessel length
Decreased vessel diameter

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Viscosity
The physical property of a liquid characterized by the friction between its component molecules (e.g., between the blood cells and between the plasma proteins)
Normally plays a minor role in blood flow regulation as it remains constant in healthy people

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Blood Flow Resistance (1 of 2)
Arteries are large and offer little resistance to flow unless they have an abnormal narrowing (stenosis).

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Blood Flow Resistance (2 of 2)
Arterioles have a much smaller diameter and offer the major resistance to blood flow.– Smooth muscles in the arteriole walls can
relax or contract.– Can change the diameter of the vessel as
much as fivefold.– Arterial blood pressure is regulated
primarily by the vasoconstriction or vasodilation of these vessels.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Microcirculation (1 of 3)
Can be divided into pulmonary microcirculation and peripheral microcirculation.
Pressure in each division is produced by the right and left heart, respectively.
Approximately 5% of the total circulating blood flow is always flowing through capillaries.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Microcirculation (2 of 3)
Venules and veins serve as collecting channels and storage vessels (capacitance).
Normally contain 70% of the blood volume.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Microcirculation (3 of 3)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Mechanisms That Control Blood Flow
Local control of blood flow by the tissues
Nervous control of blood flow

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Local Control
Blood usually flows through capillaries intermittently due to:– The pulsatile manner of blood flow
resulting from cardiac pumping action and vasomotion
– The intermittent constriction and dilation of arterioles and precapillary sphincters

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Vasomotion (1 of 3)
Regulated primarily by the concentration of oxygen in the tissues.
When oxygen concentration is low, the cells lining and adjacent to the closed capillaries secrete histamine, which is thought to be responsible for arteriolar smooth muscle vasodilation, causing the capillary to open.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Vasomotion (2 of 3)
Histamine is quickly destroyed in the blood and does not enter the general circulation.
As cells become reoxygenated they stop the histamine secretion, and the capillary closes.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Vasomotion (3 of 3)
A decrease in oxygen concentration leads to a local release of vasodilating substances, which allows blood flow to increase.– This in turn increases the delivery of
oxygen and restores aerobic metabolism.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Nervous control of circulation is accomplished
by negative feedback mechanisms.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
CNS Ischemia Response
CNS ischemia response is activated when blood flow to the vasomotor center of the medulla is decreased.– In the presence of ischemia, the neurons within
the medulla stimulate the sympathetic nervous system.
Sympathetic vasoconstriction can elevate arterial pressure for as long as 10 minutes.
The cerebral ischemia response functions only in emergency situations.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Blood and Blood Components

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Blood
Blood Volume– Average adult male has a blood volume
of 7% of total body weight.– Average adult female has a blood volume
of 6.5% of body weight.– Normal adult blood volume is 4.5–5 L.
Remains fairly constant in the healthy body.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Blood Components (1 of 2)
Erythrocyte: 45%– Hemoglobin– Hematocrit
Miscellaneous blood products: <1%– Platelets– Leukocytes
Monocytes, basophils, esonophils, neutrophils
Plasma: 54%

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Blood Components (2 of 2)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Plasma (1 of 2)
Approximately 92% water– The liquid portion of blood
Circulates salts, minerals, sugars, fats, and proteins throughout the body

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Contains 3 major proteins: – Albumin
Most plentiful plasma proteinSimilar in consistency to egg whitesGives blood its gummy textureHelps keep water concentration of blood low enough to allow water to diffuse readily from tissues into blood
– Globulins serve 2 main functions:Alpha and beta globulins transport other proteinsGamma globulins give people immunity to disease
– FibrinogenAids in blood clotting by forming a web of protein fibers that binds blood cells together
Plasma (2 of 2)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Other Functions of Plasma
Proteins function as an acid or base to correct changes in blood acidity.
Can temporarily meet nutritional need of the body should the body run short of food.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Proteins
Account for 50% of the body’s organic material– Components of most body structures– Roles in the chemical reactions in the body
Specialized proteins are responsible for:– Immune responses– Coagulation– Digestion of foodstuffs– Metabolism of nutrients– Many other functions

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Erythrocytes (RBCs)
Transport 99% of blood oxygen.– Remaining 1% carried in plasma
Make up approximately 45% of the blood and are the most abundant cells in the body.
Provide oxygen to tissues and remove carbon dioxide.
Each RBC contains approximately 270 million hemoglobin molecules.– Allow RBCs to pick up oxygen in the lungs and
release it to body tissues

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Leukocytes (WBCs)
Defend the body against various pathogens (bacteria, viruses, fungi, and parasites)
Produced in bone marrow and lymph glands– Release reserves when pathogens
invade the body

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Platelets
Part of the body’s defense mechanism
Formed in red bone marrow
Work by swelling and adhering together to form sticky plugs (initiating the clotting phenomenon)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Clotting (1 of 2)
Three-Step Process– Vascular phase
Vasoconstriction
– Platelet phaseTunica intima damaged
Turbulent blood flowFrictional damage to platelets
Agglutination and aggregation
– CoagulationRelease of enzymes
Extrinsic – nearby tissueIntrinsic – damaged plateletsFibrin release
Normal coagulation in 7–10 minutes

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Clotting (2 of 2)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Factors Affecting Clotting (1 of 2)
Movement of the wound site
Aggressive fluid therapy– Increased BP and displaced clots– Dilution of clotting factors
Low body temperature– Ineffective clot formation
Medications– ASA, heparin, Ticlid, warfarin (Coumadin)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Factors Affecting Clotting (2 of 2)
Nature of the wound– Transverse (clean tear)
Vessels constrict and draw inward
Reduction of the lumenReduction of blood loss
– Longitudinal (crush injury)Constriction of the smooth muscle
Enlarges the woundIncreases blood loss

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of ShockCellular Level

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Four Stages
Stage 1: Vasoconstriction
Stage 2: Capillary and venule opening
Stage 3: Disseminated intravascular coagulation
Stage 4: Multiple organ failure

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 1: Vasoconstriction (1 of 4)
Vasoconstriction begins as minimal perfusion to capillaries continues.– Oxygen and substrate delivery to the
cells supplied by these capillaries decreases.
– Anaerobic metabolism replaces aerobic metabolism.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 1: Vasoconstriction (2 of 4)
Production of lactate and hydrogen ions increases.– The lining of the capillaries may begin to
lose the ability to retain large molecular structures within its walls.
– Protein-containing fluid leaks into the interstitial spaces (leaky capillary syndrome).

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 1: Vasoconstriction (3 of 4)
Sympathetic stimulation produces:– Pale, sweaty skin– Rapid, thready pulse– Elevated blood glucose levels
The release of epinephrine dilates coronary, cerebral, and skeletal muscle arterioles and constricts other arterioles.– Blood is shunted to the heart, brain, skeletal
muscle, and capillary flow to the kidneys and abdominal viscera decreases.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 1: Vasoconstriction (4 of 4)
If this stage of shock is not treated by prompt restoration of circulatory volume, shock progresses to the
next stage.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 2: Capillary and Venule Opening (1 of 5)
Stage 2 occurs with a 15% to 25% decrease in intravascular blood volume. Heart rate, respiratory rate, and capillary refill are increased, and pulse pressure is decreased at this stage. Blood pressure may still be normal.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 2: Capillary and Venule Opening (2 of 5)
As the syndrome continues, the precapillary sphincters relax with some expansion of the vascular space.
Postcapillary sphincters resist local effects and remain closed, causing blood to pool or stagnate in the capillary system, producing capillary engorgement.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 2: Capillary and Venule Opening (3 of 5)
As increasing hypoxemia and acidosis lead to opening of additional venules and capillaries, the vascular space expands greatly.– Even normal blood volume may be inadequate to
fill the container.
The capillary and venule capacity may become great enough to reduce the volume of available blood for the great veins and vena cava.– Resulting in decreased venous return and a fall in
cardiac output.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 2: Capillary and Venule Opening (4 of 5)
Low arterial blood pressure and many open capillaries result in stagnant capillary flow.
Sluggish blood flow and the reduced delivery of oxygen result in increased anaerobic metabolism and the production of lactic acid.– The respiratory system attempts to compensate
for the acidosis by increasing ventilation to blow off carbon dioxide.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 2: Capillary and Venule Opening (5 of 5)
As acidosis increases and pH falls, the RBCs may cluster together (rouleaux formation).– Halts perfusion – Affects nutritional flow and prevents removal of cellular
metabolites
Clotting mechanisms are also affected, leading to hypercoagulability.
This stage of shock often progresses to the third stage if fluid resuscitation is inadequate or delayed, or if the shock state is complicated by trauma or sepsis.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 3: Disseminated Intravascular Coagulation (DIC)
(1 of 4)
Time of onset will depend on degree of shock, patient age, and pre-existing medical conditions.
Stage 3 occurs with 25% to 35% decrease in intravascular blood volume. At this stage, hypotension occurs. This stage of shock usually requires blood replacement.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 3: Disseminated Intravascular Coagulation (DIC)
(2 of 4)
Stage 3 is resistant to treatment (refractory shock), but is still reversible.Blood begins to coagulate in the microcirculation, clogging capillaries.– Capillaries become occluded by clumps of
RBCs.Decreases capillary perfusion and prevents removal of metabolites
– Distal tissue cells use anaerobic metabolism, and lactic acid production increases.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 3: Disseminated Intravascular Coagulation (DIC)
(3 of 4)
Lactic acid accumulates around the cell.– Cell membranes no longer have the
energy needed to maintain homeostasis.– Water and sodium leak in, potassium
leaks out, and the cells swell and die.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 3: Disseminated Intravascular Coagulation (DIC)
(4 of 4)
Pulmonary capillaries become permeable, leading to pulmonary edema.– Decreases the absorption of oxygen and results
in possible alterations in carbon dioxide elimination
– May lead to acute respiratory failure or adult respiratory distress syndrome (ARDS)
If shock and disseminated intravascular coagulation (DIC) continue, the patient progresses to multiple organ failure.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 4: Multiple Organ Failure (1 of 2)
The amount of cellular necrosis required to produce organ failure varies with each organ and the underlying condition of the organ.– Usually hepatic failure occurs, followed by renal failure,
and then heart failure.– If capillary occlusion persists for more than 1 to 2 hours,
the cells nourished by that capillary undergo changes that rapidly become irreversible.
In this stage, blood pressure falls dramatically (to levels of 60 mmHg or less).– Cells can no longer use oxygen, and metabolism stops.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stage 4: Multiple Organ Failure (2 of 2)
If a critical amount of the vital organ is damaged by cellular necrosis, the organ soon fails.– Failure of the liver is common and often presents early.– Capillary blockage may cause heart failure.– GI bleeding and sepsis may result from GI mucosal
necrosis.– Pancreatic necrosis may lead to further clotting disorders
and severe pancreatitis.
Pulmonary thrombosis may produce hemorrhage and fluid loss into the alveoli.– Leading to death from respiratory failure.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Shock and Hemorrhage

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Defining Shock (1 of 2)
Shock is best defined as inadequate tissue perfusion.– Can result from a variety of disease
states and injuries.– Can affect the entire organism, or it can
occur at a tissue or cellular level.
“The rude unhinging of the machinery of Life”
Gross, 1877

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Defining Shock (2 of 2)
Shock is not adequately defined by: – Pulse rate– Blood pressure– Cardiac function– Hypovolemia– Loss of systemic vascular resistance

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Classification

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
External Hemorrhage
Results from soft tissue injury.Accounts for nearly 10 million emergency department visits in the United States each year.Most soft tissue trauma is accompanied by mild hemorrhage and is not life threatening.– Can carry significant risks of patient morbidity and
disfigurement
The seriousness of the injury is dependent on:– Anatomical source of the hemorrhage (arterial, venous,
capillary)– Degree of vascular disruption– Amount of blood loss that can be tolerated by the patient

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Internal Hemorrhage (1 of 2)
Can result from:– Blunt or penetrating trauma– Acute or chronic medical illnesses
Internal bleeding that can cause hemodynamic instability usually occurs in one of four body cavities:– Chest– Abdomen– Pelvis– Retroperitoneum

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Internal Hemorrhage (2 of 2)
Signs and symptoms that may suggest significant internal hemorrhage include:– Bright red blood from mouth, rectum, or
other orifice– Coffee-ground appearance of vomitus– Melena (black, tarry stools)– Dizziness or syncope on sitting or
standing– Orthostatic hypotension

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Internal hemorrhage is associated with higher morbidity
and mortality than external hemorrhage.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Physiological Response to Hemorrhage
The body’s initial response to hemorrhage is to stop bleeding by chemical means (hemostasis).– This vascular reaction involves:
Local vasoconstriction
Formation of a platelet plug
Coagulation
Growth of tissue into the blood clot that permanently closes and seals the injured vessel

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Fick Principle
A method for measuring cardiac output.The Fick principle assumes that the quantity of oxygen delivered to an organ is equal to the amount of oxygen consumed by that organ plus the amount of oxygen carried away from that organ.Used to estimate perfusion either to an organ or to the whole body when oxygen content of both the arterial and venous blood is known and oxygen consumption is assumed to remain fixed.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Control
External Hemorrhage– Direct pressure and pressure dressing– General Management
Direct pressureElevationIcePressure pointsConstricting bandTourniquet
May use a BP cuff by inflating the cuff 20–30 mmHg above the SBPRelease may send toxins to heart
Lactic acid and electrolytes

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Tourniquets are ONLY used as a last resort!

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Internal Hemorrhage Control
Hematoma– Pocket of blood
between muscle and fascia
UNEXPLAINED SHOCK is BEST attributed to abdominal trauma
General Management– Immobilization,
stabilization, elevation
– Epistaxis: Nose BleedCauses: trauma, hypertension
Treatment: lean forward, pinch nostrils
– Hemoptysis– Esophageal Varices– Melena– Diverticulosis – Chronic Hemorrhage
Anemia

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage
60% of body weight is fluid.– 7% circulating blood volume (CBV) in
men5 L (10 units)
– 6.5% CBV in women4.6 L (9–10 units)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Stage 1
15% loss of CBV– 70 kg pt = 500–750 mL
Compensation– Vasoconstriction– Normal BP, pulse pressure, respirations– Slight elevation of pulse– Release of catecholamines
EpinephrineNorepinephrine
Anxiety, slightly pale and clammy skin

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Stage 2 (1 of 2)
15–25% loss of CBV– 750–1250 mL
Early decompensation– Unable to maintain BP– Tachycardia and tachypnea

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Stage 2 (2 of 2)
Decreased pulse strength
Narrowing pulse pressure
Significant catecholamine release– Increase PVR– Cool, clammy skin and thirst– Increased anxiety and agitation– Normal renal output

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Stage 3 (1 of 2)
25–35% loss of CBV– 1250–1750 mL
Late decompensation (early irreversible)– Compensatory mechanisms unable to
cope with loss of blood volume

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Stage 3 (2 of 2)
Classic Shock– Weak, thready, rapid pulse
Narrowing pulse pressure
– Tachypnea– Anxiety, restlessness– Decreased LOC and AMS– Pale, cool, and clammy skin

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Stage 4
>35% CBV loss– >1750 mL
Irreversible– Pulse: Barely palpable– Respiration: Rapid, shallow, and ineffective– LOC: Lethargic, confused, unresponsive– GU: Ceases– Skin: Cool, clammy, and very pale– Unlikely survival

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Concomitant Factors (1 of 2)
Pre-existing condition
Rate of blood loss
Patient Types– Pregnant
>50% greater blood volume than normal
Fetal circulation impaired when mother compensating
– AthletesGreater fluid and cardiac capacity
– ObeseCBV is based on IDEAL weight (less CBV)

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Stages of Hemorrhage Concomitant Factors (2 of 2)
Children – CBV 8–9% of body weight– Poor compensatory mechanisms– TREAT AGGRESIVELY!
Elderly– Decreased CBV– Medications
BP
Anticoagulants

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Assessment (1 of 5)
Scene Size-up– Is it safe?
BSI– Blood loss
Law enforcement
– Mechanism of Injury/Nature of IllnessShould only be used in conjunction with vital signs and other clinical signs of injury to determine the probability of injury
– Number of Patients– Need for Additional Resources

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Assessment (2 of 5)
Initial Assessment– General Impression
Obvious Bleeding
– Mental Status– CABC– Interventions
Manage as you goO2
Bleeding controlShockBLS before ALS!

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Assessment (3 of 5)
Focused H&P– Rapid Trauma Assessment
Full head to toe
Consider air medical if stage 2+ blood loss
– Focused Physical ExamGuided by c/c
– Vitals, SAMPLE, and OPQRST– Additional Assessment
Orthostatic hypotension
Tilt test: 20BP or P from supine to sitting

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Assessment (4 of 5)
Fractures and Blood Loss
Pelvic fracture:
Femur fracture:
Tibia/fibula fracture:
Hematomas and contusions:
2,000 mL
1,500 mL
500–750 mL
500 mL

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Hemorrhage Assessment (5 of 5)
Ongoing Assessment– Reassess vitals and mental status:
Q 5 min: UNSTABLE patientsQ 15 min: STABLE patients
– Reassess interventions:OxygenETIVMedication actions
– Trending: improvement vs. deteriorationPulse oximetry
End-tidal CO2 levels

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
SHOCK is…INADEQUATE TISSUE
PERFUSION.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Shock Management

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Specific Wound Considerations (1 of 2)
Head Wounds– Presentation
Severe bleeding
Skull fracture
– ManagementGentle direct pressure
Fluid drainage from ears and nose
DO NOT pack
Cover and bandage loosely
Neck Wounds– Presentation
Large vessel can entrap air
– ManagementConsider direct digital pressure
Occlusive dressing

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Specific Wound Considerations (2 of 2)
Gaping Wounds– Presentation
Multiple sitesGaping prevents uniform pressure
– ManagementBulky dressing
Trauma dressing
Sterile, non-adherent surface to woundCompression dressing
Crush Injury– Presentation
Difficult to locate source of bleedingNormal hemorrhage control mechanism non-functional
– ManagementConsider an air-splint and pressure dressingConsider tourniquet

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Transport Considerations
Consider rapid transport:– Suspected serious blood loss– Suspected serious internal bleeding– Decompensating shock
AMS, pulse, narrowing pulse pressure
– WHEN IN DOUBT, TRANSPORT.
Other Considerations– Sympathetic response– Anxiety

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Shock Management (1 of 2)
Airway and Breathing– NRB– PPV (overdrive respiration)– ET– CPAP– PEEP
Hemorrhage ControlFluid Resuscitation– Catheter size and length– Large bore– 20 mL/kg of NS or LR– Polyhemoglobins – STABILIZE VITALS to SBP of 80 mmHg or 90 mmHg in head injuries.
Any injury to the head or torso is
ALSO considered an injury to the spine.

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Shock Management (2 of 2)
Temperature Control– Conserve core temperature– Warm IV fluids
PASG– Action
Increase PVRReduce vascular volumeIncrease central CBVImmobilize lower extremities
– AssessPulmonary edemaPregnancyVital signs

Bledsoe et al., Paramedic Care Principles & Practice Volume 4:Trauma© 2006 by Pearson Education, Inc. Upper Saddle River, NJ
Summary
Introduction to Hemorrhage and Shock
Hemorrhage
Shock