Embed Size (px)
Citation preview

Bismarck, Beveridge and “The Blues”
The Paul H. Nitze School of Advanced International StudiesBologna, Italy
October 14, 2010
Lloyd B. Minor, M.D.Provost and Senior Vice President for Academic Affairs
University Distinguished Service Professor of Otolaryngology—Head & Neck Surgery
The Johns Hopkins University

Bi-Polar Public Opinion?
• Since the 1990s, large majorities of Americans have stated that the health care system is broken and needs major reform
• On average, 70% of Americans are pleased with the health care they receive and with their health care plan
7681
88 8489 89
99 9788
97
109 106
116 115 113
130134
128
115
65 71 71 74 74 77 80 82 82 84 84 90 93 96 101 103 103 104 110
0
50
100
150
1997/98 2002/03
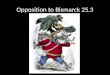
Mortality Amenable to Health CareA measure of health system performance
Preventable deaths per 100,000 population*
*Countries’ age-standardized death rates before age 75; including ischemic heart disease, diabetes, stroke and bacterial infectionsData: E. Nolte and C. M. McKee, London School of Hygiene and Tropical Medicine analysis of WHO mortality files (2008)Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2008

Infant Mortality RatesInfant deaths per 1,000 live births
International Comparison, 2004
Data: OECD Health Data 2007, Version 10/2007Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2008
2.8 2.83.1 3.2 3.3
4.4
5.3
6.8
Japan Iceland Sweden Norway Finland Denmark Canada U.S.
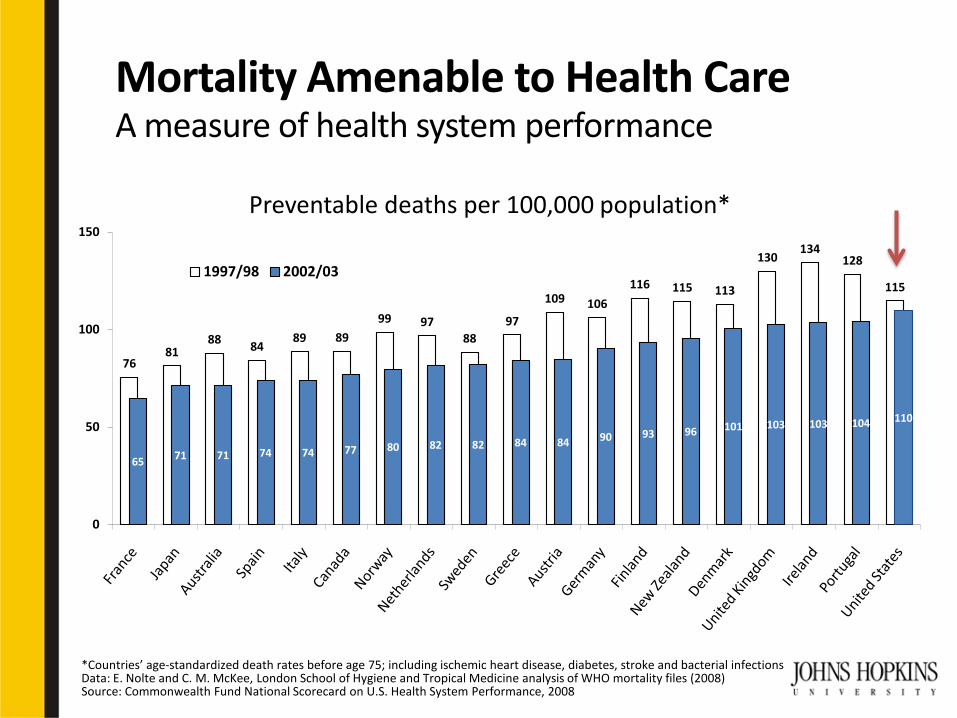
Notes: *Estimate; expenditures shown in $US PPP (purchasing power parity)Source: Calculated by The Commonwealth Fund based on 2007 International Health Policy Survey; 2008 International Health Policy Survey of Sicker Adults; 2009 International Health Policy Survey of Primary Care Physicians; Commonwealth Fund Commission on a High Performance Health System National Scorecard; and OECD Health Data, 2009 (Nov. 2009)
AUS CAN GER NETH NZ UK US
OVERALL RANKING (2010) 3 6 4 1 5 2 7
Quality Care 4 7 5 2 1 3 6
Effective Care 2 7 6 3 5 1 4
Safe Care 6 5 3 1 4 2 7
Coordinated Care 4 5 7 2 1 3 6
Patient-Centered Care 2 5 3 6 1 7 4
Access 6.5 5 3 1 4 2 6.5
Cost-Related Problem 6 3.5 3.5 2 5 1 7
Timeliness of Care 6 7 2 1 3 4 5
Efficiency 2 6 5 3 4 1 7
Equity 4 5 3 1 6 2 7
Long, Healthy, Productive Lives 1 2 3 4 5 6 7
Health Expenditures/Capita, 2007 $3,357 $3,895 $3,588 $3,837* $2,454 $2,992 $7,290
Health Care Rankings by Country
Best
Middle
Worst

Note: $US PPP = purchasing power paritySource: OECD Health Data, 2009 (Nov. 2009)
0
2
4
6
8
10
12
14
16
1980 1984 1988 1992 1996 2000 2004
United StatesGermanyCanadaNetherlandsNew ZealandAustraliaUnited Kingdom
$7,290
$2,454
16%
8%
International Comparison of Health Spending 1980–2007
Average Health Expendituresper capita ($US PPP)
Total Health Expendituresas % of GDP
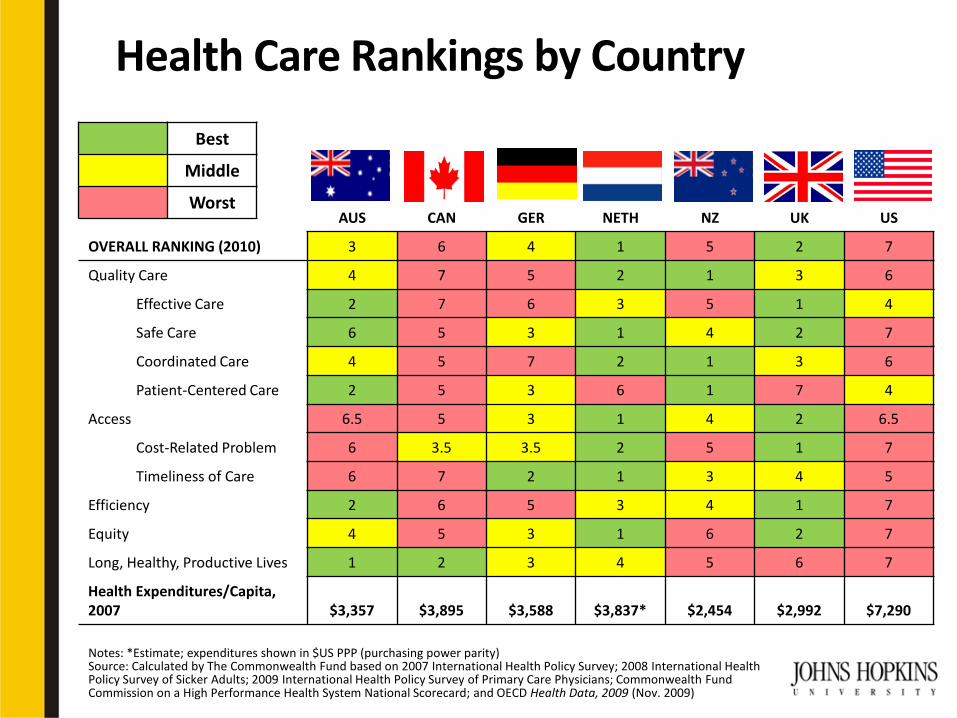
Source: Congressional Budget Office, testimony of Peter R. Orszag, Growth in Health Care Costs before the Committee on the Budget, United States Senate, January 31, 2008
Projected Spending on Health Care Under Assumption that Cost Growth Continues at Historical Averages
Percent of GDP
Affordable Care Act
• Largest expansion of private sector health insurance in U.S. history– Federal subsidies for those without employer
coverage
• Tax credits for small businesses• Private insurance market reform
– Eliminate “rescission” and most other forms of underwriting
– Required medical loss ratios• 85% for plans in large group market• 80% for plans in individual and small group markets
– Compete on quality, service, outcomes, price

Affordable Care Act
• Insurance exchanges – More efficiently pool risk– Lower administrative costs– Provide a choice of health plans to eligible
individuals and small businesses
• Significantly expanded Medicaid eligibility to capture 16 million uninsured
• Large role for the states via both Medicaid and new insurance exchanges
Affordable Care Act
• Goal: To cover all citizens
• Reality: Reduction of number of uninsured from over 50 million in 2007 to estimated 23 million in 2019– Uninsured will be mostly “illegal aliens” and those
who fail or refuse to enroll in insurance plan
• Insurance mandate

Health System Models
• Bismarck (decentralized)– Established end of 19th century by Bismarck in
newly-unified Germany– Patients pay insurance premiums to a sick fund– Local/regional social insurance model
• Beveridge (centralized)– Established in 1948 by Lord Beveridge in the UK
as the National Health Service (NHS)– State owns and runs hospitals– Funded through general taxation
• Market-Based
Nations with Bismarck ModelSocial Insurance
• Austria • Germany• The Netherlands • Belgium • France• Switzerland • Luxembourg• Japan
Current Moved from Bismark to Beveridge in 1970-80s• Greece• Italy• Portugal • Spain • South Korea

Nations with Beveridge ModelNational Health System (NHS)
• UK • Ireland • Denmark• Norway• Sweden• Finland• Iceland• Australia • New Zealand
Long-Standing Moved from Bismark to Beveridge in 1970-80s• Greece• Italy• Portugal • Spain • South Korea

Public Policy ConundrumOutcomes vs. Popularity
• Outcomes– Bismarck has higher rates of per capita growth
in health expenditures– Beveridge has a cost advantage– Beveridge has a possible advantage in health
outcomes related to diseases requiring systematic, organized population-based screening (e.g., breast cancer, TB)
• Popularity– Satisfaction in decentralized Bismarck systems
generally higher than in centralized Beveridgesystems

Marked-Based Models
• American Blue Cross and Blue Shield model– Established in 1934– Private insurance and provider markets– Access depends on ability to pay– Provisions for the poorest and most vulnerable
• Other nations with market-based models– South Africa– Uruguay– The Bahamas– Chile– Argentina

True “Blues”
• The rest of the developed world has Bismarck and Beveridge
• America has “The Blues”
• U.S. health care reform represents the first-ever attempt at “universal” health care on the foundation of a market-based model
Borrowing Among the Models
• Course of reform is never straight
• “The Blues”– Borrow from Beveridge in the VA Health System– Borrow from Bismarck in Medicaid and
federally-sponsored community health centers
• Beveridge models have long experimented with “managed competition”
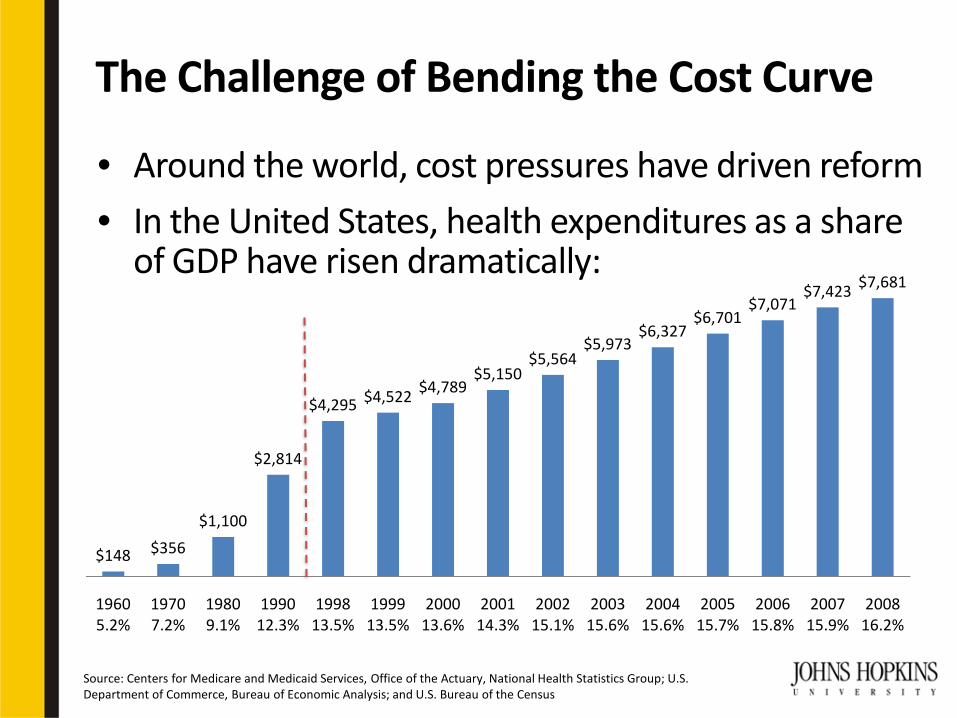
The Challenge of Bending the Cost Curve
• Around the world, cost pressures have driven reform
• In the United States, health expenditures as a share of GDP have risen dramatically:
$148 $356
$1,100
$2,814
$4,295 $4,522 $4,789$5,150
$5,564$5,973
$6,327$6,701
$7,071$7,423 $7,681
1960 5.2%
1970 7.2%
1980 9.1%
1990 12.3%
1998 13.5%
1999 13.5%
2000 13.6%
2001 14.3%
2002 15.1%
2003 15.6%
2004 15.6%
2005 15.7%
2006 15.8%
2007 15.9%
2008 16.2%
Source: Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group; U.S. Department of Commerce, Bureau of Economic Analysis; and U.S. Bureau of the Census

National Health Expenditures, 2008$2.3 Trillion
Source: Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group
Investment7%
Hospital Care30%
Physician/Clincial Services21%Other Professional Services
6%
Dental4%
Nursing Home Care6%
Home Health3%
Rx Drugs10%
Other Retail Products3% Program
Admin7%
Govt Public Health Activities3%

Health Policy Brief: Accountable Care Organizations. Health Affairs, July 27, 2010, http://www.healthaffairs.org/healthpolicybriefs/
Accountable Care Organizations
Mode of Payment Savings Incentives
Risk
Tier 1 Fee-for-service Low Low
Tier 2 Fee-for-service, partial capitation, some bundled payments
Medium Medium
Tier 3 Full or partial capitation, extensive bundled payments
High High

Models of Accountable Care Organizations
Integrated Delivery System
Organization of physician practices, hospitals,and health plan, like Kaiser Permanente
Multispecialty Group Practice
Affiliation of physicians from multiple specialties, like Mayo Clinic
Physician-Hospital Organization
Joint venture between one or more hospitals and a group of physicians
Independent Practice Association
Organization of individual physician practices that contract with health plans
Virtual Physician Organization
Organization of small, independent physician practices, many located in rural areas
Health Policy Brief: Accountable Care Organizations. Health Affairs, July 27, 2010, http://www.healthaffairs.org/healthpolicybriefs/

*Expenditures for Portugal are from 2004 due to missing data for 2005Source: OECD Health Data 2009 (Accessed June 2009); OECD Social Expenditure Dataset (Accessed Dec. 2009); Health and Social Service Spending; Associations with Health Outcomes by Elizabeth Bradley, Benjamin Elkins, Brian Elbel
Health and Social Service Expenditures OECD Countries, 2005
Expenditures as % of GDP
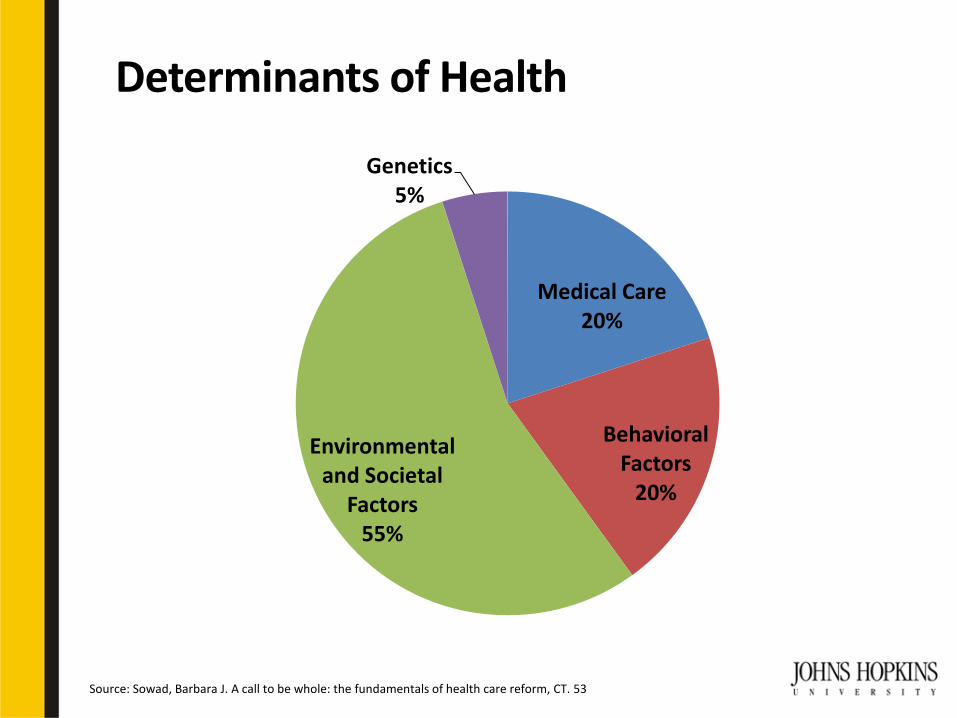
Determinants of Health
Source: Sowad, Barbara J. A call to be whole: the fundamentals of health care reform, CT. 53
Medical Care20%
Behavioral Factors
20%
Environmental and Societal
Factors55%
Genetics5%
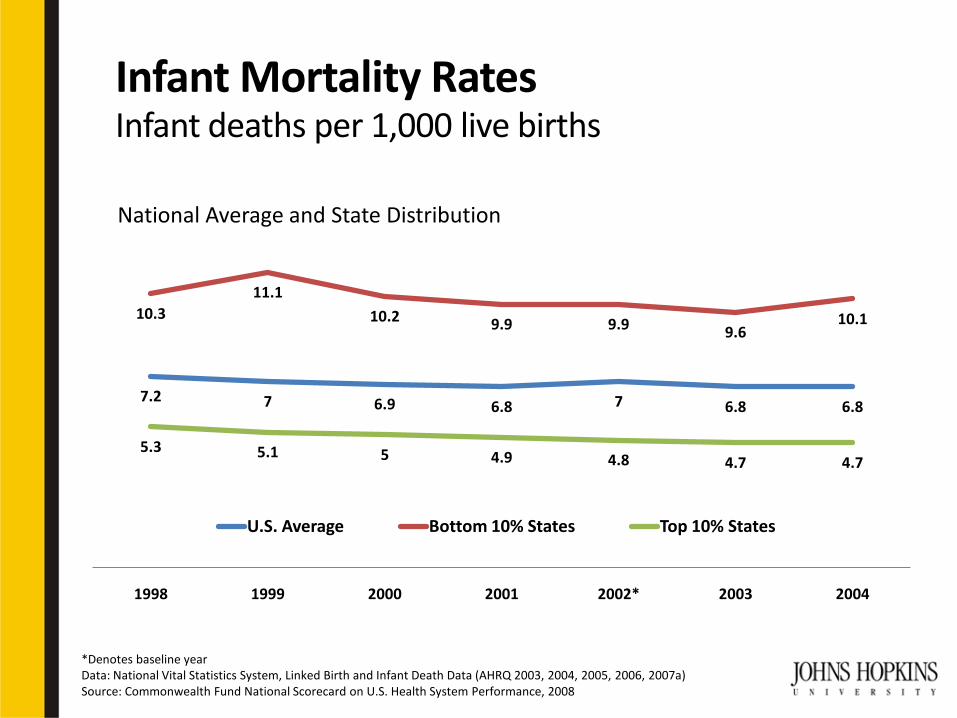
Infant Mortality RatesInfant deaths per 1,000 live births
National Average and State Distribution
*Denotes baseline yearData: National Vital Statistics System, Linked Birth and Infant Death Data (AHRQ 2003, 2004, 2005, 2006, 2007a)Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2008
7.2 7 6.9 6.8 7 6.8 6.8
10.311.1
10.2 9.9 9.9 9.610.1
5.3 5.1 5 4.9 4.8 4.7 4.7
1998 1999 2000 2001 2002* 2003 2004
U.S. Average Bottom 10% States Top 10% States
America’s Got “The Blues”
“The Blues is life.” –Brownie McGhee
“It is from the blues that all thatmay be called American music [and health care?] derives its most distinctive characteristics…”–James Weldon Johnson


![The Bismarck tribune (Bismarck, D.T. [N.D.]). (Bismarck, D ...lithograph of Gen. Custer, two dollars. Address TRIBUNE, Bismarck, D. T. OPPOSITION Pye and others are trying to get up](https://img.pdfslide.us/doc/110x75/5e7562122844324962071477/the-bismarck-tribune-bismarck-dt-nd-bismarck-d-lithograph-of-gen.jpg)

![The Bismarck tribune. (Bismarck, N.D.) 1922-09-13 [p ].chroniclingamerica.loc.gov/lccn/sn85042243/1922-09-13/ed...THE BISMARCK TRIBUNE Entered at the Fostofflce, Bismarck, N. I>„](https://img.pdfslide.us/doc/110x75/5addd20e7f8b9a9a768d6deb/the-bismarck-tribune-bismarck-nd-1922-09-13-p-bismarck-tribune-entered.jpg)