Embed Size (px)
Citation preview
Black Death and White Plague in an English Medieval Cemetery Darlene A. Weston, Dept of Anthropology, University of British Columbia,
Vancouver, Canada
.
In the early 1990’s, the Hereford Cathedral Close cemetery in Hereford, England,
was excavated to make way for a new building housing the treasures of the
Cathedral, including the 13th century Hereford Mappa Mundi, the largest
medieval map known to exist. The excavation yielded over 1100 articulated
burials, including over 300 involving children, dating from the late Anglo Saxon
period to the late medieval period.
Of particular interest in the Hereford burial assemblage were 188 individuals
interred in three mass graves –presumed to be a result of the epidemics of the
Black Death, which swept through Hereford in AD1349 and AD1360-61. In order
to investigate if the mass graves did indeed contain Black Death casualties,
alternative investigative methods needed to be employed, as the Black Death
would have killed its victims relatively quickly, leaving no pathological traces on
the skeleton.
Paleodemographic and statistical tools indicated that the mass graves had a
catastrophic demographic profile when compared to the other medieval period
burials in the cemetery. The catastrophic nature of the mass graves and their
causative agent was confirmed through pathogen DNA analysis, which proved
that the individuals were in fact victims of the bubonic plague, caused by the
pathogen Yersinia pestis. The Hereford Cathedral cemetery is currently one of
only two excavated Black Death cemeteries in the UK (the other being St Mary
Graces, London).
In addition to being a Black Death cemetery, during the medieval period the
Hereford Cathedral Close cemetery was virtually the sole burial place for the
inhabitants of Hereford, although from AD1140 onwards, some children and

paupers were buried elsewhere. Thus it provided a great opportunity to examine
the wide range of ailments afflicting the Hereford citizens. Individuals
demonstrated a wide range of pathological conditions including joint disease,
dental disease, congenital defects, circulatory diseases, trauma, activity-related
pathology, and infections, particularly tuberculosis, also known as the “White
Plague” during the 19th Century.
A relatively large proportion of the population, 4.8% of females and 2.3% of
males with examinable spines, demonstrated signs of spinal tuberculosis (TB).
Some of these individuals also had other joints affected and there was one case
of gastrointestinal TB. Oddly, there were few cases of rib lesions, a pathological
feature that often accompanies spinal lesions. TB is often a disease of poverty,
but as a rather prosperous medieval market town with the cathedral cemetery
post AD1140 being primarily the burial place of higher status individuals,
Hereford’s high TB rate might have been due to consumption patterns (ingestion
of TB infected meat and milk) rather than overcrowding, poor hygiene and poor
diet.
Bibliography Haensch S, Bianucci R, Signoli M, Rajerison M, Schultz M, Kacki S, Vermunt M, Weston
DA, Hurst D, Achtman M, Carniel, E, Bramanti B. 2010. Distinct clones of Yersinia pestis caused the Black Death. PLOS Pathogens 6(10):e1001134.doi:10.1371/journal.ppat.1001134.
Weston DA, Boylston AE, Ogden AR, Hurst D. 2009. Juvenile growth in the medieval
English cemetery population of Hereford Cathedral Close. American Journal of Physical Anthropology S48:421-22.
Weston DA, Boylston AE, Ogden AR, Hurst D. 2007. The palaeodemography of the
Black Death: the Hereford Cathedral Close cemetery. American Journal of Physical Anthropology S44:247-48.
What Can Bone-forming Conditions in Archeological Populations Tell Us About Their Environment and Culture?
Cynthia A Wilczak San Francisco State University
1. Entheses and Enthesophytes
a. Bioarchaeology has used changes in the surface morphology of entheses (Musculoskeletal Stress Markers) to reconstruct activity patterns in past populations.
b. Hawkey and Merbs classification distinguishes between “robusticity markers” and “stress markers”.
c. In most populations, robusticity markers are the most frequent class of change and include all types of mineralized tissue formation.
d. Enthesophytes – marginal ossifications/calcifications that form a bony projection.
e. Used as indicators of activity by subsistence and labor division by gender and class.
i. Agriculture more intense labor stress then hunter-gatherers ii. Gender-based labor divisions
f. Problems in using entheses markers i. Now called entheseal changes to indicate multifactorial
etiology – e.g., age, hormones, disease ii. Marginal ossifications/calcifications, including enthesophytes,
appear to be the most sensitive to signals other than mechanical stress.
iii. Enthesophytes are linked with diseases such as DISH and the seronegative spondyloarthropathies.
iv. Bone-former concept suggests individuals have different propensities to form enthesophytes, osteophytes and mineralizations of non-skeletal tissues.
2. Diffuse idiopathic skeletal hyperostosis (DISH) a. Ossification of anterior longitudinal ligament with ankylosis of
vertebrae, beginning with thoracic i. Flowing “candle wax” appearance; right side in thoracic
vertebrae. ii. Extraspinal enthesophyte formation
b. Uncommon before 40 years with ~2:1 male bias c. Clinically benign in most cases but in severe cases may have
symptoms such as postural abnormalities and pain at the site of enthesophytes.
d. Associated with obesity, diabetes/metabolic dysfunctions, acromegaly e. Archaeology of DISH
i. Lower frequency then modern populations ii. Has been associated with monks and high status, particularly
in males which likely relates to rich diets and the accompanying risk factors of obesity and metabolic disorders.
3. Hyperostosis Frontalis Interna (HFI) a. Endocranial thickening - often nodular b. Bilateral with sparing of the midline c. Usually no clinical disease but severe cases have been associated with
neurological disorders such as headache, dementia and epilepsy d. Strong female bias 9:1 - mainly postmenopausal e. Associated with diabetes, obesity, hirsutism/virulism, acromegaly f. Low androgens – high estrogens and hypogonadism in males
4. Archaeology of HFI a. HFI at Pueblo Bonito, Chaco Canyon, New Mexico, AD 850-1150 – only
cases reported in an indigenous population of the Americas (8.3% males, 44% females)
b. Worldwide there is a much lower prevalence prior to the 18th century c. Most reported are single cases d. Pompeii, Italy and Qatna, Syria also higher frequencies. e. Why HFI in these populations?
i. Genetic predisposition - some evidence ii. Menarche to menopause lengthened & fewer births leading to
increased lifetime estrogen exposure iii. High phytoestrogens in the diet is a possibility but it would
mean a drastically different diet then neighboring populations at Chaco Canyon.
iv. Obesity and diabetes are risk factors and there is some evidence that the skeletal samples from Pueblo Bonito, Qatna and Pompeii represent high-status populations.
5. HFI and DISH a. Some of the same risk factors b. Clinical/medical literature have noted co-occurrence c. Terry Anatomical Collection, Smithsonian, 19th-20th century found a
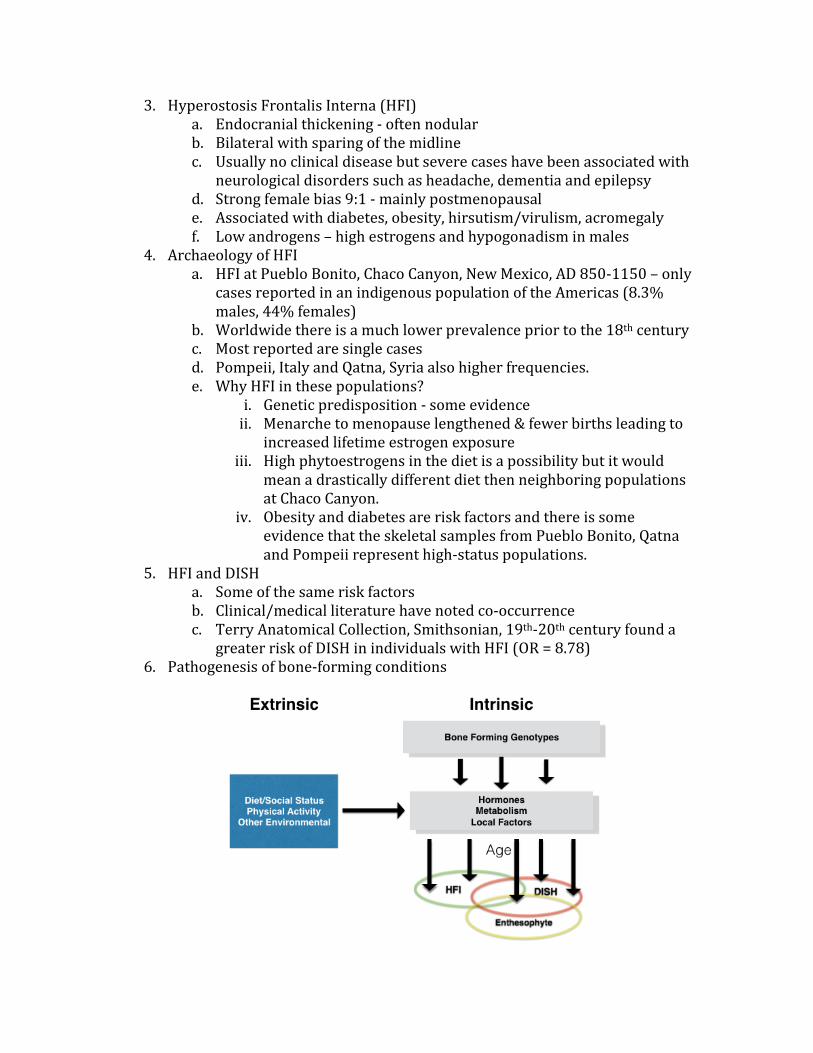
greater risk of DISH in individuals with HFI (OR = 8.78) 6. Pathogenesis of bone-forming conditions
Selected References Flohr S, and Witzel C. 2011. Hyperostosis frontalis interna - a marker of social status?
Evidence from the Bronze-Age “high society” of Qatna, Syria. Homo 62:30–43. Henderson C. 2008. When hard work is disease: the interpretation of enthesopathies. BAR
Int. Series. 1743:17. Henderson CY, Mariotti V, Pany-Kucera D, Villotte S, Wilczak C. 2015. The New “Coimbra
Method”: A Biologically Appropriate Method for Recording Specific Features of Fibrocartilaginous Entheseal Changes. Int J Osteoarchaeol (published on-line ahead of print)
Hershkovitz I, Greenwald C, Rothschild BM, Latimer B, Dutour O, Jellema LM, and Wish-Baratz S. 1999. Hyperostosis frontalis interna: an anthropological perspective. Am. J. Phys. Anthropol. 109:303–325.
Jurmain R, Cardoso FA, Henderson C, Villotte S. 2012. Bioarchaeology's Holy Grail: The Reconstruction of Activity. In: Grauer AL, editor. A Companion to Paleopathology. Grauer/A Companion to Paleopathology. Oxford, UK: Wiley-Blackwell. p 531–552.
Lazer E. 2009. Resurrecting Pompeii. Routledge: New York. Maat GJR. 2007. Diffuse idiopathic skeletal hyperostosis in ancient clergymen. European
Spine J 16:1129–1135. Mader R, Buskila D, Verlaan JJ, Atzeni F, Olivieri I, Pappone N, Di Girolamo C, Sarzi- Mader R,
Verlaan J-J, Buskila D. 2013. Diffuse idiopathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nature Reviews Rheumatology 9:741–750.
May H, Peled N, Dar G, Abbas J, and Hershkovitz I. 2011. Hyperostosis frontalis interna: what does it tell us about our health? Am. J. Hum. Biol. 23:392–397.
Mulhern DM, Wilczak CA, and Dudar JC. 2006. Brief communication: Unusual finding at Pueblo Bonito: Multiple cases of hyperostosis frontalis interna. Am J Phys Anthropol 130:480–484.
Raikos A, Paraskevas GK, Yusuf F, Kordali P, Meditskou S, Al-Haj A, Brand-Saberi B. 2011. Etiopathogenesis of hyperostosis frontalis interna:A mystery still. Ann Anat 193:453–458.
Rogers J, and Waldron T. 2001. DISH and the monastic way of life.Int J Osteoarchaeol 11:357–365.
Rogers J, Shepstone L, Dieppe P. 1997. Bone formers: osteophyte and enthesophyte formation are positively associated. Ann Rheum Dis 56:85–90.
Rühli FJ, Henneberg M. 2002. Are hyperostosis frontalis interna and leptin linked? A hypothetical approach about hormonal influence on human microevolution. Med Hypoth 58:378–381.
Villotte S, Assis S, Alves Cardoso F, Henderson CY, Mariotti V, Milella M, Pany-Kucera D, Speith N, Wilczak CA and Jurmain R. in press. In Search of Consensus: Terminology for Entheseal Changes (EC). Int J Paleopath.
Waldron T. 1985. DISH at Merton Priory: evidence for a “new” occupational disease? Br Med J (Clin Res Ed) 291:1762–1763.
Wilczak C, and Mulhern D. 2010. Co-occurrence of DISH and HFI in the Terry Collection. Int. J. Osteoarchaeol. doi: 10.1002/oa.1218.
Wilczak CA. 1998. Consideration of sexual dimorphism, age, and asymmetry in quantitative measurements of muscle insertion sites. Int J Osteoarch. 5: 311-325.
Wilczak CA. and Kennedy KAR. 1998. Mostly MOS: Technical aspects of identification of skeletal markers of occupational stress. In: K.J. Reichs (ed) Forensic Osteology. 2nd ed. Springfield: Charles C. Thom as. pp. 461 -490.

Two Diseases unique to Papua New Guinea that were identified in the 1950s and 1960s.
Robin A. Cooke
University of Queensland, Brisbane, Australia They were caused by specific eating habits. When these habits were altered, both diseases disappeared without leaving any traces for palaeopathologists to discover in future centuries. Kuru Without any doubt this is the most famous disease which was unique to Papua New Guinea. It occurred in a very restricted language area in the Eastern Highlands - in the Fore Linguistic Group. Missionaries and Government administrative officers working in the area in 1951 reported the common occurrence of a ‘shaking disease.’ A medical officer was sent to examine the problem in 1956. At that time between 1% and 5% of Fore people had Kuru; and it was a major cause of death and a major pre-occupation of the people. Its clinical features were quite constant. It affected particularly teenage and young adult women. It began with ataxia and clumsiness in gait. A useful clinical test devised by the research team to detect early Kuru was to see whether the person could stand on one leg. (It is said that the local males had their own test to see whether a potential bride had Kuru. They observed them crossing one of the fast flowing streams in the district by means of the traditional bridge, i.e. a thin tree trunk laid from one bank to the other. If they were unable to cross they were suffering from ataxia which indicated that they had Kuru). The clumsiness and ataxia progressed and became increasingly disabling. Then irregular and involuntary movements occurred including grimacing which gave the disease its early name of ‘The Laughing Sickness.’ The involuntary movements produced the ‘shaking’ for which the name ‘Kuru’ was used by the people. The ataxia and movements continued until the patient could no longer sit up. She then became unable to move from a reclining position, became incontinent of faeces and urine, and died of starvation and pneumonia. The course of the disease from onset to death was about nine months. It could be distinguished from most other similar disorders by the fact that there was no sensory or upper motor neuron abnormality. Post mortem examinations were performed on about 40 patients, and brains were sent to neuropathologists in Washington, London, Adelaide, and Melbourne with the question "Is this a new disease?" The neuropathologists demonstrated changes in many areas of the brain, but the major changes were present in the cerebellum: spongiform change in the molecular layer with loss of neurons loss of Purkinje cells and degenerative changes in those that remained decrease in the numbers of cells in the granular layer gliosis in the white matter
amyloid containing glial plaques somewhat similar to those seen in Alzheimer's disease Prion stains became available in the 1980s and some kuru brains have been stained with them. They show the presence of PrP linear staining of neuron synapses and plaques of more condensed PrP material. William Hadlow, a veterinary pathologist from the Rocky Mountain Laboratory in Montana observed that the spongiform changes looked like those he was seeing in the transmissible disease, scrapie in sheep. Gajdusek and his team immediately obtained some brain tissue from the next autopsy, froze it and transported it to the National Institutes of Health in the USA. His assistant, Joe Gibbs inoculated some of the brain tissue into the brains of chimpanzees. The chimpanzees developed a disease which was clinically identical to kuru, and examination of their brains showed the same changes as those seen in kuru. This led to the demonstration that kuru was caused by a slow virus infection which occurred as well in other diseases with similar spongiform changes in the brain - Jacob Creutzfeldt Disease, Scrapie (a disease of sheep), Mink Encephalopathy and more recently, Mad Cow Disease. Carlton Gajdusek was the chief researcher on kuru. In 1976 he received a Nobel Prize for his work. The Fore people believed that kuru was the result of sorcery. A person became afflicted because an enemy had put a spell upon her. It was the responsibility of the patient's relatives to identify the sorcerer and kill him. This usually initiated a series of payback killings. ‘Payback’ killings were, and still are, very common in most parts of Papua New Guinea. If one member of a clan is killed by a member of another clan, the dead person's kinsmen are obliged to seek out and kill a member of the offending clan. This may stop at two killings, but the first killing may initiate a whole series of others. In the Fore, each death from kuru would result in the death of at least one other person, and frequently a number. Thus, the people were extremely preoccupied with the subject of kuru and many more people were dying from ‘kuru-associated’ deaths than from kuru itself. Finally, it was anthropological investigations of the habits of the people that provided the clue to the method of transmission. Ritualistic eating of deceased relatives as well as of enemies was widespread, but women, and sometimes children, ate the brains. By ingestion, or other contamination the slow virus was transmitted. Not only does this explain the transmission of the disease, but also its rapid decline in incidence since the late 1960s. After European contact, cannibalism was discouraged, and the effect of this was to reduce the incidence of Kuru. In the past 50 years there has been tremendous social change. The people have collaborated with the researchers and they have taken an active interest in the collection and preservation of the data related to kuru. Michael Alpers is in the final stages of cataloguing and indexing the case histories of the 2700 patients who have died from the disease since the investigations began in 1957.

During the past two years I have been trying to collect sections from as many of the postmortem brains as possible. I have now found 24 of these brains. Not all of them have had prion stains done and I am rectifying this deficiency. I am also taking microscopic photographs so that the pathology can be demonstrated in greater clarity than has been done before. I also found some gross brain tissue to demonstrate the gross appearances (or lack of them.) References Kuru placed in chronological order to demonstrate the stages in the development of knowledge about the disease. First description of the disease Gajdusek DC, Zigas V. Degenerative Disease of the Central Nervous System in New Guinea. The endemic occurrence of ‘kuru’ in the native population. New Engl. J. Med 1957; 257:974-978. (Carlton Gajdusek shared the Nobel Prize in 1976 with Baruch Blumberg (who identifed the Hepatatis B virus) Gajdusek won the Prize for demonstrating that "Kuru was the first chronic degenerative disease of man shown to be a slow virus infection, with incubation periods measured in years and with a progressive accumulative pathology always leading to death.") The pathology resembled that of scrapie in sheep which was transmissible by inoculation from an affected sheep to a normal one. Hadlow WJ. Scrapie and Kuru. Lancet 1959; ii:289-290. Kuru was transmissible to Apes by inoculation of brain from human cases of kuru Gajdusek DC, Gibbs CJ Jr., and Alpers M. Experimental transmission of Kuru-like Syndrome to Chimpanzees. Nature 1966; 209:794. Michael Alpers records this episode in his contribution amongst the total of 15 contributions in the Theme Issue in the following reference: Collinge J and Alpers MP, editors “The End of Kuru: 50 Years of Research into an Extraordinary Disease.” Philosophical Transactions of the Royal Society B Biological Sciences (2008) 363: 3605-3763. "When I first wrote down the word ‘kuru’ in my clinical notes after examining one of the sick chimpanzees, Joe Gibbs and I discussed the implications of this for a few minutes and he went into action: Carleton came back from the wilds of Papua New Guinea (PNG) by the next available flights. He grumbled at first, but not the next day after he had seen that the chimps - Daisey and Georgette; Daisey, in particular, looked uncannily like human kuru.
Later in the year, when the first autopsy was being done, Elisabeth Beck came to see that Joe and I were doing it right. Elisabeth took the brain back with her to London. When, in early February 1966, we received Elisabeth's telegram saying that the pathology of the chimpanzee brain was indistinguishable from human kuru, Carleton, Joe and I were all in Bethesda. We divided the paper into three parts and wrote it in a day. With the help of Marion Poms it was typed and mailed by midnight—and published in Nature within two weeks." Gajdusek DC and Gibbs CJ Jr., Transmission of two subacute spongiform encephalopathies of man (kuru and Creutzfeldt-Jakob disease) to New World monkeys. Nature, Lond 1971; 230: 588-591. Beck E, Daniel PM, Asher DC, Gajdusek DC and Gibbs CJ Jr., Experimental kuru in the chimpanzee a Neuropathological study. Brain 1973; 96: 441-462 Kuru is caused by transmission from brain tissue consumed mainly by women as a mark of respect to the dead person Mathews JD, Glasse RM, Lindenbaum S. Kuru and Cannibalism. Lancet ii:1968; 449-452 Gajdusek DC, Gibbs CJ Jr., Alpers M.P. Experimental transmission of a kuru-like syndrome to chimpanzees. Nature. 1966;209:794–796. Prusiner SB (1982). Novel proteinaceous infectious particles cause scrapie. Science 1982; 216 (4542): 136–144. (Stanley Prusiner (1942-) from the University of Pennsylvania demonstrated that the infectious agent of scrapie contained a protein but no DNA. The diseases that were then called 'slow virus diseases' became known as Prion diseases [prusiner and infectious] He received a Nobel Prize in 1997) Reviews of the Kuru experience Hornabrook RW. Essays on Kuru. Monograph Series No. 3. Papua New Guinea Institute of Medical Research; 1976. Collinge J and Alpers MP, editors “The End of Kuru: 50 Years of Research into an Extraordinary Disease.” Philosophical Transactions of the Royal Society B Biological Sciences (2008) 363: 3605-3763. References to the pathology of Kuru Fowler M & Robertson EG. Observations on kuru. Pathological features in five cases. 1958 Australas. Ann. Med. 8, 16–26. Kakulas BA, Lecours AR & Gajdusek, DC Further observations on the pathology of kuru: a study of the two cerebra in serial section. J. Neuropathol. Exp. Neurol. 1967, 26, 85–97. (doi:10.1097/00005072-196701000-00007)

(These are the two brains that are now in the Paul Yakovlev (1894-1983) collection in the National Museum of History of Medicine, Washington. Byron Kakulas said in the article on the End of Kuru - 50 years of research that this is the definitive report on the pathology of Kuru.) Beck E & Daniel P Kuru and Creutzfeldt–Jakob disease: neuropathological lesions and their significance. In: "Slow transmissible diseases of the nervous system" 1979 (eds Prusiner SB & Hadlow WJ), pp. 253–270. New York, NY: Academic Press. Collinge J, Whitfield J, McKintosh E, Beck J, Mead S, Thomas, DJ & Alpers MP. Kuru in the 21stcentury—an acquired human prion disease with very long incubation periods. Lancet 2006: 367, 2068–2074. (doi:10.1016/S0140-6736(06)68930-7) Masters CL, Kakulas BA, Alpers MP, Gajdusek DC, Gibbs CJ Jr., Preclinical lesions and their progression in the experimental spongiform encephalopathies (kuru and Creutzfeldt–Jakob disease) in primates. J. Neuropathol. Exp. Neurol 1976; 35:593–605 McLean CA, Ironside JW, Alpers MP, Brown, PW, Cervena´kova´ L, Anderson R McD, & Masters C L Comparative neuropathology of kuru with the new variant of Creutzfeldt–Jakob disease: evidence for strain of agent predominating over genotype of host. Brain Pathol. 1998, 8, 429–437. (This was a review of the pathology of 11 Kuru brains held in the University of Melbourne, Australia.) Neumann MA, Gajdusek DC & Zigas V Neuropathological findings in exotic neurologic disorders among natives of the highlands of New Guinea. J. Neuropathol. Exp. Neurol. 1964. 23, 486–507. (doi:10.1097/00005072-196407000-00007) Klatzo I, Gajdusek D C & Zigas V. Pathology of kuru. Lab. Invest. 1959. 8, 799–847. Beck E, Daniel PM, Asher DM, Gajdusek DC, Gibbs CJ Jr. Experimental kuru in the chimpanzee. A neuropathological study. Brain. 1973: 96, 441-62.
Beck E, Daniel PM, Alpers M, Gajdusek DC, Gibbs CJ Jr. Neuropathological comparisons of experimental kuru in chimpanzees with human kuru. Int Arch Allergy Appl Immunol. 1969; 36: Suppl:553-62.
McLean CA, Review:The neuropathology of kuru and variant Creutzfeldt-Jacob disease Phil.Trans.R. Soc. B (2008) 363, 3685-3687 doi:10.1098/rstb.3008.0086

Pigbel (Enteritis Necroticans) (pain in the belly associated with the eating of pig meat) This is another of the diseases that was unique to Papua New Guinea. It was first recognised among the Highland dwelling people by a surgeon Lajos Roth, a Hungarian graduate in the early 1960's, assisted by a newly arrived Australian graduate, Tim Murrell. About half the population of New Guinea lived in the Highlands. They were farmers growing sweet potatoes (called by the local name kau kau) for their staple diet. They kept pigs which were allowed to roam freely. The food gardens were protected from the pigs by fences made by hammering slabs of wood into the ground around the gardens. Pigs were regarded as wealth and status symbols. An important man was one who owned many pigs. They were killed and eaten only on special occasions - the most important of these being called ‘Pig Feasts.’ A feast was arranged by a particular clan whose responsibility it was to breed enough pigs and to grow enough sweet potatoes to feed the hundreds of guests from neighbouring clans who attended the feast. The host clan had to build sufficient houses for the guests, too. There was considerable prestige in running a successful feast and considerable disgrace if it was unsuccessful. (Some Westerners would regard Stone Age people such as these as being backward and inferior. The organisation of a Pig Feast is further evidence against this assumption, when one considers the technical and managerial expertise required to produce a successful feast.) Before the advent of the Australian administration, neighbouring tribes were continually at war with one another. Pig Feasts were peaceful occasions, times for arranging deals, including marriages, and for repaying debts for land or wives. Pigs formed an important part of these exchanges. Pig Feasts still occur and they are regarded as being enjoyable and exciting occasions by the younger, as well as by the older, generation. Pig Feasts are now not such big occasions as they were, and the butchering is done in a much more hygienic way. The pigs to be slaughtered were lined up in the flat space in the centre of the village. The owner had the right to kill his own pigs. The hair was singed over a fire, the pig skinned and disembowelled. All parts of the animal, including the intestines (previously washed in the water of a nearby stream), were cooked in earth ovens, i.e. holes dug in the ground. The meat and sweet potatoes were wrapped in big leaves, water was poured in to provide steam and the oven was closed by filling the hole with soil. Some of the meat was eaten soon after cooking, but some was kept for eating during succeeding days. Because the butchering was unavoidably unhygienic, the meat was contaminated by a variety of organisms including Clostridium perfringens type C spores, which abound in the village environment in which the meat was prepared.
Roth and Murrell found this to be the commonest cause of admission with acute abdomen to the hospitals throughout the Highlands. People of all ages were affected but it was particularly common in children. Cases varied in severity, the majority being mild and self limiting. In severe cases, fever and acute abdominal pain came on some hours after eating the contaminated food. Melaena occurred and was followed by intestinal obstruction. Untreated, the mortality in hospital patients was about 90%. Roth and Murrell were able to reduce the mortality to about 30% by excising the affected segments of bowel and then re-anastomosing the healthy areas. The surgical pathology consisted in segmental involvement of the small intestine with normal small bowel between the involved segments. The affected bowel was thickened and there were blotchy, red areas on the serosal surface. These areas consisted of full thickness necrosis of the bowel wall. Perforations or internal fistulae were frequently encountered. The length of small intestine involved varied from about 30cm to the entire small intestine. Examination of the mucosal surface of the affected small intestine showed small green or black spots which corresponded with focal areas of mucosal necrosis. These spots expanded and coalesced to form segmental areas of full thickness inflammation and necrosis. The junction between normal and affected bowel was marked by a line of neutrophils just as one sees at the margin of any infarcted tissue. A prominent feature of the microscopic pathology was the marked obliterative endothelial proliferation of submucosal veins at the junction between necrotic and normal bowel. Lajos Roth noticed the similarity to the pathology of a disease that occurred shortly after WW2 in a brief outbreak in Hamburg. The German pathologist J.N. Zeissler reported this outbreak in the BMJ 1949, 1:267-269. He called it Darmbrand – Black bowel disease. In 1974 he kindly sent me a section of one of his cases. This condition continued to be the commonest cause of acute abdominal emergencies in the Highlands, and the commonest cause of death in hospital of children over two years of age. Murell investigated the epidemiology of the disease and coined the name Pigbel - i.e. pain in the belly related to eating pig meat. John Egerton, veterinary microbiologist in Papua New Guinea, identified the presence of C.perfringens Type C organisms in the intestines of patients, and also in the village environments in which the cases occurred. Peter Walker from the Wellcome Laboratories in London developed a vaccine, which was given field trials by the physician Greg Lawrence during the 1980's. As a result of this vaccination programme and the changes in the method of conducting Pig Feasts, improved hygiene in butchering, and probably also the overall improvement in nutrition of the population, Pigbel disappeared. After completing his detailed clinical examinations of patients, and performing the highly successful double-blind field vaccination trials, Greg Lawrence moved to the Queensland Institute of Medical Research in Brisbane. He devised a number of experiments in guinea pigs to find the cause of Pigbel. I assisted him with the examination of the pathology produced in his guinea pigs. Together we showed that

experimentally produced Pigbel in guinea pigs had a pathology identical to that of the human disease. As a result of these experiments the following theory of pathogenesis was developed:- This population has a very low protein diet, which leaves them with low levels of protease production. The staple food is sweet potato which itself contains significant quantities of a heat stable protease inhibitor. At the time of a ceremonial feast, at which meat, contaminated with C.perfringens spores is eaten, large amounts of Clostridial exotoxin is produced in the intestine. The subject is not able to inactivate this protease sensitive toxin, because of the low levels of endogenous protease and the presence of protease inhibitors. As a result, the toxin is absorbed, causing the pathology illustrated. In the Highlands of Papua New Guinea most of the cases were associated with the eating of pig meat, but I had a number of cases referred to my laboratory in which other forms of protein were implicated. It was known that occasional cases of what appeared to be Pigbel were reported in the Chiang Mai area of Thailand and occasionally from other places. Lawrence and Cooke postulated that the condition may occur in other parts of the world where conditions similar to those which were found in Papua New Guinea were encountered. In the mid 1980's, Lawrence and Cooke were sent a number of bowel specimens from Cambodian refugees on the Thailand border. Some of these had the typical pathology of Pigbel. As a result of this, the Pigbel vaccine was given to all the people in the refugee camps. In 1991 Greg Lawrence was invited to visit Hanoi and Saigon in Vietnam, because the paediatricians there had been collecting cases which looked like Pigbel for about ten years. He found that Pigbel was indeed present and was affecting, not the rice eating people, but those people living in poorer areas and having sweet potatoes as their staple diet. The disease was similar in its prevalence and in its clinical presentation to what it was in PNG before the introduction of the vaccine. This is a second disease which was found for the first time in Papua New Guinea. In the short space of twenty years, its clinicopathological features were defined, its pathogenesis and prevention were elucidated, and effective control measures were instituted. Thus, a disease which was very common before the arrival of the Australian administration has virtually disappeared. Pigbel Murrell TGC, Roth L. Necrotising Jejunity: A newly discovered disease in the Highlands of New Guinea. MJA 1963; 1:61. Egerton JR, Walker PD. The Isolation of Clostridium perfringens type C from necrotic enteritis of man in Papua New Guinea J.Pathol.Bacteriol. 1964; 88:275/ Murrell TG, Pig Bel - Epidemic and Sporadic Necrotising Enteritis in the Highlands of New Guinea. Aust.Ann.Med.1967; 16:4/

Cooke RA. The Pathology of Pig Bel. Perspectives in Pediatric Pathology. 1979; 5:137. Lawrence G, Cooke R. Experimental Pig Bel: The Production and Pathology of Necrotizing Enteritis due to Clostridium Welchii type C in the Guinea Pig. Br.J.Exp.Path. 1980; 61:261 Lawrence GW, and Walker PD. The Pathogenesis of Enteritis Necroticans in Papua New Guinea. Lancet; 1976; 1:125-127 7. Davis MW, et al. Active Immunization decreases the Incidence of Necrotising Enteritis in Papua New Guinea. 1985 Davis MW. Pig Bel, Necrotising Enteritis in Papua New Guinea. - Proceedings of a workshop held in Goroka, Papua New Guinea, September 2-5, 1980. Monograph Series No. 6. Papua New Guinea Institute of Medical Research; 1984. Lawrence GW, et al. Impact of active immunisation against enteritis necroticans in Papua New Guinea. Lancet 1990; Nov 10; 336(8724): 1165-1167. Lawrence G, et al. Prevention of necrotising enteritis in Papua New Guinea by active immunisation. Lancet 1979 Feb 3; 1(8110):227-230. Johnson S, et al. Enteritis necroticans among Khmer children at an evacuation site in Thailand. Lancet 1987 Aug 29; 2(8557): 496-500. Smith F. Surgical aspects of enteritis necroticans in the highlands of New Guinea. Aust NZ J Surg 1969 Feb; 38(3): 199-205. Easton RJ, et al. Pigless Pigbel: enteritis necroticans in the Solomon Islands. PNG Med J 1984 Mar; 27(1):42-44. Rooney J, et al. Clostridium welchii type C antitoxin in the treatment of ‘Pigbel’ (enteritis necroticans): a controlled trial in Papua New Guinea. PNG Med J 1979 Mar; 22(1): 57-59.