Embed Size (px)
Citation preview

ll(l_‘ Ambry Genetics®
A Konica Minolta Company
Lifetime Risk of Breast Cancer from Polygenic Risk Scores Combined with
Clinical Assessment in Women Referred for Genetic TestingMary Helen Black, Stephanie Gutierrez, Shuwei Li, Jill S. Dolinsky, Jessica Profato, Holly LaDuca
Ambry Genetics, Aliso Viejo, CA
Mary Helen Black [email protected]
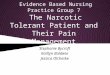
BACKGROUND Figure 1. Mean (95% CI) Lifetime Risk Estimated from Tyrer—Cuzick (TC) Table I- Patient Characteristics (n=523)
Various models based on a woman’s personal and family history are and Combined PRS—TC Models, by Age at Testing .
N %
currently used for clinical breast cancer (BC) risk assessment. Age at testing (years)0
In addition, a wide spectrum of genetic variation, from rare high- 35:8 1:; 33974:;penetrance genes to common polymorphisms with modest effects,
0 0
_
' O
is associated with increased BC risk.TC' mean(95 A) CI) PRS—TC' mean(95 A) CI) 40-49 146 27.9%
. . .
50—59 107 20.5%Several studIes have shown that polygenlc rIsk scores (PRS) may be
_
. . . . . . >—60 55 10.5%useful for BC rIsk stratification, and that combining such a score
, _
. . . . . . . . Family hIstory of any cancerwrth personal and family history Information collected In the cIInIc
, ,
0
further improves BC risk prediction.>I IIISI degree relatIve
428 8I'8 /0
. . . .Ln >1 second degree relatIve only 94 18.0%
As the majorlty of women test negatlve for hIgh-penetrance gene 00None 1 0 2%
mutations, a score based on common polymorphisms and clinical 3’0 . .
'
. . . . . . <1: FamIIy hIstory of breast cancer
hIstory affords an opportunity to provrde them wrth addItIonaI, ,
. . . 3 >1 fIrst degree relatIve 272 52.0%Information that can be used for rIsk assessment.
x .
,9 >1 second degree relatIve only 194 37.1%
‘3; None 57 10.9%
METHODS E Family history of ovarian cancer
The sample was comprised of women referred for multigene panel 59:) >1 first degree relative 55 10.5%
testing inclusive of 17 BC predisposition genes at a single clinicalTI
>1 second degree relative only 74 14.1%
laboratory from April through October 2018. None 394 75.3%
Genetic testing was performed with next-generation sequencing of
all requisite gene regions and 100 SNPs previously shown to be
associated with BC at genome-wide significance in genome-wideassociation studies of Caucasian women4.
A 100-SNP population-standardized PRS was computed for each
woman.
° Using previously published estimates of the per-allele odds ratio
(OR) and risk allele frequency (p) for each SNP, and assuming
independent and additive risks on the log OR scale, we
computed the unscaled population average risk as:
H= (1
- p)2+2p(1 -
p)0R + 29201?2
Adjusted risk values were then calculated as:
1 OR OR2
M’ M’
M
for the 3 genotypes defined by the number of risk alleles: 0,1 or
2, respectively. Missing genotypes were assigned a population
average risk of 1.0. Adjusted risk values for each SNP were
multiplied to compute the overall PRS-associated risk for each
individual based on her observed genotypes.
Personal and family history information was provided by orderingclinicians.
Women who met the following criteria were eligible to receive a
supplemental test report:
'18—84 years of age at the time of testing°
no personal history of cancer
° self-reported Caucasian but without Ashkenazi Jewish ancestry
°no history of atypical hyperplasia or lobular carcinoma in situ
°no known familial mutation in a BC predisposition gene
° tested negative for pathogenic/likely pathogenic variants in any
BC predisposition gene (ATM, BARDY, BL/VI, BRCAY, BRCAZ,
BRIP1, CDHI, CHE/<2, FANCC, MREIIA, NBN, NF7, PALBZ, PTEN,
RAD50, RAD51C, RAD51D, STK11, TP53).
The supplemental report included
° clinically-assessed Tyrer-Cuzick (TC, v8.0)-estimated absolute
risk5
° population-standardized PRS relative risk
° combined PRS-TC lifetime risk to age 85
In view of guidelines for increased BC screening of women with
>20% lifetime risk, and the fact that 50% lifetime risk approachesthat associated with high-penetrance gene mutations, we
categorized clinical and PRS risks according to these thresholds, and
assessed the proportion of patients in each risk category and their
associated characteristics.
30-39
(n=154)
40-49
(n=146)
50-59
(n=107)
Overall
(n=523)
Age at Testing (years)
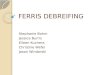
Figure 2. Proportion of Women with Lifetime Risks Estimated from
Combined PRS-TC Scores, by Initial TC Risk Category
20-50%
PRS-TC Combined Risk
TC Risk<20%
(n=211)
PRS-TC Combined Risk
TC Risk>=20%
(n=312)
CONCLUSIONS
On average, lifetime risks of BC estimated by TC model alone and by a combined PRS-TC model are similar.
While a small fraction of women with clinically—assessed lifetime risk <20% may in fact have a high PRS
that substantially increases the overall estimate of lifetime risk, a substantial proportion of women with
clinically-assessed risk 320% may have a modest PRS that decreases the overall lifetime risk estimate.
Our ongoing multi-site clinical utility study is aimed at examining whether and to what extent these groups
of women would benefit from increased or reduced screening, respectively.
15 Argonaut, Aliso Viejo, CA 92656 Toll Free 866 262 7943 Fax 949 900 5501 ambrygen.com
RESULTS
PATIENT CHARACTERISTICS
A total of 523 eligible women received the supplemental test report.
The majority of women were <50 years of age at the time of testing
(69.0%) and had 31 first-degree relative with breast cancer
(52.0%). Approx. 24.6% of women also had 31 first-degree relative
with ovarian cancer (Table 1).
Among eligible women, those who opted in were slightly younger
(meaniSD age 44.1i11.6 vs. 46.4i12.1 years, p<0.001), and more
likely to have 31 first-degree relative with a history of breast or
ovarian cancer (58.9% vs. 43.1%, p<0.001) than women who
provided family history information but did not opt to receive the
report. There was no appreciable difference in the type or size of
multigene panel ordered for women who opted in compared to
those who did not.
LIFETIME BREAST CANCER RISK: TC—ONLY vs PRS—TC
MeaniSD PRS was 0.99i0.71; 95th and 99th percentiles of the PRS
distribution were 2.38 and 3.59, respectively.
MeaniSD TC-estimated lifetime risk was 22.8%i9.9%. A total of
312 women (59.7%) had a TC-estimated lifetime risk >20%.
Mean lifetime risk estimated from the combined PRS-TC model was
23.0% overall, and decreased with increasing age, from 26.6% in
women <30 years to 13.4% in women >60 years (Figure 1).
Average lifetime risks estimated by TC alone vs. combined PRS-TC
model were similar, overall and by age group, with overlappingconfidence intervals (Figure 1).
Among the 211 women with TC-estimated risk <20%, 79.6% had a
TC-PRS combined risk <20%, while 19.0% and 1.4% had combined
risks ranging 20-50% and >50%, respectively (Figure 2).
° Of the women who’s risks increased after accounting for the
PRS, risks estimated by TC alone ranged 10.0-19.9%, and the
majority (75%) had TC-estimated risk >15.0%.
Among the 312 women with TC-estimated risk >20%, 42.0%,
45.5% and 12.5% had combined lifetime risks <20%, 20-50%, and
>50%, respectively (Figure 2).
° Of the women who’s risks decreased after accounting for the
PRS, risks estimated by TC alone ranged 20.0-45.3%, and the
majority (82.4%) had TC-estimated risk <30.0%.
References1) Chatterjee N, Shi J, Garcia-Closas M. Nat Rev Genet. 2016;17(7):392-406.
2) Cuzick J, Brentnall AR, Segal C, et al. J Clin Oncol. 2017;35(7):743-750.
3) Shieh Y, Hu D, Ma L, et al. Breast Cancer Res Treat. 2016;159(3):513-525.
4) Michailidou K. et al. Nature 2017; 551(7678):92-94.
5) Tyrer-Cuzick v8 http://wwwems-triaIs.org/riskeva|uator/