Embed Size (px)
Citation preview

Bisphosphonates in Oncology: Breast Cancer and Beyond
Debu Tripathy
Breast cancer frequently spreads to bone and is asso-
ciated with increased osteoclastic bone resorption.
Bisphosphonates exert a powerful inhibitory effect on
osteoclast activity and have been shown to reduce the
frequency of skeletal complications in patients with
breast cancer and metastatic bone disease. Laboratory
models have shown that bisphosphonates can reduce
the tumor burden in bone. Although improvements in
overall survival (the gold standard outcome measure in
oncology studies) have been seen in patient subpopu-
lations in many phase Ill studies of bisphosphonates in
breast cancer, only three major trials have been pow-
ered to assess overall survival as a primary efficacy
endpoint. The results of these studies have been equiv-
ocal, a phenomenon largely attributable to method-
ologic differences in study design and patient selection.
Well-designed confirmatory clinical studies are now
required to elucidate the true benefits of bisphospho-
nates in breast cancer. This article discusses future
prospects for research with these agents. The benefits
and drawbacks of standard clinical parameters and sur-
rogate marker studies are discussed based on experi-
ence from past investigations.
Semin Oncol 28 (suppl I 1):86-91. Copyright 0 ZOO/ by
MB. Saunders Company.
B REAST CANCER FREQUENTLY spreads to bone and is almost always associated with
osteolysis caused by increased osteoclastic bone resorption. The molecular mechanisms by which tumor cells metastasize to bone are likely to in- volve invasion, cell adhesion to bone, and the release of soluble mediators from tumor cells that stimulate osteoclast-mediated bone resorption. The osteoclast is, therefore, a suitable site for ther- apeutic intervention in the bone metastatic pro- cess.
Bisphosphonates are powerful inhibitors of os- teoclast activity and are used in combination with standard chemotherapy or hormonal therapy for
From the Carol Franc Buck Breast Cancer Center, Department
of Medicine and Cancer Center, University of California at Sun Francisco, CA.
Dr Tripathy has sewed on the speakers’ bureau for F Hoff- mann-la Roche.
Address reprint requests to Debu Tripathy, MD, Associate Clin- ical Professor of Medicine, Carol Franc Buck Breast Cancer Cen-
ter, Department of Medicine and Cancer Center, Box f714, Uni- versity of California at San Francisco, CA 94930.
Copyright 0 2001 by W.B. Saunders Company 0093-7754/01/2804-1116$35.00/O doi:l0.1053/sonc.2001.25443
86
the treatment of cancer-associated osteolytic me- tastases. The precise mechanism by which bisphos- phonates inhibit osteoclast activity is still unclear; it may include inhibition of osteoclast formation as well as increased apoptosis in mature oste- oclasts. Direct antineoplastic effects,i and poorly understood effects on bone pain may occur and animal models have shown that bisphosphonates are capable of suppressing the growth and spread of bone metastases, affecting the adhesion of tumor cells to bone matrix and delaying/decreasing bone complications from both malignant and nonmalig nant bone metastases.213
As a consequence of bisphosphonate-mediated inhibition of osteoclast activity, there is a marked reduction in the skeletal events associated with metastatic cancer to bone, such as pain, fracture, and hypercalcemia.4 However, and possibly even more importantly, there is also a reduction of tumor burden in bone.5 In experimental situations, this has been shown to affect not only morbidity but also survival.6 Nevertheless, studies have re- ported varying results with regard to the effect of bisphosphonates on survival rates in patients with breast cancer and bone metastases. It is thought that the nonconfirmatory nature of these results can largely be attributed to differences in study design, particularly the choice of primary and sec- ondary outcome measures.
This article discusses future prospects for the use of bisphosphonates in breast cancer and beyond. Methodologic problems that may present barriers (or opportunities) to research in this field are dis- cussed based on experience from past studies.
DEFINING ENDPOINTS IN BISPHOSPHONATE STUDIES
At present, bisphosphonates are not used as antitumor agents, but rather as palliative treat- ment for the effects of cancer on the skeleton. Clinical endpoints used in the design of trials of bisphosphonate therapy have to be sensitive to the perspective of patient care. Studies must be able to show that a reduction in the rate of osseous recur- rence translates into an improvement in overall survival, disease-free survival, or an improvement in quality of life through a reduction of adverse skeletal events.7
Seminon in Oncology, Vol 28, No 4, Suppl I I (August), 200 I : pp 86-9 I
BISPHOSPHONATES FOR BREAST CANCER AND BEYOND 87
Study
NO. Bone Metastases (2-S Year Follow-up)
Patients Clodronate Versus Placebo
Disease-Free Overall Survival
state (%) 6)
Powles et allo 1,079
Die1 et al9 302
Saarto et al ’ ’ 299”
28 (5.2%) versus 44 (8. I %)*
8% versus 17%
-
-
87% versus 7 I %
52% versus 69%
NS
96% versus 85%
86% versus 8 I %
"P = ,054.
*Patients received therapy with cyclophosphamide, methotrexate, fluorouracil (CSF) (pretreatment), or antiestrogens.
SURVIVAL: THE GOLD STANDARD
CLINICAL ENDPOINT
Improvements in survival time of certain sub- groups of patients have been found in several phase III studies with bisphosphonates.8 However, these studies were not powered to detect survival time as a primary or secondary outcome measure, thus, these results can only be seen as important indicators for future research.8
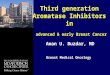
To date, only three major trials have examined the effect of the bisphosphonate clodronate on survival rates as a primary efficacy parameter of adjuvant therapy in patients with early stage breast cancer. The first, an open-label controlled trial by Die1 et aI,9 investigated the effects of clodronate on the incidence and extent of new metastases in patients with breast cancer who were at high risk for developing distant metastases on the basis of the presence of bone marrow micrometastases. In total, 302 patients with primary breast cancer were randomized to 2 years’ oral treatment with clo- dronate (1,600 mg/d) or a control treatment arm of standard follow-up. The study was conducted over a 5year period with a median length of follow-up of 36 months. Patients received standard care (surgical, hormonal, or chemotherapy) during this time. Overall, an increase was seen in disease- free and overall survival in patients taking the bisphosphonate therapy (Table 1).9 Significantly fewer women in the clodronate group developed distant metastases and osseous and visceral metas- tases compared with the control group.g Further- more, the number of bony metastases per patient in the clodronate group was roughly half of that in the control group.
An interim analysis from a larger, multicenter, double-blind, placebo-controlled trial involving 1,079 women with primary operable breast cancer
reported a significant reduction in osseous metas- tases after treatment with clodronate (1,600 mg/d) for 2 years (Table l).lO However, disease-free and overall survival were unchanged compared with the placebo group.
In contrast, a third open-label trial, conducted in Finland in 299 patients with lymph node-posi- tive breast carcinoma, did not find clodronate (1,600 mg/d) to have a significant effect on the relapse of bone metastases (Table 1 ).ll The inves- tigators reported a deleterious effect on relapse rates of nonosseous lmetastases and a deterioration in overall survival after 3 years’ treatment with clodronate.
Taken together, the results of these studies are clearly equivocal with regard to the effect of adju- vant clodronate on overall survival rates in pa- tients with breast cancer. The differing effects seen are likely to be attributable to random or method- ologic factors, such as diversity in inclusion criteria and patient populati.ons, use of alternative assess- ment techniques, and differences in sample size ( met o o o IC 1 h d 1 g’ d’ff erences between these three key studies are discussed in detail by Die1 elsewhere in this supplement). It is clear that the bisphospho- nates have a role in the treatment of breast cancer and further investigation of their effects is war- ranted. Well-designed confirmatory clinical trials are now required to elucidate the true benefits of these agents.
MAINTENANCE OF BONE HEALTH
Lowering the risk of disease progression, either in the adjuvant setting or in the metastatic setting, preserving bone mineral density, and reducing the risk of osteoporosis complications are the key clin- ical endpoints in breast cancer that are important with regard to bone health.

88 DEBU TRIPATHY
Women with breast cancer have an increased risk of developing osteoporosis; those older than 40 years are at particularly high risk.12 A number of factors are involved: (1) the majority of pre- menopausal breast cancer patients are likely to undergo early menopause because of chemother- apy-induced ovarian failure or oophorectomy, known to be a strong predictor of osteoporosisls; (2) chemotherapy may have a direct adverse effect on bone mineral density, and osteoclastic activity may increase from the breast cancer itself; and (3) though estrogen therapy is considered standard for the prevention and treatment of osteoporosis, use of estrogen in women with a history of breast cancer is usually contraindicated because of its associated risk of breast cancer.
Men undergoing androgen deprivation therapy for advanced prostate cancer, a frequently diag- nosed condition in the aging male population, are also at increased risk for developing osteoporosis; androgen deprivation has been associated with the loss of bone mineral density in these patientsr4J5 Steroid therapy is occasionally used in patients with breast and prostate cancer. It can also accel- erate the loss of bone mineral density and there- fore constitutes a risk factor for osteoporosis.
Most women in whom early stage breast cancer is detected and treated appropriately will survive. Furthermore, in breast cancer patients with bone metastases, those responding to systemic therapy for their metastases have a good chance of being alive at 3 years, and 20% will be alive at 5 years.16 The bisphosphonates have been shown to decrease chemotherapy-induced bone loss in women with breast cancer.12 Combined with their potential benefits on bone metastases, there is, therefore, a rationale for using the bisphosphonates early in the treatment of this disease. Current standard procedure for postmenopausal women recom- mends waiting until bone mineral density is below normal before commencing adjuvant therapy.
SURROGATE MARKERS AS ENDPOINTS FOR BISPHOSPHONATE STUDIES
It is possible that surrogate markers, such as circulating micrometastases, bone turnover mark- ers, and bone mineral density may become valu- able adjuncts to clinical endpoints in studies of bisphosphonates. Although clinical endpoints are unquestionably required for the drug approval pro- cess, to show clinical benefit and to provide the
confidence for an agent to be adopted into clinical practice, these studies require larger sample sizes and longer study durations than those assessing surrogate markers (Table 2). Surrogate biological endpoints may also provide insight into the mech- anisms of action underlying the effects of bisphos- phonates in the disease process; knowledge that in itself would permit further refinement of research methodology.
DESIGNING THE OPTIMAL SURROGATE MARKER STUDY
Current knowledge of the effects of bisphospho- nates in the metastatic setting indicates that these agents hold much promise for patients with early stage breast cancer and in the adjuvant setting. Clinical studies are urgently required to check the preliminary, but encouraging, results that have been obtained to date.
Defining the optimal population at risk is im- portant to obtain results quickly. A planned study by the National Surgical Adjuvant Breast and Bowel Project (NSABP), and other studies cur- rently in progress, have attempted to maximize the event rate seen in their studies by selecting smaller sample sizes consisting of patients with specific characteristics that put them at high risk for early metastasis (eg, regional lymph node involvement, local progression or tumor cells present in the bone marrow, or patients with elevated concen- trations of specific prognostic factors for bone me- tastasis).
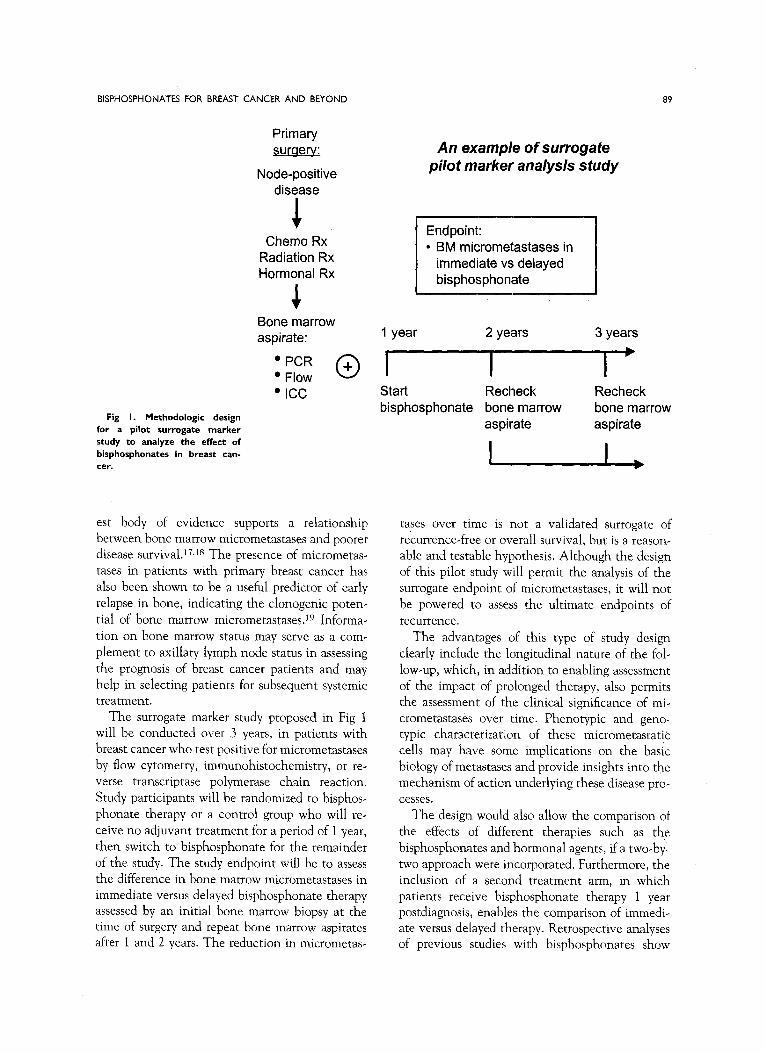
Figure 1 is a schematic for a pilot study designed to assess the feasibility of measuring eradication/ modulation of micrometastases as a surrogate marker for the assessment of bisphosphonate ther- apy. Several lines of evidence suggest that micro- metastases predict metastatic potential. The larg
Smaller sample size More definitive (and approvable)
Shorter study
Biological endpoints may
explain mechanisms of
action
Larger sample size
Linkage of markers to clinical
endpoints
BISPHOSPHONATES FOR BREAST CANCER AND BEYOND 89
Primary surgery:
Node-positive disease
1 Chemo Rx
Radiation Rx Hormonal Rx
Bone marrow aspirate:
‘PCR + . Flow 0 . ICC
Fig I. Methodologic design for a pilot surrogate marker
study to analyze the effect of bisphosphonates in breast can-
cer.
est body of evidence supports a relationship between bone marrow micrometastases and poorer disease survival.i7Js The presence of micrometas- tases in patients with primary breast cancer has also been shown to be a useful predictor of early relapse in bone, indicating the clonogenic poten-
tial of bone marrow micrometastases.19 Informa- tion on bone marrow status may serve as a com-
plement to axillary lymph node status in assessing the prognosis of breast cancer patients and may help in selecting patients for subsequent systemic treatment.
The surrogate marker study proposed in Fig 1 will be conducted over 3 years, in patients with breast cancer who test positive for micrometastases by flow cytometry, immunohistochemistry, or re- verse transcriptase polymerase chain reaction.
Study participants will be randomized to bisphos- phonate therapy or a control group who will re- ceive no adjuvant treatment for a period of 1 year,
then switch to bisphosphonate for the remainder of the study. The study endpoint will be to assess the difference in bone marrow micrometastases in immediate versus delayed bisphosphonate therapy assessed by an initial bone marrow biopsy at the time of surgery and repeat bone marrow aspirates after 1 and 2 years. The reduction in micrometas
An example of surrogate pilot marker analysis study
Endpoint: l BM micrometastases in
immediate vs delayed bisphosphonate
1 year 2 years 3 years
I I I b Start Recheck bisphosphonate bone marrow
aspirate
Recheck bone marrow aspirate
tases over time is not a validated surrogate of
recurrence-free or overall survival, but is a reason- able and testable hypothesis. Although the design of this pilot study will permit the analysis of the surrogate endpoint of micrometastases, it will not be powered to assess the ultimate endpoints of
recurrence. The advantages of this type of study design
clearly include the longitudinal nature of the fole
low-up, which, in addition to enabling assessment of the impact of prolonged therapy, also permits the assessment of the clinical significance of mi- crometastases over time. Phenotypic and gene, typic characterization of these micrometastatic cells may have some implications on the basic biology of metastases and provide insights into the mechanism of action underlying these disease pro-
cesses. The design would also allow the comparison; of
the effects of different therapies such as the
bisphosphonates and hormonal agents, if a two-by: two approach were incorporated. Furthermore, the inclusion of a second treatment arm, in which patients receive bisphosphonate therapy 1 year postdiagnosis, enables the comparison of immedi- ate versus delayed therapy. Retrospective analyses of previous studies with bisphosphonates show

90 DEBU TRIPATHY
that therapy was often started long after the diag nosis of osseous lesions; in one study with ibandr- onate the difference was approximately 200 days.20 This delay may be a contributing factor to some of the differences observed in overall survival out- come.
ENDPOINTS OF TRUE CLINICAL USE
In the future, pharmacoeconomic consider- ations are likely to become increasingly important in making decisions from a clinical practice stand- point, particularly given the number and associ- ated cost of bone health-related disorders. A re- cent cost-utility study conducted in Canada looked specifically at the bisphosphonate, pami- dronate.21 The investigators concluded that the drug provided patients with a substantial quality+ adjusted survival benefit at a reasonable cost to the Canadian health care system. Further research is warranted to better determine the cost-benefit consequences of bisphosphonates.
CONCLUSIONS
The gold standard endpoint for oncology studies is clearly overall survival. However, the bisphos- phonates have not yet been shown to have a conclusive impact on this critical outcome mea- sure. These agents gained approval based on their quality of life merit in terms of beneficial reduc- tions in skeletal complications in cancer patients (ie, the ability to reduce the incidence of patho- logic fractures, surgery for fracture or impending fracture, radiation, spinal cord compression, and hypercalcemia). To detect an effect of bisphospho, nates on disease-free or overall survival it is likely that clinical studies will need to select specific groups of patients at high risk for disease progres- sion, particularly skeletal. The study by Die1 et al9 suggests that patients with histologically detect- able bone marrow involvement, but without radio- logic evidence of bone metastasis, may be an ap- propriate group for such studies. The newer bisphosphonates, with more patient-friendly oral and intravenous administration regimens, offer the potential for long-term adjuvant use with good patient compliance.
Quality of life outcomes are undoubtedly crucial endpoints from the patient’s perspective and bisphosphonates have been shown to provide a meaningful supportive benefit to many patients with bone metastases arising from breast cancer.
However, further research into the use of markers of bone turnover and micrometastases as surrogate endpoints will help to provide insight into the clinical predictors of bisphosphonates and provide guidance on when to start and stop therapy and appropriate dosing regimes. Good data from ran- domized trials currently being designed or already in progress are awaited with interest.
REFERENCES
1. Fromigue 0, Lagneaux L, Body JJ: Bisphosphonates in- duce breast cancer cell death in vitro. J Bone Miner Res
15:2211-2221, 2000
2. Boissier S, Ferreras M, Peyruchaud 0, et al: Bisphospho- nates inhibit breast and prostate carcinoma cell invasion, an
early event in the formation of bone metastases. Cancer Res
60:2949-2954, 2000 3. Boissier S, Magnetto S, Frappart L, et al: Bisphosphonates
inhibit prostate and breast carcinoma cell adhesion to unmin- eralized and mineralized bone extracellular matrices. Cancer
Res 57:3890-3894, 1997 4. Body JJ, Bard R, Burckhardt P, et al: Current use of
bisphosphonates in oncology. J Clin Oncol 16:3890-3899, 1998
5. Mundy GR: Bisphosphonates as anticancer drugs. N Engl
J Med 339:398400, 1998 6. Mundy GR: Mechanisms of bone metastasis. Cancer 80:
1546.1556, 1997 (suppl 8) 7. Paterson AH: The potential role of bisphosphonates as
adjuvant therapy in the prevention of bone metastases. Cancer 88:3038-3046, 2000
8. Die1 IJ, Solomayer EF, Bastert G: Bisphosphonates and
the prevention of metastasis. First evidences from preclinical and clinical studies. Cancer 88:3080-3088, 2000 (suppl 12)
9. Die1 IJ, Solomayer EF, Costa SD, et al: Reduction in new metastases in breast cancer with adjuvant clodronate treat-
ment. N Engl J Med 339:357,363, 1998 10. Powles TJ, Paterson AHG, Nevantaus A, et al: Adju.
vant clodronate reduces the incidence of bone metastases in
patients with primary operable breast cancer. Proc Am Sot Clin Oncol 17:468A, 1998 (abstr)
11. Saarto T, Blomqvist C, Virkkunen, et al: No reduction of bone metastases with adjuvant clodronate treatment in
node-positive breast cancer patients. Proc Am Sot Clin Oncol
18:128A, 1999 (abstr) 12. Saarto T, Blomqvist C, Valimaki M, et al: Chemical
castration induced by adjuvant cyclophosphamide, methotrex- ate, and fluorouracil chemotherapy causes rapid bone loss that
is reduced by clodronate: A randomized study in premenopausal breast cancer patients. J Clin.Oncol 15:1341-1347, 1997
13. Mincey BA, Moraghan TJ, Perez EA: Prevention and treatment of osteoporosis in women with breast cancer. Mayo Clin Proc 75:821-829, 2000
14. Daniel1 HW, Dunn SR, Ferguson DW, et al: Progressive
osteoporosis during androgen deprivation therapy for prostate cancer. J Urol 163:181-186, 2000
15. Wei JT, Gross M, Jaffe CA, et al: Androgen deprivation
therapy for prostate cancer results in significant loss of bone density. Urology 54:607-611, 1999

BISPHOSPHONATES FOR BREAST CANCER AND BEYOND 91
16. British Association of Surgical Oncology Guidelines: The management of metastatic bone disease in the United
Kingdom. The Breast Specialty Group of the British Associa- tion of Surgical Oncology. Bur J Sung Oncol 25:3,23, 1999
17. Simmons R, Hoda S, Osborne M: Bone marrow micro- metastases in breast cancer patients. Am J Surg 180:309-312, 2000
18. Yeatman TJ, Cox CE: The significance of breast cancer lymph node micrometastases. Surg Oncol Clin N Am 8:481-
496, 1999 19. Mansi JL, Berger U, Easton D, et al: Micrometastases in
bone marrow in patients with primary breast cancer: Evaluation
as an early predictor of bone metastases. Br Med J 295:1093- 1096, 1987
20. Die1 IJ, Lichinister MR, Body JJ, et al: Improvement of bone pain, quality of life and survival time of breast cancer patients with metastatic bone disease treated with intravenous
ibandronate. Eur J Cancer 35:A269, 1999 (suppl 4) (abstr) 21. Dranitsaris G, Hsu T: Cost utility analysis of prophylac-
tic pamidronate for the prevention of skeletal related events in patients with advanced breast cancer. Support Care Cancer
7:271-279, 1999