Embed Size (px)
DESCRIPTION
This report details the purpose of biosurveillance and disease reporting systems and the barriers to early adoption and success. Much like the federal government’s BioSense project, state and local health departments are rapidly deploying their own disease surveillance systems, in an effort to connect the dots between local and regional health care providers.
Citation preview

Biosurveillance and Disaster 1
Running Head: BIOSURVEILLANCE AND DISASTER
Biosurveillance and Disaster Reporting: Barriers to Accuracy and Timeliness
Nia Llenas
UMUC
Peer Reviewer: Carl Mueller

Biosurveillance and Disaster 2
Executive Summary
This report details the purpose of biosurveillance and disease reporting systems
and the barriers to early adoption and success. Much like the federal government’s
BioSense project, state and local health departments are rapidly deploying their own
disease surveillance systems, in an effort to connect the dots between local and regional
health care providers.
Unfortunately, implementing and maintaining a surveillance system requires skill
and attention that many health professionals have yet to practice. While previous studies
have shown success in timeliness and completeness of data capture and transmission,
much of the workflow is left to human intervention.
Several areas to be considered when implementing disease surveillance or disaster
response systems are patient data privacy/security, system languages and coding, and
staff training. Dually noted, are the limitations to current research, namely the small
sample sizes in previous work and the lack of accuracy in electronic laboratory reporting.
In considering biosurveillance system implementation, health care administration
must look to secure patient data behind facility firewalls. Additionally, ensuring that
information is contained in HL-7 fields, coded in LOINC, SNOMED, IDC-9 and NDC,
minimizes delays in downloading and translation by public health officials. Finally, staff
should be trained diligently to recognize the importance of reporting notifiable diseases,
completely and in a time-efficient manner.

Biosurveillance and Disaster 3
Table of Contents
1. Introduction
a. Purpose
b. Problem
c. Background
d. Objectives
2. Literature Review
a. Implementation
b. ELR and EMR reporting
3. Barriers to adoption
a. Patient data security
b. Languages
c. Training staff
d. Reporting and monitoring limitations
4. Conclusion
5. References
6. Appendices
7. Glossary

Biosurveillance and Disaster 4
Introduction
In 2007, the Department of Health and Human Services released a working draft
of the Biosurveillance Workgroup Priority Areas. The stated focus of the workgroup is to
“recognize the critical importance of an integrated and interconnected public health and
healthcare delivery system that enables real-time, secure, and appropriate bi-directional
exchange of information” (Biosurveillance Priority Areas, 2007). Specifically, the
workgroup centers around the effort to produce a secure and timely method of
transmitting standardized data from a patient’s electronic medical records (EMR) and
electronic laboratory systems (ELR) to public health officials and back. This direct
communication between public health systems, healthcare delivery organizations, VA,
laboratory organizations and poison control centers will result in real-time reporting of
adverse events and outbreaks, while providing current public health statistics to
clinicians.
Several factors play a role in the success of systems like BioSense; real-time
transmission, geospatial mapping, patient privacy, and concise ICD-9 coding are some of
the areas under examination that can affect the reliability of surveillance systems. In this
paper, the barriers to timely, accurate surveillance data are investigated in conjunction
with the efforts of several states to implement effective surveillance and disaster response
systems.
In the past, communicable disease outbreaks and regional health statistics have
been largely reported on paper-based systems. Early adoption of electronic laboratory
reporting systems have subsequently reduced reporting errors while increasing test
volume, thereby being hailed as milestone in disease surveillance (Nguyen, Lorna,

Biosurveillance and Disaster 5
Mostashari, & Makki, 2007). Unfortunately, problems still arise and early adoption has
been slow as public health officials determine vocabulary standards of laboratory code,
patient identification/security and HIPPA considerations (Overhage, Grannis, &
McDnoald, 2008)
Currently, public health is still reliant on clinicians to interpret laboratory data and
assign specific demographic characteristics to that data in order to transmit useful
information to public health officials. This process is time consuming as most of it is still
done by fax, email or phone, resulting in incomplete data capture (Klompas, et al., 2007).
Overhage, Grannis and McDonald (2008) recently reported that in a study of the Vermont
Department of Health, 71% of all infectious cases were reported directly by laboratories,
giving more meaning to the need for automated ELR and EMR systems link to public
health officials.
This present research attempts to address the problems associated with the
implementation of detection systems, data collection and data transmission to the national
disease surveillance system and subsequent effects of disaster response on the health
system. This directly relates to the concepts under review in the University of Maryland
University College HCAD 610 course.
Literature Review
Implementation
Previous research provides similar experiences with structuring and implementing
surveillance systems. Brownstein and Mandl (2006) reported the efforts of the
Massachusetts Department of Public Health transforming its AEGIS system into a real-
time influenza monitoring system using chief complaint data from emergency

Biosurveillance and Disaster 6
departments to formulate the predictions of the start of influenza and pneumonia
outbreaks, subsequently comparing data to trends of the previous five years. Although
AEGIS was able to accurately predict influenza outbreaks, some systems are struggling
to transmit consistently accurate reports.
Grannis, Wade, Gibson and Overhage (2006) presented early finding from the
Indiana State Department of Health’s statewide surveillance project. The platform is built
on a standard of HL7 messages containing chief complaint data, clinical messaging and
ELR, transmitting results from emergency departments to local and state health
departments for review. Public health officials are attempting to reduce the number of
false positive signals that prompt human interaction and review, furthermore causing
unnecessary staff attention and investigation.
On a larger scale, clinical systems are rapidly testing and implementing
surveillance systems to include multi-location hospitals and outpatient facilities.
Gundlapalli et al., (2007) detailed a pivotal study on the implementation in of hospital
EMR surveillance during the 2002 Winter Olympic Games in, in which, a rules-based
system was developed to monitor admission/discharge/transfer, laboratory and radiology
databases of Utah’s University Hospital system. Klompas et al. (2007) also undertook
multi-practice implementation, which succeeded in protecting patient privacy in data
transfers to public health authorities by keeping patient health information (PHI) behind
the facilities firewall.
ELR and EMR reporting
Laboratories and hospital records play a pivotal role in disease surveillance.
While labs cannot attest to the nature of patient care, they do however possess the

Biosurveillance and Disaster 7
“information infrastructure and processes to facilitate reporting” (Overhage, Grannis, &
McDnoald, 2008). Unfortunately, the transition from paper to electronic lab reporting has
been slow, according to Nguyen et al. (2007) report on the New York City Department of
Mental Health and Hygiene (NYC DOMHM) largely due to improper training and low
sense of urgency among laboratory staff. Additionally, Overhage et al. (2008), et al found
that lack of communication with laboratory IT staff greatly hampered efforts to transition
to electronic reporting methods.
The use of EHR in surveillance and disaster response has been mastered by the
Department of Veterans Affairs (VA) medical system. During the most recent disaster,
Hurricane Katrina, the VA “rehosted” its VistA system by moving all data to Houston. In
effect, they lost only four days of access and were able to create a web-based system for
access to patient files of those who were displaced (Brown, et al., 2007). As an
afterthought, patient data of those who survived the disaster provides real-time
biosurveillance information to both the VA and Department of Defense.
Data security and privacy
Data security is a concern not only for patients but medical and public health
officials alike. When clinics and laboratories transmit data to health departments, the
CDC and the federal BioSense surveillance systems, data security parameters vary
widely. The Harvard Vanguard’s Medical Associates’ Electronic medical records Support
for Public health (ESP) database and software systems are located separately on location,
not only to relieve any burden on the host server, but to also secure PHI behind the
practice firewall until information is sent to the health department (Klompas, et al.,
2007). Similarly, the TheraDoc system, utilized during the 2002 Winter Olympics,

Biosurveillance and Disaster 8
available for access through the hospital intranets, was subject to the same security layers
as the hospital itself. In this instance, only infection control practitioners were provided
access to surveillance data. (Gundlapalli et al., 2007)
The aforementioned models serve as examples of measures taken to properly
secure access and transmission of PHI. Unfortunately, there are issues with securing all
demographic attributes of a patient diagnosed with a notifiable condition and
subsequently compiling accurate data. BioSense uses a complex set of rules to define
geographic location of infection. By utilizing the reporting facilities zip code and the
patient residence zip code, a common zip code is mapped and recorded as the point of
infection (English, et al., 2006). Likewise, cluster detection is at the forefront of the
patient privacy debate in surveillance. Epidemiologists are arguing whether the insecurity
of using patient locations (home addresses) to pinpoint disease clusters outweighs the risk
of less accurate data associated with using administrative regions (zip codes). Studies
have shown that exact coordinates found 73% of disease clusters compared to 45% of
administrative coordinates, and are likely to lead other surveillance systems to use the
same information, leaving patients health records exposed. (Olson, Grannis, & Mandl,
2006)
Languages
Currently, there are several major languages utilized by disease surveillance
systems. HL7 is the nationally recognized standard for communication between hospitals,
laboratories and public health applications and is frequently used in conjunction with
free-text messaging in the transmission of patient information (Grannis, Wade, Gibson, &
Overhage, 2006). Equally important is the HL7 supported bi-directional communication

Biosurveillance and Disaster 9
in free-text, supporting quick responses to health department queries for case details from
laboratories and clinic sites (Klompas, et al., 2007). The importance of HL7 in disease
surveillance will become more apparent as more clinic level providers begin using EMR
systems, supplying more in-depth patient information to surveillance systems.
Surveillance systems also read SNOMED and LOINC codes, the universal
medical and laboratory terminology used by clinicians, practices, laboratories and
hospitals. Laboratories have historically used free-text coding instead of SNOMED,
causing some issues in workflow for public health officials. Ideally, laboratory tests
should be identified using LOINC, there results as SNOMED and finally the diagnoses as
ICD-9. The NYC DOHMH saw a high numbers of false positives due to laboratory staff
forsaking the use of proper codes for free-text, causing common illnesses to flag more
serious rare illnesses (Nguyen, Lorna, Mostashari, & Makki, 2007).
Training staff
It has been suggested that the success of disease surveillance largely depends on
the level of trust, respect and familiarity between health officials and healthcare
personnel (Buehler, Isakov, Prietula, Smith, & Whitney, 2007). When introducing new
systems and workflows to hospital, laboratory and IT staff, careful measures must be
taken to stress the importance of compliance. Staff must be trained to use and trouble
shoot the system effectively and efficiently. In actuality, implementing an ELR system
that reports to state health systems may require site certification that depends on the staff
knowledge and presence.
Laboratories in New York City must complete a certification process to transmit
electronically to public health departments and additionally, lab staff and IT department’s

Biosurveillance and Disaster 10
need training on quality assurance and database management (Nguyen, Lorna,
Mostashari, & Makki, 2007). Success in reporting completeness has also been attributed
to provider awareness, staff motivation, and effective processes in laboratories and clinics
where systems are monitored regularly (Overhage, Grannis, & McDnoald, 2008).
Therefore, staff should undergo training to stress the importance of proper coding and
reporting and its implication on local and national efforts to maintian healthy
communities.
Reporting limitations
While electronic surveillance is an effective way to monitor communicable or
notifiable diseases, it does carry risks that are assumed as a result of reporting limitations.
Current research is generally limited to local databases and laboratories, therefore
limiting sample sizes. Equally important, many notifiable conditions do not translate well
in ELR, such as tuberculosis, syphillis and meningitis. Condidtions requiring multiple or
varied tests to confirm a true positive are frequently reported incorrectly and may prompt
further investigation from public health officials (Nguyen, Lorna, Mostashari, & Makki,
2007) (Overhage, Grannis, & McDnoald, 2008).
Recommendations
A strong push towards electronic methods of storing and transmitting medical
data will transform the biosurveillance industry and health care providers must prepare
themselves with the knowledge and facilities to join in. Transmitting patient and disease
data will no doubt require careful planning regarding vendor systems, integration into the
state and local networks, designating staff, improving training and mastering quality
assurance.

Biosurveillance and Disaster 11
Also, being aware that as technology evolves, barriers to success are consistently
present. These barriers mentioned in this paper, can be overcome through new , thorough
innovations in electronic laboratory reporting and expanded research in the field.
Conclusion
As the U.S. moves towards a more complete and connected biosurveillance
system, consideration must be given to the security, timeliness and accuracy of the data
and its transmission. All efforts to respect patient privacy should be taken, even if at the
expense of accuracy. Furthermore, in order for system implementation and execution to
be successful, laboratory teams and clinical staff must have proper training that highlights
the importance of data reporting to local health departments and the CDC.
Biosurveillance and disaster reporting depend on accuracy and dedication of all involved,
for without it, national security and health may be at risk.

Biosurveillance and Disaster 12
Bibliography
“Biosurveillance Priority Areas”. (2007). Department of Human Health and Human
Service. Retrieved February 28, 2008, from
http://www.hhs.gov/healthit/ahic/materials/04_07/phc/bsvpriority.html
Blair, R. (2007). Disaster-proof patients. Health Management Technology , 28 (2), 44-47.
Retrieved February 27, 2008, from Buisness Source Premier database.
Brown, S. H., Fischetti, L. F., Graham, G., Bates, J., Lancaster, A. E., McDaniels, D., et
al. (2007). Use of electronic health records in disaster response: The Experience
of Department of Veterans Affairs after hurricane Katrina. American Journal of
Public Health , 97 (S1), S136-S141. Retrieved February 23, 2008, from Buisness
Source Premier database.
Brownstein, J. S., & Mandl, K. D. (2006). Reeingineering real time outbreak detection
systems for influenza epidemic monitoring. American Medical Informatics
Association (p. 866). Washington: AMIA.
Buehler, J. W., Isakov, A. P., Prietula, M. J., Smith, D. J., & Whitney, E. A. (2007).
Preliminary findings from the BioSense evaluation project. Advances in DIsease
Surveillance , 4, 237.
English, R., McMurray, P. C., Sokolow, L. Z., Rolka, H., Walker, D., Quinn III, J. F., et
al. (2006). Geographic categorization methods used in BioSense. Advances in
Disease Surveillance , 1 (24).
Grannis, S., Wade, M., Gibson, J., & Overhage, J. M. (2006). The Indiana public health
emergency surveillance system: Ongoing progress, early findings, and future

Biosurveillance and Disaster 13
directions. AMIA 2006 Symposium Proceedings (pp. 304-308). Washington:
American Medical Informatics Association.
Gundlapalli, A. V., Olson, J., Smith, S. P., Baza, M., Hausam, R., Eutropius, L. J., et al.
(2007). Hospital electronic medical record-based public health surveillance
system deployed during the 2002 winter Olympic games. American Journal of
Infection Control , 35 (3), 163-171. Retrieved February 23, 2008, from Buisness
Source Premier database.
Klompas, M., Lazarus, R., Daniel, J., Haney, G. A., Campion, F. X., Kruskal, B. A., et al.
(2007). Electronic medical record support for public health (ESP): Automatic
detection and reporting of statutory notifiable diseases to public health authorities.
Advances in Disease Surveillance , 3 (3), 1-5. Retrieved February 26, 2008, from
Google Scholar database.
Krishna, R., Kelleher, K., & Stalhberg, E. (2007). Patient confidentiality in the research
use of clinical medical databases. American Journal of Public Health , 97 (4),
654-658. Retrieved February 25, 2008, from ABI/Inform database.
Mack, D., Brantley, K., & Bell, K. G. (2007). Mitigating the health effects of disasters for
medically underserved populations: Electronic health records, telemedicine,
research, screening and surveillance. Journal of Health Care for the Poor and
Underserved , 18, 432-442. Retrieved February 29, 2008, from Project Muse
database.
Nguyen, T. Q., Thorpe, L., Makki, H., & Mostashari, F. (2007). Benefits and barriers to
electronic laboratory results reporting for notifiable diseases: The New York City
Department of health and mental hygeine expert. American Journal of Public

Biosurveillance and Disaster 14
Health , 97 Olson, K. L., Grannis, S. J., & Mandl, K. D. (2006). Privacy
protection bersus cluster detection in spatial epidemiology. American Journal of
Public Health , 96 (11), 2002-2008. (S1), S142-S145. Retrieved February 23,
2008, from Buisness Source Premier database.
Olson, K. L., Grannis, S. J., & Mandl, K. D. (2006). Privacy protection bersus cluster
detection in spatial epidemiology. American Journal of Public Health , 96 (11),
2002-2008.
Overhage, J. M., Grannis, S., & McDonald, C. J. (2008). A Comparison of the
completedness and timeliness of automated electronic laboratory reporting and
spontaneous reporting of notifiable conditions. American Journal of Public
Health , 98 (2), 344-350. Retrieved February 29, 2008 from Academic Search
Premier database.

Biosurveillance and Disaster 15
Appendix
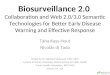
View of patient distribution map from BioSense
Downloaded from http://www.cdc.gov/biosense/images/patient_distribution_full.jpg
BioSense map of weekly volume of notifiable diseases from LabCorp
Downloaded from http://www.cdc.gov/biosense/publichealth.htm

Biosurveillance and Disaster 16
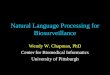
Clinic system formats data:Data fields>HL7Lab tests>LOINCResults>SNOMEDDiagnoses>ICD-9Prescription>NDC
Case is identified; system is queried
ICD-9 codes and vital are assessed to determine if case is reportable disease
Case is sent to health department and CDC for submission to local and national database
Yes
Case management system presents infection control practitioner (ICP) with list of suspected positives
Possible positives
ICP reviews cases behind practice firewall
ICP rejects false positives
ICP sends positives back to ordering clinician, and reports to health department and CDC
Flow of data from reporting health system to the surveillance system, i.e. Health department, BioSense, etc.

Biosurveillance and Disaster 17
Glossary
BioSense- national real-time surveillance system operated by the Centers for Disease
Control. Information can be found at http://www.cdc.gov/biosense/
Biosurveillance- related to epidemiology; immediate monitoring of public health data
preferable through electronic reporting
Deidentification- terminology used to describe the process systems use to encrypt patient
data in order to comply with HIPPA regulations
HL7-Health Level 7 information can be found at http://www.hl7.org/
ICD-9- International Classification of Diseases information can be found at
http://www.cdc.gov/nchs/icd9.htm
NDC- National Drug Code directory information can be found at
http://www.fda.gov/cder/ndc/
Notifiable diseases- diseases that present a danger to the public and should be
immediately reported to public health officials
LOINC-Logical Observation Identifiers Names and Codes information can be found at
http://www.regenstrief.org/medinformatics/loinc/
SNOMED or SNOMED-CT- Systemized Nomenclature of Medicine- Clinical Terms
information can be found at http://www.snomed.org/