Embed Size (px)
Citation preview

10/12/2016
1
PRETERM DELIVERY IN THE U.S.:DO WE FINALLY HAVE A ROADMAP TO
SUCCESS??
Legacy Emanuel
OB/GYN Educational Series Speaker: Carey Winkler, MD
Oct 24, 2016
ACC-42
Approved 1/11
Practice Gap: Become aware of the multi-faceted causes of preterm birth in the United States
Desired Outcome: Review a “road map” of proposed interventions to decrease the preterm birth rate to 5.5% by 2030
Disclosure of relevant financial relationships in the past 12 months:
Sadly, I have nothing to disclose!!!!
RESULTS FOR PREVIOUS PRETERM BIRTH PREVENTION PROGRAMS BACKGROUND
• Until recently, preterm births were stable at approximately 12%
• That equates to 1 in 8 births!!!!!
• Maybe starting to see a decrease in the overall incidence
BACKGROUND
•Why the decrease???• 39 week initiative???
• 17-P???
• More awareness???
• Changing definition???• 11.5% vs. 9.7% comparing LMP dating to obstetrical dating
BACKGROUND
•39 week initiative has had a major effect on PTB• Number of late preterm deliveries have decreased (iatrogenic)
•VLBW have remained stable

10/12/2016
2
BACKGROUND BACKGROUND
BACKGROUND
• Multi factorial disease process
• Therefore, no one “silver bullet”
• Need to take many baby steps to achieve goal of reducing preterm delivery rate
RISK FACTORSPrior preterm birth Multiple gestations
Uterine anomalies Trauma
Obesity Substance abuse
Closely spaced pregnancies Tobacco
Some medical conditions Cervical surgery
Congenital malformations Ethnicity
Social economic factors STD’s
Extremes of age Low BMI
Short cervix
ETIOLOGIES OF PRETERM BIRTHS SUCCESS ON THE HORIZON??

10/12/2016
3
PRIOR PRETERM BIRTH
Prevention of recurrent PTL by 17 alpha-hydroxyprogesterone caproate
• Randomized prospective placebo controlled trial
• Over 450 patients with 2:1 ratio of progesterone to placebo
• All had prior preterm birth
• Singleton fetus
• No significant medical problems
Meis PJ et al NEJM June 2003 pp2379-2385
Prevention of recurrent PTL by 17 alpha-hydroxyprogesterone caproate
• Based on patient demographics, recurrence risk in placebo arm determined to be about 37%
• Require approximately 500 patients in 2:1 randomization to demonstrate a 33% reduction in preterm delivery
Meis PJ et al NEJM June 2003 pp2379-2385
Prevention of recurrent PTL by 17 alpha-hydroxyprogesterone caproate
• Initial part of study that involved 150 patients was terminated due to violation of manufacturing/compounding process
•86 completed treatment• 57 (61%) with 17-P• 29 (39%) with placebo
•Delivery at < 37 weeks• 17-P 43%• Placebo 38%
Meis PJ et al NEJM June 2003 pp2379-2385
Prevention of recurrent PTL by 17 alpha-hydroxyprogesterone caproate
Characteristic Progesterone Placebo RR
# of PTD 1.4 1.6 NS
Del. < 37 wks
(%)
36.3 54.9 0.66
Del. < 35 wks
(%)
20.6 30.7 0.67
Del. < 32 wks
(%)
11.4 19.6 0.58
IVH (%) 1.3 5.4 0.25
NEC (%) 0.0 2.6 NS
Meis PJ et al NEJM June 2003 pp2379-2385

10/12/2016
4
Excuse me, do you think it really works???
PRIOR PRETERM BIRTH
• One of the biggest risk factors
• The more preterm births, the higher the risk in subsequent pregnancies• 1 prior preterm birth 20%
• 2 prior preterm births 30%
• 3 prior preterm births TUBAL!!!!
RECURRENCE RISKRISK OF PRETERM BIRTH
• Term/term 4%
• PTD/term 12%
• Term/PTD 23%
• PTD/PTD 32%
Carr-Hol RA BJOG 1985
RECURRENCE RATES OF PRETERM BIRTH
Carr-Hol 32%
Bloom ~35%
Esplin ~35%
O’Brien 40%
Da Fonseca 29%
SMFM prediction 37%
Meis 54%
RECURRENCE RISK FOR PRETERM BIRTH
•Retrospective review
•15,945 consecutive deliveries
•10 year period
•Spontaneous preterm delivery of singleton in first pregnancy
•16% delivered early in next pregnancy
•41% early if first 2 were early
•67% early if first 3 were early (small #’s)
Bloom SL et al Obstet Gynecol 2001;98:379-85

10/12/2016
5
RECURRENCE RISK FOR PRETERM BIRTH
• Of the preterm patients• 49% delivered within 1 week
• 70% delivered within 2 weeks
• All of these patients accounted for only 10% of the preterm births
• Only treating patients with prior preterm birth will not have significant impact on preterm rate
Bloom SL et al Obstet Gynecol 2001;98:379-85
Prophylactic administration of progesterone by vaginal suppositories
to reduce recurrent preterm birth
•142 high risk patients (mostly a prior preterm birth)
•Randomized to daily suppository of 100 mg progesterone vs. placebo
•Delivery: Progesterone Placebo
< 37 wks 13.8% 28.5%
< 34 wks 2.8% 18.6%
Da Fonseca EB et al AJOG 2003;188:419-424
PROGESTERONE GEL FOR RECURRENT PRETERM BIRTH
• Randomized placebo controlled trial of 659 patients• 328 placebo
• 331 Prochieve (8% progesterone)
• 60% in each group had prior delivery at < 32 weeks
• No demographic differences
O’Brien JM Ultra OB/GYN, 2007;30(5):687
PROGESTERONE GEL FOR RECURRENT PRETERM BIRTH
• No difference between groups in:• Mean gestational age at delivery
• Deliveries < 37 weeks
• Deliveries < 32 weeks
• Mean birthweight
• Neonatal morbidity
• Neonatal mortality
O’Brien JM Ultra OB/GYN, 2007;30(5):687
RECURRENCE RISKFOR PRETERM BIRTH
Progesterone Placebo
# prior PTB 1.3 1.4
> 1 prior PTB 23.6% 25.5%
EGA @ rand. 19.9 wks 20.1 wks
Del. < 37 (%) 41.7 40.7
Del. < 35 (%) 22.7 26.5
Del. < 32 (%) 10.0 11.3
Del. < 28 (%) 3.2 3.0
O’Brien JM et al Ultrasound Obstet Gynecol 2007;30(5):687-696
SUMMARY
• Weekly 17-P may be helpful in reducing recurrence risk of PTB
• Only 10% of preterm deliveries are in a patient who had a prior PTB
• Vaginal progesterone may not be as effective as 17-P for prophylaxis
• Need other interventions!!!!!!

10/12/2016
6
WHAT MIGHT BE A GAME CHANGER!!!
Source: Iams JD et al. N Engl J Med. 1996;334:567-572.
Preterm Delivery <35 Weeks
Risk of PTD by Cervical Length
Pro
ba
bilit
y o
f P
rete
rm D
eliv
ery
0.5
0.4
0.3
0.2
0.1
0.0
0 20 40 60 80
Cervical Length (mm)
SHORT CERVIX AND VAGINAL PROGESTERONE
Fonseca, NEJM. 2007;357:462
• 413 patients with TVUSCL < 15 mm• 250 vaginal PG @ 200 mg nightly
• 163 placebo
• Mean EGA = 22 weeks
• Randomized between 20 -25 weeks
• Delivery at < 34 weeks• Progesterone 19.2%
• Placebo 34.4%
SHORT CERVIX AND VAGINAL PROGESTERONE
Hassan et al. US OB/GYN 2011
•458 patients randomized• 235 vaginal progesterone• 223 to placebo
•Progesterone: 90 mg at night
•TVUSCL: 1.0 to 2.0 cm
•EGA: 19.0 to 24 weeks
•Continued until 36 weeks
SHORT CERVIX AND VAGINAL PROGESTERONEHassan et al. US OB/GYN 2011
•Vaginal progesterone had: • < 35 weeks (14.5% vs 23.3%)
• < 33 weeks (8.9% vs. 16.1%)• < 28 weeks (5.1% vs 10.3%)• Less RDS (3.0% vs. 7.6%)• Less BWT < 1500 gms (6.4% vs. 13.6%)• Less any morbidity (7.7% vs. 13.6%)
SHOULD WE SCREEN EVERY0NE’S CERVIX AT 20 WEEKS?
•Mathematical models using 4 scenarios• No screening/treatment at all• Treat at risk patients with 17-P due to history• Cervical length on high risk patients and treat with
vaginal progesterone if short• Screen all patients and treat if short cervix
•Short cervix < 1.5 cm
•Universal screening and treatment if short was the best strategy
Cahill AG AJOG June 2010 202(6);548.e1-548.e8.
10/12/2016
7
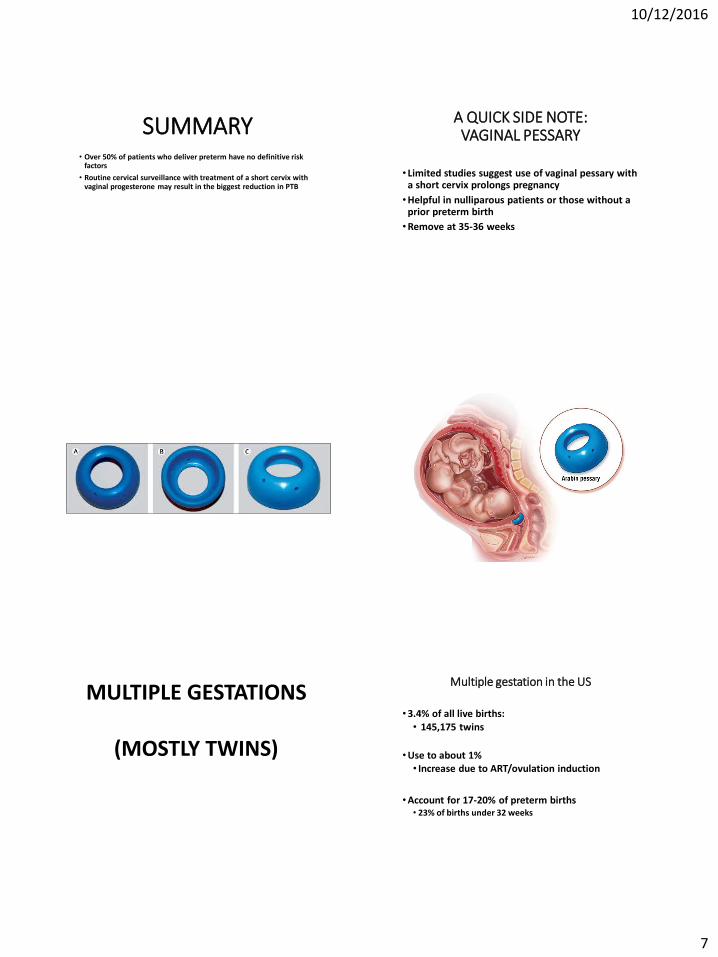
SUMMARY• Over 50% of patients who deliver preterm have no definitive risk
factors
• Routine cervical surveillance with treatment of a short cervix with vaginal progesterone may result in the biggest reduction in PTB
A QUICK SIDE NOTE:VAGINAL PESSARY
• Limited studies suggest use of vaginal pessary with a short cervix prolongs pregnancy
•Helpful in nulliparous patients or those without a prior preterm birth
•Remove at 35-36 weeks
MULTIPLE GESTATIONS
(MOSTLY TWINS)
Multiple gestation in the US
•3.4% of all live births:• 145,175 twins
•Use to about 1%• Increase due to ART/ovulation induction
•Account for 17-20% of preterm births• 23% of births under 32 weeks

10/12/2016
8
Gestational age at delivery
• Twins: 35.3 weeks• 11% deliver prior to 32 weeks
• Triplets: 32.0 weeks
• Quads: 30.7 weeks
• Natl Vital Stat Rep (2008)
Risk of Twinning1. Ethnic background
2. Maternal age
3. Parity
4. Family history of dizygotic twins
5. Previous twins
6. Clomid therapy (5-10%)
7. Gonadotropin therapy (20-40%)
8. IVF : 25-30 %
ART and management of multiple gestation risks:
• In 2003, revision of Swedish law regarding multiple embryo transfer
• Single embryo transfer strongly recommended
• Multiple birth rate fallen from 35% to 5%
Single and multiple embryo transfers: successful pregnancy and multiple gestation Multiple embryo transfers in IVF in the US:
• 90% of transfers - at least 2 embryos
• 40% of transfers - 3 embryos
• CDC -2006: ART success rates

10/12/2016
9
40% decline in rate of triplets and quadruplets in the US:
•1998: 7,625
•2014: 4,526
• “Single embryo transfers” more routine
CDC-NCHS : May 2016
INDICATEDPRETERM
DELIVERIES
INDICATED PRETERM BIRTH
• Account for 20-30% of PTB
• Include but not limited to• Preeclampsia
• Abruption
• IUGR with fetal compromise
• Previa/implantation issues
• Other things I can’t think of right now!!!
RISK FACTORS FOR PREECLAMPSIA
• Primiparity
• Previous preeclamptic pregnancy (especially if severe) –
has 7 fold increase
• Chronic hypertension, chronic renal disease, or both
• History of thrombophilia (?)
• Multifetal pregnancy
• In vitro fertilization
• Family history of preeclampsia - 2-4 fold increase
• Diabetes mellitus
• Obesity
• Systemic lupus erythematosus
• Advanced maternal age (> 40 years
OTHER STUFF
• Accounts for 12% - 16% of maternal deaths
• 15% of preterm births are related to preeclampsia
• Leading cause of:
-Fetal growth restriction
-Indicated preterm delivery
-Maternal and perinatal death and morbidity

10/12/2016
10
LOW DOSE ASPIRIN
• Unclear how it works
• May alter prostacyclin/thromboxane ratio to favor vasodilatation
• Fell out of favor in the early 2000’s
• Recent review/recommendations of the USPSTF now recommends LDA
LOW DOSE ASPIRIN
• Needs to be started early• Between 12 and 16 weeks
• Recommended dose• 81 mg/day
• Continue until delivery
• Which group(s) of patients may benefit most is somewhat unclear
• No maternal or fetal risks
LOW DOSE ASPIRIN
• Benefits of LDA are reduction of• Preterm birth 10-14%
• Preeclampsia 10-24%
• IUGR 10-20%
• Too small of numbers to demonstrate a reduction in perinatal mortality
SUMMARY• Recommended to start low dose aspirin between 12-16 weeks
• High risk patients with one risk factor
• Medium risk patient with multiple risk factors

10/12/2016
11
INTERPREGNANCY INTERVAL
• Defined as time from last pregnancy to conception of the next
• Optimal timing is 18 months or greater
• The shorter the interval, the higher the risk of complications
INTERPREGNANCYINTERVAL
• Spacing closer to 18 months increases the risk of • Preterm birth
• Small for gestational age infants
• Low birthweight
• The closer the spacing, the higher the risks, especially if < 6 months
For each month that birth spacing was less than 18
months,
Preterm births increased 1.9%
Low birthweight increased 3.3%
Poor intrauterine growth increased 1.5%
Conde-Agudelo JAMA 2006 295(15) 1809-23.
INTERPREGNANCYINTERVAL
•Many pregnancies are unplanned• Nearly 50%, higher in younger patients
•Nearly 1/3 of pregnancies have an IPI of < 18 months
•Concern of many organizations
•ACOG Committee Opinion Feb 2016 addresses some of these issues
• “encourages obstetrician-gynecologists and other health care providers to use every patient encounter as an opportunity to talk with patients about their pregnancy intentions and to support initiatives that promote access to and availability of all effective contraceptive methods.”
18 Months: HP 2020 Goal, ACOG Recommendation
•Healthy People 2020 birth spacing goal: reduce the proportion of pregnancies conceived within 18 months of a previous birth by 10%, to 29.8%.
•ACOG recommends that “women wait at least 18 months after having a baby before trying to get pregnant again in order to have the best health outcomes for both mom and baby.”
ACOG Committee Opinion. 2015. Your Pregnancy and Childbirth Month to Month. Sixth Edition. pp. 585-586

10/12/2016
12
One Key Question® Initiative: Recommended in ACOG Committee Opinion
• This campaign promotes direct screening for women’s pregnancy intentions by asking the following question ……
• “Would you like to become pregnant in the next year?”
• If the answer is “no,” discuss pregnancy prevention, including education and counseling on all available contraceptive options.
• If the response is “yes,” provide preconception counseling and discuss evidence-based lifestyle modifications to optimize health status in preparation for future pregnancies.
QUESTIONS?
CENTERING CARE• Patient centered care
• Group visits for patients with• Similar medical problems
• Similar gestational age
• Recent postpartum patients
• Parenting
CENTERING CARE• Group setting health care leads to
• Greater engagement
• Better learning
• More self confidence
• Better compliance
• Overall improved outcomes
• Reduced costs
CENTERING CARE• Centering Pregnancy has led to
• Lower preterm deliveries• Decreased racial disparities in preterm births
• Less low birthweight babies
• Higher rates of breastfeeding
• Better pregnancy spacing
• Better compliance with well baby follow up along with immunizations
CENTERING CARE• Less excessive maternal weight gain
• Better compliance with GDM management
• Improved exercise compliance
• Lower infant mortality

10/12/2016
13
SOMEEXAMPLES!
• Retrospective cohort analysis• 5003 traditional care deliveries (TC)• 444 Centering care deliveries (CC)
• Controlled for parity, race, prior preterm deliveries
• Comparing CC to TC, CC had• Less NIU admissions 12.6 to 18.3%
• Less deliveries < 34 weeks (OR = 0.43, p = 0.006)
• Higher mean EGA at delivery by nearly 1 week (p = 0.0004)
Obstet Gynecol May 2016; vol 127: no 5, 17S
• Retrospective cohort study with GDM• 89 with CC, 118 with TC
• In CC care patients, had:• Less need for medication (26.1% vs 38.1%)• Less need for inductions (27.3% vs 42.7%)• Higher breastfeeding (89.8% vs 65.8%)• Higher postpartum testing (86.5% vs 60.2%)
Am J Obstet Gynecol : Jan 2013
Group Prenatal Care Versus Individual Prenatal Care: A Systematic Review and Meta-Analyses
• Total of 8 studies of mostly low quality• 3 randomized, 5 cohort trials involving 3242 patients
• The GPC to IPC, the GPC had• Lower PTB (RR = 0.71 CI 0.56 – 0.96)
• Lower cesarean section (RR = 0.80 CI 0.67 – 0.93)
• Higher breastfeeding (RR = 1.08 CI 1.02 -1.14)
• No difference in LBW, IUGR
• Conclusion: Though low quality studies, it appears GPC has some benefits over traditional IPC specifically PTB
Ruiz-Mirazo et al, J OB/GYN Canada 2012: 34(3); 223-229

10/12/2016
14

10/12/2016
15
SUMMARY• Preterm birth is still a major health care problem in the U.S.
• During the last few years, the preterm delivery rate may be slowing
• Preterm birth is a multi-faceted problem requiring multi-pronged approach
SUMMARY• How to achieve goal of a preterm delivery rate of 5.5% by 2030???
• Decrease rate of multiples
• Universal cervical length screening• Treat with pessary and progesterone
• Low dose aspirin in patients at high and moderate risk for preeclampsia
SUMMARY• How to achieve goal of a preterm delivery rate of 5.5% by 2030???
• Increasing interpregnancy interval to at least 18 months
• Centering prenatal care
• Centering postpartum/parenting care to decrease infant mortality rate
THANK YOU!!!
QUESTIONS??





























