Embed Size (px)
Citation preview

Biosimilars and the New Drug Development Paradigm laboratory tests versus clinical trials
Arnold G. Vulto FCP PharmD PhD
Professor of Hospital Pharmacy & Practical Therapeutics
Erasmus University Medical Center, Rotterdam, The Netherlands
2nd MENA Regulatory conference on Bioequivalence, Biowaivers,
Bioanalysis, Dissolution and Biosimilars
Amman, 17 September 2015

The question I will address today
Why would a doctor prescribe a biosimilar and/or a pharmacist dispense a biosimilar?
The decision to prescribe a drug is a yes/no decision, black or white.
This first talk is on the background why physicians have reservations to prescribe biosimilars.
2

Who is Arnold Vulto?
A practising hospital pharmacist, not a lawyer or regulator
Member of ErasmusMC Medical Ethical Review Board
We see and run all drug trials
Got involved in biosimilars as early as 2004 via Eur J Hosp Pharmacy
How to guide hospital pharmacists in this difficult area
2008 Founder of GaBI, together with Huub Schellekens and Lasia Tang
To provide transparency to cost-effective medicines
2013 Co-founder of the Dutch Biosimilar Initiative
Independent platform to promote efficient use of medicines
My motto: For each patient the best medicine at the best price
3

Conflict of Interest
I declare no personal financial interest in any pharmaceutical bussiness
I entertain friendly relationships with all innovative and generic / biosimilar companies
As a co-founder I have a societal – but not financial - interest in the advocacy of cost-effective treatments via the Generics & Biosimilar Initiative (GaBI)
My employer – Erasmus University Hospital - receives any speakers honoraria if they let me speak at scientific or commercial meetings (like this one).
4

Agenda
1. What are biosimilars?
2. How are biosimilars developped?
A paradigm shift
3. Biosimilars: not a container-principle
3 “generations” of biosimilars
4. Indication extrapolation
Is “totality of evidence” a valid principle?
5. Why would a physician prescribe a bisimilar?
6. Take home message
5

Biosimilars: What are we talking about?
6
The only true definition of a biosimilar as of September 2015: A biosimilar is a pharmaceutical product, that as such has been licensed
via the WHO regulatory pathway (=minimum global standard)
What does that mean? It is a version of an already licensed biotech-drug, for which similarity has
been proven in an extensive comparability exercise, encompassing physical, chemical, biological and pharmacological properties, including efficacy and safety
This excludes all kinds of bio-questionables in existence in other regions of the world that have not been endorsed via the WHO pathway as a biosimilar. Reference to such products as if biosimilars may be inferior is thus WRONG.

List of EU-licensed biosimilars (1/1/2015)
7

How are biosimilars developped?
“Reversed engineering” and “reversed body of evidence”
An existing drug (“reference-product”) is disassembled and characterised in great detail
The resulting protein is cloned and expressed in a polyclonal cellsystem.
Hundreds of cells are scrutinised for the best similarity
The best cell-molecule combinations are worked up in an extensive physical-chemical test battery
Next comparison in animal experiments and more advanced test systems
If resemblance is > 99,9% sure, similarity is CONFIRMED in a small trial.
This limited trial is performed in a representative and sensitive indication.
8

This is a new drug development paradigm, in which the “similarity excercise” is key
9
Clinical trials
PK / PD
Pre-clinical
Analytical

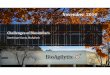
Integration of data from multiple analytical and biological tests provides complete understanding
Primary structure
Posttranslational modifications
Higher order structure
Impurities
Σ Combination of attributes
Biological activity
+
+
+
• Combined data from ~40 different methods provide information on multiple attributes (orthogonality)
• Every attribute is evaluated more than once (redundancy)
Berkowitz SA, et al. Nat Rev Drug Discov 2012; 11(7): 527–540

The sensitivity of analytical methods has increased enormously: Mass spectrometry example
11

12

Physicochemical characterisation of Celltrion’s biosimilar infliximab Vs Remicade
A multitude of state-of-the-art analysis
Identical primary structure (amino-acid sequence etc.)
Indistinguishable higher order structure
Peptide mapping (chromatography)
Higher order structure analysis
Antibody conformation array
Crystalline micrographs
Size exclusion chromatography
Iso-electro focussing looking for isoforms
Etc etc
13

14

15

16

17

18
With a real innovative drug we need to explore unknown territory Uncertainty is by nature large
Research is focussed on reducing uncertainty in knowledge and on proof of efficacy and safety
In biosimilars we compare with an existing drug, we know already for 10 – 15 years Uncertainty is relatively small
Research is focussed on the confirmation of similarity (and not proof of efficacy or safety)
What is the essential difference in approach?

The role of clinical trials in biosimilar development
Not for proof of efficacy
Confirmation of similarity
Laboratory tests (fingerprinting) are more sensitive to find small difference
The stronger the pre-clinical evidence, the smaller the requirements for clinical trials.
Physicians have been trained in the principles of Evidence Based Medicine, with the controlled clinical trial as golden standard for proof of efficacy.
This is not the case for biosimilars (and therefore difficult to accept)
19

Agenda
1. What are biosimilars?
2. How are biosimilars developped?
A paradigm shift
3. Biosimilars: not a container-principle 3 “ generations” of biosimilars
4. Indication extrapolation
Is “totality of evidence” a valid principle?
5. Why would a physician prescribe a bisimilar?
6. Take home message
20

Three Generations of Therapeutic Proteins / biosimilars
Generation 1: substitution products (“replacement therapy”)
Like hormones, growth factors
Generation 2: proteins with a distinct pharmacologcial effect
Like TNF-alfa inhibitors
Generation 3: proteins with a more remote clinical effect
Targeted therapies in oncology

First generation: proteins mimicking biological functions
Mostly hormones
Insulin
Follicle stimulating hormone
Growth hormone
Coagulation factors and thrombolytic agents
Hematopoietic growth factors
Pharmacological effects:
almost instantaneous or visible within days
Mostly a simple dose-effect relationship

1st generation biosimilar replacement therapy
Examples of such effects
Insulin: glucose goes down
FSH: ovulation occurs
Growth hormone
Initially effect on “biomarkers”
On the longer term: increased length growth
Coagulation factors: stop bleeding
Thrombolytic agents: dissolve blood clots
Hematopoietic growth factors:
increase in white or red blood cell count

2nd generation: Therapeutic proteins with a pharmacological action
These proteins do not mimic a biological function, but act mostly as an pharmacologcial antagonist e.g. binding a circulating protein or blocking a receptor
The clinical effect may be visible and measurable within days or weeks
Example: TNF-alpha inhibitors like infliximab and etanercept.

Second generation of EU licensed biosimilar
Active Substance Brand Name Approval Date
Infliximab (CT-P13) Inflectra Remsima
September 2013 September 2013
Approved indications Supported by clinical research:
• Ankylosing spondylitis • Rheumatoid arthritis
Extrapolated indications: • Psoriatic arthritis • Psoriasis • Crohn’s Disease • Ulcerative colitis
Due to patent restrictions, the product could only be marketed after February 2015

www.gabionline.net (1/09/2015)
(The best patentdeal of the century)
26
Will be extended

3rd generation: therapeutic proteins with a remote clinical effect
These protein drugs provide a statistical chance on benefit some time in the future (e.g. trastuzumab, rituximab).
Now we need deep trust in the principles of similarity.
On what is the purported clinical effect based?
Can we expand the use in other types of cancer?
Doctors may be very reluctant to accept clinical similarity of these molecules (“You can’t gamble with patients’ lives”)
As yet, these are theoretical questions: as yet no biosimilar of this type has been granted marketing authorization.

More complex molecules require also deeper understanding of the similarity principles
Different generations are confronted with different emotions
First generation biosimilars are a no-brainer They work, and have a proven safety track record
Second generation biosimilars: Are now available in the greater part of Europe
The current knowledge base looks promising
Extrapolation of indications under debate among professionals
Third generation biosimilars: Difficult to say: as yet no product in registration (August 2015)

Agenda
1. What are biosimilars?
2. How are biosimilars developped?
A paradigm shift
3. Biosimilars: not a container-principle
3 “generations” of biosimilars
4. Indication extrapolation Is “ totality of evidence” a valid principle?
5. Why would a physician prescribe a bisimilar?
6. Take home message
29

DIA meeting Berlin
30

31

Extrapolation is not a free ride It is based on rigorous scientific principles
32

Extrapolation of indications: how does that work?
If the comparability exercise in a battery of tests shows that biosimilar and reference product behave the same, biosimilarity is assumed
This means that the biosimilar will work for the same conditions as the reference product
It is the ultimate conclusion of the comparability exercise
A limited trial is used to confirm these expectations
This conflicts with traditional “evidence based” thinking, where the clinical trial is the ultimate proof of efficacy and saftey
Result of > 30 years education in “evidence based medicine”
33

34

Extrapolation of indications with Inflectra / Remsina (Source: EPAR para 2.6.3.)
Based on an extensive review on mode of action in different indications
Indeed, mode of action of infliximab is complex and partly unknown
Major effect: binding to soluble / membrane bound TNF
Possibly also other actions, like direct cytotoxicity (ADCC)
In inflammatory bowel disease it is unknown which “mixture” is best
CTP-13 is virtually identical to Remicade ®
Somewhat less fucosylation; likely clinically irrelevant
The best in-vitro models support similarity
There was a very small series of IBD patients treated
Follow up in post-marketing surveillance (as with any other new drug)
35

ECCO survey on concerns of GE-physicians (2013)
36
Immunogenicity: - Analytical data cannot predict immunogenicity - Issues around methodology used to detect Anti-drug-antibodies Safety:
- manufacturer may not have assessed differences between attributes biosimilar vs originator
- subtle changes may have profound effects on immunogenicity Trial sensitivity:
- appropriate statistics / margins to capture clinically relevant differences in phase 3 trials ?
Extrapolation: - safety and efficacy data transferable to other indications ? - different effects / distribution of mAbs in different tissues ? - role of other confounding factors eg. co-medication (eg MTX) ? - different safety profiles in different populations ? Molecular stability : - what if originator and biosimilar drift apart over time ?

Agenda
1. What are biosimilars?
2. How are biosimilars developped?
A paradigm shift
3. Biosimilars: not a container-principle
3 “generations” of biosimilars
4. Indication extrapolation
Is “totality of evidence” a valid principle?
5. Why would a physician prescribe a bisimilar? 6. Take home message
37

Acceptance of a new drug
Affinity with the existing product (Innovator brand) (= current value, including habit)
Versus Attractiveness of the alternative (biosimilar) (= it implies a change with uncertain outcome)
Without an incentive for change,
A physician will not change it’s prescribing habits
Drug prescribing is highly emotion and information driven Where to obtain convincing information?
38

We perceive an information gap
EMA’s EPAR (50+ pages) is difficult to read / understand for a busy healthcare professional
Need support to understand the comparability excercise
Is a snapshot in time with no updates
No access to risk management information / PSUR’s
Research findings should be published and made accesible
Please use open-access publications
Clinical trials scattered and not easily accesible 39

Take home message: what we need to do
Educate health-care professionals on
How the similarity excercise works
Science based and transparant
Paradigm shift
Classical “evidence based’ thinking is not valid for biosimilars
Focus on high-tech analytical techniques and science
Clinical trial for confirmation, not for proof
How extrapolation of indications is justified
Acceptance by prescribers will be dependent on the understanding of the development model and accepting principles of extrapolation
40

Thank you for your attention
Contact: [email protected] 41
GaBI is supporting you
Please support GaBI

42