Embed Size (px)
Citation preview

Blair County Heal thChoices
Annual Report2009 - 2010

2 Blair County HealthChoices Program
ContentsCounty CommissionersTerry Tomassetti, ChairpersonDiane L. Meling, Vice-ChairpersonDonna D. Gority, Secretary
Board of DirectorsNancy Imes, ChairpersonMaryanne Burger, Vice-ChairpersonKathleen Wallace, Secretary/TreasurerDonna D. GorityBob KuntzJames Hudack
Management GroupBlaine L. Smith, Executive DirectorAmy Marten-Shanafelt, Clinical DirectorNicole L. Hess, ControllerJennifer Way, Quality Assurance Specialist
HealthChoicesEnrollmentServicesUtilization All Members YouthAverage Cost per MemberDenials and ComplaintsGrievancesArticles Myths and Facts about Mental Illnesses The Recovery ModelTerminology
3 4 5
5-7 8 9 10 11
12
1314-15
BLAIR

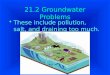
21243
21,509
22,378
FY 2007-2008 FY 2008-2009 FY 2009-2010
HealthChoices is the Commonwealth of Pennsylvania’s mandatory Medicaid managed care program administered by the Department of Public Welfare (DPW). This new, integrated and coordinated health care delivery system was introduced by the Commonwealth to provide medical, psychiatric, and substance abuse services to Medical Assistance (Medicaid) recipients.
The needs of the high risk populations included in the HealthChoices managed care program requires broad-based coordination to assure appropriate access, service utilization, and continuity of care for persons with serious mental illness and/or addictive diseases. Because of the cross-cutting coordination needs of Medical Assistance recipients, the unique structure of the behavioral health and human service delivery systems administered by the counties, and their over 30 years experience in administering behavioral health services programs, it was determined that county government would be offered the right-of-first opportunity to enter into a capitated contract with the Commonwealth.
As of July 1, 2007, Blair County accepted the right-of-first- opportunity to manage the local program and entered into a full-risk capitation contract with the Commonwealth. The County formed a 501(c)(3) corporation called Central PA Behavioral Health Collaborative, Inc. d/b/a Blair HealthChoices, which manges the local program.
Blair HealthChoices sub-contracts with a behavioral managed care organization, Community Behavioral Health Network of Pennsylvania (CBHNP). Services provided by CBHNP include care management, provider network development, quality assurance, member services, and claims management. Blair HealthChoices provides oversight and monitoring of all of CBHNP’s activities to ensure full compliance with its contract with DPW.
This summary presents data for the Fiscal Year beginning July 1, 2009 and ending June 30, 2010.
HEALTHCHOICES
Annual Report 2009-2010 3
Blair HealthChoicesEligible Members on Last Day of Fiscal Year
FY 2007-2008 through 2009-2010
Approximately 20% of the total population of Blair County received Medicaid benefits according to the Pennsylvania Medicaid Policy Center, July 2009.

Enrollment
4 Blair County HealthChoices Program
Categories of Aid:Temporary Assistance to Needy Families (TANF) Assistance to families with dependent children who are deprived of the care or support of one or both parents.
Healthy Beginnings Assistance for women during pregnancy and the postpartum period.
State Only General Assistance State funded program for individuals and families whose income and resources are below established standards and who do not qualify for the TANF program. This includes the Categorically Needy (CNO) and Medically Needy Only (MNO) groups.
Federally Assisted Medical Assistance for General Assistance Recipients Federal and state funded program for individuals and families whose income and resources are below established standards and who do not qualify for the TANF program.
Supplemental Security Income without Medicare Assistance for people who are aged, blind, or determined disabled for less than two years.
Supplemental Security Income with Medicare Assistance for people who are aged, blind or determined disabled for over two years.
Female 12,553 56.1%
Male 9,825 43.9%
African American
1,005 4.5%
Caucasian 21,048 94.0%
Other 325 1.5%
Federal General Assistance
275 1.2%
Healthy Beginnings 4,580 20.5%
Medically Needy 219 1.0%
SSI without Medicare
5,326 23.8%
SSI with Medicare 3,333 14.9%
Categorically Needy 443 2.0%
TANF 8,202 36.6%
Age 0 to 5 3,917 17.5%
Age 6 to 12 3,878 17.3%
Age 13 to 17 2,265 10.1% Age 18 to 20
1,347 6.0%
Age 21 to 44 6,153 27.6%
Age 45 to 64 3,539 15.8%
Age 65 and older 1,279 5.7%

Annual Report 2009-2010 5
ServicesHealthChoices members are eligible to receive in-plan services offered by their choice of at least two service providers as well as additional services that have been approved for use by the Blair HealthChoices Program.
In-Plan Services:
• Inpatient Psychiatric Hospitalization• InpatientDrug&AlcoholDetoxification,Treatment,Non-HospitalRehabilitation,andHalfwayHouse• Psychiatric Partial Hospitalization Services• Outpatient Mental Health and Drug & Alcohol Counseling• Laboratory and Diagnostic Services• Medication Management and Clozapine Support• Psychiatric Evaluation and Psychological Testing• Residential Treatment Facilities for Adolescents (RTF)• Behavioral Health Rehabilitative Services for Children and Adolescents (BHRS)• Methadone Maintenance• Intensive Case Management• Resource Coordination• Crisis Intervention• Family Based Mental Health Services• Peer Support Services• Mobile Mental Health Treatment
Supplemental Services:
• Drug & Alcohol Level of Care Assessment• Drug & Alcohol Intensive Outpatient• Drug & Alcohol Targeted Case Management• Drug & Alcohol Partial Hospitalization• Psychiatric Rehabilitation• Children’s Services enrolled as Program Exceptions Multi-Systemic Therapy (MST) Functional Family Therapy (FFT) Multidimensional Treatment Foster Care (MTFC)
UtilizationGender
Members Served: 5,818Total Expenditures: $25,038,343
Female 3,105 53.4%
Male 2,713 46.6%
Female $9,657,440
38.6%
Male $15,380,903
61.4%

Utilization
6 Blair County HealthChoices Program
Age Groups
Level of Care
Members Served: 5,818Total Expenditures: $25,038,343
**The Other service category is comprised of supplemental services,
such as Drug & Alcohol Partial Hospital, Assertive Community Treatment Team,
and Children’s Services Program Exceptions.
BHRS 1,004 10.4%
Community Support Svcs
1,829 18.9%
D&A Rehabilitation 204 2.1%
Inpatient MH 526 5.4%
Other-Supplemental Svcs
940 9.7%
Outpatient D&A 755 7.8%
Outpatient MH 4,374 45.4%
RTF 31
0.3%
BHRS $8,413,432
33.6%
Community Support Svcs $3,780,230
15.1%
D&A Rehabilitation $1,200,742
4.8%
Inpatient MH $4,070,247
16.3%
Other-Supplemental Svcs
$1,108,920 4.4%
Outpatient D&A $1,385,465
5.5%
Outpatient MH $3,196,567
12.8%
RTF $1,882,740
7.5%
Age 0-5 336 5.8%
Age 6-12 1,032 17.7%
Age 13-17 725
12.5%
Age 18-20 305 5.2%
Age 21-44 2,236 38.4%
Age 45-64 1,088 18.7%
Age 65+ 96
1.7%
Age 0-5 $1,897,903
7.6%
Age 6-12 $7,914,613
31.5%
Age 13-17 $5,922,351
23.7%
Age 18-20 $972,106
3.9%
Age 21-44 $5,661,172
22.6%
Age 45-64 $2,618,224
10.5%
Age 65+ $51,974
0.2%

Alcohol 240
21.2%
Cannabis 84
7.4%
Cocaine 25
2.2%
Opioid 574
50.8%
Other D&A 208
18.4%
Annual Report 2009-2010 7
**Other Mental Health/Drug & Alcohol Disorders include dementia, drug or alcohol psychosis, drug or alcohol withdrawal, delirium, organic psychotic or non-psychotic
conditions, personality disorders, eating disorders, sleep disorders, tic disorders, child abuse, mental retardation, mental disorders due to unknown causes, transient organic mental disorders, amphetamine abuse/dependence, hallucinogen abuse/dependence,
inhalant abuse/dependence, sedative-hypnotic/anxiolytic abuse/dependence, polysubstance abuse/dependence.
Mental Health Members Served: 5,254 Total Expenditures: $21,984,882
Mental Health Diagnoses
Drug & Alcohol Members Served: 1,008 Total Expenditures: $3,053,462
Drug & Alcohol Diagnoses
UtilizationADHD/Conduct
1,441 17.3%
Adjustment 942
11.3%
Anxiety 777 9.3%
Autism Spectrum 322 3.9% Bipolar
1,118 13.5%
Depression 2,104 25.4%
Other MH 1,148 13.8%
Schizophrenia/ Psychosis
459 5.5%
Alcohol $450,321
14.7%
Cannabis $164,900
5.4% Cocaine $29,545
1.0%
Opioid $1,822,354
59.7%
Other D&A $586,341
19.2%
ADHD/Conduct $5,455,146
24.8%
Adjustment $1,904,137
8.7%
Anxiety $637,128
2.9%
Autism Spectrum $4,185,425
19.0%
Bipolar $3,067,034
14.0%
Depression $4,736,426
21.5%
Other MH $495,770
2.3%
Schizophrenia/ Psychosis
$1,503,816 6.8%

BHRS 1,004 27.3%
D&A Rehabilitation 8
0.2% Community Support Svcs
718 19.6%
Inpatient MH 127 3.4%
Supplemental Svcs 223 6.0%
Outpatient Svcs 1,576 42.7% RTF
31 0.8%
8 Blair County HealthChoices Program
Youth
Included in the Youth category are all HealthChoices members under age 18 and all members involved in BHRS or RTF services
Youth Served: 2,124Total Expenditures: $16,038,997
**The Supplemental service category is comprised of supplemental services, such as Drug & Alcohol Partial Hospital, Assertive Community Treatment Team, and Children’s Services Program Exceptions.
Utilization
BHRS $8,413,432
52.5%
D&A Rehabilitation $98,435
0.6%
Community Support Svcs $2,608,943
16.3%
Inpatient MH $1,380,278
8.6%
Supplemental Svcs $97,408
0.6%
Outpatient Svcs $1,557,760
9.7%
RTF $1,882,740
11.7%

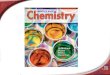
Average Cost per Member
$541
$2,406
$2,532
$3,187
$8,169
$7,669
$5,649
$730
$1,815
$2,403
$3,465
$8,485
$7,848
$4,736
Age 65+
Age 45-64
Age 21-44
Age 18-20
Age 13-17
Age 6-12
Age 0-5
Blair HealthChoices Average Cost per Member by Age Group
08-09 CPM 09-10 CPM
$60,734
$731
$1,835
$1,180
$7,738
$5,886
$2,067
$8,380
$59,803
$622
$1,720
$311
$7,352
$4,764
$1,961
$8,559
RTF
Outpatient MH
Outpatient D&A
Other-Supplemental Svcs
Inpatient MH
D&A Rehabilitation
Community Support Svcs
BHRS
Blair HealthChoices Average Cost per Member by Level of Care
2008-09 2009-10
Annual Report 2009-2010 9

127 126
144 146
72
57 65
37
Quarter 12008-09
Quarter 22008-09
Quarter 32008-09
Quarter 42008-09
Quarter 12009-10
Quarter 22009-10
Quarter 32009-10
Quarter 42009-10
Quality Assurance
8
4
7
6
8
5 5
3
Quarter 12008-09
Quarter 22008-09
Quarter 32008-09
Quarter 42008-09
Quarter 12009-10
Quarter 22009-10
Quarter 32009-10
Quarter 42009-10
10 Blair County HealthChoices Program
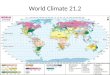
A service may be denied in full, a lesser amount of the service may be approved,
or a different level of care may be authorized. Only a small percentage of
authorization requests are totally denied. The overall trend for service denials
decreased significantly as the 2009-2010 operating year progressed.
Blair HealthChoices closely monitors com-plaints filed by HealthChoices members. Only a small number of complaints were
filed during the 2009-2010 operating year and each was resolved to the satisfaction
of the involved member.
Authorization Denials by QuarterFiscal Years 2008-09 through 2009-10
Member Complaints File by QuarterFiscal Years 2008-09 through 2009-10

43 40
52
41
21
17 17
13
Quarter 12008-09
Quarter 22008-09
Quarter 32008-09
Quarter 42008-09
Quarter 12009-10
Quarter 22009-10
Quarter 32009-10
Quarter 42009-10
6
10
18
15
7
3 3 2
Quarter 12008-09
Quarter 22008-09
Quarter 32008-09
Quarter 42008-09
Quarter 12009-10
Quarter 22009-10
Quarter 32009-10
Quarter 42009-10
Annual Report 2009-2010 11
Members who are dissatisfied with treat-ment decisions may opt to file grievances
to have the decisions changed. There are two grievance levels and an external
review process. Additionally, a member may also choose to file a request for a
Fair Hearing at any point during the griev-ance process.
Level II Grievances Filed by QuarterFiscal Years 2008-09 through 2009-10
Level I Grievances Filed by QuarterFiscal Years 2008-09 through 2009-10

Myth: Mental illnesses are brought on by a weakness of character.Fact: Mental illnesses are a product of the interaction of biological, psychological, and social factors. Research has shown genetic and biological factors are associated with schizophrenia, depression, and alcoholism. Social influences, such as loss of a loved one or a job, can also contribute to the development of various disorders.
Myth: People with mental illnesses cannot tolerate the stress of holding down a job.Fact: In essence, all jobs are stressful to some extent. Productivity is maximized when there is a good match between the employee’s needs and working conditions,
whether or not the individual has mental health needs.
Myth: Once people develop mental illnesses, they will never recover.Fact: Studies show that most people with mental illnesses get better, and many recover completely. Recovery refers to the process in which people are able to live, work, learn, and participate fully in their communities. For some individuals, recovery is the ability to live a fulfilling and productive life. For others, recovery implies the reduction or complete remission of symptoms. Science has shown that having hope plays an integral role in an individual’s recovery.
Myth: Therapy and self-help are wastes of time. Why bother when you can just take one of those pills you hear about on TV? Fact: Treatment varies depending on the individual. A lot of people work with therapists, counselors,
their peers, psychologists, psychiatrists, nurses, and social workers in their recovery process. They also use self-help strategies and community supports. Often these methods are combined with some of the most advanced medications available.
Myth: Children do not experience mental illnesses. Their actions are just products of bad parenting.Fact: A report from the President’s New Freedom Commission on Mental Health showed that in any given year 5-9 percent of children experience serious emotional disturbances. Just like adult mental illnesses, these are clinically diagnosable health conditions that are a product of the interaction of biological, psychological, social, and sometimes even genetic factors.
Department of Health and Human Services, 2006
It’s important to learn the facts about mental illnesses to stop discrimination and to begin treating people with mental illnesses with respect and dignity. Here are some common myths and facts about mental health.
Myth: There’s no hope for people with mental illnesses.Fact: There are more treatments, strategies, and community supports than ever before, and even more are on the horizon. People with mental illnesses lead active, productive lives.
Myth: I can’t do anything for someone with mental health needs.Fact: You can do a lot, starting with the way you act and how you speak. You can nurture an environment that builds on people’s strengths and promotes good mental health. For example: Avoid labeling people with words like “crazy,” “wacko,” “loony,” or by their diagnosis. Instead of saying someone is a “schizophrenic” say “a person with schizophrenia.” Learn the facts about mental health and share them with others, especially if you hear something that is untrue. Treat people with mental illnesses with respect and dignity, as you would anybody else. Respect the rights of people with mental illnesses and don’t discriminate against them when it comes to housing, employment, or education. Like other people with disabilities, people with mental health needs are protected under Federal and State laws.
Myth: People with mental illnesses are violent and unpredictable.Fact: In reality, the vast majority of people who have mental health needs are no more violent than anyone else. You probably know someone with a mental illness and don’t even realize it.
Myth: Mental illnesses cannot affect me.Fact: Mental illnesses are surprisingly common; they affect almost every family in America. Mental illnesses do not discriminate—they can affect anyone.
Myth: Mental illness is the same as mental retardation.Fact: The two are distinct disorders. A mental retardation diagnosis is characterized by limitations in intellectual functioning and difficulties with certain daily living skills. In contrast, people with mental illnesses—health conditions that cause changes in a person’s thinking, mood, and behavior—have varied intellectual functioning, just like the general population.
Myths and Facts About Mental Illnesses
12 Blair County HealthChoices Program

The Recovery Model refers to the process of recovery from a mental health disorder or substance dependence, and/or from being labeled in those terms. Recovery has been defined as “an individual’s journey of healing and transformation to live a meaningful life in a community of his or her choice while striving to achieve maximum human potential” (U.S. Department of Health and Human Services, 2005). It incorporates a philosophy of support, respect, empowerment, choice, hope, and social inclusion. Originating in programs to overcome substance dependency, the concept of recovery in mental health usage emerged from deinstitutionalization resulting in more individuals living in community settings but there being a perceived failure to support full recovery or enable proper integration into the community in a meaningful manner. The recovery model is a form of social model of disability by contrast to a medical model of disability and may involve “consumers” and “survivors” of mental health service as well as mental health professionals.
In general medicine or psychiatry, recovery has long been used to refer to the end of a particular experience of illness. In the context of long-term conditions, it might refer to a period of remission and therefore potentially relapse.
The concept of full ‘recovery’ as a general philosophy first became popular in relation to substance use programs, including 12-step approaches. Application of full recovery concepts to psychiatric disorders is comparatively recent and stems largely from two interrelated sources: the consumer/survivor movement, a grassroots self-help and advocacy initiative, and psychiatric rehabilitation, a professional approach to mental health services provision. It has emerged as a significant paradigm shift in the field of mental health and became increasingly implemented in the policies and practices of mental health systems. The recovery model has been said to be based on the premise that all consumers have the capacity to improve and develop a life distinct from illness. Scientific and consumer models of recovery have differences and commonalities; the consumer model of recovery involves a nonlinear process in which an individual gradually adapts to and moves beyond what may be termed an illness, while scientific and clinical models typically view recovery as an outcome, primarily involving reduced symptoms and improved functional capacity (sustained for a particular duration, for example two years). Scientific-professional views also place considerable emphasis on the role of treatment, especially including maintenance pharmacotherapy, while the consumer model places greater emphasis on peer support and personal experience.
Hope is a feature proposed to be important, including a realistic openness to failure, disappointment and possible relapse along the way. Recovery can be seen as an individual experience; a fundamental change in the concept of self. For many, “recovery” has a political as well as personal implication, where to recover is to find meaning, to challenge prejudice, to reclaim a chosen life and place within society, to validate the self. Recovery can thus be viewed as one manifestation of empowerment. An empowerment model of recovery may emphasize that conditions are not necessarily permanent, that other people have recovered who can be role models and share experiences, and symptoms can be understood as expressions of distress related to lack of a connection on a deep emotional level to the people around them, involving loss and trauma and interruption in social development. One such model from the US National Empowerment Center advances 10 such principles of recovery framed within a cognitive-behavioral approach.In psychiatric rehabilitation, the concept of recovery has often been used in a more limited way to refer to functional criteria and reduction of psychosocial disability. To recover is to improve and maintain personal capacity in one or more of the major domains of life, whether it be work, housing, relationships, or recreation. Psychiatric rehabilitation also focuses on individuals’ role performance.
The recovery model has been supported by evidence from both quantitative and qualitative research. Long term (longitudinal) studies have shown that a psychiatric disorder does not necessarily take a course of inevitable deterioration and that, for a significant number of people, a return to full potential is possible. Other research, including studies of reports by consumers/survivors of mental health services, has identified resilience and resourcefulness, diverse and individual pathways of healing, and factors which can enhance or detract from recovery. Increasingly, recovery has become both a subject of mental health services research and a term that is emblematic of many of the goals of the consumer/survivor movement. Specific policy and clinical strategies are currently being used to implement recovery principles although key questions remain.
The Recovery Model
Annual Report 2009-2010 13

ADMISSION RATEThe number of admissions into services per 1000 HealthChoices enrollees.
AUTHORIZATIONA process that is related to the payment of claims by which a provider receives approval from CBHNP to provide a particular service. Authorizations typically limit the number of units and the time in which the service can be provided. If a service requires authorization for payment, the lack of authorization will result in an unpaid claim.
CAPITATIONA set amount of money received or paid out; it is based on membership rather than on services delivered and is usually expressed in units of PMPM (per member per month) or PMPD (per member per day). Under the HealthChoices program, capitation rates vary by categories of assistance.
CLAIMSA request for reimbursement for a behavioral health service.
COMMUNITY RESIDENTIAL REHABILITATION (CRR)CRRs are residential programs designed and operated to assist persons with chronic psychiatric disability to live as independently as possible in the least restrictive setting.
COMPLAINTA process by which a consumer or provider can address a problem experienced in the HealthChoices program.
CONSUMERHealthChoices enrollees on whose behalf a claim has been adjudicated for behavioral health care services during the reporting period.
DENIALA denial is defined as “a determination made by a managed care organization in response to a provider’s request for approval to provide in-plan services of a specific duration and scope which (1) disapproves the request completely; (2) approves provision of the requested service(s), but for a lesser scope or duration than requested by the provider; (an approval of a requested service which includes a requirement for a concurrent review by the BHMCO during the authorized period does not constitute a denial); or (3) disapproves provision of the requested service(s), but approves provision of an alternative service( s).”
DIAGNOSISA behavioral health disorder based on DSM-IV-TR or ICD-9 diagnostic criteria.
DIAGNOSTIC CATEGORIESSubgroups of behavioral health disorders. This report contains the following groupings:
Bipolar Disorders – a group of mood disorders that characteristically involve mood swings. This group includes: Bipolar I Disorder, Bipolar II Disorder, Bipolar Disorder Not Otherwise Specified, Mood Disorder, andMood Disorder Not Otherwise Specified. DepressiveDisorders – a group of mood disorders that includes Major Depressive Disorder, Dysthymia, and Depressive Disorder Not Otherwise Specified.
Schizophrenia and Psychotic Disorders – a collection of thought disorders such as Schizophrenia, Schizoaffective Disorder, Schizophreniform Disorder,and Psychotic Disorder Not Otherwise Specified.
Anxiety Disorders – a group of disorders that includes: Panic Disorder, Social Phobia, Posttraumatic Stress Disorder, Obsessive Compulsive Disorder, Generalized Anxiety Disorder, and Anxiety Disorder Not Otherwise Specified.
Adjustment Disorder – the development of clinically significant emotional or behavioral symptoms inresponse to an identifiable psychosocial stressor orstressors.
Impulse Control Disorders – includes Intermittent Explosive Disorder, Trichotillomania, and Impulse Control Disorder Not Otherwise Specified.
ADHD and Disorders in Children – includes Attention Deficit Hyperactivity Disorder, Conduct Disorder,Oppositional Defiant Disorder, and DisruptiveBehavior Disorder Not Otherwise Specified.
Terminology
14 Blair County HealthChoices Program

HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT OF 1996 (HIPAA)This is a Federal law that allows persons to qualify immediately for comparable health insurance coverage when they change their employment relationships. Title II, Subtitle F, of HIPAA gives the Health and Human Services Department of the federal government the authority to mandate the use of standards for the electronic exchange of health care data; to specify what medical and administrative code sets should be used within those standards; to require the use of national identification systems for health care patients, providers, payers (or plans), and employers (or sponsors); and to specify the types of measures required to protect the security and privacy of personally identifiable health care information.
MEMBEREligible Medical Assistance recipients enrolled in the HealthChoices program during the reporting period.
MENTAL HEALTH COMMITMENTAn involuntary admission into a psychiatric hospital as per the Pennsylvania Mental Health Procedures Act. Also referred to as a ‘302 commitment’.
OUTPATIENT REGISTRATIONThe process by which HealthChoices members are registered with CBHNP to receive specific outpatient services. eliminating the need for pre-authorization.
RESIDENTIAL TREATMENT FACILITY (RTF)A self-contained, secure, 24-hour psychiatric residence for children and adolescents who require intensive clinical, recreational, educational services and supervision.
UTILIZATIONThe amount of behavioral health care services used by Medicaid recipients. Utilization is based on encounter (paid claims) information.
Other Mental Health Disorders – includes Tic Disorders, Learning Disorders, Communications Disorders, and Motor Skills Disorders.
Substance Abuse/Dependence Disorders – the DSM-IV refers to 11 classes of substances: alcohol, amphetamines, caffeine, cannabis (marijuana or hashish), cocaine, hallucinogens, inhalants, nicotine, opiates (heroin or other narcotics), PCP, and sedatives/hypnotic/anxiolytics.
Mental Retardation – includes Mild, Moderate, Severe and Profound Mental Retardation.
DSM-IV-TRThe Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, published by the American Psychiatric Association. This manual provides a diagnostic coding system for mental and substance abuse disorders (also see ICD-9-CM).
ENROLLMENTThe number of Medicaid recipients who are active in the Medical Assistance program at any given point in time.
FAIR HEARING APPEALA grievance process through which a HealthChoices member can file a written appeal, to the Department of Public Welfare, regarding a behavioral health care service decision.
GRIEVANCEThe process by which a consumer addresses a problem with a decision made about his/her behavioral health care service. This may include denial of a service, approving less service than what was requested, or approving a level of care different from that requested. There are two levels of grievances and an external review process.
1st Level Grievance: An issue which is subject to review within 24 hours for urgent care and 30 days for non-urgent care.
2nd Level Grievance: A 2nd Level Grievance may be filed if the member has not received satisfactory resolution to the 1st Level Grievance. The 2nd Level Grievance Committee reviews the issue within 30 days.
External Review: An External Review can be requested after the 2nd level Grievance decision. This process is independent from the managed care organization or the primary contractor.
Annual Report 2009-2010 15

Blair HealthChoices1906 NORTH JUNIATA STREETHOLLIDAYSBURG, PA 16648
814-696-5680http://www.blairhealthchoices.org