Embed Size (px)
Citation preview

R
1
2
3
4
5
6
7
BEMTNa
DRM
BahtWtit1p
TirOt
sb
rtswddrbgmes
Atttwrpt
bmwt
d(dwVras
A
APK
Fm
654 CASE REPORT TALAL AHMED REDA MAHMOUD ET AL Ann Thorac SurgBISMUTH PASTE FOR EMPYEMA THORACIS 2010;90:654–5
©P
FEAT
UR
EA
RT
ICLES
eferences
. Puskas JD, Mathisen DJ, Grillo HC, et al. Treatment strategiesfor bronchopleural fistula. J Thorac Cardiovasc Surg 1995;109:989–95.
. Tsai FC, Chen HC, Chen SH, et al. Free deepithelializedanterolateral thigh myocutaneous flaps for chronic intractableempyema with bronchopleural fistula. Ann Thorac Surg 2002;74:1038–42.
. Chen HC, Tang YB, Noordhoff MS, Chang CH. Microvascularfree muscle flaps for chronic empyema with bronchopleuralfistula when the major local muscles have been divided—onestage operation with primary wound closure. Ann Plast Surg1990;24:510–6.
. Huang WC, Chen HC, Wei FC, Cheng MH, Schnur DP.Chimeric flap in clinical use. Clin Plast Surg 2003;30:457–67.
. Kuo YR, Jeng SF, Kuo FM, Liu YT, Lai PW. The versatility offree anterolateral thigh flap for reconstruction of soft tissuedefects: a review of 140 cases. Ann Plast Surg 2002;48:161–6.
. Pairolero PC, Trastek VF. Surgical management of chronicempyema: the role of thoracoplasty. Ann Thorac Surg 1990;50:689–90.
. Koshima I, Yamamoto H, Hosoda M. Free combined compositeflaps using the lateral circumflex femoral system for repair ofmassive defects of the head and neck regions: an introduction tothe chimeric flap principle. Plast Reconstr Surg 1993;92:411–20.
ismuth Paste Injection formpyema Thoracis: A 100-Year-Oldethod Revisited
alal Ahmed Reda Mahmoud, PhD,or Izham Ismail, MD, Ahmad Sobri Muda, MMed,
nd Mohd Ramzisham Abdul Rahman, MS
ivision of Cardiothoracic Surgery and Department ofadiology, Heart and Lung Centre, Universiti Kebangsaanalaysia Medical Centre, Kuala Lumpur, Malaysia
ismuth paste injection into the pleural cavity used to betreatment for chronic empyema thoracis. This method,owever, was long forgotten and scarcely practiced due
o advanced surgical techniques and antibiotic therapy.e report a 50-year-old man with chronic empyema
horacis who was successfully treated with bismuth pastenjection after a failed surgical decortication and a long-erm chest drainage. This case highlights a trial of a00-year-old method of bismuth paste injection whichroved effective after standard measures had failed.
(Ann Thorac Surg 2010;90:654–5)© 2010 by The Society of Thoracic Surgeons
he management of chronic empyema thoracis hasalways been challenging. The treatment options
nclude chest tube drainage, surgical decortication, tho-acoplasty, and an open window thoracostomy [1, 2].wing to its multifactorial etiology and the complexity of
he disease, even in the present time there is still no
ccepted for publication Feb 15, 2010.
ddress correspondence to Dr Talal Ahmed Reda Mahmoud, 26-19-4
rima Midah Height condo, Jalan Midah 8A, Taman Midah, Cheras, 56000uala Lumpur, Malaysia; e-mail: [email protected]. s2010 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ingle ideal treatment or a gold standard practice that cane successfully applied to treat this condition.Even though the incidence of empyema thoracis has
educed remarkably with the advancement of antibioticherapy, the morbidity and mortality as a result of this istill high [1, 2]. On the other hand, performing an openindow thoracostomy results in a long hospital stay, andisfigurement of the chest wall after thoracoplasty is veryemoralizing to the patients. Historically, empyema tho-acis and suppurative sinuses were mainly treated withismuth paste injection into the affected cavity, withreat success [3]. We report a successful case of a bis-uth paste injection in a long-standing chronic empy-
ma thoracis that failed conservative treatment andurgery.
50-year-old man was referred for a right-sided chronicuberculous empyema thoracis. He initially underwent ahoracotomy and decortication, after which he wasreated with a long-term chest tube for more than 5 years,ithout success. A redo thoracotomy, decortication, pleu-
ectomy, and resection of the osteomyelitic fifth rib wereerformed. The lung failed to expand, however, and
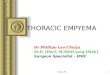
here was a persistent cavity with pus collection (Fig 1).Four weeks postoperatively, he underwent a trial of a
ismuth paste injection, a method that was first practicedore than 100 years ago. His condition improved, and heas discharged well a week later. He remained asymp-
omatic at the 2-year follow-up.This procedure should only be initiated when the
ischarge from the nonhealing pleural cavity is minimal�50 mL/d). The bismuth paste (bismuth subnitrate io-oform paste, Zulat Pharmacy, Kuala Lumpur, Malaysia)as prepared by a mixture of bismuth subnitrate andaseline (white soft paraffin, Pharmaniaga, Selangor Da-
ul Ehsan, Malaysia) in 1:9 ratio, with the latter acting assolvent resulting in a semisolid preparation, and sub-
equently heated to allow liquefaction. The amount re-
ig 1. A computed tomography image of the thorax before the bis-uth injection shows the nonhealing cavity in the right pleural
pace.
0003-4975/$36.00doi:10.1016/j.athoracsur.2010.02.031

qth
ipprirwstpctrfi
C
Iabitbstmntys
ptrqde
wiwpwagntsotl
eehecap
R
1
2
3
SMLJ
DHC
Mawbaucrms
A
A
Fmm
655Ann Thorac Surg CASE REPORT LEI2010;90:655–7 BRONCHIAL MUCOEPIDERMOID CARCINOMA IN A LONGSTANDING COLLAPSED LUNG
©P
FEA
TU
RE
AR
TIC
LES
uired was estimated from the size of the cavity seen onhe computed tomography scan of the affectedemithorax.Under fluoroscopic guidance, a syringe was used to
mmediately administer 250 mL of bismuth paste to theleural cavity through the existing chest tube to avoidremature solidification of the preparation. A strongesistance was felt once the cavity was filled, and thenjection was discontinued. The chest tube was thenemoved immediately after the procedure, and theound was closed using a 2-0 polypropylene suture. A
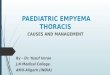
mall amount of the bismuth paste, however, leakedhrough the wound during the next 2 days, and a com-uted tomography scan of the thorax revealed that theavity was 90% filled. A repeat injection was performedo refill the residual cavity, and the wound suture waseinforced. A repeat scan confirmed adequacy of thelling (Fig 2).
omment
t is a common practice to insert a chest tube for drainages the initial treatment for empyema thoracis, followedy an antibiotic therapy and aggressive respiratory phys-
otherapy with postural drainage. In some cases, decor-ication with pleurectomy or, rarely, thoracoplasty maye required as a more definitive treatment. A repeaturgical procedure is not uncommon. Reaccumulation ofhe pus into an unhealed pleural cavity will recur in
any cases once the chest tube is removed. Unfortu-ately, some of these patients require a long-term chest
ube. As seen in our patient, he had been living for 5ears with a portable chest tube after several failedurgical treatments.
The injection of bismuth paste into the nonobliteratedleural space came into practice with the idea of substi-
uting the air in the space with an inert material, and itsadiopaque characteristic helps in confirming the ade-uacy of the filling. Beck [3] initially used bismuth in theiagnosis and treatment of suppurative sinus and empy-
ig 2. A computed tomography image of the thorax after the bis-uth injection shows that the cavity has been filled with the bis-uth paste.
ma in 1906. He later presented a series of 110 patients, ofhR
2010 by The Society of Thoracic Surgeonsublished by Elsevier Inc
hom approximately 80% were cured by bismuth pastenjection alone. As seen in our patient, his first injectionas also incomplete, and several cases warranted re-eated injections during an interval of several months,ith relapse occurring occasionally after 1 or 2 years. He
lso observed that cavities that required more than 200rams of bismuth were less likely to heal by this tech-ique. In our case, the patient was well after this
herapy, without any immediate or early complicationsuch as respiratory distress, pneumonia, severe pain,r allergic reaction, as previously stated in the litera-ure, and he remained asymptomatic at the last fol-ow-up at 2 years.
In conclusion, bismuth paste injection can be consid-red as an alternative method of treatment for chronicmpyema thoracis, especially when other treatmentsave failed or patients are unfit for surgery. It is safe,asy, and noninvasive. The underlying cause of thehronic empyema thoracis, however, must be treatedggressively to gain maximum benefit from bismuthaste injection.
eferences
. LeMense GP. Empyema thoracis, therapeutic managementand outcome. Chest 1995;107:1532–7.
. Molnar TF. Current surgical treatment of thoracic empyemain adults. Eur J Cardiothorac Surg 2007;32:422–30.
. Beck EG. The present status of bismuth paste treatment ofsuppurative sinuses and empyema. Ann Surg 1914;59:145–57.
uccessful Treatment of Bronchialucoepidermoid Carcinoma in a
ongstanding Collapsed Lungiang Lei, MD
epartment of Thoracic Surgery, Shanghai Pulmonaryospital, Tongji University School of Medicine, Shanghai,hina
ucoepidermoid carcinoma is a rare tumor of the lung thatccounts for 0.1% to 0.2% of all pulmonary tumors. Hereine report our experience with a patient who suffered fromronchial mucoepidermoid carcinoma and 2-year left lungtelectasis. The tumor originated from the orifice of the leftpper bronchus and obstructed the left main stem bron-hus. A left upper sleeve lobectomy was performed and theemaining atelectatic lower lobe was fully expanded by 6
onths postoperatively. The patient’s pulmonary functionignificantly improved.
(Ann Thorac Surg 2010;90:655–7)© 2010 by The Society of Thoracic Surgeons
ccepted for publication Dec 17, 2009.
ddress correspondence to Dr Lei, Department of Thoracic Surgery, Shang-
ai Pulmonary Hospital, Shanghai Tongji University, No. 507 Zhengmingd, Shanghai, 200433 China; e-mail: [email protected].0003-4975/$36.00doi:10.1016/j.athoracsur.2009.12.079