Embed Size (px)
Citation preview

Biosimilar Development: Design and Statistical Challenges
Moumita Sinha, PhD
Biocon Ltd
IASCT, Annual Conference, 2012
5/17/2012 Biocon Limited 1

Outline of Talk
• What is a Biosimilar?
• Guidelines on Biosimilars
• Clinical Studies in Human – PK/PD
– Immunogenicity
– Safety/Efficacy
• Case Study – Avastin
• Challenges
5/17/2012 Biocon Limited 2

Kozlowski et al, 2011, NEJM. 5/17/2012 Biocon Limited 3
Biologics

FDA Definition Biosimilar or biosimilarity means that “the biological product is highly similar to the reference product notwithstanding minor differences in clinically inactive components,” and that “there are no clinically meaningful differences between the biological product and the reference product in terms of the safety, purity, and potency of the product WHO Definition A biotherapeutic product which is similar in terms of quality, safety and efficacy to an already licensed reference biotherapeutic product.
Biosimilar Definition
5/17/2012 Biocon Limited 5

5/17/2012 Biocon Limited 6
Biosimilarity

Dranitsaris et al, 2011. 5/17/2012 Biocon Limited 7

Biologics going off patent
Drug Earliest Patent expiry date Rituximab: Rituxan/Mabthera 2013
Cetuximab: Erbitux 2014
Infliximab: Remicade 2014
Trastuzumab: Herceptin 2014
Palivizumab: Synagis 2015
Adalimumab: Humira 2016
Denosumab: Prolia 2017
Natalizumab: Tysabri 2017
Omalizumab: Xolair 2018
Bevacizumab: Avastin 2019
Ranibizumab: Lucentis 2019
Ipilimumab: Yervoy 2022
5/17/2012 Biocon Limited 8

Biosimilar Development Guidelines
• WHO (2009) – Guidelines on Evaluation of Similar Biotherapeutic Products
• EMA Draft Guideline (2010) - Guideline on similar biological medicinal products containing monoclonal antibodies
• FDA Draft Guidelines(2012) – Scientific Considerations in Demonstrating Biosimilarity to a Reference Product
• No one size fits all approach • “Totality of Evidence” – Stressed by FDA for approval of Biosimilars • Risk based approach • Step by step evaluation of biosimilarity to clear residual uncertainity 5/17/2012 Biocon Limited 9

5/17/2012 Biocon Limited 10
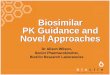
Scientific Considerations: FDA Draft Guidance

5/17/2012 Biocon Limited 11
Data Driven Decisions

PK/PD Study
• Comparative PK and PD (if relevant markers are available) in sensitive population
• Sponsors should predefine and justify the criteria for selection of study population and parameters
• Current knowledge of the inter-subject and intra-subject variability for human PK and PD for the reference product
• Establishing similar PK/PD profile as the reference product contributes to the demonstration of biosimilarity and may provide a scientific basis for a selective and targeted approach to subsequent clinical testing
• Important factors to be considered for PK/PD studies are: – Clinically relevant PK and PD parameters (different PD measures that assess different domains
of activities may be of value) – Populations, doses(s) and route of administration that are the most sensitive to detect
differences in PK and PD profiles – Sensitive and relevant assays
5/17/2012 Biocon Limited 12

Immunogenicity Study
• Establishing that there are no clinically meaningful differences in immune responses between a proposed product and reference product is a key element
• If clinical consequence is severe, extensive immunogenicity assessments will likely be required
• If immune response to reference product is rare – Pre-market study powered to detect major differences
– Post market study to detect more subtle differences
• Recommended to use a parallel design – One-sided design is sufficient
– Acceptable differences in immune response parameters to be discussed with FDA in advance
• Most sensitive study population and treatment regimen
• Follow up period to be determined carefully – Chronically administered agents should be one year unless a shorter duration can be justified by
sponsor
5/17/2012 Biocon Limited 13

Clinical Safety/Efficacy Study
• Decreased activity – Preclude licensure of the proposed product
• Increased activity – Might be associated with more adverse event
– Might suggest product should be treated as entirely different product and different licensure pathway should be used
• Most straightforward approach: An equivalence design with scientifically justified margins and the bounds of the margin are same – Different upper and lower bound may be appropriate
– One-sided non-inferiority design may be appropriate • If it is well established that doses of the reference product higher than that
recommended in labeling don’t create safety concerns
• This will allow smaller sample size for clinical study
5/17/2012 Biocon Limited 14

Clinical Safety/Efficacy Study
• A sponsor can use endpoints that are different from those in the reference product’s clinical trials if they are scientifically justified
• EMA: – Preferred endpoint for efficacy in oncology is PFS/DFS/OS
– Long trial duration, may be suitable for certain indications
– May not be suitable to establish similar efficacy between Biosimilar product and reference mAb
– A clinical endpoint that measures activity may be used as primary endpoint, for example Overall Response Rate (ORR), ORR at a specific timepoint, percent change in tumor mass from baseline
5/17/2012 Biocon Limited 15

AVASTIN CASE STUDY
5/17/2012 Biocon Limited 16

Avastin Trial Design Glioblastoma
• The primary objective was to evaluate ORR and 6-month PFS by independent review in patients with glioblastoma in first or second relapse
• Non-comparative design – Two arms each with Avastin;
– Avastin (85 patients)
– Avastin+ Irinotecan (82 patients)
• Results compared to historical trials (Assumed historical control rate 5%)
5/17/2012 Biocon Limited 17

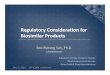
Progression Free Survival
5/17/2012 Biocon Limited 18
Assumed historical control rate: 15%

Challenges in Designing a Clinical Trial for Biosimilar Development
5/17/2012 Biocon Limited 19
• Consider using PFS at six month as an endpoint
• Response rate in Avastin arm is 42.6% – Historical control rate is 15%
– M1= 27.6
– M2=13.8 (preserving 50% effect)
• For 90% power and alpha=5% sample sizes required
– Equivalence Trial :334 (668)
– Non-inferiority Trial : 270 (540)

Challenges in Designing a Clinical Trial for Biosimilar Development
5/17/2012 Biocon Limited 20
• Consider using ORR as an endpoint
• Response rate in Avastin arm is 28.2% – Historical control rate is 5%
– M1= 23.2
– M2=11.6 (preserving 50% effect)
• For 90% power and alpha=5% sample sizes required
– Equivalence Trial :392 (784)
– Non-inferiority Trial : 317 (634)

Challenges
• Choice of Endpoint
• Margin determination – Statistical or Clinical Reasoning
• Sample Size
• Reference Product Cost
• High trial cost and long recruitment period erodes biosimilar price advantage for patients
5/17/2012 Biocon Limited 21

Thank You
5/17/2012 Biocon Limited 22