Embed Size (px)
Citation preview

Blast InjuriesBlast Injuries
Amy Kaji, MD, MPHAmy Kaji, MD, MPHNovember 16, 2005November 16, 2005Acute Care College Acute Care College
Medical Student SeminarMedical Student Seminar

Iraq: Car BombingsIraq: Car BombingsCurrent Events Current Events
Historically in US…Historically in US…
• Few US bombings have caused mass casualtiesFew US bombings have caused mass casualties– First World Trade Center Attack, February 1993First World Trade Center Attack, February 1993
– Oklahoma City Bombing – April 19, 1995 Oklahoma City Bombing – April 19, 1995 • Fuel and fertilizer used to create a bomb Fuel and fertilizer used to create a bomb
• 518 injuries and 168 deaths 518 injuries and 168 deaths
– Atlanta Olympic Park Bombing, July 27, 1996Atlanta Olympic Park Bombing, July 27, 1996
– World Trade Center and PentagonWorld Trade Center and Pentagon• September 11September 11thth, 2001 , 2001
– Explosive Device Attacks at Abortion Clinics Explosive Device Attacks at Abortion Clinics

Oklahoma CityOklahoma CityApril 19, 1995April 19, 1995

New York City New York City September 11, 2001September 11, 2001

Classification of ExplosivesClassification of Explosives
• High Order (HE) Explosive High Order (HE) Explosive – Produce a high pressure shock waveProduce a high pressure shock wave– Examples include TNT, C-4, Semtex, dynamiteExamples include TNT, C-4, Semtex, dynamite
• Low Order (LE) ExplosiveLow Order (LE) Explosive– Produce a subsonic explosionProduce a subsonic explosion– Examples include pipe bombs, molotov cocktailsExamples include pipe bombs, molotov cocktails
• Manufactured ExplosiveManufactured Explosive– Standard military-issued quality-tested weaponStandard military-issued quality-tested weapon
• Improvised Explosive Device (IED) Improvised Explosive Device (IED) – Use a device outside its intended purposeUse a device outside its intended purpose– Commercial jet as a guided missileCommercial jet as a guided missile– Loaded with metallic objects to inflict penetrating injuryLoaded with metallic objects to inflict penetrating injury

Atlanta, GeorgiaAtlanta, Georgia July 27, 1996 July 27, 1996

Bag with BombBag with Bomb

Types of Blast InjuriesTypes of Blast Injuries
• Primary Primary – Due to direct effect of pressureDue to direct effect of pressure
• SecondarySecondary– Due to effect of projectiles from explosionDue to effect of projectiles from explosion
• TertiaryTertiary– Due to structural collapse and from persons being Due to structural collapse and from persons being
thrown from the blast windthrown from the blast wind• Quaternary Quaternary
– Burns, inhalation injury, exacerbations of chronic Burns, inhalation injury, exacerbations of chronic disease disease
Primary Blast InjuryPrimary Blast Injury
• Unique to high explosivesUnique to high explosives• Due to impact of over-pressurization wave with body surfacesDue to impact of over-pressurization wave with body surfaces• Most commonly involve air-filled organs and air-fluid interfacesMost commonly involve air-filled organs and air-fluid interfaces
– Middle earMiddle ear– LungsLungs– Gastrointestinal tract Gastrointestinal tract
• Types of injuries Types of injuries – Blast lung Blast lung – Tympanic Membrane (TM) rupture Tympanic Membrane (TM) rupture – Abdominal hemorrhage and perforationAbdominal hemorrhage and perforation– Globe ruptureGlobe rupture– Traumatic brain injury (TBI) without physical signs of head injuryTraumatic brain injury (TBI) without physical signs of head injury

TM InjuryTM Injury
• TM - structure most frequently injured by blast TM - structure most frequently injured by blast – TM ruptureTM rupture– Ossicle dislocationOssicle dislocation– Disruption of oval or round windowDisruption of oval or round window
• Symptoms may include hearing loss, tinnitus, Symptoms may include hearing loss, tinnitus, vertigo, bleeding from external canal, vertigo, bleeding from external canal, mucopurulent otorrheamucopurulent otorrhea
• Otologic exam and audiometry for allOtologic exam and audiometry for all• TM rupture is sensitive marker, but absence does TM rupture is sensitive marker, but absence does
not exclude other organ injurynot exclude other organ injury

TM RuptureTM Rupture

Blast LungBlast Lung
• Lung – 2Lung – 2ndnd most susceptible organ to blast injury most susceptible organ to blast injury • Most common fatal primary blast injury among Most common fatal primary blast injury among
initial survivors initial survivors • Pulmonary barotrauma includesPulmonary barotrauma includes
– Pulmonary contusionsPulmonary contusions– Systemic air embolismSystemic air embolism– Free radical associated injuries Free radical associated injuries • Thrombosis Thrombosis • Lipoxygenation Lipoxygenation • Disseminated Intravascular Coagulation (DIC) Disseminated Intravascular Coagulation (DIC)

Blast LungBlast Lung
• Clinical triad of apnea, bradycardia, and hypotension Clinical triad of apnea, bradycardia, and hypotension • Signs usually at initial presentation but may manifest as Signs usually at initial presentation but may manifest as
late as 48 hours after explosionlate as 48 hours after explosion• Should be suspected if dyspnea, cough, hemoptysis, or Should be suspected if dyspnea, cough, hemoptysis, or
chest pain chest pain • Radiographic findingsRadiographic findings
– Bihilar “butterfly” patternBihilar “butterfly” pattern– Pneumothorax or hemothoraxPneumothorax or hemothorax– Pneumomediastinum and subcutaneous emphysemaPneumomediastinum and subcutaneous emphysema
• Prophylactic chest tube before general anesthesia and air Prophylactic chest tube before general anesthesia and air transport if blast lung suspected transport if blast lung suspected

Blast LungBlast Lung

Blast Abdominal InjuryBlast Abdominal Injury
• Colon – visceral organ most frequently affectedColon – visceral organ most frequently affected• Mesenteric ischemia from gas embolism may cause Mesenteric ischemia from gas embolism may cause
delayed rupture of large or small intestinedelayed rupture of large or small intestine• Intestinal barotrauma more common with underwater air Intestinal barotrauma more common with underwater air
blast blast • Solid organ injury less likely Solid organ injury less likely • Signs and symptoms Signs and symptoms
– Abdominal pain, nausea, vomiting, hematemesisAbdominal pain, nausea, vomiting, hematemesis– Rectal pain and tenesmusRectal pain and tenesmus– Testicular painTesticular pain– Unexplained hypovolemia Unexplained hypovolemia

Blast Abdominal InjuryBlast Abdominal Injury

Other Primary Blast InjuriesOther Primary Blast Injuries
• Eye Eye – Globe rupture, serous retinitis, hyphema, lid laceration, Globe rupture, serous retinitis, hyphema, lid laceration,
traumatic cataracts, injury to optic nervetraumatic cataracts, injury to optic nerve
– Signs and symptoms include eye pain, foreign body Signs and symptoms include eye pain, foreign body sensation, blurred vision, decreased vision, drainagesensation, blurred vision, decreased vision, drainage
• Brain Brain – TBI due to barotrauma of gas embolism TBI due to barotrauma of gas embolism
– Signs and symptoms include headache, fatigue, poor Signs and symptoms include headache, fatigue, poor concentration, lethargy, anxiety, and insomnia concentration, lethargy, anxiety, and insomnia

Globe RuptureGlobe Rupture

Secondary Blast InjurySecondary Blast Injury
• Due to flying debris and bomb fragmentsDue to flying debris and bomb fragments
• Penetrating ballistic or blunt injuriesPenetrating ballistic or blunt injuries– Leading cause of death in military and civilian Leading cause of death in military and civilian
terrorist attacks except in cases of major terrorist attacks except in cases of major building collapse building collapse
– Wounds can be grossly contaminated Wounds can be grossly contaminated • Consider delayed primary closure and tetanus Consider delayed primary closure and tetanus
vaccinationsvaccinations
Tertiary Blast InjuriesTertiary Blast Injuries
• Due to persons being thrown into fixed objects by wind of Due to persons being thrown into fixed objects by wind of explosions explosions
• Also due to structural collapse and fragmentation of Also due to structural collapse and fragmentation of building and vehiclesbuilding and vehicles
• Structural collapse may cause extensive blunt traumaStructural collapse may cause extensive blunt trauma– Crush syndrome Crush syndrome
• Damage to muscles and subsequent release of myoglobin, urates, Damage to muscles and subsequent release of myoglobin, urates, potassium, and phosphatespotassium, and phosphates
• Oliguric renal failure Oliguric renal failure – Compartment syndrome Compartment syndrome
• Edematous muscle in an inelastic sheath promotes local ischemia, Edematous muscle in an inelastic sheath promotes local ischemia, further swelling, increased compartment pressures, decreased tissue further swelling, increased compartment pressures, decreased tissue perfusion, and further ischemia perfusion, and further ischemia

Crush and Compartment SyndromeCrush and Compartment Syndrome

Potential Intra-operative and Post-Potential Intra-operative and Post-resuscitation Complicationsresuscitation Complications
• Surgeons, Anesthesiologists, and Critical Surgeons, Anesthesiologists, and Critical Care Specialists will need to be aware of Care Specialists will need to be aware of potential intraoperative and post-potential intraoperative and post-resuscitation complicationsresuscitation complications– Occult pneumothoraxOccult pneumothorax– Occult compartment syndromeOccult compartment syndrome– Hyperkalemia Hyperkalemia • Crush syndromeCrush syndrome• Rhabdomyolysis Rhabdomyolysis

Quaternary Blast InjuriesQuaternary Blast Injuries
• Explosion related injuries or illnesses not due to Explosion related injuries or illnesses not due to primary, secondary, or tertiary injuries primary, secondary, or tertiary injuries – Exacerbations of preexisting conditions, such as Exacerbations of preexisting conditions, such as
asthma, COPD, CAD, HTN, DM, etc.asthma, COPD, CAD, HTN, DM, etc.– Burns (chemical and thermal) Burns (chemical and thermal) • White Phosphorous (WP) from munitions causes extensive White Phosphorous (WP) from munitions causes extensive
burns, hypocalcemia and hyperphosphatemia burns, hypocalcemia and hyperphosphatemia
– Toxic inhalationToxic inhalation– Radiation exposureRadiation exposure– Asphyxiation (carbon monoxide and cyanide) Asphyxiation (carbon monoxide and cyanide)

Madrid, Spain Madrid, Spain March 11, 2004 March 11, 2004

General ConsiderationsGeneral Considerations
• Information about distance from and type of Information about distance from and type of explosion predict injury severity and type explosion predict injury severity and type – Confined space vs. open space Confined space vs. open space • Increased number of penetrating and primary blast injuries if Increased number of penetrating and primary blast injuries if
closed spaceclosed space
– Intensity of explosion pressure wave declines with Intensity of explosion pressure wave declines with cubed root of distance away from explosive cubed root of distance away from explosive • Standing at 3m has 9x greater pressure than if at 6mStanding at 3m has 9x greater pressure than if at 6m
– Blast wave reflected by solid surfaces Blast wave reflected by solid surfaces • Person next to a wall may sustain a greater primary blast Person next to a wall may sustain a greater primary blast
injury injury

General ConsiderationsGeneral Considerations
• Half of all initial casualties seek medical care over Half of all initial casualties seek medical care over first hour first hour
• Expect upside down triage Expect upside down triage – Most severely injured arrive after less injured who Most severely injured arrive after less injured who
bypass EMS and self-transport to closest hospitals bypass EMS and self-transport to closest hospitals
• Secondary devices Secondary devices – Initial explosion attracts law enforcement and rescue Initial explosion attracts law enforcement and rescue
personnel who will be injured by second explosionpersonnel who will be injured by second explosion

London, EnglandLondon, England July 7, 2005 July 7, 2005

General ManagementGeneral Management
• Focus on two examsFocus on two exams• Otoscopic exam Otoscopic exam
– If ruptured TM, chest radiography and eight hour If ruptured TM, chest radiography and eight hour observation recommendedobservation recommended• Primary blast injury notorious for delayed presentation Primary blast injury notorious for delayed presentation
– If nonruptured TM and no other symptoms, may If nonruptured TM and no other symptoms, may conditionally exclude other serious primary blast conditionally exclude other serious primary blast injuries injuries
• Pulse oximetry Pulse oximetry – Decreased oxygen saturation signals early blast lung Decreased oxygen saturation signals early blast lung
even before symptoms even before symptoms

Treatment of Blast LungTreatment of Blast Lung
• High inspiratory pressures increase risk of High inspiratory pressures increase risk of air embolism and pneumothorax air embolism and pneumothorax – Ventilation should use limited inspiratory Ventilation should use limited inspiratory
pressures pressures
– Permissive hypercapniaPermissive hypercapnia
– High frequency ventilation may be of value High frequency ventilation may be of value

PneumothoraxPneumothorax

Treatment of TM ruptureTreatment of TM rupture
• Generally expectant management Generally expectant management – Most resolve spontaneously Most resolve spontaneously
– Avoid irrigating or probing the auditory canalAvoid irrigating or probing the auditory canal
– Avoid swimming Avoid swimming
– Refer to ENT if no healing or complications occurRefer to ENT if no healing or complications occur• Complications include ossicle disruption, cholesteatoma, Complications include ossicle disruption, cholesteatoma,
perilymphatic fistula, and permanent hearing loss (1/3)perilymphatic fistula, and permanent hearing loss (1/3)
• Steroids may be helpful in sensorineural hearing Steroids may be helpful in sensorineural hearing lossloss

Treatment for Acute Gas Embolism Treatment for Acute Gas Embolism (AGE)(AGE)
• Recompression with 100% oxygen Recompression with 100% oxygen • Left lateral recumbent positionLeft lateral recumbent position• Hyperbaric oxygen (HBO) is definitiveHyperbaric oxygen (HBO) is definitive
– Transfer may be necessary Transfer may be necessary
• Aspirin may be helpful in AGE Aspirin may be helpful in AGE – May reduce inflammation-mediated injury in May reduce inflammation-mediated injury in
pulmonary barotrauma pulmonary barotrauma • Weigh bleeding risk in acute trauma settingWeigh bleeding risk in acute trauma setting

AGEAGE

Treatment of Eye InjuriesTreatment of Eye Injuries
• 28% of blast survivors sustain eye injuries28% of blast survivors sustain eye injuries
• Objects penetrating eye (or any other body part) Objects penetrating eye (or any other body part) should not be removed in an emergency setting should not be removed in an emergency setting – Cover affected eye with a paper cup that will not exert Cover affected eye with a paper cup that will not exert
pressure on the globe pressure on the globe
– Remove object in operating room under controlled Remove object in operating room under controlled conditions conditions
– Refer patient to ophthalmology for definitive treatment Refer patient to ophthalmology for definitive treatment

Treatment of BurnsTreatment of Burns
• Cover burns to minimize heat and fluid loss Cover burns to minimize heat and fluid loss • WP burns require special management WP burns require special management
– Copious lavage and removal or particles and debrisCopious lavage and removal or particles and debris– Rinse with 1% copper sulfate solutionRinse with 1% copper sulfate solution
• Combines with phosphorous particles and impedes further Combines with phosphorous particles and impedes further combustioncombustion
– Cardiac monitor Cardiac monitor • Hypokalemia and hyperphsophatemia commonHypokalemia and hyperphsophatemia common
– Use moistened face masks to protect from phosphorous pentoxide Use moistened face masks to protect from phosphorous pentoxide gas exposure gas exposure
– Avoid use of flammable anesthetic agents and excessive oxygenAvoid use of flammable anesthetic agents and excessive oxygen

WP Smoke Hand GrenadeWP Smoke Hand Grenade
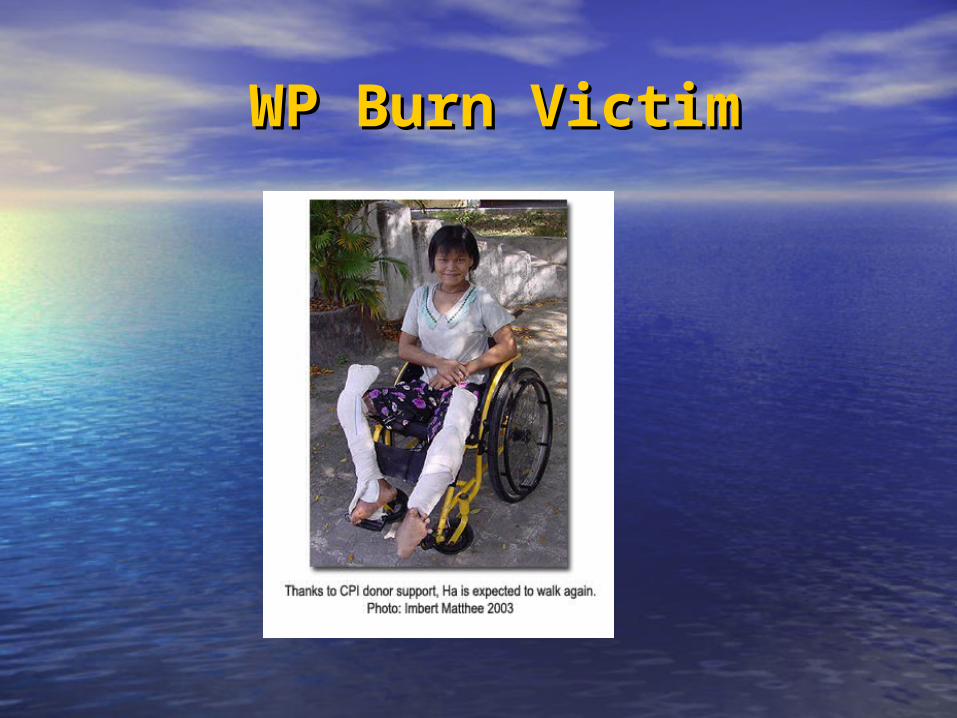
WP Burn VictimWP Burn Victim

Special PopulationsSpecial Populations
• Pediatric trauma due to terrorism vs. pediatric trauma due Pediatric trauma due to terrorism vs. pediatric trauma due to non-terrorism related events to non-terrorism related events – Increased use of Intensive Care Unit (ICU) resourcesIncreased use of Intensive Care Unit (ICU) resources– Higher injury severity scores (ISS)Higher injury severity scores (ISS)– Longer hospital staysLonger hospital stays
• Pregnancy Pregnancy – Direct injury to fetus is uncommonDirect injury to fetus is uncommon– Fetus protected by amniotic fluid Fetus protected by amniotic fluid – Fetal attachment to placenta is tenuousFetal attachment to placenta is tenuous
• Risk for placental abruptionRisk for placental abruption
– If blast in second or third trimester admit to labor and delivery for If blast in second or third trimester admit to labor and delivery for fetal monitoring fetal monitoring
Guidelines for DispositionGuidelines for Disposition
• Limited data prevent establishing optimal duration of Limited data prevent establishing optimal duration of observationobservation
• Low riskLow risk and may be discharged with strict precautions and may be discharged with strict precautions after four hours of observation:after four hours of observation:– Persons exposed to open-space explosions with no apparent Persons exposed to open-space explosions with no apparent
significant injury, normal vital signs and unremarkable lung and significant injury, normal vital signs and unremarkable lung and abdominal examinationabdominal examination
• Moderate riskModerate risk and should be observed for longer periods and should be observed for longer periods of time for delayed complications:of time for delayed complications:– Persons exposed to closed-space explosion or in-water explosionsPersons exposed to closed-space explosion or in-water explosions– Persons with TM rupturePersons with TM rupture

Guidelines for AdmissionGuidelines for Admission
• High risk patients who require admissionHigh risk patients who require admission– Significant burnsSignificant burns– Suspected air embolismSuspected air embolism– Radiation Radiation – WP contaminationWP contamination– Abnormal vital signsAbnormal vital signs– Abnormal lung examination findingsAbnormal lung examination findings– Clinical or radiographic evidence of pulmonary contusion or Clinical or radiographic evidence of pulmonary contusion or
pneumothoraxpneumothorax– Abdominal pain or vomiting Abdominal pain or vomiting – Penetrating injuries to the thorax, abdomen, neck, or cranial Penetrating injuries to the thorax, abdomen, neck, or cranial
cavity cavity

Selected ReferencesSelected References
• Arnold JL, Halperin P, Tsai MC, Smithline H. Mass casualty terrorist Arnold JL, Halperin P, Tsai MC, Smithline H. Mass casualty terrorist bombings: a comparison of outcomes by bombing type. Ann Emerg Med bombings: a comparison of outcomes by bombing type. Ann Emerg Med 2004;43:263-73. 2004;43:263-73.
• DePalma RG, Burris DG, Champion HR, Hodgson MJ. Blast Injuries. N Engl DePalma RG, Burris DG, Champion HR, Hodgson MJ. Blast Injuries. N Engl J Med 2005; 352:1335-42. J Med 2005; 352:1335-42.
• Hogan DE, Waeckerle JF, Dire DJ, Lillebridge ST. Emergency department Hogan DE, Waeckerle JF, Dire DJ, Lillebridge ST. Emergency department impact of the Oklahoma City terrorist bombing. Ann Emerg Med 1999; impact of the Oklahoma City terrorist bombing. Ann Emerg Med 1999; 34:160-7. 34:160-7.
• Karmy-Jones R, Kissinger D, et. al. Bombing related injuries. Mil Med Karmy-Jones R, Kissinger D, et. al. Bombing related injuries. Mil Med 1994;159:536-9. 1994;159:536-9.
• Lavanos E. Blast Injuries. (Accessed September 21, 2005, at Lavanos E. Blast Injuries. (Accessed September 21, 2005, at http://www.emedicine.com/emerg/topic63.htmhttp://www.emedicine.com/emerg/topic63.htm .). .).
• Wightman JM, Gladish SL. Explosions and blast injuries: a primer for Wightman JM, Gladish SL. Explosions and blast injuries: a primer for clinicians. Atlanta: Centers for Disease Control and Prevention. (Accessed clinicians. Atlanta: Centers for Disease Control and Prevention. (Accessed September 21, 2005, at September 21, 2005, at http://www.cdc.gov/masstrauma/preparedness/primer.pdfhttp://www.cdc.gov/masstrauma/preparedness/primer.pdf .).)











![one way MACHINE 2011 /8 97 T-REV] Hiroyuki Kaji …one way MACHINE 2011 /8 97 T-REV] Hiroyuki Kaji (BiG MACHINE) tñJfiE0 btcJ httpth](https://img.pdfslide.us/doc/110x75/5f293c37adc7166f4225e226/one-way-machine-2011-8-97-t-rev-hiroyuki-kaji-one-way-machine-2011-8-97-t-rev.jpg)