Embed Size (px)
Citation preview
Biosurgery: Core Products Provide Foundation for Growth
Ann Merrifield, President
May 7, 2008 Analyst Day

2
Biosurgery Today
Sepra® Family Epicel®
Marketed Products and Services
Carticel® / MACI®*Synvisc®
Osteoarthritis OrthopaedicBiologics
AdhesionPrevention
Severe Burn
*Marketed in Europe and Australia
3
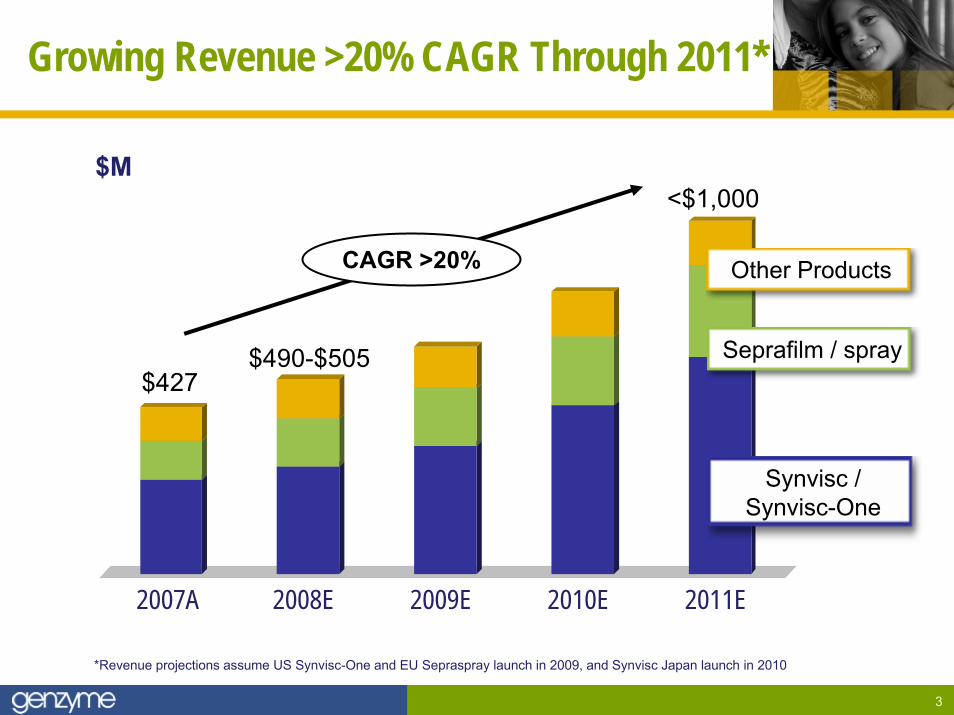
Growing Revenue >20% CAGR Through 2011*
2007A 2008E 2009E 2010E 2011E
$427
<$1,000
$490-$505
Synvisc / Synvisc-One
Seprafilm / spray
Other Products
$M
*Revenue projections assume US Synvisc-One and EU Sepraspray launch in 2009, and Synvisc Japan launch in 2010
CAGR >20%
4
Agenda
► Sepra family
► Synvisc and Synvisc-One
► Growth opportunities beyond 2011
5
Sepra Growth Drivers
►Seprafilm: diversification to adjacent procedures– Colorectal trauma– Gynecology ob-gyn
►Sepraspray: 2-3x film opportunity
►Ex-US “relaunch” with combined film / spray portfolio
Growth

6
Global Seprafilm Revenue Growth
2003 2004 2005 2006 2007
$46
$99
$59$64
$79
$M
7
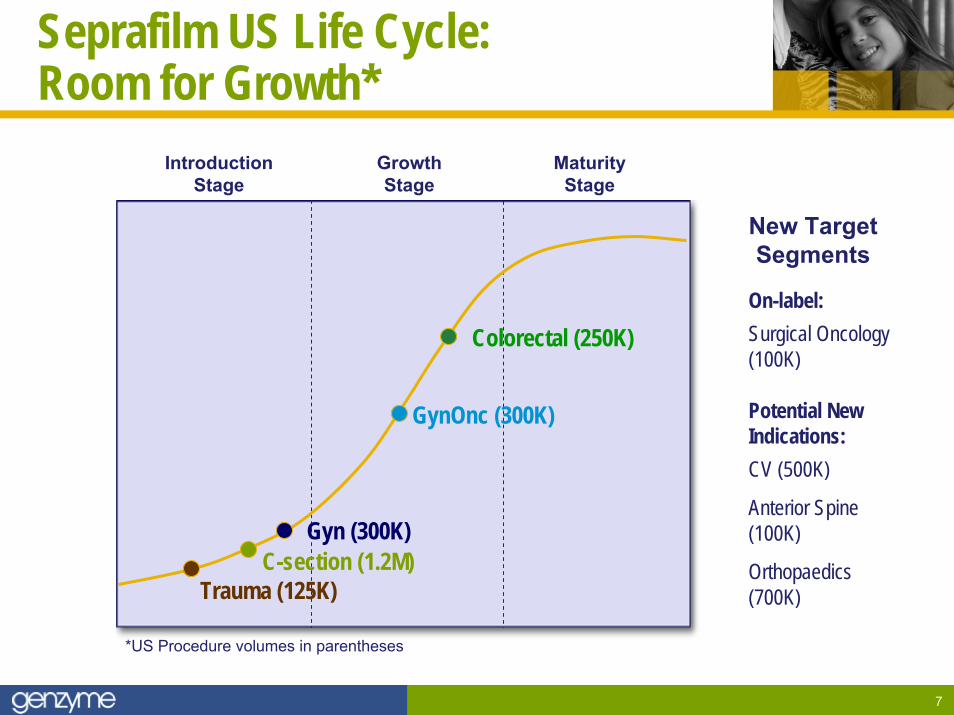
Seprafilm US Life Cycle: Room for Growth*
*US Procedure volumes in parentheses
On-label:Surgical Oncology (100K)
Potential New Indications:CV (500K)
Anterior Spine (100K)
Orthopaedics(700K)
New TargetSegments
Introduction Stage
GrowthStage
MaturityStage
C-section (1.2M)
GynOnc (300K)
Colorectal (250K)
Gyn (300K)
Trauma (125K)
8
Creating Opportunity: US C-Section Consumer Program
► Branded program educating women on internal scarring
► Seprafilm Concierge offers useful services for women and metrics for Genzyme
► Enabling the sales process: – Sales representatives targeted
to educate specific physician as directed by patient
► Program initiated Q2:08
CSectionhealing.com
9
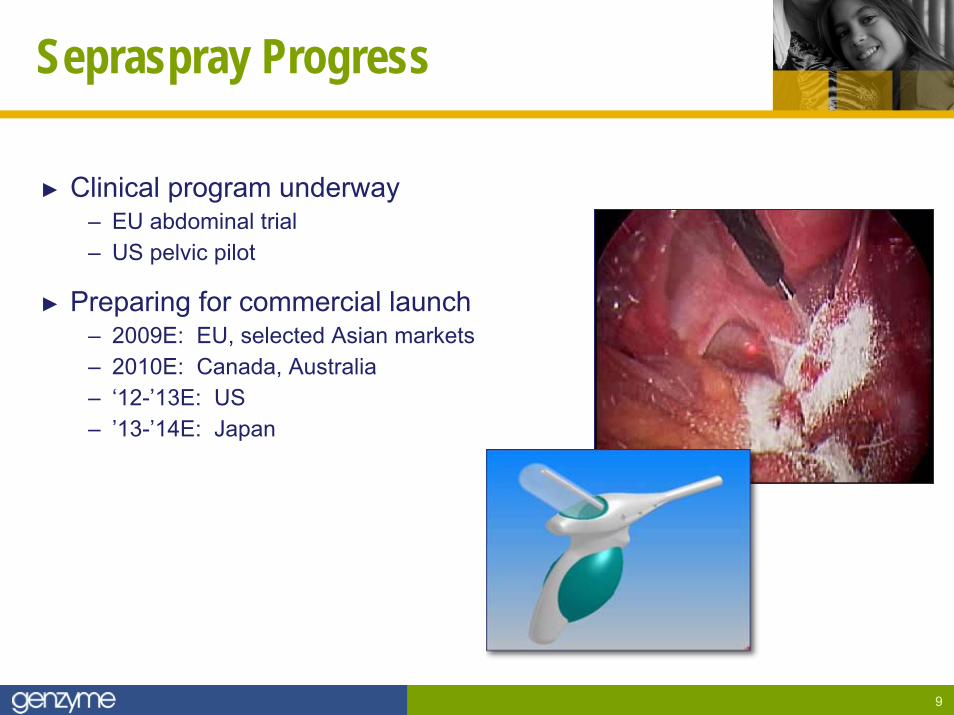
Sepraspray Progress
► Clinical program underway– EU abdominal trial – US pelvic pilot
► Preparing for commercial launch– 2009E: EU, selected Asian markets– 2010E: Canada, Australia– ‘12-’13E: US– ’13-’14E: Japan

10
Seprafilm Global Markets: Early Stagesof Geographic Penetration
Major Markets
11
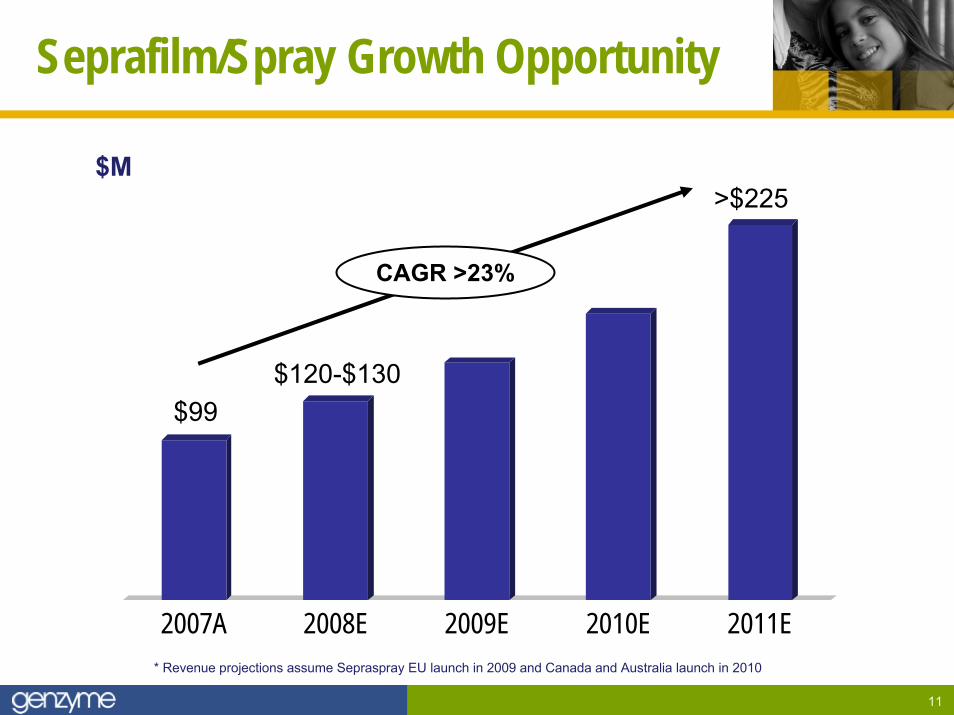
Seprafilm/Spray Growth Opportunity
2007A 2008E 2009E 2010E 2011E
$99$120-$130
>$225
CAGR >23%
* Revenue projections assume Sepraspray EU launch in 2009 and Canada and Australia launch in 2010
$M
12
Agenda
► Sepra family
► Synvisc and Synvisc-One
► Growth opportunities beyond 2011

13
Synvisc Growth Drivers
► Expanding patient types and repeat usage
► Robust competitive positioning
► Expanding consumer program
► Stabilizing US pricing and share– 3 – 4% ASP increase
effective April 1, 2008
► Synvisc Japan launch: 2010E
► Synvisc-One launches:– 2008E: EU, Canada, Australia– 2009E: US– 2012E: Japan
Growth
14
1215
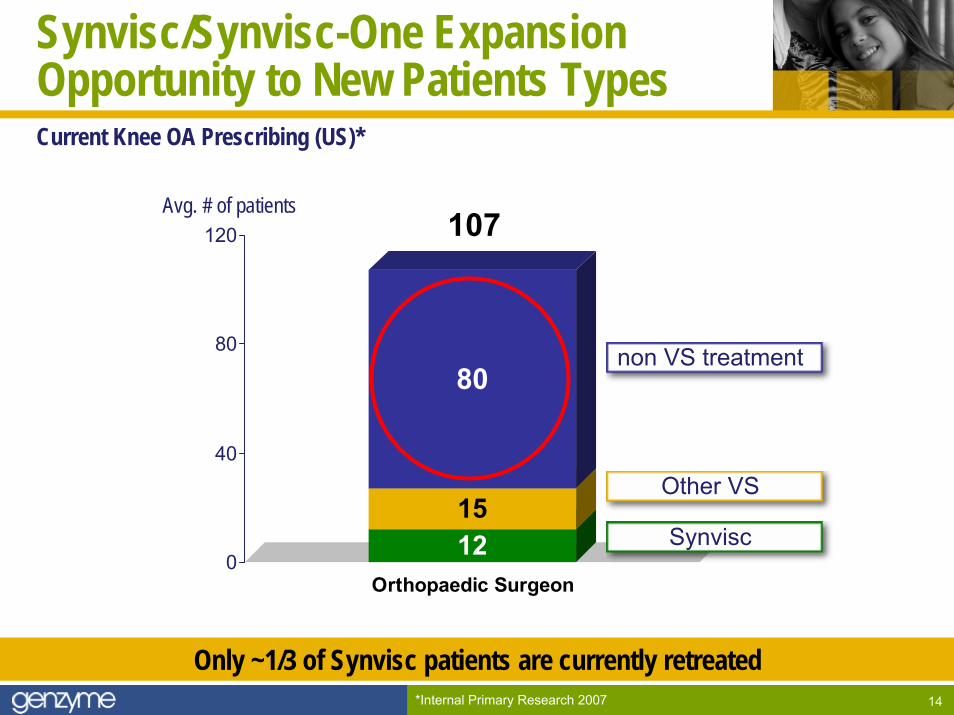
80
0
40
80
120
Orthopaedic Surgeon
107
Synvisc
Other VS
non VS treatment
Avg. # of patients
Synvisc/Synvisc-One Expansion Opportunity to New Patients TypesCurrent Knee OA Prescribing (US)*
*Internal Primary Research 2007
Only ~1/3 of Synvisc patients are currently retreated
15
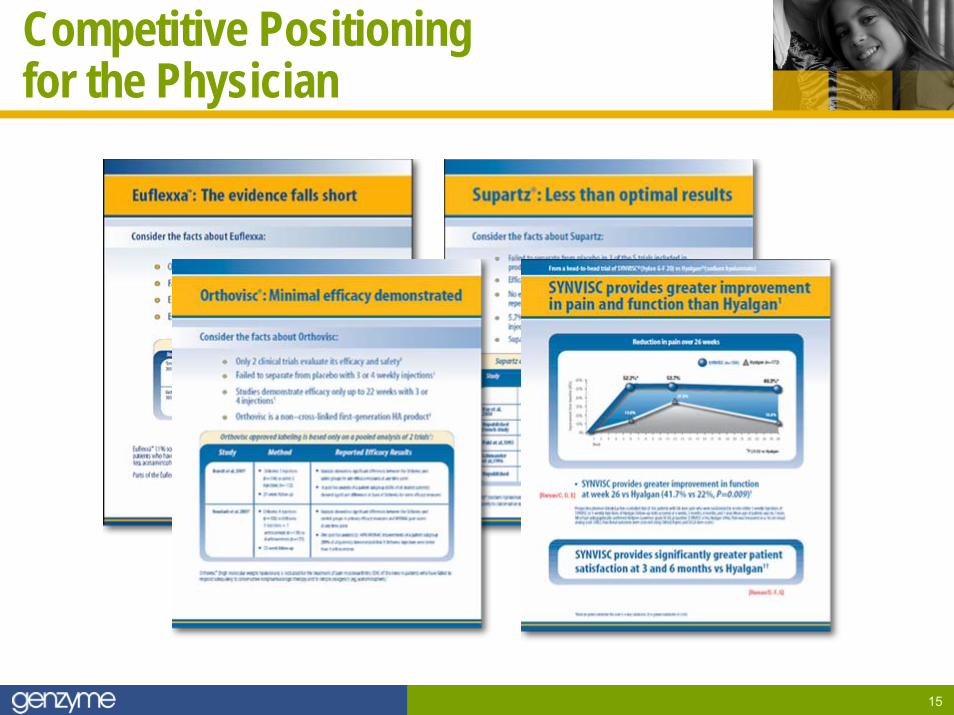
Competitive Positioning for the Physician
16
Synvisc and Managed CareEmerging Opportunities
► Select insurers are creating preferred product arrangements in the viscosupplementation class
► Genzyme has begun to secure “one-of-two” positioning. Examples: – Precision Rx / Wellpoint Affiliates (January 2008)– Rx Solutions / Pacificare (October 2007)
► As the number one product in the class, Synvisc is usually selected
17
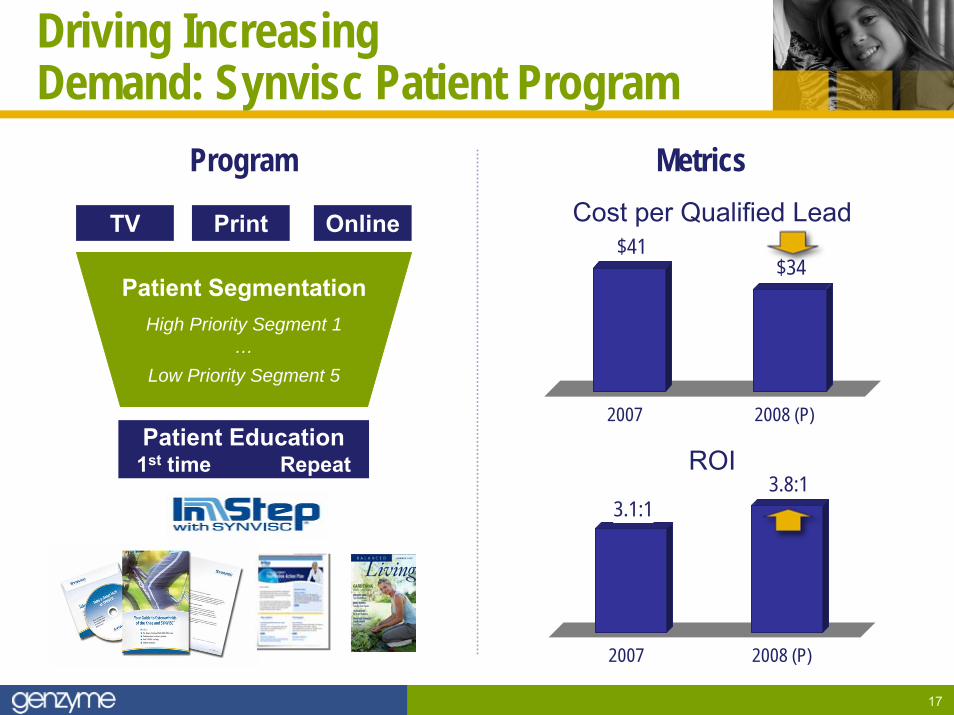
Driving Increasing Demand: Synvisc Patient Program
TV Print Online
Patient SegmentationHigh Priority Segment 1
…Low Priority Segment 5
Patient Education1st time Repeat
Cost per Qualified Lead
ROI
Program Metrics
$41$34
2007 2008 (P)
3.1:13.8:1
2007 2008 (P)
18
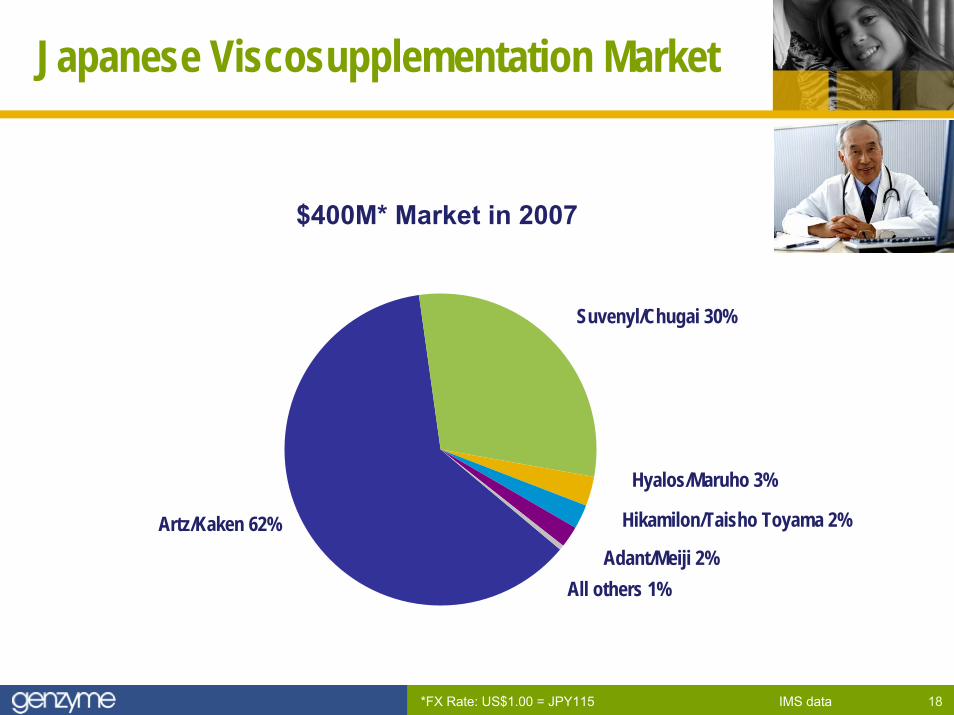
Japanese Viscosupplementation Market
$400M* Market in 2007
IMS data*FX Rate: US$1.00 = JPY115
Artz/Kaken 62%
All others 1%Adant/Meiji 2%
Hikamilon/Taisho Toyama 2%
Hyalos/Maruho 3%
Suvenyl/Chugai 30%
19
Synvisc–One FDA Status
► Submitted PMA supplement in June 2007
► Received deficiency letter from FDA in November 2007
► Genzyme asked to meet with FDA to discuss the issues identified
► Submitted response on key issue and requested a meeting with FDA in March 2008
► Meet with FDA to discuss key deficiency in April 2008
► Anticipated timeline – Submit full response to deficiency letter: June 2008E– FDA action: December 2008E
20
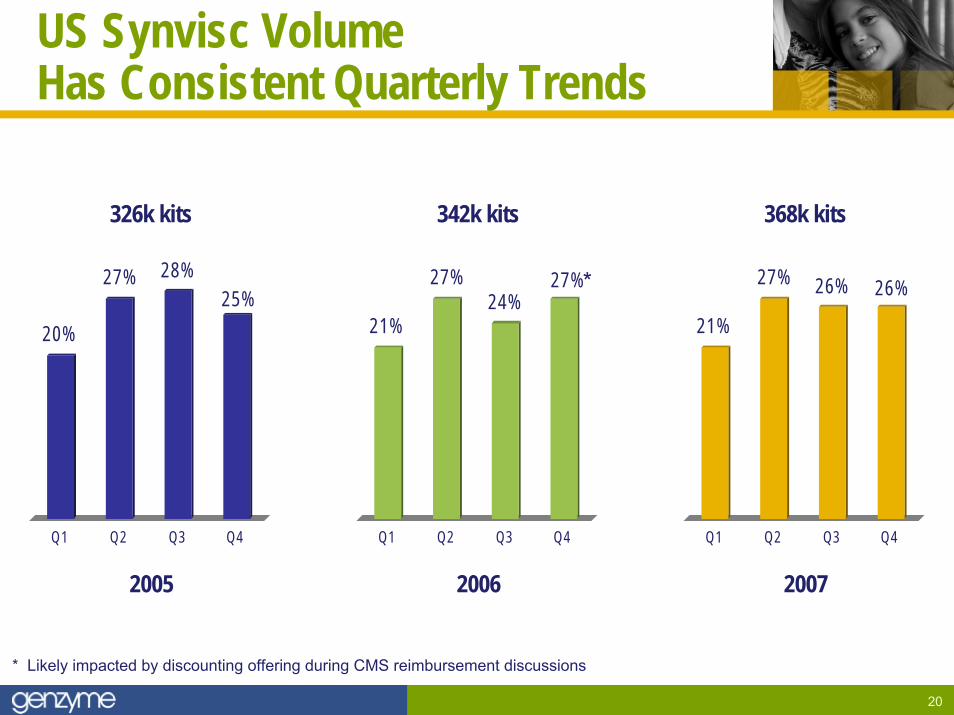
US Synvisc Volume Has Consistent Quarterly Trends
* Likely impacted by discounting offering during CMS reimbursement discussions
326k kits
20%
27% 28%25%
Q1 Q2 Q3 Q4
342k kits
21%
27%24%
27%
Q1 Q2 Q3 Q4
368k kits
21%
27% 26% 26%
Q1 Q2 Q3 Q4
20072005 2006
*
21
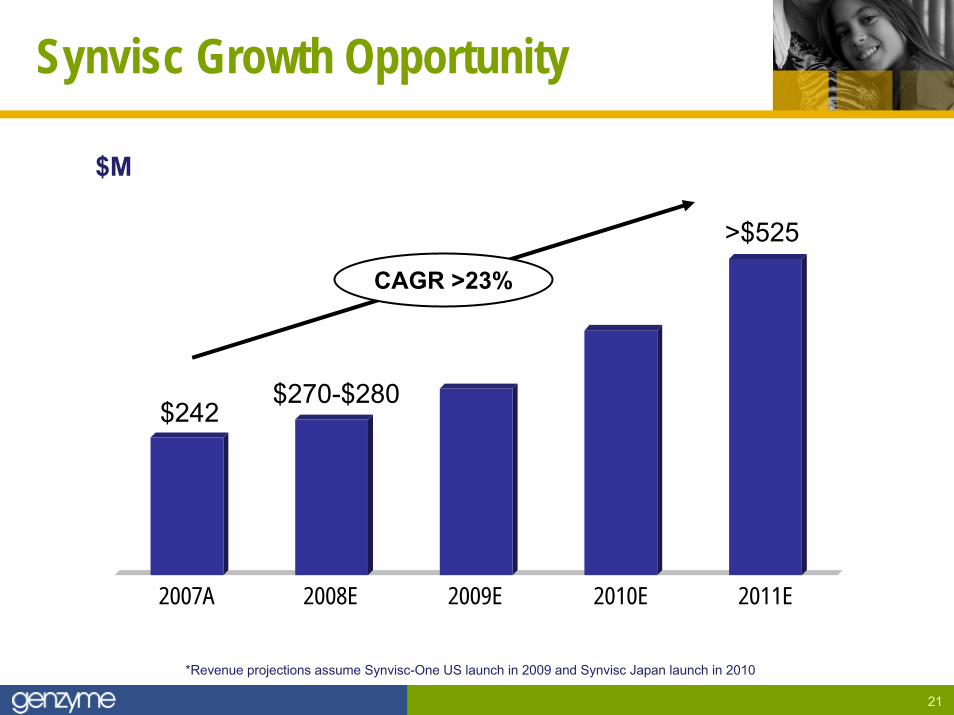
Synvisc Growth Opportunity
2007A 2008E 2009E 2010E 2011E
$242$270-$280
>$525
CAGR >23%
*Revenue projections assume Synvisc-One US launch in 2009 and Synvisc Japan launch in 2010
$M
22
Agenda
► Sepra family
► Synvisc and Synvisc-One
► Growth opportunities beyond 2011

23
Growth Drivers Beyond 2011
► Synvisc-One and Sepraspray
► Expanding Synvisc US label to other joint(s)
► OA combination products (drugs)– Gen-S for enhanced OA pain relief
(into clinic H1 ’09)– Further opportunities: pain and structure
► New adhesion prevention indications (ortho, spine, cardiac)
► MACI EU, US, China
► Business development
Growth

24
S U M M A R Y:
Strong Foundation for Growth
Sepra ► Procedure diversification
for film
► Sepraspray for laparoscopic
► Ex-US opportunities
► New indications beyond 2011
Synvisc / Synvisc-One► Expanding patient types
and repeat usage
► Synvisc-One
► Synvisc Japan
► Combination products beyond 2011
Growth Drivers
+
Alemtuzumab in MS: A Promising New Standard of CareTerry L. Murdock, Sr. Vice President
May 7, 2008 Analyst Day
26
Agenda
► Phase 2 data
► Phase 3 program
► Market research
27
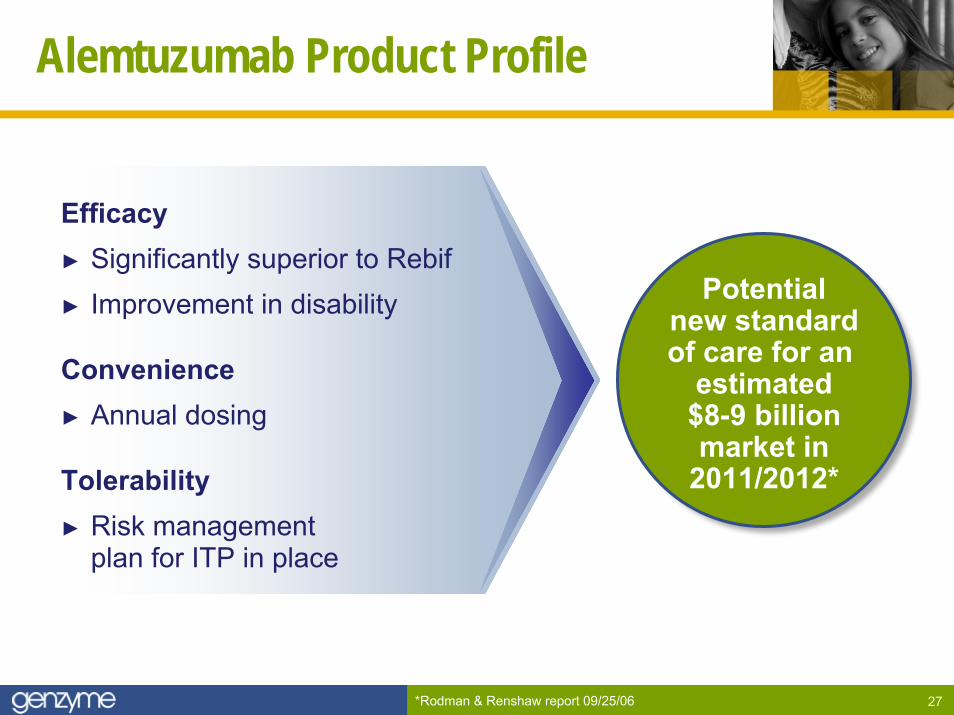
Alemtuzumab Product Profile
Potentialnew standardof care for an
estimated$8-9 billionmarket in
2011/2012*
Efficacy► Significantly superior to Rebif► Improvement in disability
Convenience► Annual dosing
Tolerability► Risk management
plan for ITP in place
*Rodman & Renshaw report 09/25/06
28
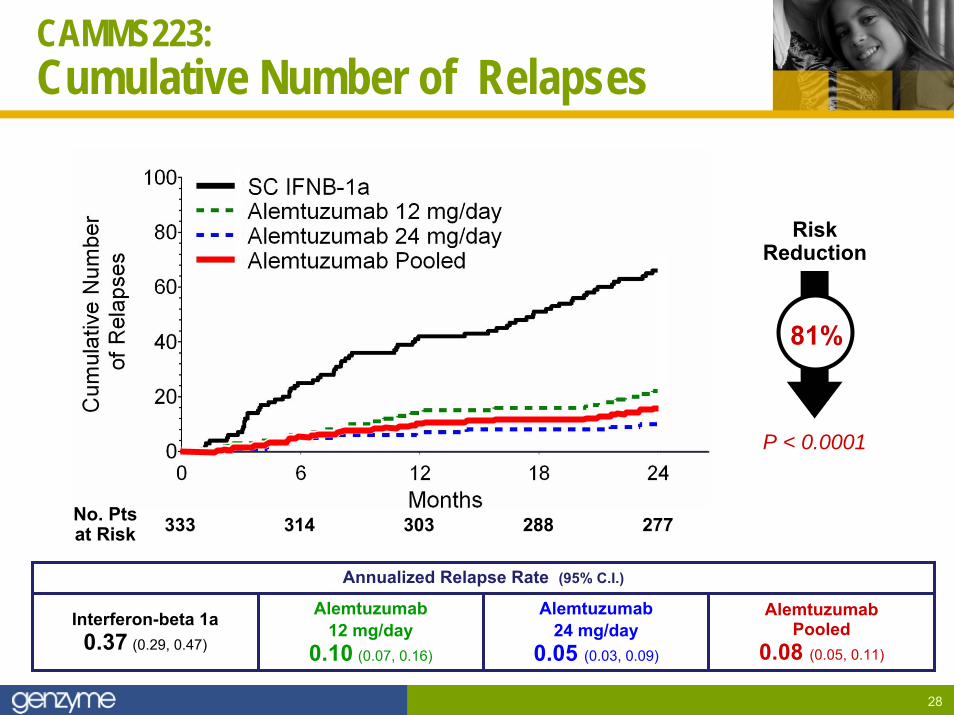
CAMMS223:Cumulative Number of Relapses
Annualized Relapse Rate (95% C.I.)
Interferon-beta 1a0.37 (0.29, 0.47)
Alemtuzumab 12 mg/day
0.10 (0.07, 0.16)
Alemtuzumab 24 mg/day
0.05 (0.03, 0.09)
AlemtuzumabPooled
0.08 (0.05, 0.11)
333 314 303 288 277No. Ptsat Risk
P < 0.0001
RiskReduction
81%
29
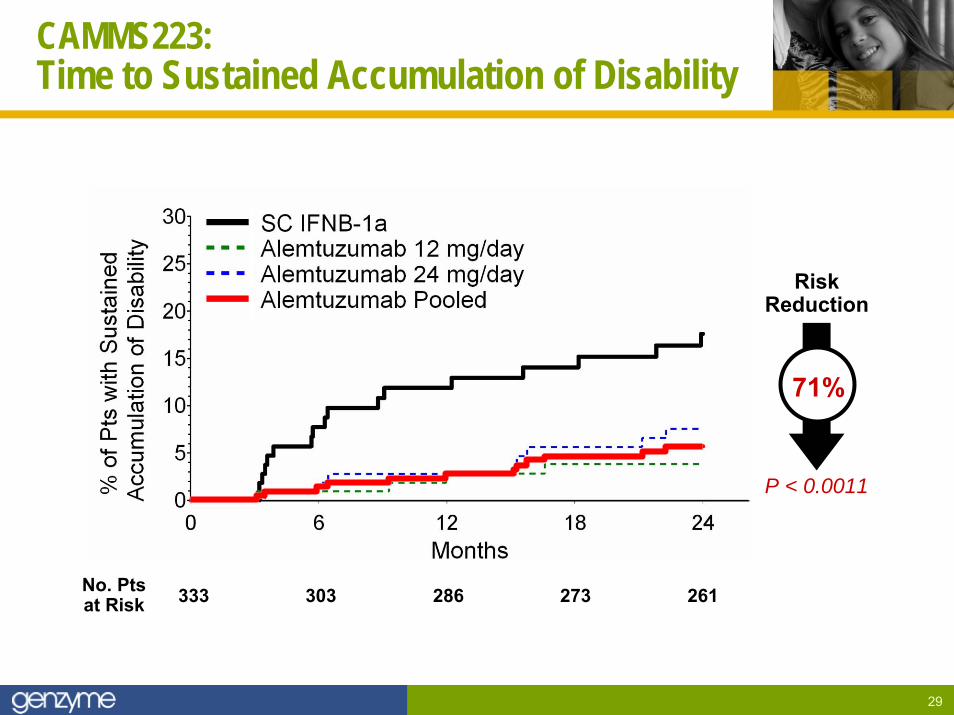
CAMMS223:Time to Sustained Accumulation of Disability
333 303 286 273 261No. Ptsat Risk
P < 0.0011
RiskReduction
71%
30
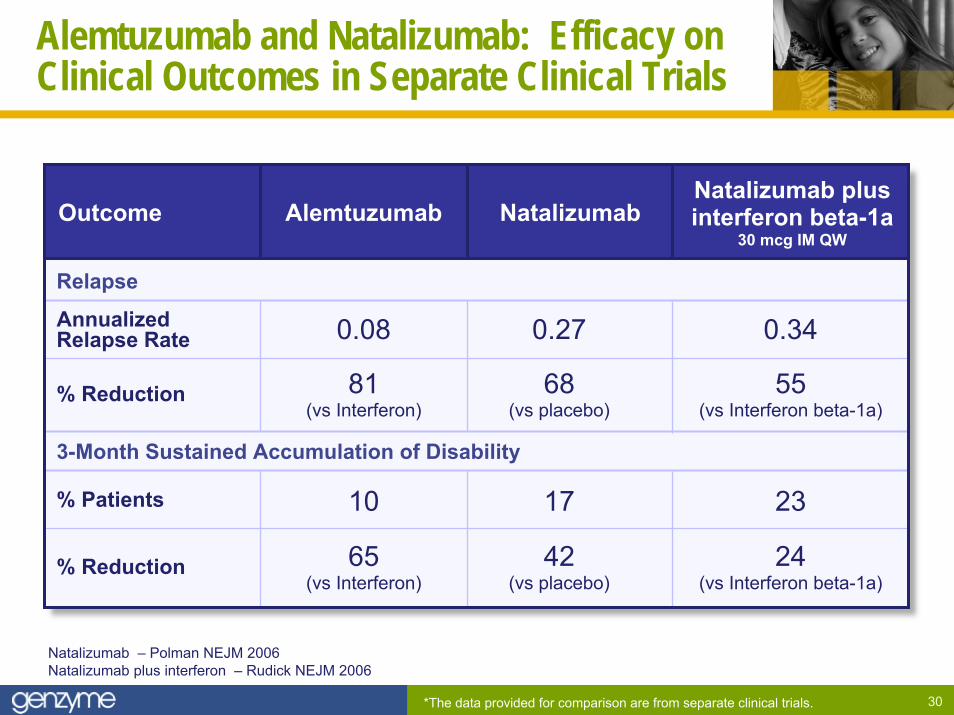
Alemtuzumab and Natalizumab: Efficacy onClinical Outcomes in Separate Clinical Trials
AlemtuzumabOutcome NatalizumabNatalizumab plusinterferon beta-1a
30 mcg IM QW
3-Month Sustained Accumulation of Disability
Relapse
% Reduction
% Patients
% Reduction
AnnualizedRelapse Rate
24(vs Interferon beta-1a)
42(vs placebo)
65(vs Interferon)
231710
55(vs Interferon beta-1a)
68(vs placebo)
81(vs Interferon)
0.340.270.08
Natalizumab – Polman NEJM 2006Natalizumab plus interferon – Rudick NEJM 2006
*The data provided for comparison are from separate clinical trials.
31
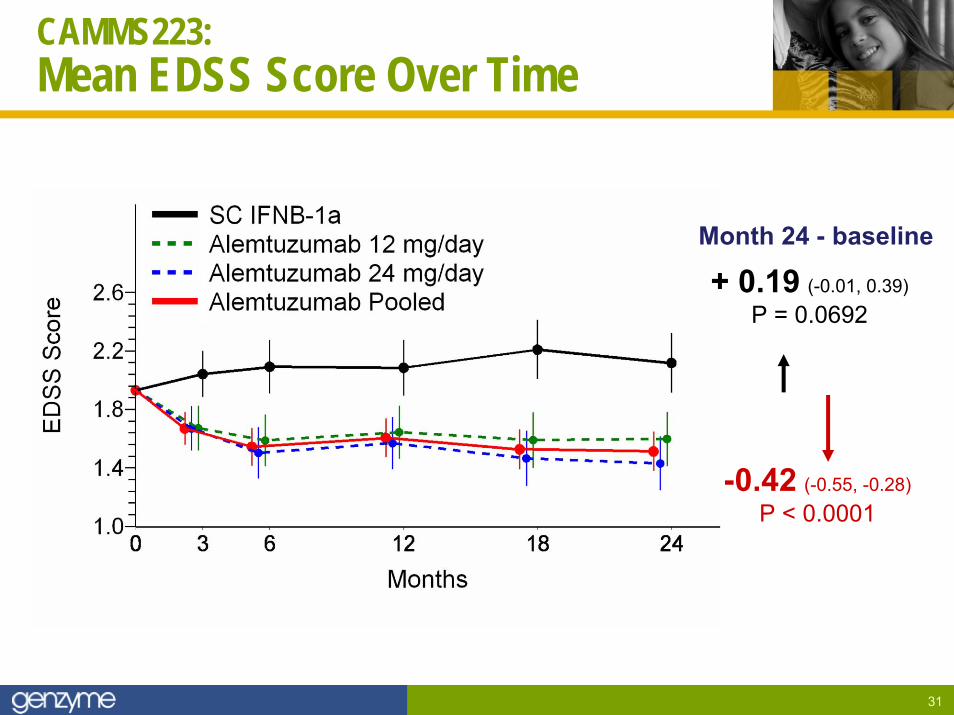
CAMMS223: Mean EDSS Score Over Time
+ 0.19 (-0.01, 0.39)P = 0.0692
Month 24 - baseline
-0.42 (-0.55, -0.28)P < 0.0001
32
Strong 3-Year Results
► Three-year results presented at AAN 2008 confirm and extend conclusions from the interim analyses at 1- and 2-years:
– Markedly reduced the risk of relapse versus IFNB-1a (statistically significant)– Markedly reduced the risk for SAD versus IFNB-1a (statistically significant)
► Significant improvements observed on MRI– Markedly reduced T2 lesion load (statistically significant)– Increase in brain volume v. atrophy with INFB-1a (statistically significant)
► No new cases of ITP since September of 2006

33
Agenda
► Phase 2 data
► Phase 3 program
► Market research

34
Phase 3 Program
Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis
35
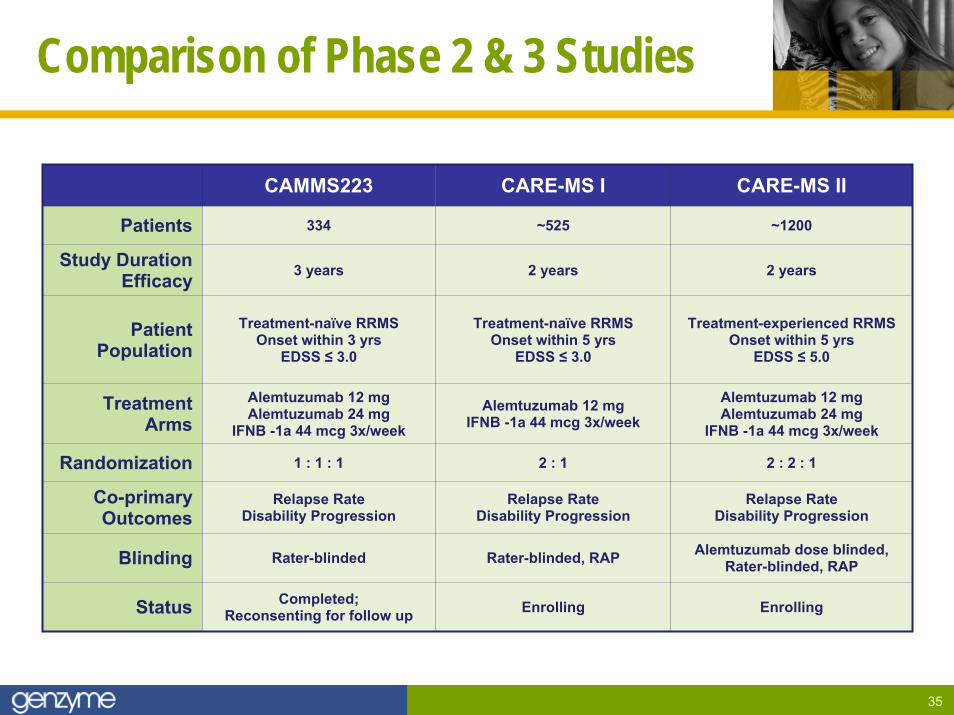
Comparison of Phase 2 & 3 Studies
CAMMS223 CARE-MS I CARE-MS II
Patients 334 ~525 ~1200
2 years 2 years
Treatment-naïve RRMSOnset within 5 yrs
EDSS ≤ 3.0
Treatment-experienced RRMSOnset within 5 yrs
EDSS ≤ 5.0
Alemtuzumab 12 mgIFNB -1a 44 mcg 3x/week
Alemtuzumab 12 mgAlemtuzumab 24 mg
IFNB -1a 44 mcg 3x/week
Randomization 1 : 1 : 1 2 : 1 2 : 2 : 1
Blinding Rater-blinded Rater-blinded, RAP Alemtuzumab dose blinded,Rater-blinded, RAP
Relapse RateDisability Progression
Relapse RateDisability Progression
Enrolling Enrolling
Study Duration Efficacy 3 years
Patient Population
Treatment-naïve RRMSOnset within 3 yrs
EDSS ≤ 3.0
TreatmentArms
Alemtuzumab 12 mgAlemtuzumab 24 mg
IFNB -1a 44 mcg 3x/week
Co-primary Outcomes
Relapse RateDisability Progression
Status Completed;Reconsenting for follow up
36
Safety Monitoring Plan
► Hematologic monitoring– Monthly (or more frequent) complete blood counts (CBCs) with platelets– Monthly phone calls from sites to patients
• Offset from CBCs by 2 weeks– At least 3 years of follow-up after last alemtuzumab treatment
► Patient and physician education about ITP
► Monitoring for thyroid disorders
37
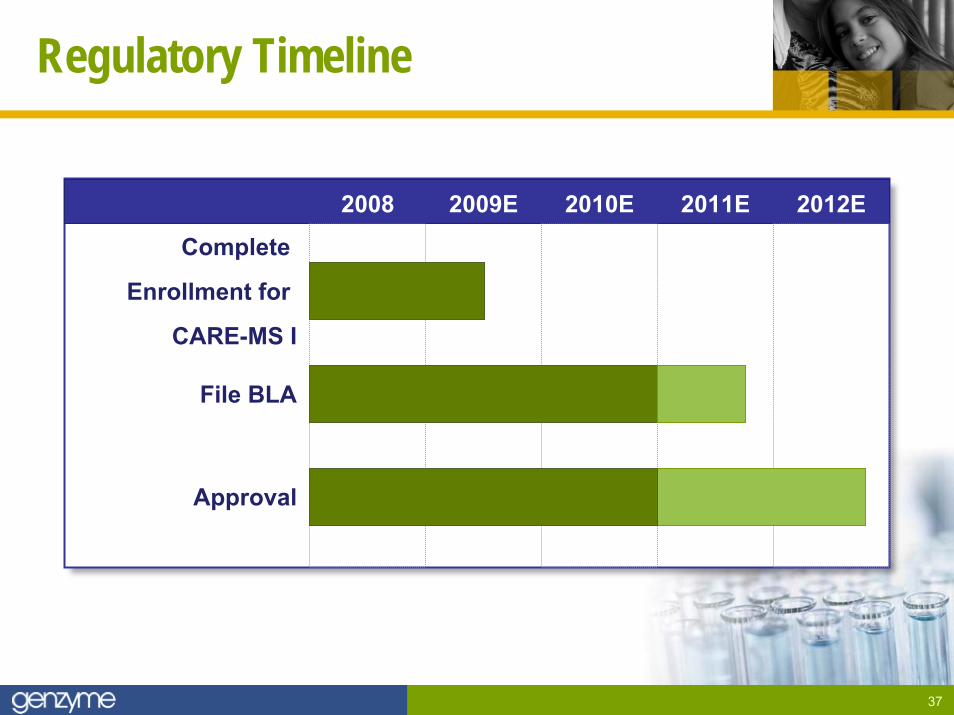
Regulatory Timeline
2008 2009E 2010E 2011E 2012E
Complete
Enrollment for
CARE-MS I
File BLA
Approval

38
Agenda
► Phase 2 data
► Phase 3 program
► Market research
39
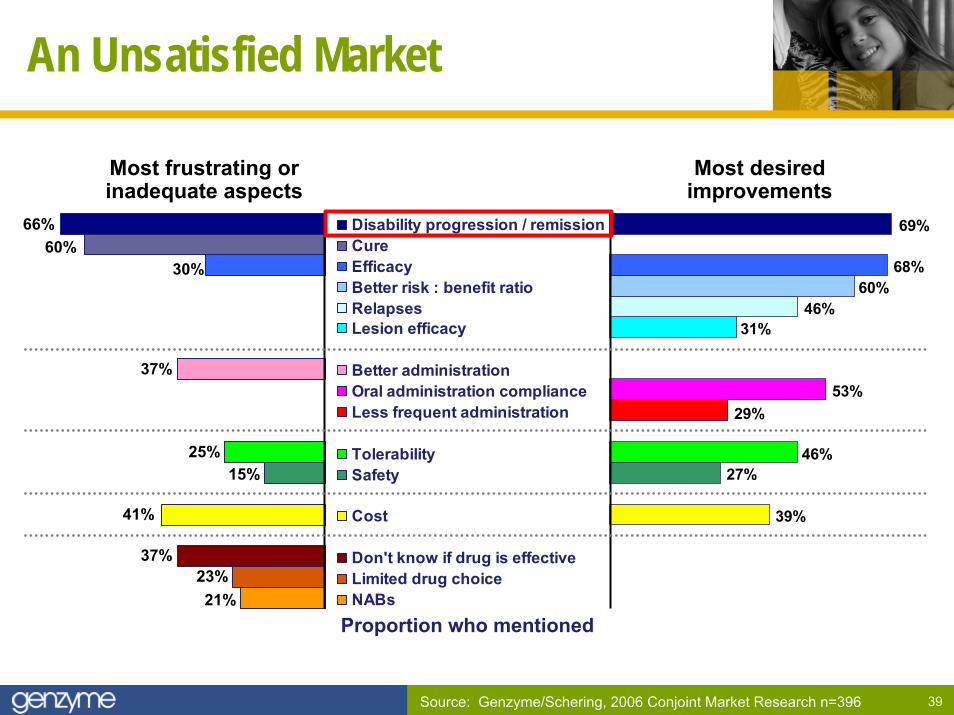
An Unsatisfied Market
Most frustrating orinadequate aspects
Most desiredimprovements
Source: Genzyme/Schering, 2006 Conjoint Market Research n=396
Disability progression / remissionCureEfficacyBetter risk : benefit ratioRelapsesLesion efficacyBar 13Better administrationOral administration complianceLess frequent administrationBar 9TolerabilitySafetyBar 6CostBar 4Don't know if drug is effectiveLimited drug choiceNABs
39%
27%46%
29%53%
31%46%
60%68%
69%66%60%
30%
37%
25%15%
41%
37%23%21%
Proportion who mentioned
40
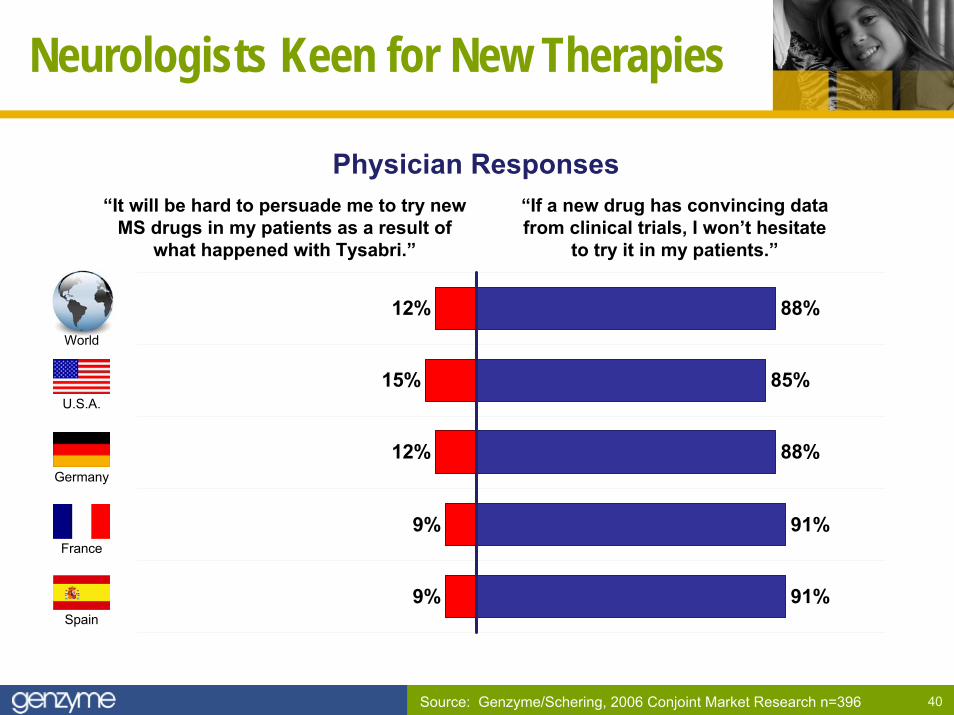
Neurologists Keen for New Therapies
91%
91%
88%
85%
88%
9%
9%
12%
15%
12%
“If a new drug has convincing data from clinical trials, I won’t hesitate
to try it in my patients.”
“It will be hard to persuade me to try new MS drugs in my patients as a result of
what happened with Tysabri.”
Physician Responses
Source: Genzyme/Schering, 2006 Conjoint Market Research n=396
World
U.S.A.
Germany
France
Spain
41
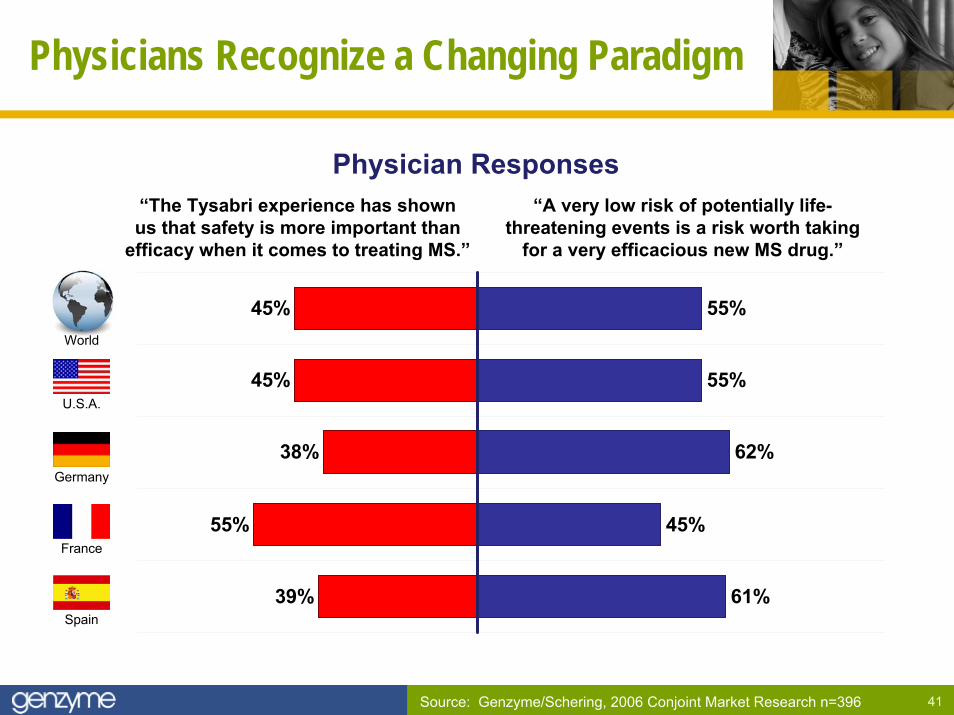
Physicians Recognize a Changing Paradigm
61%
45%
62%
55%
55%
39%
55%
38%
45%
45%
“A very low risk of potentially life-threatening events is a risk worth taking
for a very efficacious new MS drug.”
“The Tysabri experience has shownus that safety is more important than
efficacy when it comes to treating MS.”
Physician Responses
Source: Genzyme/Schering, 2006 Conjoint Market Research n=396
World
U.S.A.
Germany
France
Spain
42
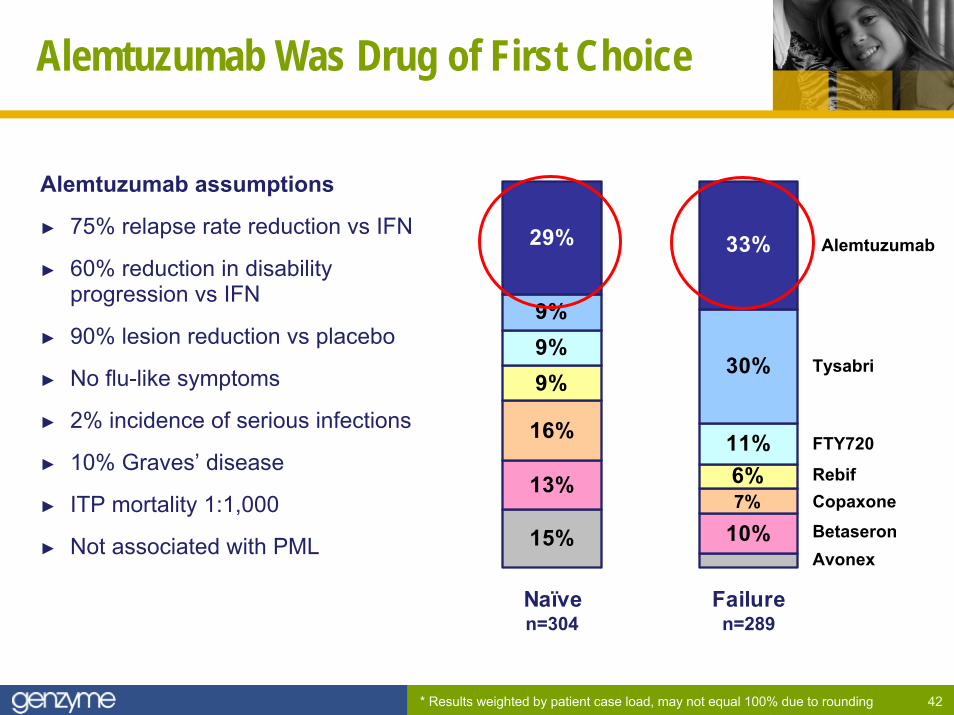
Alemtuzumab Was Drug of First Choice
Alemtuzumab assumptions
► 75% relapse rate reduction vs IFN
► 60% reduction in disability progression vs IFN
► 90% lesion reduction vs placebo
► No flu-like symptoms
► 2% incidence of serious infections
► 10% Graves’ disease
► ITP mortality 1:1,000
► Not associated with PML
* Results weighted by patient case load, may not equal 100% due to rounding
n=289n=304
13%
10%
16%
9%
6%
9%
11%
30%
29% 33%
15%7%
9%
Naïve Failure
Alemtuzumab
Tysabri
FTY720
RebifCopaxoneBetaseronAvonex
43
Research Confirmed and Extended
► 20 in-depth interviews with community-based neurologists
► Board certified in neurology
► See at least 30 MS patients monthly
► Physicians provided alemtuzumab interim Phase 2 data and Phase 3 MS trial designs to review prior to the interview
44
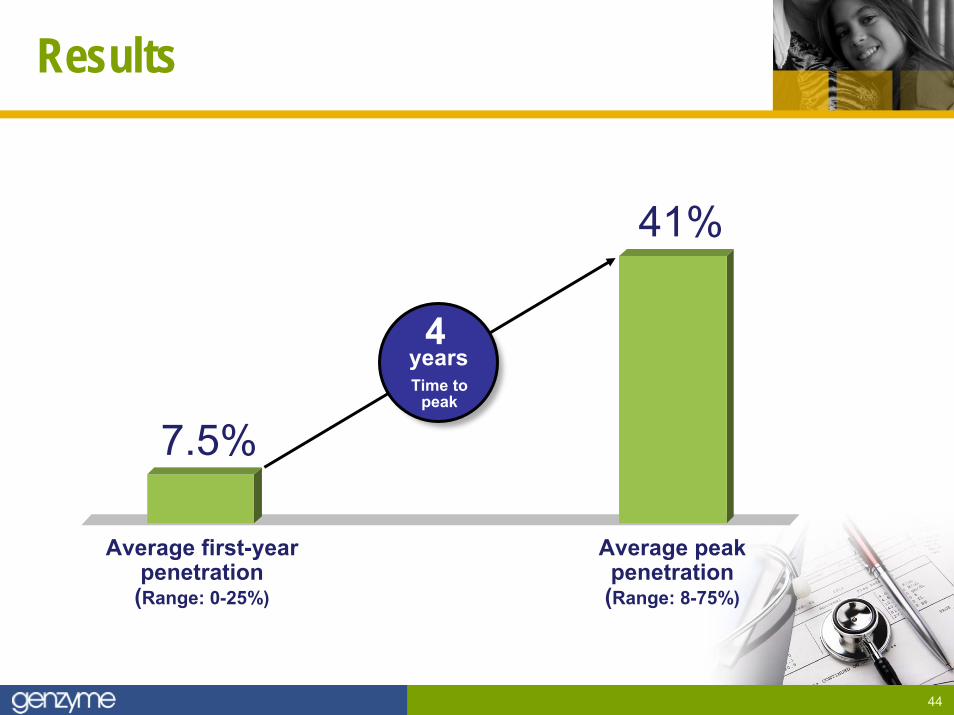
Results
Average first-yearpenetration(Range: 0-25%)
Average peakpenetration(Range: 8-75%)
7.5%
41%
4yearsTime to
peak
45
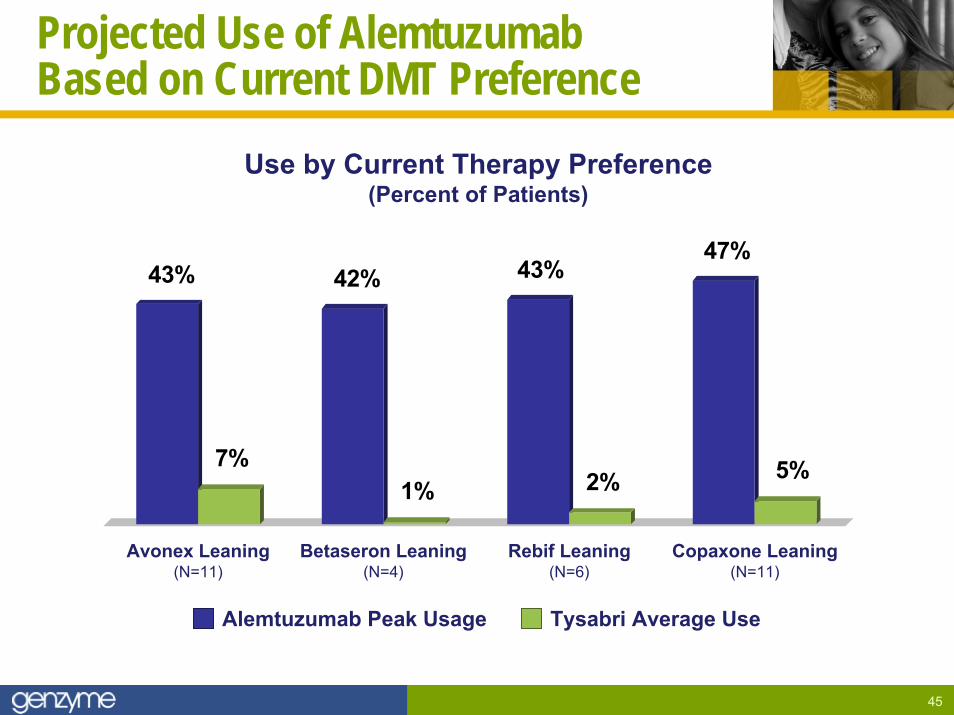
Projected Use of Alemtuzumab Based on Current DMT Preference
Use by Current Therapy Preference(Percent of Patients)
43%
7%
42%
1%
43%
2%
47%
5%
Avonex Leaning(N=11)
Betaseron Leaning(N=4)
Rebif Leaning(N=6)
Copaxone Leaning(N=11)
Alemtuzumab Peak Usage Tysabri Average Use

46
S U M M A R Y:
A Promising New Standard of Care
► Significant efficacy and manageable safety profile in comparison to Rebif
► Pivotal trials are on-track for BLA filing in 2011E
► Potential revenue beginning in 2011/2012

Mipomersen: An Attractive New OpportunityJames A. Geraghty, Senior Vice President
May 7, 2008 Analyst Day
48
Agenda
► Hypercholesterolemia: unmet needs
► Introduction to Mipomersen
► Responses to investor questions
Cholesterol
49
Profile of Homozygous FH Patients (HoFH)
► Extremely high LDL levels
► Unable to be controlled on optimal current therapy
► Coronary events common in childhood/adolescence
► Regular apheresis recommended
The need for a new therapy is clear
50
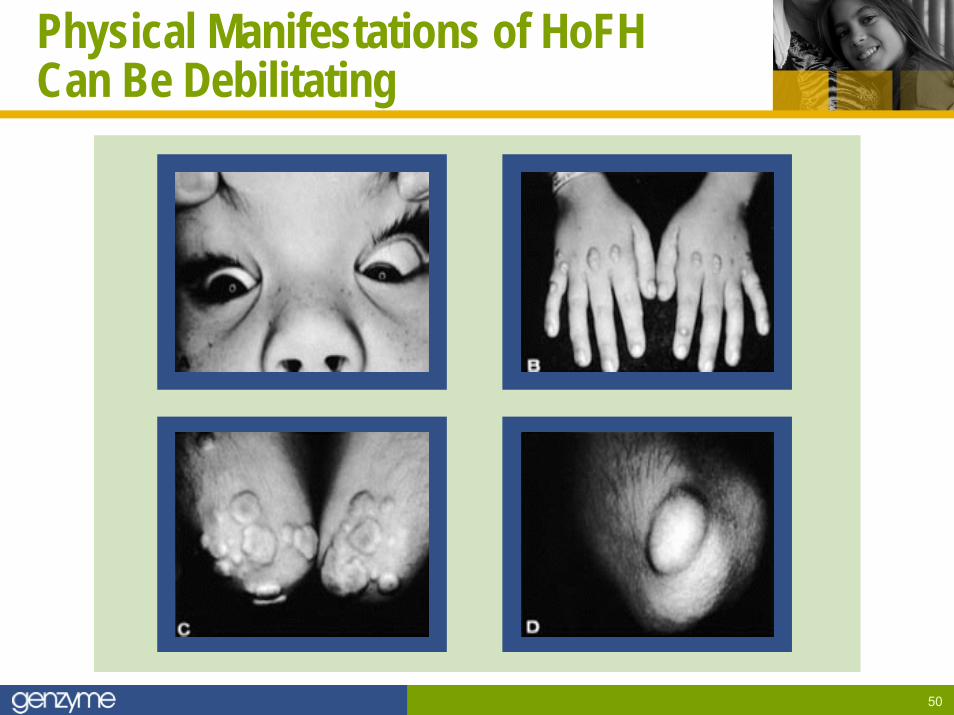
Physical Manifestations of HoFHCan Be Debilitating
51
Other High-Risk Patients:Achieving LDL Goals is Key to Avoiding Events
► High risk patients have >20% 10 year CVD risk
► Some are highly statinintolerant/resistant
► Highest risk groups have up to 30% >5 year CVD risk
Many cannot get to goal on optimal current therapy
52
Agenda
► Hypercholesterolemia: unmet needs
► Introduction to Mipomersen
► Responses to investor questions
Cholesterol
53
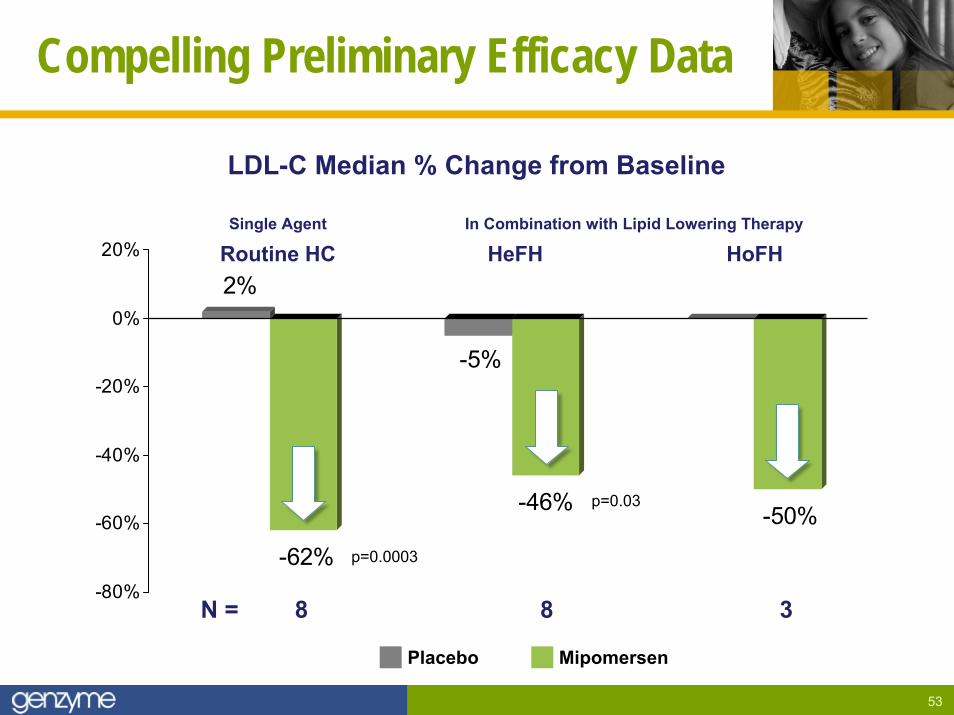
Compelling Preliminary Efficacy Data
LDL-C Median % Change from Baseline
2%
-62%
-5%
-46% -50%
-80%
-60%
-40%
-20%
0%
20%
p=0.0003
p=0.03
N = 8 8 3
Single Agent
Routine HCIn Combination with Lipid Lowering Therapy
HeFH HoFH
Placebo Mipomersen
54
Limited Adverse Events Reported
► Injection site reaction– Most frequently reported adverse event– Reported painless, spontaneously resolve– No worsening with long-term dosing
► Hepatic effects– ALT elevations: consistent with pharmacologic effects– Tend to decrease with continued dosing– No elevated bilirubin or Hy’s Law cases
Ensuring safety will be our highest concern
55
Clinicians Very Positive on Mipomersen
► Novel, first-in-class product
► Every physician interviewed was very excited about the product
► Lipid specialists see clear need in high risk populations
► All see value in FH and high risk patients not at goal
► Potential benefit for apheresis eligible patients extremely high
Positivephysicianresponse
56
Agenda
► Hypercholesterolemia: unmet needs
► Introduction to Mipomersen
► Responses to investor questions
Cholesterol
57
Investor Questions
1. How do you define each patient population?
2. What are the development plans for the HoFH population?
3. What are the plans for the apheresis eligible population?
4. What would be the design of the clinical outcome study?
5. What is the timing for the expected filings?
58
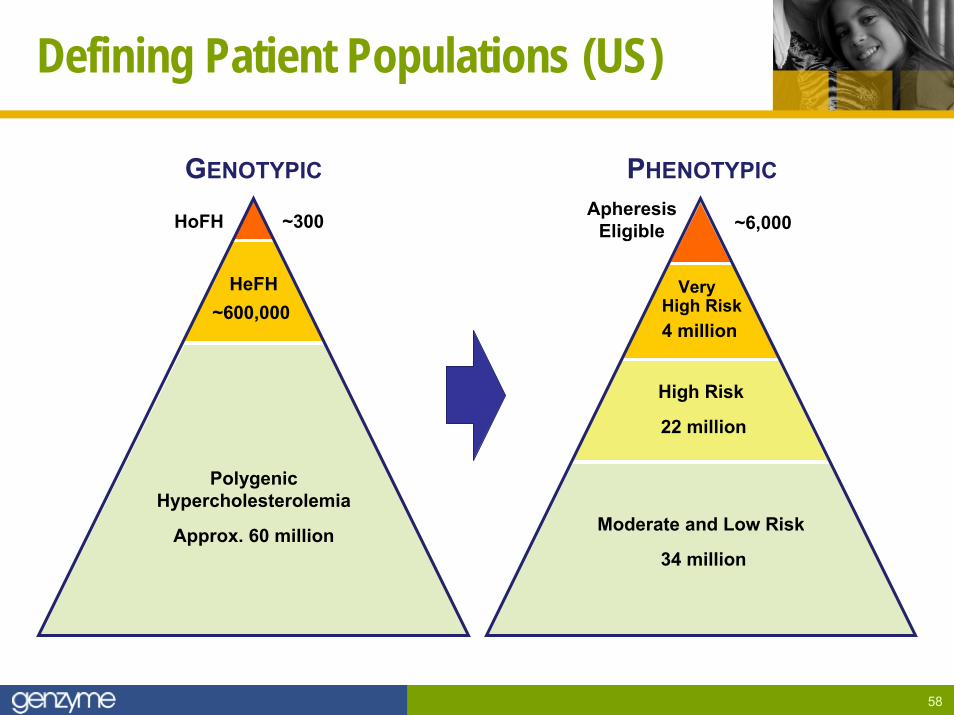
Defining Patient Populations (US)
HoFH
PolygenicHypercholesterolemia
Approx. 60 million
HeFH~600,000
GENOTYPIC
~300 ApheresisEligible
High Risk
22 million
Moderate and Low Risk
34 million
Very High Risk4 million
PHENOTYPIC
~6,000
59
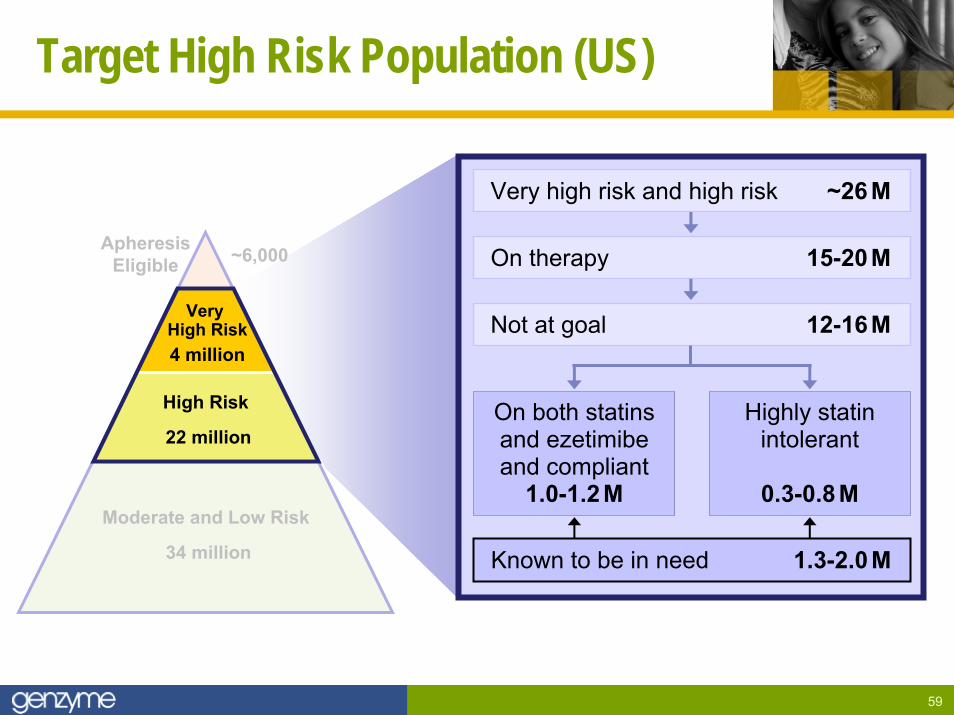
Target High Risk Population (US)
ApheresisEligible
High Risk
22 million
Moderate and Low Risk
34 million
Very High Risk4 million
~6,000
On both statinsand ezetimibeand compliant
1.0-1.2M
Highly statinintolerant
0.3-0.8M
Very high risk and high risk ~26 M
On therapy 15-20M
Known to be in need 1.3-2.0M
Not at goal 12-16M
60
Investor Questions
1. How do you define each patient population?
2. What are the development plans for the HoFH population?
3. What are the plans for the apheresis eligible population?
4. What would be the design of the clinical outcome study?
5. What is the timing for the expected filings?
61
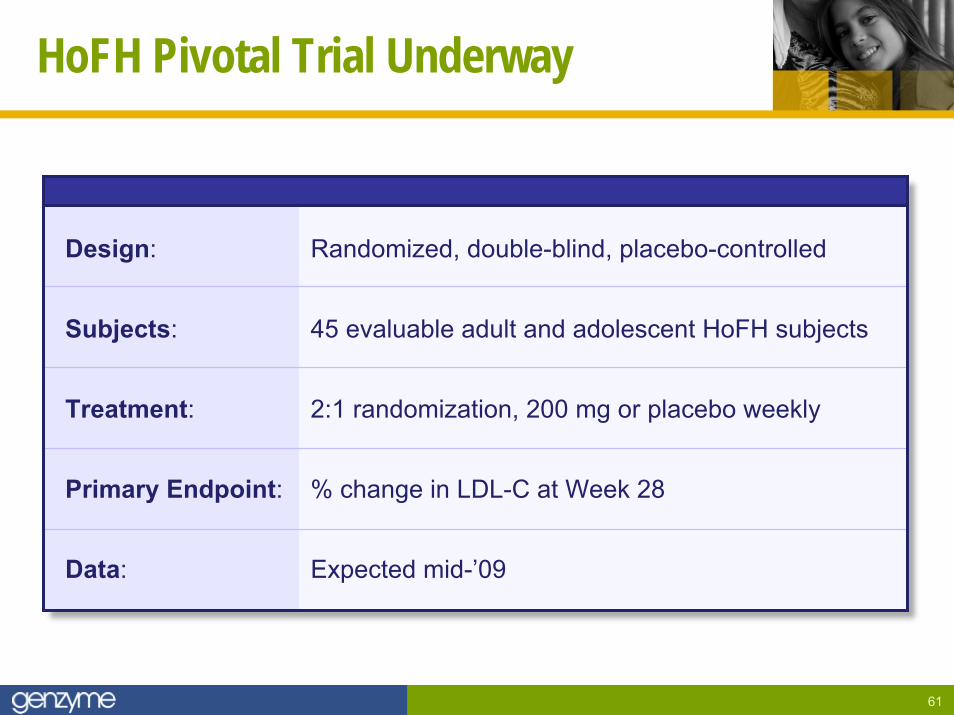
HoFH Pivotal Trial Underway
Design: Randomized, double-blind, placebo-controlled
Subjects: 45 evaluable adult and adolescent HoFH subjects
Treatment: 2:1 randomization, 200 mg or placebo weekly
Primary Endpoint: % change in LDL-C at Week 28
Data: Expected mid-’09
62
Investor Questions
1. How do you define each patient population?
2. What are the development plans for the HoFH population?
3. What are the plans for the apheresis eligible population?
4. What would be the design of the clinical outcome study?
5. What is the timing for the expected filings?
63
Apheresis Eligible Patients
► Like HoFH, defined primarily by very high LDL levels
► LDL apheresis very expensive and uncomfortable
► Rapid LDL rebound limits therapeutic value
► Estimated 10-15,000 eligible in US and Europe
► Very few eligible patients remain on therapy
► Annual costs range from $75,000-$150,000 per year
64
Preliminary Apheresis Trial Plans
► Eligible patients not currently on apheresis
► All patients kept on optimal current therapy
► Randomized 2:1 mipomersen to placebo
► Approximately 60 patients with 6 months of treatment
► Goal is to have data at time of the HoFH filing
65
Investor Questions
1. How do you define each patient population?
2. What are the development plans for the HoFH population?
3. What are the plans for the apheresis eligible population?
4. What would be the design of the clinical outcome study?
5. What is the timing for the expected filings?
66
Emerging Clinical Outcome Study Plans
► Goal is to start and finish as soon as possible
► Focus on highest risk, highest event rate groups
► Includes patients with CVD, diabetes, very high LDL levels
► Assumptions being drawn from many prior large LDL reduction studies
► Working target is to begin enrollment in H1:09E
► Details to be finalized in coming months
67
Investor Questions
1. How do you define each patient population?
2. What are the development plans for the HoFH population?
3. What are the plans for the apheresis eligible population?
4. What would be the design of the clinical outcome study?
5. What is the timing for the expected filings?
68
Preliminary Regulatory Plans
US► Targeting HoFH filing by H2:10E
► Broader high risk filing date not yet finalized
► Will discuss pathway forward for apheresis eligible patients with the FDA
EUROPE► Authorities have taken a different view on similar products
► May also look at mipomersen very differently
► Beginning active dialogue on product and plans
► Will seek opportunities for earlier intermediate filings
69
S U M M A R Y:
Significant Near Term Opportunity
► HoFH and apheresis-eligible patients have high unmet needs
► Mipomersen may represent an alternative to apheresis
► Physicians are eager for mipomersen in multiple segments
► Genzyme has a long experience with similar products
70
Question and Answer
Moderator:
► Duke Collier, Esquire, Executive Vice President
Panel:
► Joe Lobacki, Sr. Vice President and General Manager, Transplant
► Terry Murdock, Sr. Vice President and General Manger, Campath
► Jim Geraghty, Sr. Vice President
► Michael Wyzga, Executive Vice President, Chief Financial and Accounting Officer

Concluding Comments
Henri Termeer, Chairman, CEO, President
May 7, 2008 Analyst Day
72
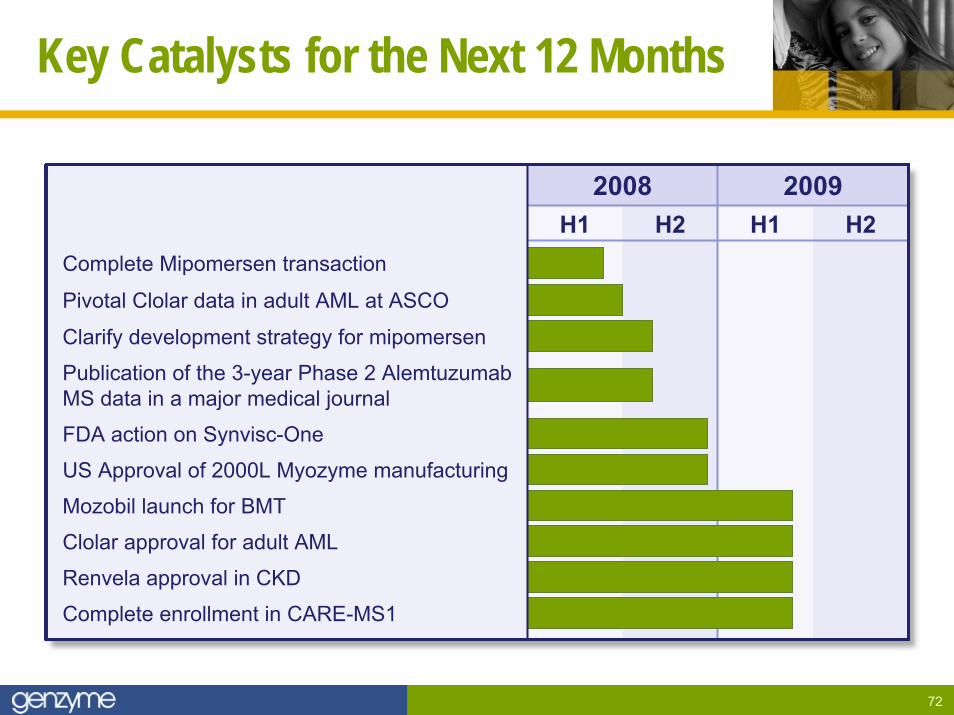
Key Catalysts for the Next 12 Months
H1 H2 H1 H22008 2009
Complete Mipomersen transaction
Pivotal Clolar data in adult AML at ASCO
Clarify development strategy for mipomersen
Publication of the 3-year Phase 2 AlemtuzumabMS data in a major medical journal
FDA action on Synvisc-One
US Approval of 2000L Myozyme manufacturing
Mozobil launch for BMT
Clolar approval for adult AML
Renvela approval in CKD
Complete enrollment in CARE-MS1