Embed Size (px)
Citation preview

Biosimilars Switching: What is Left to Learn? Jonathan Kay, MD
Professor of MedicineTimothy S. and Elaine L. Peterson Chair in Rheumatology
UMass Memorial Medical CenterUniversity of Massachusetts Medical School
Worcester, Massachusetts

Disclosures
Research Grants (paid to the University of Massachusetts Medical School): Eli Lilly and Company; Gilead Sciences Inc.; Pfizer Inc.; UCB, Inc.
Consultant: Amgen Inc.; Boehringer Ingelheim GmbH; Celgene Corp.; CelltrionHealthcare Co. Ltd.; Janssen Biotech Inc.; Merck Sharp & Dohme Corp.; Myriad Genetics, Inc.; Pfizer Inc.; Roche Laboratories, Inc.; Samsung Bioepis; Sandoz Inc.
Overview
• Definition of biosimilars
• Current state of biosimilarsmarket
• Principles of demonstrating biosimilarity
• Definitions of interchangeability & switching: EU vs. US
• Clinical trial designs to assess biosimilar switching
• FDA draft guidance on demonstrating interchangeability
• Switching: European experience
• Nocebo effect
• Future studies

Biosimilars: Regulatory Definitions
Committee for Medicinal Products for Human Use. Guideline on similar biologic medicinal products. Draft. London: European Medicines Agency; 2013.
A biosimilar is a biologic medicinal product that contains a version of the active substance of an already authorized original biologic medicinal product (reference medicinal product). A biosimilar demonstrates
similarity to the reference medicinal product in terms of quality characteristics, biologic activity, safety, and efficacy based on a comprehensive comparability exercise.
US Food and Drug Administration. Guidance for Industry. Biosimilars: questions and answers regarding implementation of the Biologics Price Competition and Innovation Act of 2009. Department of Health & Human Services, 2015.
Biosimilarity means “that the biologic product is highly similar to the reference product notwithstandingminor differences in clinically inactive components” and that “there are no clinically meaningful
differences between the biologic product and the reference product in terms of the safety, purity, and potencyof the product”

Current State of Biosimilars Market
Class Reference Drug
# of Approved Biosimilars
European Union
United States
Canada Australia JapanSouth Korea
Erythropoiesis-stimulating agentsepoetin alfa (Eprex) 5 3 1
darbepoetin alfa (Aranesp) 1
Granulocyte-colony stimulating factor filgrastim (Neupogen) 7 1 1 3 3
Human growth hormone somatropin (Genotropin) 1 1 2 1 1
Follicle-stimulating hormone follitropin alfa (Gonal-F) 2 1
TNF Inhibitors
infliximab (Remicade) 3 3 2 2 2 2
etanercept (Enbrel) 2 1 2 2 2
adalimumab (Humira) 4 2 1 1
Insulinsinsulin glargine (Lantus) 2 1 2
insulin lispro (Humalog) 1
Anticoagulant enoxaparin sodium (Lovenox) 2
N-terminal parathyroid hormone teriparatide (Forteo) 2
Anti-CD20 monoclonal antibody rituximab (Rituxan, MabThera) 6 1 1
HER2 receptor inhibitor trastuzumab (Herceptin) 1 1 2
VEGF-A inhibitor bevacizumab (Avastin) 1 1
TOTAL 39 9 6 16 10 9
Updated February 23, 2018

Biosimilars for Inflammatory Diseases Approved by EMA & FDA
*Positive CHMP opinion. Pending EC decision
1. EMA. European public assessment reports for human medicines: Accessed October 2017; 2. FDA. FDA approves Erelzi, a biosimilar to Enbrel, 2016; 3. FDA. FDA approves Inflectra, a biosimilar to Remicade, 2016; 4. FDA. FDA approves Amjevita, a biosimilar to Humira, 2016; 5. FDA. FDA approves Renflexis biosimilar to Remicade, 2017; 6. FDA. FDA approves Cyltezo biosimilar to Humira, 2017; 7. Pfizer. FDA approves new Pfizer biosimilar, 2017.
2013 2014 2015 2016 2017
Adalimumab(Amjevita)4
(Erelzi)2(Benepali)1
Etanercept
(Flixabi)1 (Inflectra)3InfliximabInfliximab
(Inflectra, Remsima)1
Etanercept (Erelzi)1
Rituximab(Rixathon, Riximyo)1 (Truxima)1
Adalimumab(Amgevita, Solymbic)1(Imraldi)1
(Cyltezo*)1,6
Infliximab(Renflexis)5 (Ixifi)7

Demonstrating Biosimilarity: General Principles
• Biosimilar has been shown to be highly similar to reference product in extensive comparative analytical studies
• Clinical efficacy and safety have already been demonstrated by reference product
• Biosimilar must demonstrate similar efficacy and safety, compared to reference product • PK/PD, and immunogenicity studies
• Smaller, double-blind, parallel-group, active comparator clinical trial(s)• Patients with disease most responsive to reference product
• Use clinical endpoint most sensitive to detect product-related differences
• No need to demonstrate efficacy in all indications
• No differences in safety or efficacy are expected between an approved biosimilar and its reference product
US Food and Drug Administration. Scientific Considerations in Demonstrating Biosimilarity to a Reference Product: Guidance for Industry. Department of Health & Human Services, 2015.Committee for Medicinal Products for Human Use. Concept paper on the revision of the guideline on similar biological medicinal products containing biotechnology-derived proteins as active substance: non-clinical and clinical issues. London: European Medicines Agency, 2011.Committee for Medicinal Products for Human Use. Guideline on similar biological medicinal products containing monoclonal antibodies: non-clinical and clinical issues. London: European Medicines Agency, 2012.

Definitions: “A European Perspective”
• Interchangeability = “the medical practice of changing one medicine for another that is expected to achieve the same clinical effect in a given clinical setting and in any patient on the initiative, or with the agreement of, the prescriber.”
• Switching = “the decision by the treating physician to exchange one medicine with another medicine with the same therapeutic intent in a given patient.”
• Automatic substitution = “a practice of dispensing one medicine instead of another equivalent and interchangeable medicine at the pharmacy level without consulting the prescriber.”
Kurki P, et al. BioDrugs. 2017; 31:83-91.

Biologics Price Competition and Innovation Act of 2009: Interchangeability
FDA. Guidance Compliance Regulatory Information. http://www.fda.gov/downloads/Drugs/Guidance ComplianceRegulatoryInformation/UCM216146.pdf.

Definitions: ACR White Paper on Biosimilars
• Changing = “an intentional therapeutic alteration that is initiated by a health care provider in partnership with the patient.”• Often made for economic reasons, since biosimilar usually costs less than its
reference product (”non-medical changing”)
• May be made for medical reasons when a patient is not responding adequately to a drug other than reference product & biosimilar is chosen because of its lower cost.
• Switching = “used in the Biologics Price Competition & Innovation Act of 2009 when referring to transitioning to or from a biosimilar which has been designated as ‘interchangeable.’”
Bridges SL Jr, et al. Arthritis Rheumatol. 2018; 70:334-344.

Translating Definitions: From European to American
• Interchangeability (EU) = Changing (US)
• Switching (EU) = Changing (US)
• Automatic substitution (EU) = Switching (US)
Bridges SL Jr, et al. Arthritis Rheumatol. 2018; 70:334-344.

Clinical Trial Designs To Assess Biosimilar Switching
http://gabionline.net/Reports/Interchangeability-and-switching-study-designs-for-biosimilars
Reference Biosimilar
Single switch / single arm
Reference Biosimilar
Biosimilar
Single switch / parallel arm
Reference
Biosimilar
Reference
Biosimilar
rand
Single switch / parallel arm(includes non-switch comparator arm)
Reference Biosimilar
Biosimilar Reference
Single switch / cross-over
Reference Biosimilar
Reference Biosimilar
Reference
Biosimilar
Multiple switch / alternating

Clinical Trial Designs To Assess Biosimilar Switching
http://gabionline.net/Reports/Interchangeability-and-switching-study-designs-for-biosimilars
Reference Biosimilar
Biosimilar
Single switch / parallel arm

Phase 1 Double-Blind RCT of Infliximab-dyyb (CT-P13) vs. Infliximab Originator in Ankylosing Spondylitis
• 250 patients with active AS randomized 1:1 to receive either infliximab-dyyb or infliximab originator (5 mg/kg 2-hour IV infusion per dose)
• Dose-loading phase: Weeks 0, 2, & 6
• Maintenance phase: Weeks 14, 22, & 30
• Assessments• Ratios of geometric means of primary PK
parameters between Weeks 22-30 were subjected to ANCOVA analysis at 90% CIs
• ASAS20 & ASAS40 at Week 30
• Safety (incidence of AEs)
• Primary endpoint: Ratio of geometric means of PK parameters in infliximab-dyyb & infliximab originator arms (Weeks 22-30)
• AUCτ: 1.05 (90% CI 0.94 to 1.16)
• Cmax,ss : 1.02 (90% CI 0.95 to 1.09)
Related AEs(to Week 54)
Infliximab-dyyb(n=128)
Infliximab originator
(n=122)
Total 62 (48.4%) 63 (51.6%)
Infections 30 (23.4%) 24 (19.7%)
Infusion reactions 4 (3.1%) 11 (9.0%)
Tuberculosis 2 (1.6%) 1 (0.8%)
62,6%
70,5%67,0%
64,8%
72,4%69,4%
41,7%
51,8%54,7%
45,9% 47,4% 49,1%
0%
20%
40%
60%
80%
100%
Week 14 Week 30 Week 54
CT-P13 ASAS20 INX ASAS20CT-P13 ASAS40 INX ASAS40
ASAS20 & ASAS40 Responses up to Week 54
ASAS20
ASAS40
Park W, et al. Ann Rheum Dis. 2013; 72:1605-1612 Park W, et al. Arthritis Res Ther. 2016;18:25
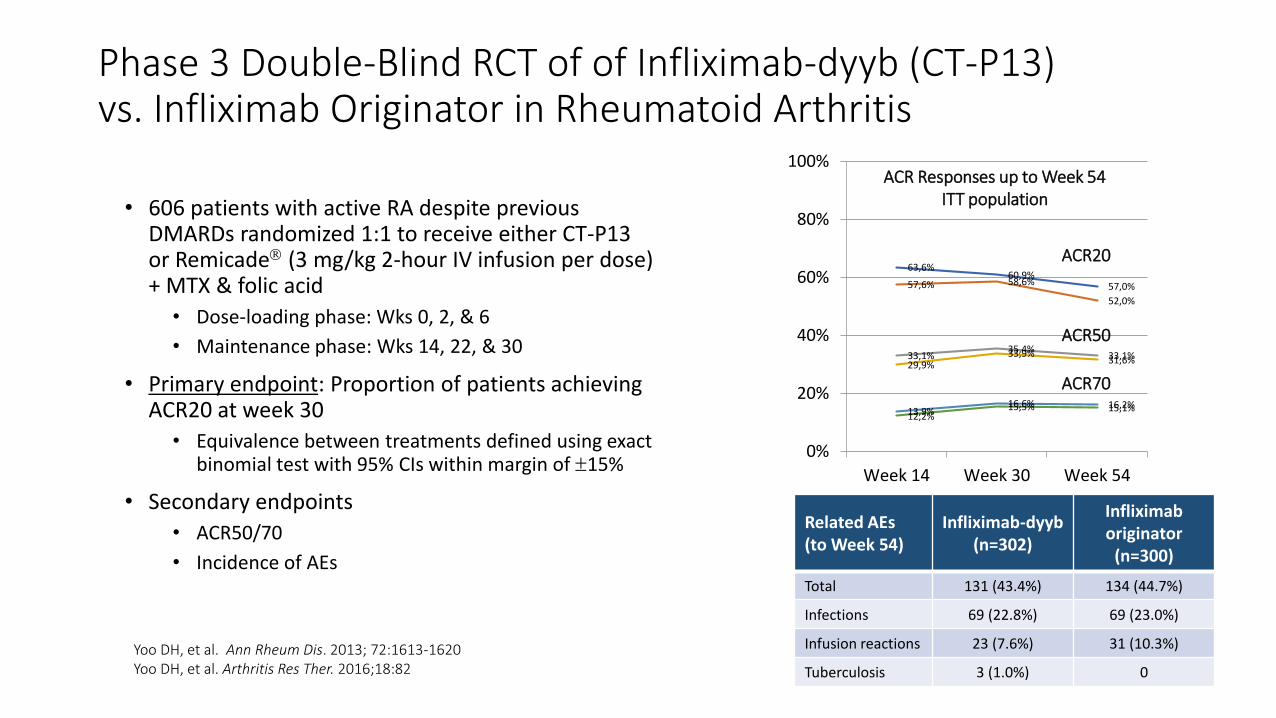
Phase 3 Double-Blind RCT of of Infliximab-dyyb (CT-P13) vs. Infliximab Originator in Rheumatoid Arthritis
• 606 patients with active RA despite previous DMARDs randomized 1:1 to receive either CT-P13 or Remicade (3 mg/kg 2-hour IV infusion per dose) + MTX & folic acid
• Dose-loading phase: Wks 0, 2, & 6
• Maintenance phase: Wks 14, 22, & 30
• Primary endpoint: Proportion of patients achieving ACR20 at week 30
• Equivalence between treatments defined using exact binomial test with 95% CIs within margin of 15%
• Secondary endpoints
• ACR50/70
• Incidence of AEs
Yoo DH, et al. Ann Rheum Dis. 2013; 72:1613-1620 Yoo DH, et al. Arthritis Res Ther. 2016;18:82
63,6%60,9%
57,0%57,6% 58,6%
52,0%
33,1%35,4%
33,1%29,9%
33,9%31,6%
13,9%16,6% 16,2%
12,2%15,5% 15,1%
0%
20%
40%
60%
80%
100%
Week 14 Week 30 Week 54
ACR Responses up to Week 54ITT population
ACR20
ACR50
ACR70
Related AEs(to Week 54)
Infliximab-dyyb(n=302)
Infliximab originator
(n=300)
Total 131 (43.4%) 134 (44.7%)
Infections 69 (22.8%) 69 (23.0%)
Infusion reactions 23 (7.6%) 31 (10.3%)
Tuberculosis 3 (1.0%) 0

74,376,3 77,0
71,7 71,773,9
77,5 77,5 78,2
71,8
0
20
40
60
80
100
Week 14 Week 30 Week 54 Week 78 Week 102
Maintenance group Switch group
Infliximab-dyyb (CT-P13) Open-Label Extension: Similar Efficacy Before & After Switching
Park W, et al. Ann Rheum Dis. 2017; 76:346-354Yoo DH, et al. Ann Rheum Dis. 2017; 76:355-363
CI: -10%, 11% CI: -10%, 10%CI: -16%, 4%CI: -10%, 9%CI: -11%, 9%
PLANETAS: Ankylosing Spondylitis PLANETRA: Rheumatoid Arthritis
AC
R2
0 R
esp
on
se R
ate
(%)
Mea
n B
ASD
AI S
core
Switch group: Infliximab originator → infliximab-dyyb at week 54

0%
10%
20%
30%
40%
50%
60%
0 20 40 60 80 100 120
Ankylosing Spondylitis
Maintenance CT-P13 5 mg/kg (n=90)
Switch INX -> CT-P13 5 mg/kg (n=84)
Infliximab-dyyb (CT-P13) Open-Label Extension: Similar Immunogenicity Before & After Switching
ADA = anti-drug antibodiesPark W, et al. Ann Rheum Dis. 2017; 76:346-354Yoo DH, et al. Ann Rheum Dis. 2017; 76:355-363
0%
10%
20%
30%
40%
50%
60%
0 20 40 60 80 100 120
Rheumatoid Arthritis
Maintenance CT-P13 5 mg/kg (n=159)
Switch INX -> CT-P13 5 mg/kg (n=143)
PLANETRA
Week Week
% S
ub
ject
s w
ith
AD
A
PLANETAS
p=0.48p=0.82
p=0.91p=0.82
p=1.00
p=0.60p=0.39
p=0.60
p=1.00
p=0.79
Note: Anti-drug antibodies were assessed by an electrochemiluminescentimmunoassay using Meso Scale Discovery technology

ELISA bridging assay
Patient cohort(# samples, # patients)
Promonitor-ANTI-IFX
(Infliximab originator)
CT-P13 SB2
ATI-positive samples, n 30 30 30
Infliximab originator only (60, 13) Median ATI level (AU/mL) 190 216 240
p (ANOVA) p=0.224
ATI-positive samples, n 14 14 14
CT-P13 only (28, 9) Median ATI level (AU/mL) 90 103 116
p (ANOVA) p=0.739
ATI-positive samples, n 32 32 32
Switchers (64, 12) Median ATI level (AU/mL) 203 216 228
p (ANOVA) p=0.902
Antibodies to Infliximab in IBD Patients Treated with Either Infliximab Originator or CT-P13 Show Identical Reactivity with CT-P13 & SB2
Fiorino G, et al. Inflamm Bowel Dis. 2018; 24:601-606.IBD = inflammatory bowel disease ; ATI = Antibodies to infliximab

Phase 3 Double-Blind RCT of SB4 vs Etanercept Originatorin Rheumatoid Arthritis
• 596 patients with active RA despite MTX randomized
1:1 to receive either SB4 or etanercept originator SC
weekly + MTX & folic acid for up to 52 weeks
• Primary endpoint: Proportion of patients achieving
ACR20 at week 24
• Equivalence between treatments: 95% CI of
difference of ACR20 response rates between
treatment groups had to be entirely contained within
margin of 15%
• Secondary endpoints
• ACR50/70, ACR-N, AUC of ΔDAS28, EULAR response
• Incidence of AEs and SAEs
RA = rheumatoid arthritis; SC = subcutaneous; EULAR = European League Against Rheumatism; TEAE = treatment-emergent adverse event.Emery P, et al. Ann Rheum Dis 2017; 76:51-57.
ACR Response Rates to Week 24
Per-protocol set
Related TEAEs(to Week 24)
SB4(n=299)
Etanerceptoriginator
(n=297)
Total 83 (27.8%) 106 (35.7%)
Serious TEAEs 13 (4.4%) 13 (4.4%)
Injection site reactions (ISRs)*
22 ISRs in11 pts (3.7%)
156 ISRs in51 pts (17.2%)
Tuberculosis 0 0
*p<0.001

SB4 Open-Label Extension in Rheumatoid Arthritis : Similar Efficacy Before & After Switching
ETN = etanercept originator; TEAE = treatment-emergent adverse event; ADA = anti-drug antibody.Emery P, et al. Ann Rheum Dis 2017;76:1986–1991.
Safety event(after Week 52)
SB4/SB4(n=126)
ETN/SB4(n=119)
≥1 TEAE 60 (47.6%) 58 (48.7%)
≥1 Serious TEAE 6 (4.8%) 2 (1.7%)
Serious infection 1 (0.8%) 1 (0.8%)
Injection site reactions (ISRs) 0 0
Active tuberculosis 0 0
Malignancy/death* 1 (0.8%) 0
• 245 patients in Czech republic & Poland who completed 52-week visit received SB4 for 48 additional weeks in open-label extension
• Efficacy, safety & immunogenicity were assessed up to week 100.
*Hepatic cancer
SB4/SB4(n=126)
ETN/SB4(n=119)
Wk 52 overall (after wk 0) 3/126 (2.4) 17/119 (14.3)
Wk 100 overall (after wk 0) 4/126 (3.2) 18/119 (15.1)
Wk 100 overall (after wk 52) 1/126 (0.8) 1/117 (0.9)
Incidence of ADAs After Week 52 (Extended Population)

Biologics Price Competition and Innovation Act of 2009: Interchangeability
FDA. Guidance Compliance Regulatory Information. http://www.fda.gov/downloads/Drugs/Guidance ComplianceRegulatoryInformation/UCM216146.pdf.

Demonstrating Interchangeability of a Biosimilar with a Reference Product: FDA Draft Guidance
• Postmarketing data
• Data from prospective, controlled switching study (or studies)• Design
• Lead-in period of treatment with reference product followed by randomized two-arm period (switching arm vs non-switching arm)
• At least three switches, with each switch crossing over to alternative product
• Analysis• Primary endpoints: PK data (Cmax, Tmax, Ctrough, AUC)
• Secondary endpoints: Safety, immunogenicity, and efficacy
• US-licensed reference product as comparator
US Food and Drug Administration. Considerations in Demonstrating Interchangeability With a Reference Product: Guidance for Industry (Draft Guidance). Department of Health & Human Services, 2017.

Study Designs Comparing Bio-originators & Biosimilars
Kay J. Biosimilars in rheumatology. In: Gravallese EM, Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, eds. Rheumatology, 7th Edition. Philadelphia: Elsevier Mosby [in press].

Primary EndpointRe-randomization if positive response in Treatment Period 1
Phase 3 Double-Blind RCT of Etanercept-szzs (GP2015) vs. Etanercept Originator in Psoriasis
Griffiths CEM, et al. Br J Dermatol. 2017;176:928-938.

Phase 3 RCT of Etanercept-szzs (GP2015) vs. Etanercept Originator in PsoriasisAdjusted PASI Response Rates for Continued vs. Switched Treatment Groups (PPS)
PASI = Psoriasis Area and Severity Index.
3 transitions
Griffiths CEM, et al. Br J Dermatol. 2017;176:928-938.

Phase 3 Double-Blind RCT of Filgrastim Biosimilar (EP2006) vs. Filgrastim Originator in Breast Cancer Patients Receiving Chemotherapy
Blackwell K, et al. Ann Oncol. 2015;26:1948-1953.
DSN = days of severe neutropenia

Phase 3 Double-Blind RCT of Filgrastim Biosimilar (EP2006) vs. Filgrastim Originator in Breast Cancer Patients Receiving Chemotherapy:Primary Endpoint (Cycle 1)
Blackwell K, et al. Ann Oncol. 2015;26:1948-1953.
PPS FAS

Phase 3 Double-Blind RCT of Filgrastim Biosimilar (EP2006) vs. Filgrastim Originator in Breast Cancer Patients Receiving ChemotherapyComparison of Pooled Continued vs. Pooled Switched Treatment Groups (PPS)
Adverse eventContinued arm
(n=108)Switched arm
(n=110)
Fever episodes 8 (9.3%) 12 (13.5%)
≥1 episode of febrile neutropenia 2 (2.3%) 6 (6.7%)
Febrile neutropenic episodes resulting in hospitalization
2 (2.3%) 1 (1.1%)
Infections 6 (7.0%) 9 (10.1%)
Blackwell K, et al. Ann Oncol. 2015;26:1948-1953.
In both continued & switched treatment arms • Similar depth of ANC nadir in each cycle• ANC nadir occurred on day 7 or 8 in each cycle for majority of patients
ANC = absolute neutrophil count

Switching: European Experience

NOR-SWITCH: Continuing Infliximab Originator vs. Switching to Infliximab-dyyb• 52-week randomized, double-blind, non-inferiority phase IV trial
• Primary endpoint: Disease worsening* during 52-week follow-up
*According to worsening in disease-specific composite measures and/or a consensus between investigator & patient leading to major change in treatment.
• Non-inferiority margin: 15%
• Exploratory subgroup analyses: Disease worsening within each of the 6 diagnoses
Jørgensen KK, et al. Lancet. 2017;389:2304-2316.
Week 52 Switch
Follow-up W78
Follow-up W78
Disease worsening
Disease worsening
Infliximab originator(n = 241)
Infliximab-dyyb(n = 241)R
and
om
izat
ion
1:1Patients with
stable CD, UC, SpA, RA, PsA, or PsO on
infliximab originator for ≥ 6 months
(n = 482)

NOR-SWITCH: Forest Plot of Risk Difference According to Disease
Jørgensen KK, et al. Lancet. 2017;389:2304-2316.
Per protocol population
DiagnosisCrohn’s diseaseUlcerative colitisSpondyloarthritisRheumatoid arthritisPsoriatic arthritisPsoriasisOverall
14 (21.2%)3 (9.1%)
17 (39.5%)11 (36.7%)7 (53.8%)1 (5.9%)
53 (26.2%)
23 (36.5%)5 (11.9%)
14 (33.3%)9 (30.0%)8 (61.5%)2 (12.5%)
61 (29.6%)
-14.3% (-29.3 – 0.7)-2.6% (-15.3 – 10.0)6.3% (-14.5 – 27.2)4.5% (-20.3 – 29.3)
-8.7% (-45.4 – 28.1)-6.7% (-26.7 – 13.2)-4.4% (-12.7 – 13.2)
Infliximaboriginator
n=202
Infliximab-dyyb
n=202
Risk difference(95% CI)
-50 -40 -30 -20 -10 0 10 20 30 40 50
Favours infliximaboriginator
FavoursInfliximab-dyyb
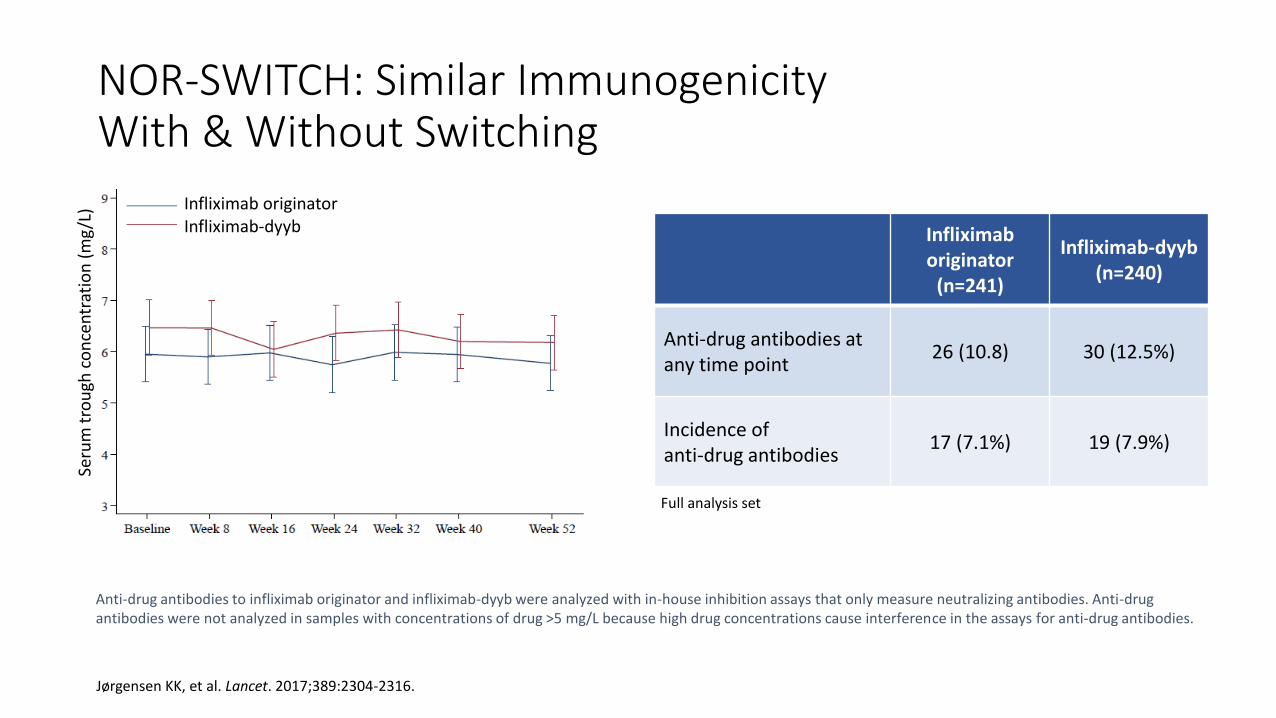
NOR-SWITCH: Similar Immunogenicity With & Without Switching
Infliximab originator
(n=241)
Infliximab-dyyb(n=240)
Anti-drug antibodies at any time point
26 (10.8) 30 (12.5%)
Incidence of anti-drug antibodies
17 (7.1%) 19 (7.9%)
Anti-drug antibodies to infliximab originator and infliximab-dyyb were analyzed with in-house inhibition assays that only measure neutralizing antibodies. Anti-drug antibodies were not analyzed in samples with concentrations of drug >5 mg/L because high drug concentrations cause interference in the assays for anti-drug antibodies.
Jørgensen KK, et al. Lancet. 2017;389:2304-2316.
Full analysis set
Design: 52-week randomized, double-blind, non-inferiority,
phase IV trial.
Main inclusion criteria: Adult patients with a diagnosis of SpA,
RA, PsA, CD, UC or Ps on stable treatment with the originator
infliximab (Remicade®, INX) for at least 6 months.
Primary endpoint: Disease worsening during follow-up
according to worsening in disease-specific composite
measures and/or a consensus between investigator and
patient leading to major change in treatment. Exploratory
subgroup analyses were performed to examine disease
worsening within each of the six diagnoses.
Statistics: Non-inferiority margin 15% and power calculations
indicated that 394 patients were required in the primary Per
Protocol Set (PPS). The primary endpoint was analysed using
logistic regression, adjusted for diagnosis and disease duration
at baseline.
Total INX CT-P13
Screened 498
Randomised 482 241 241
Full Analysis
Set (FAS) 481 241 240
Per Protocol
Set (PPS) 408 202 206
INX (n=241) CT-P13 (n=240)
Age (years) 47.5 (14.8) 48.2 (14.9)
Females (%) 41.1 36.2
Disease duration (years) 16.7 (10.9) 17.5 (10.5)
Duration of ongoing INX (years) 6.7 (3.6) 6.9 (3.8)
INX
(n=241)
CT-P13
(n=240)
ADAb at any time
point 10.8 % 12.5 %
Incidence of
ADAb 7.1 % 7.9 %
[number of events] n (%) INX (241) CT-P13 (n=240)
SUSAR 0 0
SAE [32] 24 (10.0) [27] 21 (8.8)
AE [422] 168 (69.7) [401] 164 (68.3)
AE study drug discontinuation [18] 9 (3.7) [9] 8 (3.3)
Disclosures: GL Goll Orion Pharma, Pfizer, Abbvie, Novartis IC Olsen, None KK Jorgensen Intercept, Celltrion, Tillott M Lorentzen None N Bolstad None EA Haavardsholm AbbVie, UCB, Pfizer, MSD, Roche KEA Lundin Orion Pharma, MSD, Takeda C Mork Novartis, LEO Pharma,
ACO hud, AbbVie, Galderma Nordic, Cellgene J Jahnsen Orion Pharma ,Celltrion, Pfizer, MSD, AbbVie, Takeda, Napp Pharm, AstroPharma T K Kvien Biogen, BMS, Boehringer Ingelheim, Celltrion, Eli Lily, Epirus, Hospira, Merck-Serono, Novartis, Orion Pharma, Pfizer, Sandoz, UCB
Contact information:
Tore K Kvien Diakonhjemmet Hospital, Oslo, Norway. [email protected]
Biosimilar Infliximab (CT-P13) is Not Inferior to Originator Infliximab:
Results from a 52-week Randomized Switch Trial in Norway Guro L Goll1, Inge C Olsen1, Kristin K Jørgensen 2 , Merete Lorentzen3, Nils Bolstad4, Espen A Haavardsholm1 , Knut EA Lundin 5, Cato Mørk6 , Jørgen Jahnsen2, Tore K Kvien1 and the NOR-SWITCH study group
1 Dept. of Rheumatology, Diakonhjemmet Hospital, Oslo, Norway. 2 Dept of Gastroenterology Akershus University Hospital, Lorenskog, Norway 3 Dept of Dermatology, Oslo University Hospital, Oslo, Norway 4 Dept of Medical Biochemistry, DNR-Oslo
University Hospital, Oslo, Norway 5Dept of Gastroenterology, Rikshospitalet-Oslo University Hospital 6Norwegian University of Science and Technology, Dept of Cancer and Molecular medicine, Trondheim, Norway
Abstract
Abstract 19LB
Methods Results – patients Results – secondary efficacy endpoints
Background and objective
TNF-inhibitors (TNFi) have improved treatment of
spondyloarthritis (SpA), rheumatoid arthritis (RA), psoriatic
arthritis (PsA), Crohn’s disease (CD), ulcerative colitis (UC),
and chronic plaque psoriasis (Ps). Patients starting biologic
treatment can receive biosimilar CT-P13 in many countries.
However, switching stable patients who are doing well on
originator infliximab, has been controversial. The NOR-
SWITCH trial was funded by the Norwegian government.
The aim of the NOR-SWITCH trial was to examine switching
from originator to biosimilar infliximab regarding efficacy, safety
and immunogenicity in patients on stable treatment with the
originator drug.
Results – patients
Results – primary endpoint
Results – secondary efficacy endpoints
Results – immunogenicity
Results – safety
Conclusion
Switch from INX to CT-P13 was not inferior to continued
treatment with INX for disease worsening. Results were also
similar for other efficacy endpoints, immunogenicity and safety.
We recommend caution in generalizing these findings to other
biologic agents. In our opinion, there is a need for further switch
studies which may be extended to include multiple sequenced
as well as back-and-forth switches.
Disease worsening
Remission
Background/purpose:
TNF-inhibitors (TNFi) have improved treatment of spondyloarthritis (SpA), rheumatoid arthritis (RA),
psoriatic arthritis (PsA), Crohn’s disease (CD), ulcerative colitis (UC), and chronic plaque psoriasis (Ps).
The NOR-SWITCH trial was funded by the Norwegian government. The aim of the NOR-SWITCH trial
was to examine switching from originator to biosimilar infliximab regarding efficacy, safety and
immunogenicity.
Methods:
The study was designed as a 52-week randomized, double-blind, non-inferiority, phase IV trial. Adult
patients with a diagnosis of SpA, RA, PsA, CD, UC or Ps on stable treatment with the originator infliximab
(Remicade®, INX) for at least 6 months were eligible. Patients with informed consent were randomized
1:1 to either continued INX or switch to CT-P13 treatment (biosimilar infliximab, Remsima®), using
unchanged dosing regimen. Data were collected at infusion visits. The primary endpoint was disease
worsening during follow-up according to worsening in disease-specific composite measures and/or a
consensus between investigator and patient leading to major change in treatment. Exploratory subgroup
analyses were performed to examine disease worsening within each of the six diagnoses. The non-
inferiority margin was set to 15% and power calculations indicated that 394 patients were required in the
primary Per Protocol Set (PPS). The primary endpoint was analysed using logistic regression, adjusted for
diagnosis and disease duration at baseline.
Results
Between October 6, 2014 and July 8, 2016, 481 patients (INX 241, CT-P13 240, Full Analysis Set, FAS) at
40 Norwegian study centres were randomized, received treatment and were followed for 52 weeks. The
main demographic and baseline characteristics are shown in the table. Disease worsening occurred in
26.2% and 29.6% of patients in the INX and CT-P13 arms, respectively (PPS). The 95% confidence
interval of the adjusted treatment difference (-4.4%) was -12.7 – 3.9 which was within the pre-specified
non-inferiority margin. The frequency of disease worsening in each specific diagnosis is shown in the
table (exploratory analyses). Changes in the generic disease variables and disease specific composite
measures were similar in both arms (table). The incidence of anti-drug antibodies detected during the
study was 17 (7.1%) and 19 (7.9%) in the INX and CT-P13 patients, respectively (FAS). The trough drug
levels and the frequencies of reported adverse events including infusion reactions were also similar (data
not shown).
Conclusion
The NOR-SWITCH trial demonstrated that switch from INX to CT-P13 was not inferior to continued
treatment with INX. …
Numbers are mean (SD) or percent
Seru
m t
rou
gh c
on
cen
trat
ion
(m
g/L
) Infliximab originatorInfliximab-dyyb

NOR-SWITCH: Similar Treatment-Emergent Events in Safety Population With & Without Switching
Infliximab originator (n=241)
Infliximab-dyyb(n=240)
SUSAR 0 0
Serious AE 32/24 (10%) 27/21 (9%)
AE 422/168 (70%) 401/164 (68%)
AE resulting in study drug discontinuation* 18/9 (4%) 9/8 (3%)
Infusion-related reaction 10/10 (4%) 5/4 (2%)
Data are number of events/number of patients (%). SUSAR=serious unexpected serious adverse reaction.
*Patients could have other primary reason for study drug discontinuation.
Jørgensen KK, et al. Lancet. 2017;389:2304-2316.

NOR-SWITCH: Comparable Long-Term Safety & Efficacy of Infliximab-dyyb After Switching from Infliximab Originator 26-Week Open Label Extension
Disease Measures at Week 78Maintenance group
(n=197)Switch group
(n=183)Adjusted difference
Week 78 (95% CI)
Physician Global Assessment (0-10) 1.45 (1.55) 1.15 (1.51) 0.13 (-0.13-0.4)
Patient Global Assessment (0-10) 2.58 (2.26) 1.88 (1.96) 0.48 (0.16-0.8)
Log10 ESR (mm/h) 0.89 (0.4) 0.86 (0.38) 0 (-0.05-0.05)
Log10 C-reactive protein (mg/L) 0.31 (0.48) 0.33 (0.4) -0.02 (-0.1-0.05)
Harvey-Bradshaw Index (CD) 2.93 (3.24) 2.44 (3.28) 0.57 (-0.2-1.33)
Partial Mayo Score (UC) 0.88 (1.55) 0.47 (0.82) 0.44 (-0.13-1.01)
ASDAS (SpA) 2.13 (0.85) 1.79 (0.61) 0.2 (-0.06-0.46)
DAS28 (RA, PsA) 2.48 (1.54) 2.62 (1.16) 0.19 (-0.33-0.71)
CDAI (RA, PsA) 6.81 (7.47) 6.45 (6.74) 1.92 (-1.07-4.91)
SDAI (RA, PsA) 7.41 (7.95) 6.84 (6.79) 2.13 (-1.86-6.12)
PASI (PsO) 1.49 (0.89) 1.25 (0.88) -0.28 (-0.87-0.31)
Data are n (%), mean (SD) or median (25 – 75 percentiles). 95% CI, 95% confidence interval of the adjusted treatment difference. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index. ASDAS, Ankylosing Spondylitis Disease Activity Score.DAS28, Disease Activity Score in 28 joints. CDAI, Clinical Disease Activity Index. SDAI, Simplified Disease Activity Index. PASI, Psoriasis Area and Severity Index.
Goll GL, et al. ACR 2017, Abstract 2800.
• Comparable frequencies of reported AEs.
• Anti-drug antibodies developed in:• 3/197 (1.5%) pts in
maintenance group • 5/183 (2.7%) pts in
switch group
• Comparable trough drug levels

OutcomeDisease Activity
3 Mo Pre-switch Switch 3 Mo Post-switch
Changes Over Time
Δ Pre-switch Δ Post-switch
P Value
RA (n = 403) (n = 319) (n = 310) (n = 309) (n = 276) (n = 265)
DAS28 2.2 (1.7 to 2.9) 2.2 (1.8 to 3.0) 2.2 (1.8 to 3.2) 0.1 (-0.2 to 0.5) 0.0 (-0.4 to 0.4) 0.8
HAQ (0-3) 0.6 (0.1 to 1.0) 0.6 (0.1 to 1.0) 0.6 (0.2 to 1.1) 0.0 (0.0-0.1) 0.1 (-0.1 to 0.1) 0.3
CRP, mg/L 4 (2 to 7) 4.5 (2 to 8) 5 (2 to 8) 0 (-1 to 2) 0 (-2 to 3) 0.4
Patient’s VAS global score, mm 26 (12 to 51) 25 (11 to 51) 26 (12 to 56) 0.0 (-7 to 8) 0.0 (-7 to 9) 0.5
PsA (n = 120) (n = 94) (n = 92) (n = 94) (n = 78) (n = 81)
DAS28 2.5 (1.7 to 3.1) 2.3 (1.7 to 3.1) 2.4 (1.8 to 3.3) 0.0 (-0.4 to 0.2) 0.1 (-0.4 to 0.6) 0.10
HAQ (0-3) 0.5 (0.1 to 1.1) 0.6 (0.1 to 1.1) 0.5 (0.1 to 1.1) 0.0 (-0.1 to 0.1) 0.0 (0.0-0.1) 0.5
CRP, mg/L 4 (1 to 6) 4 (1 to 6) 3 (2 to 7) 0 (-1 to 1) 0 (-1 to 2) 0.046
Patient’s VAS global score, mm 32 (10 to 56) 34 (10 to 67) 35 (11 to 62) -3 (-12 to 4) 0 (-7 to 11) 0.01
AxSpA (n = 279) (n = 202) (n = 199) (n = 204) (n = 160) (n = 169)
BASDAI, mm 23 (8 to 40) 24 (10 to 40) 25 (11 to 45) 0 (-4 to 5) 0 (-4 to 7) 0.3
CRP, mg/L 3 (1 to 6) 4 (1 to 8) 4 (1 to 8) 0 (-1 to 1) 0 (-1 to 2) 0.2
Patient’s VAS global score, mm 26 (10 to 53) 31 (14 to 56) 27 (11 to 59) 1 (-4 to 8) -1 (-7 to 7) 0.7
ASDAS 1.8 (1.2 to 2.6) 2.0 (1.4 to 2.6) 2.0 (1.2 to 2.9) 0.0 (-0.3 to 0.4) 0.0 (-0.3 to 0.3) 0.8
DANBIO Registry: Nationwide Non-medical Switch From Infliximab Originator to Infliximab-dyyb in DenmarkSimilar Disease Activity 3 Months Before & After Switch in 802 Pts With RA, PsA, or AxSpA
Glintborg B, et al. Ann Rheum Dis. 2017;76:1426-1431.
Numbers are medians (interquartile ranges) unless otherwise stated (%) . VAS = visual analogue scale.
Adjusted absolute 1-year retention rates• Infliximab-dyyb: 83.4% (95% Ci 80.8 to 86.2) • Historical IFX originator cohort: p=0.03
86.8% (95% Ci 84.8 to 88.8)

OutcomeDisease Activity
3 Mo Pre-switch Switch 3 Mo Post-switch
Changes Over Time
Δ Pre-switch Δ Post-switch
P Value
RA (n = 891)
DAS28 2.1 (1.7 to 2.9) 2.1 (1.6 to 2.9) 2.2 (1.6 to 3.1) 0.0 (-0.4 to 0.5) 0.0 (-0.4 to 0.5) 0.2
HAQ (0-3) 0.6 (0.2 to 1.3) 0.8 (0.1 to 1.3) 0.8 (0.3 to 1.3) 0.0 (-0.1 to 0.1) 0.0 (-0.1 to 0.1) 0.7
CRP, mg/L 3 (1 to 7) 2 (1 to 6) 3 (1 to 6) 0 (-2 to 1) 0 (-1 to 1) 0.02
Patient’s VAS global score, mm 30 (13 to 57) 28 (13 to 55) 31 (11 to 62) 0.0 (-11 to 9) 0.0 (-9 to 11) 0.1
PsA (n = 335)
DAS28 2.0 (1.5 to 2.6) 2.0 (1.6 to 2.8) 2.1 (1.5 to 3.0) 0.0 (-0.2 to 0.5) 0.0 (-0.6 to 0.5) 0.7
HAQ (0-3) 0.5 (0.1 to 1.1) 0.5 (0.0 to 1.1) 0.5 (0.1 to 1.1) 0.0 (-0.1 to 0.1) 0.0 (-0.1 to 0.1) 0.7
CRP, mg/L 2 (1 to 4) 2 (1 to 4) 2 (1 to 4) 0 (-2 to 1) 0 (-1 to 1) 0.04
Patient’s VAS global score, mm 31 (12-58) 30 (13 to 54) 32 (13 to 59) 0 (-9 to 7) 0 (-7 to 12) 0.2
SpA (n = 322)
BASDAI, mm 33 (15 to 51) 27 (12 to 48) 29 (16 to 47) -1 (-7 to 5) 1 (-5 to 8) 0.03
CRP, mg/L 3 (1 to 6) 3 (1 to 5) 3 (1 to 5) 0 (-2 to 1) 0 (-1 to 1) 0.4
Patient’s VAS global score, mm 34 (16 to 59) 30 (12 to 53) 31 (15 to 53) -1 (-12 to 6) 2 (-6 to 14) 0.04
ASDAS 2.0 (1.3 to 2.8) 1.9 (1.2 to 2.7) 1.9 (1.3 to 2.7) -0.1 (-0.4 to 0.2) 0.1 (-0.4 to 0.5) 0.1
DANBIO Registry: Nationwide Non-medical Switch From Etanercept Originator to SB4 in DenmarkSimilar Disease Activity 3 Months Before & After Switch in 1548 Pts With RA, PsA, or AxSpA
Glintborg B, et al. Ann Rheum Dis. 2017;76(Suppl 2):553 [EULAR 2017, Abstract FRI0190].
• 129/1548 (8.3%) pts stopped SB4 treatment during 5 mo. follow-up(59 lack of effect, 42 AEs, 2 remission, 4 cancer, 1 death, 21 other)
• Higher patient global score & not using MTX were associated with withdrawal
Numbers are medians (interquartile ranges) unless otherwise stated (%). VAS = visual analogue scale.*Δ values for disease activity pre-switch vs. post-switch, Wilcoxon matched-pair signed rank test

Nocebo Effect
• Nocebo = “I will harm” (Latin)
• Symptoms and/or physiological changes that follow administration of an inert, chemically inactive substance that patient believes to be an active drug.
• Refers to distressing symptoms that accompany placebo administration in ~25%
• May also account for side effects experienced by patients taking an active drug
• Misattribution of bodily symptoms to a drug is more likely to occur in:
• Patients who expect to experience distressing side effects
• Patients who have experienced side effects to other drugs in the past
• Patients with anxiety, depression, and somatization
• Patients with erroneous information and misunderstandings about drug
• Address by education; avoid imparting negative expectations about a drug; open, collaborative discussion; reassurance; and encouragement of patient
Barsky AJ et al. JAMA. 2002; 287:622-627Colloca L & Finniss D. JAMA. 2012; 307:567-568.
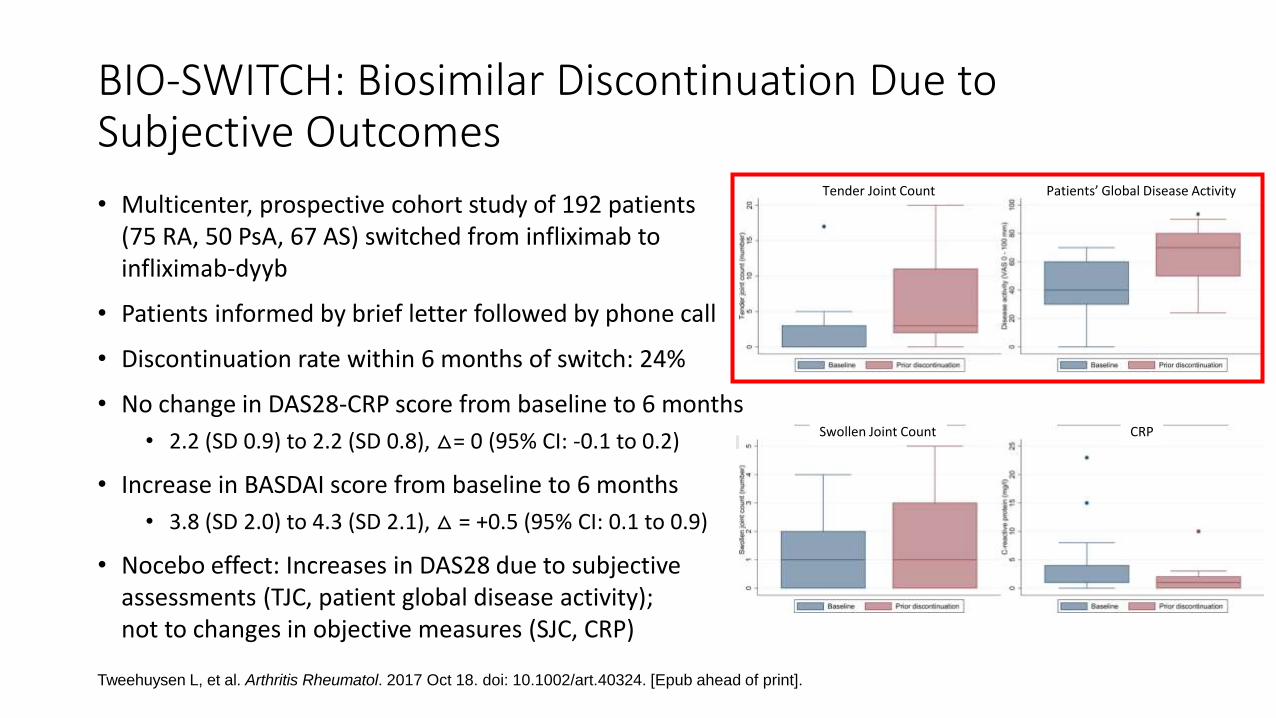
BIO-SWITCH: Biosimilar Discontinuation Due to Subjective Outcomes
• Multicenter, prospective cohort study of 192 patients (75 RA, 50 PsA, 67 AS) switched from infliximab to infliximab-dyyb
• Patients informed by brief letter followed by phone call
• Discontinuation rate within 6 months of switch: 24%
• No change in DAS28-CRP score from baseline to 6 months
• 2.2 (SD 0.9) to 2.2 (SD 0.8), △= 0 (95% CI: -0.1 to 0.2)
• Increase in BASDAI score from baseline to 6 months
• 3.8 (SD 2.0) to 4.3 (SD 2.1), △ = +0.5 (95% CI: 0.1 to 0.9)
• Nocebo effect: Increases in DAS28 due to subjective assessments (TJC, patient global disease activity); not to changes in objective measures (SJC, CRP)
Tweehuysen L, et al. Arthritis Rheumatol. 2017 Oct 18. doi: 10.1002/art.40324. [Epub ahead of print].
Accep
ted
Art
icle
This article is protected by copyright. All rights reserved.
Tender Joint Count Patients’ Global Disease Activity
Accep
ted
Art
icle
This article is protected by copyright. All rights reserved.
Swollen Joint Count CRP

BIO-SPAN: BIOsimilar switch - Study on Persistence & Role of Attribution & Nocebo
• 625 pts (433 RA, 128 PsA, 64 axSpA) in Netherlands agreed to open label non-mandatory transition from etanerceptoriginator to SB4 with structured communication strategy
• All patients informed that lower costs & fewer injection site reactions were reason for transitioning
• Rheumatology & pharmacy staff trained how to counsel pts about biosimilars & how to discuss possible nocebo response
• Compared to historical cohort of 600 etanerceptoriginator-treated patients (67% included in both cohorts)
• Primary outcome: Adjusted hazard ratio (HR) between SB4 discontinuation in transition cohort & etanerceptoriginator discontinuation in historical cohort = 1.57 (95% CI 1.05 to 2.36)
• Crude 6-month etanercept originator retention rate in historical cohort = 92% (95% CI 90% to 94%)
• Crude 6-month SB4 retention rate in transition cohort = 90% (95% CI 88% to 93%)
Tweehuysen L, et al. Ann Rheum Dis 2017;76:557.Tweehuysen L, et al. ACR 2017, Abstract 2438
Kaplan Meier plots of crude retention rates of SB4 (transition cohort) & etanercept (historical cohort)
Reason for discontinuation
SB4 in transition cohort
(n=60)
Etanerceptoriginator in
historical cohort (n=46)
Lack of effect 43% 61%
AEs 47% 28%
Malignancy 3% 4%
Pregnancy 4% 4%
Other 3% 3%

NOR-MULTISWITCH (The “Four-Switch” Study)
• Primary endpoint: Ctrough before last infusionCtrough at randomization
• Equivalence margin: 90% CI (0.8-1.25)
• Secondary endpoints: Efficacy, safety, immunogenicity
GP-1111INXSB2
Week: 0 3216 7248
CT-P13
Stable diseaseactivity onCT-P13 for ≥24 weeks
Randomization
INXSB2GP-1111
SB2GP-1111INX
CT-P13
CT-P13
Studyendpoint
Switch SwitchSwitchSwitch

Summary
• Bio-originators are subject to drift & evolution and may vary from batch to batch
• Biosimilars approved by regulators are highly similar to their reference products with equivalent efficacy and comparable safety
• Changing from bio-originators to their biosimilars in clinical trials does not result in significant loss of efficacy or increased occurrence of adverse events or immunogenicity
• Several trials have included multiple switches between bio-originator & biosimilar• No significant loss of efficacy
• Comparable safety & immunogenicity
• Prospective comparison of switching among biosimilars of same reference product is needed





























