Embed Size (px)
Citation preview
INTERVENTIONAL CARDIOLOGY 201732ND ANNUAL INTERNATIONAL SYMPOSIUM32 ANNUAL INTERNATIONAL SYMPOSIUM
Bioresorbable Stents Update: Similaritiesand Differences in Comparison to Firstand Differences in Comparison to First
Generation BVS
DariuszDariusz DudekDudek
InstituteInstitute ofof CardiologyCardiologyInstituteInstitute ofof CardiologyCardiology
JagiellonianJagiellonian UniversityUniversity, Kraków, Poland, Kraków, Poland
Chair,Chair, NationalNational CardiacCardiac SocietiesSocieties & International& International AffairsAffairs CommitteeCommittee
TheThe EuropeanEuropean AssociationAssociation ofof PercutaneousPercutaneous CardiovascularCardiovascular InterventionsInterventions (EAPCI ESC)(EAPCI ESC)
Our experience with BVS over 10 years
• Progressive expansion of angiographic indications fromvery simple lesion type A (ACC/AHA)very simple lesion type A (ACC/AHA)to lesions type C (long lesions), different clinical settings
• FDA approved Absorb in 2016
• ST up to 3% but proper technique reduces risk of ST• ST up to 3% but proper technique reduces risk of STup to 70%
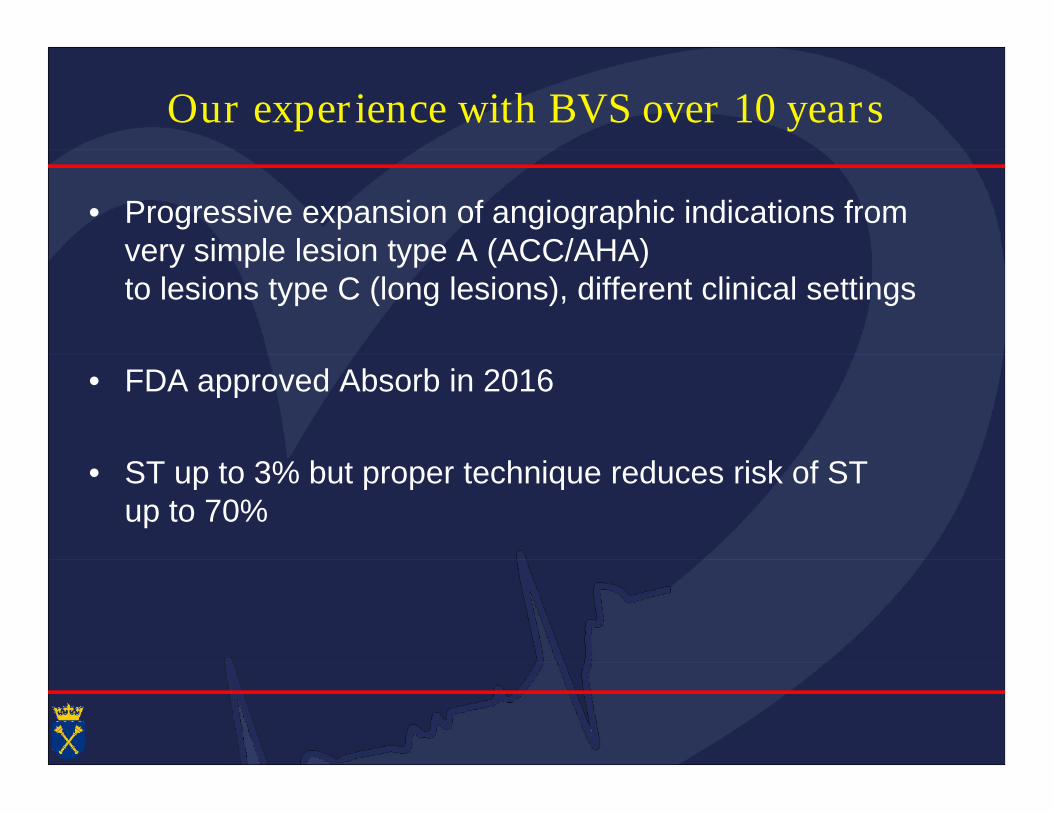
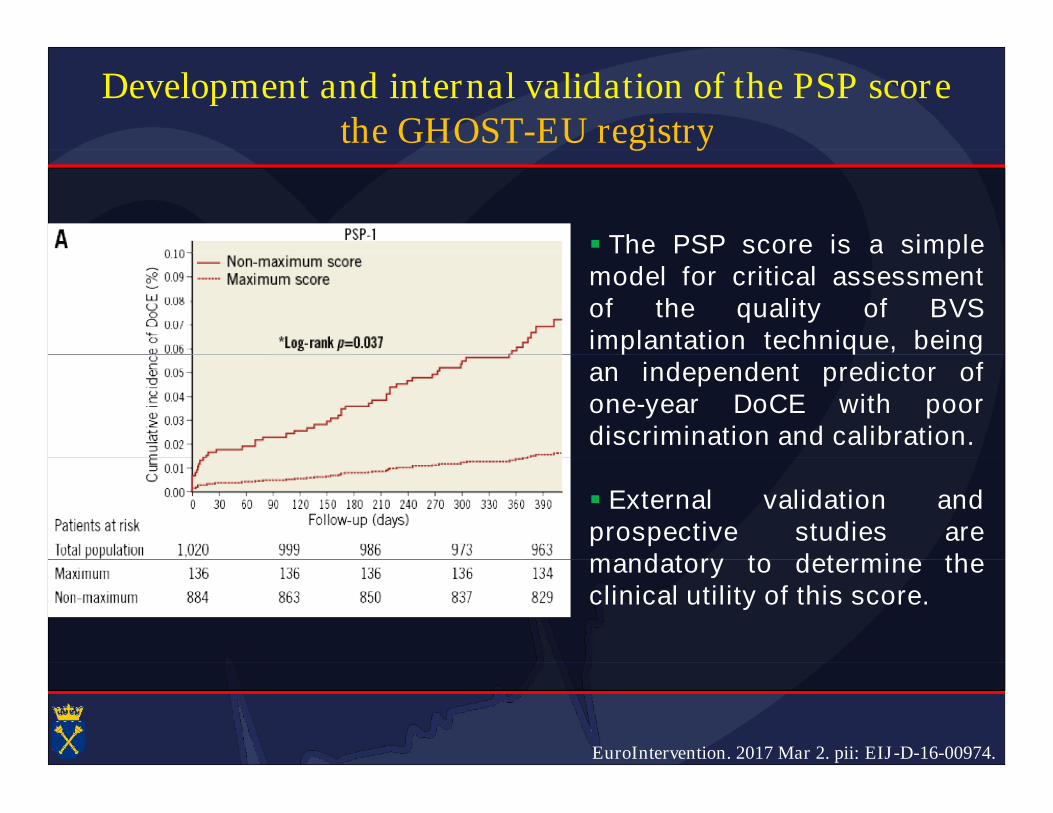
Development and internal validation of the PSP scorethe GHOST-EU registrythe GHOST-EU registry
Predilation, correct Scaffold sizing, and Post-dilation with a non-compliant balloon were performed in 95.7%, 50.2%, and 26.2% of thecases and scored 0.63, 1.96 and 1.93 points, respectively, in the PSP-1cases and scored 0.63, 1.96 and 1.93 points, respectively, in the PSP-1model.
EuroIntervention. 2017 Mar 2. pii: EIJ-D-16-00974.
Development and internal validation of the PSP scorethe GHOST-EU registrythe GHOST-EU registry
The PSP score is a simple The PSP score is a simplemodel for critical assessmentof the quality of BVSimplantation technique, beingimplantation technique, beingan independent predictor ofone-year DoCE with poordiscrimination and calibration.
External validation andprospective studies aremandatory to determine themandatory to determine theclinical utility of this score.
EuroIntervention. 2017 Mar 2. pii: EIJ-D-16-00974.
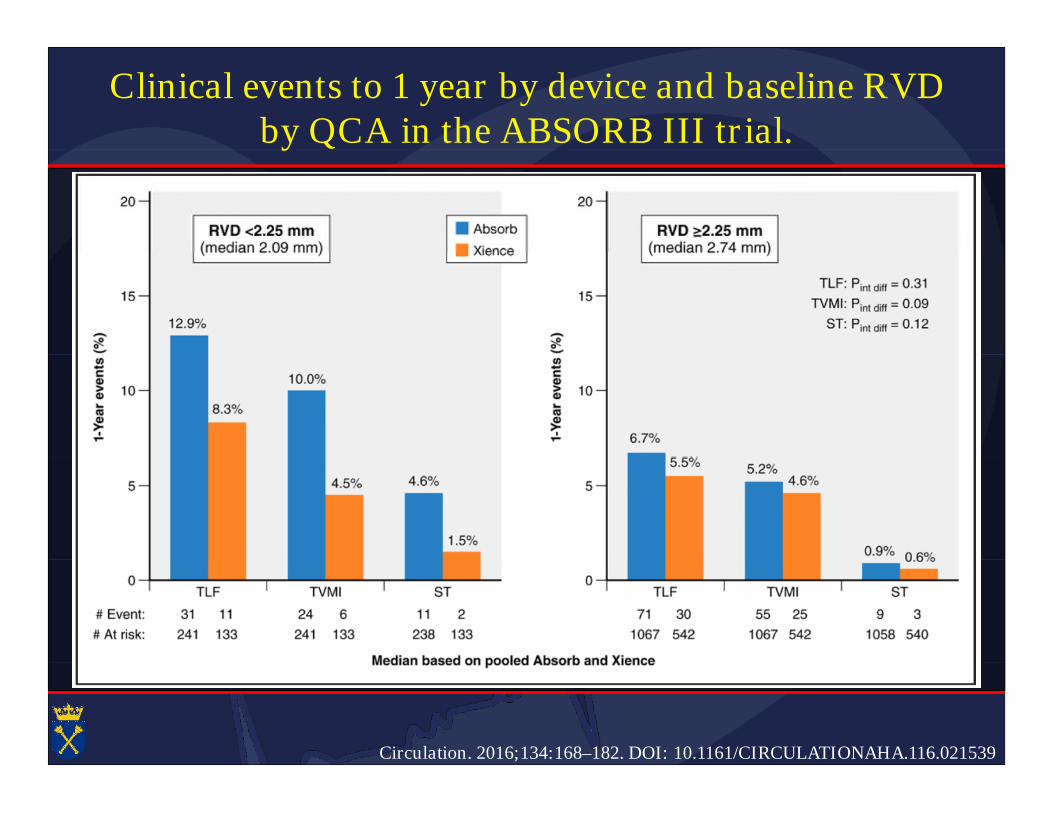
Clinical events to 1 year by device and baseline RVDby QCA in the ABSORB III trial.by QCA in the ABSORB III trial.
Circulation. 2016;134:168–182. DOI: 10.1161/CIRCULATIONAHA.116.021539
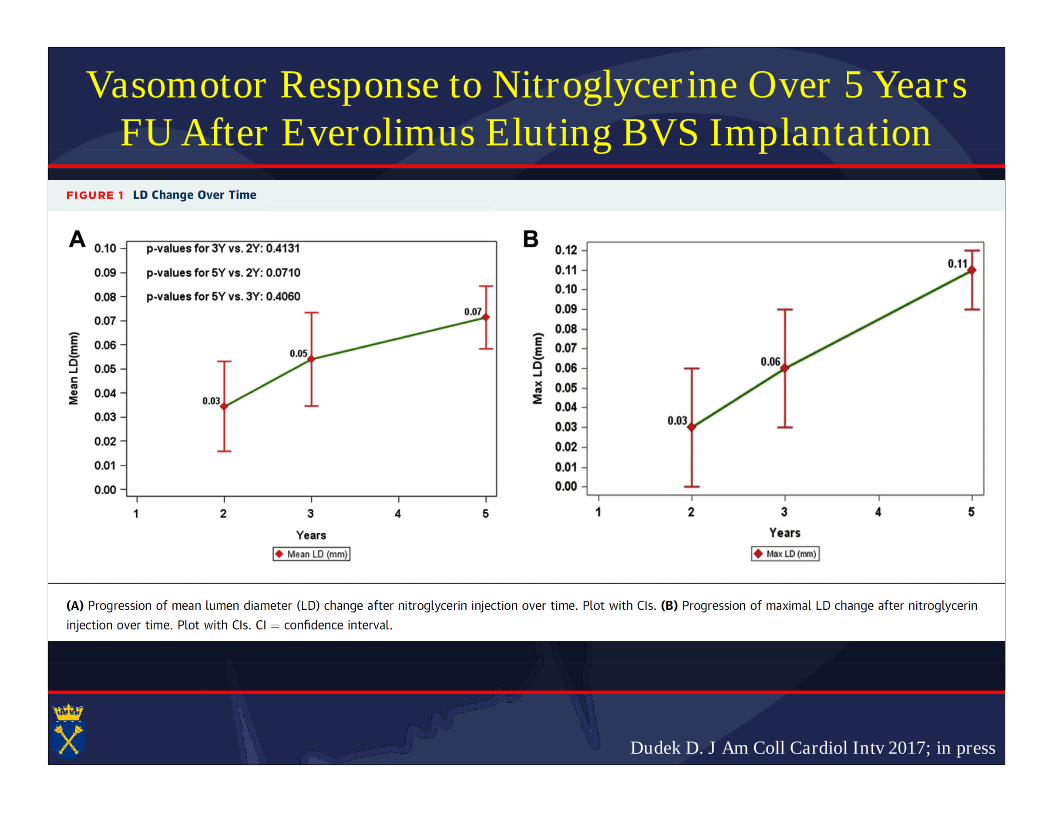
Vasomotor Response to Nitroglycerine Over 5 YearsFU After Everolimus Eluting BVS ImplantationFU After Everolimus Eluting BVS Implantation
Absorb Cohort B (n=101)
Group B1 (n=45): with invasive follow up at 6 and 24 months
Group B2 (n=56): with control imaging procedures at 12 and 36monthsmonths
6 month evaluation excluded (Nitroglicerine test performed afterAch infusion)
Dudek D. J Am Coll Cardiol Intv 2017; in press
Vasomotor Response to Nitroglycerine Over 5 YearsFU After Everolimus Eluting BVS ImplantationFU After Everolimus Eluting BVS Implantation
Dudek D. J Am Coll Cardiol Intv 2017; in press
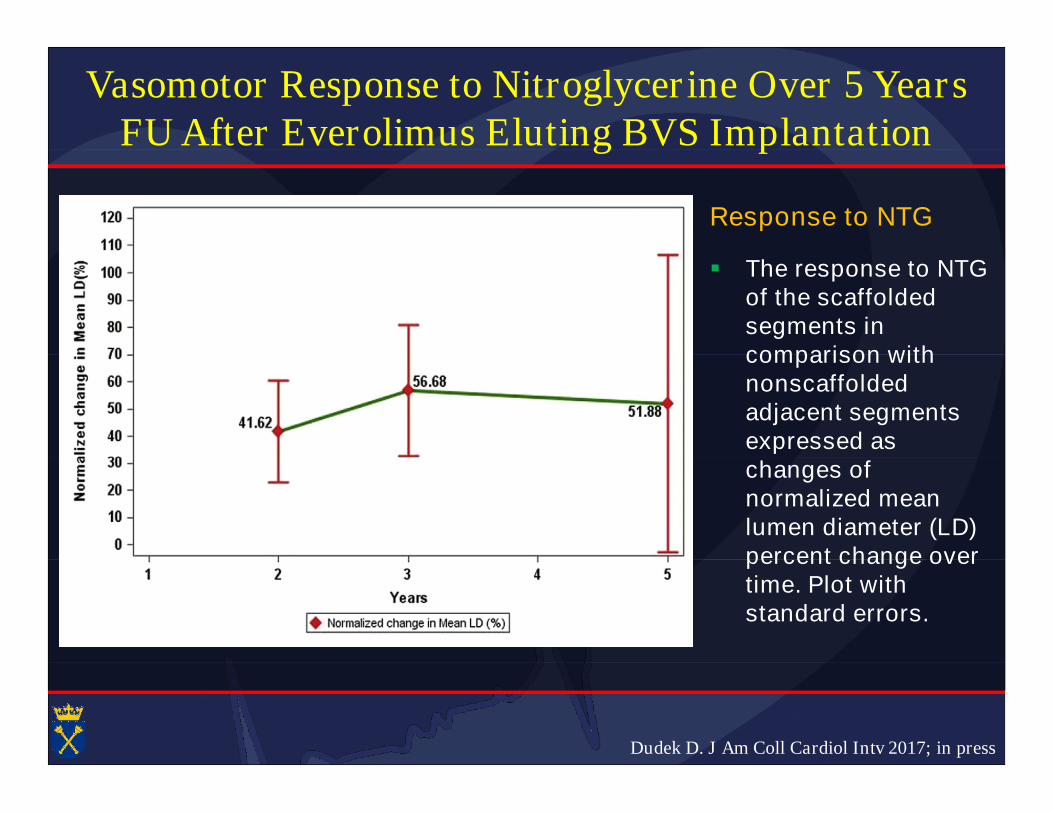
Vasomotor Response to Nitroglycerine Over 5 YearsFU After Everolimus Eluting BVS ImplantationFU After Everolimus Eluting BVS Implantation
Response to NTG
The response to NTGof the scaffoldedsegments incomparison withcomparison withnonscaffoldedadjacent segmentsexpressed aschanges ofchanges ofnormalized meanlumen diameter (LD)percent change overpercent change overtime. Plot withstandard errors.
Dudek D. J Am Coll Cardiol Intv 2017; in press
Dudek D. J Am Coll Cardiol Intv 2017; in press
Vasomotor Response to Nitroglycerine Over 5 YearsFU After Everolimus Eluting BVS ImplantationFU After Everolimus Eluting BVS Implantation
WHAT IS KNOWN? The appearance of vasomotility up to 2 years afterABSORB implantation was previously shown.ABSORB implantation was previously shown.
WHAT IS NEW? We have not found improvement in response to NTGusing mean lumen diameter change by QCA. Only the maximal LDchange increased significantly. This suggests a trend towardchange increased significantly. This suggests a trend towardvasomotor recovery in 5-year follow-up, which is consistent with theprogressive degradation and bioresorption of the scaffold; however,the degree of response to NTG remained lower than in adjacentthe degree of response to NTG remained lower than in adjacentsegments.
WHAT IS NEXT? Different stimulation agents and/or differentmethodology should be applied in further studies to verify thesemethodology should be applied in further studies to verify thesefindings.
Dudek D. J Am Coll Cardiol Intv 2017; in press
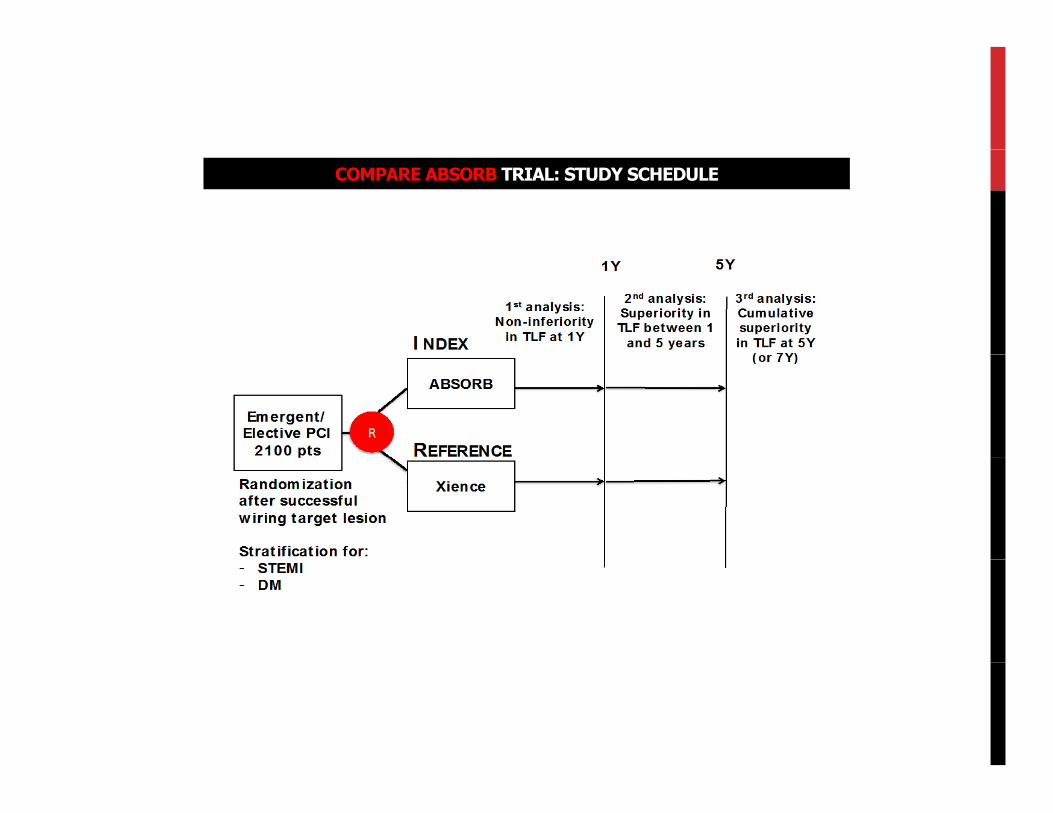
COMPARE ABSORB TRIAL: STUDY SCHEDULE
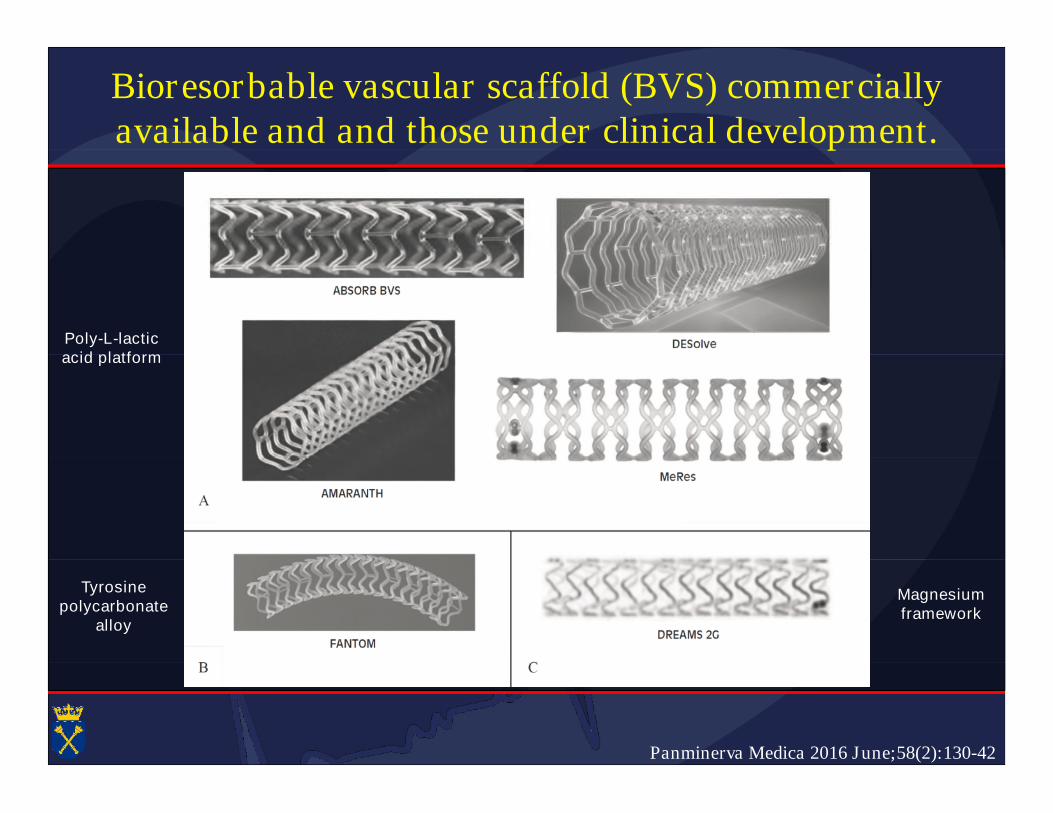
Bioresorbable vascular scaffold (BVS) commerciallyavailable and and those under clinical development.available and and those under clinical development.
Poly-L-lacticacid platformacid platform
Magnesiumframework
Tyrosinepolycarbonate
alloy
Panminerva Medica 2016 June;58(2):130-42
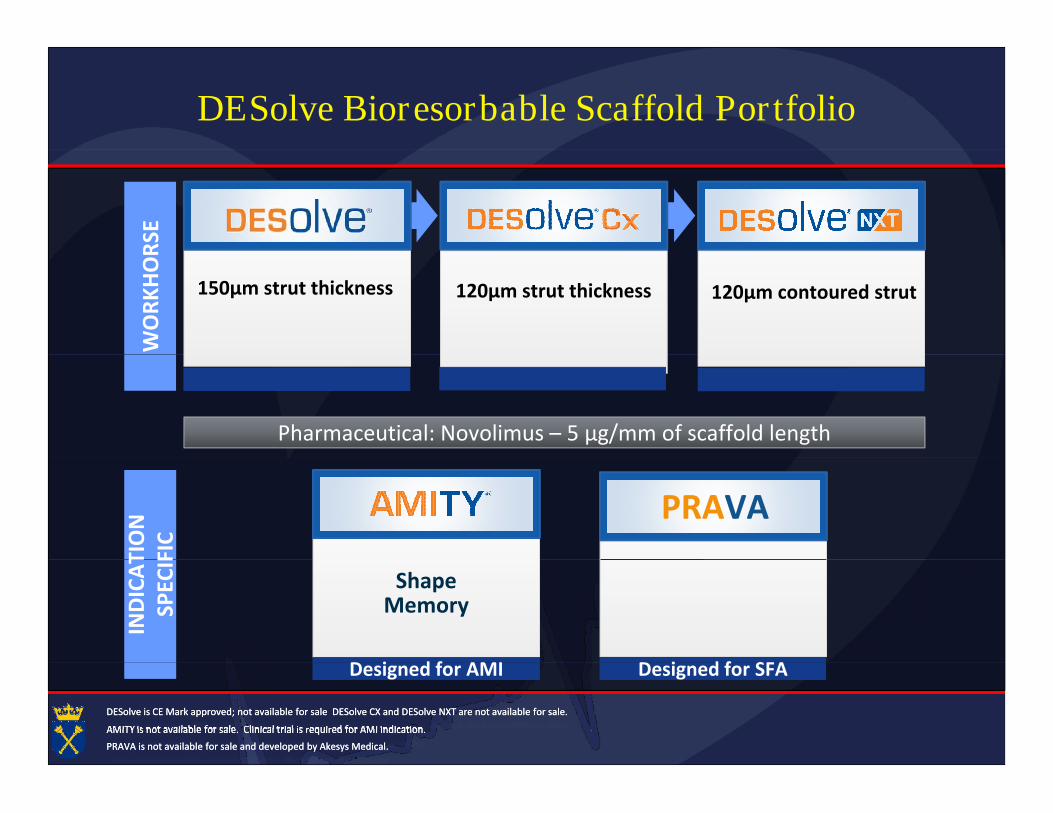
DESolve Bioresorbable Scaffold PortfolioW
OR
KH
OR
SEW
OR
KH
OR
SE
120µm strut thickness 120µm contoured strut150µm strut thickness
Pharmaceutical: Novolimus – 5 µg/mm of scaffold length
IND
ICA
TIO
NSP
ECIF
IC
PRAVA
IND
ICA
TIO
NSP
ECIF
IC
Designed for AMI Designed for SFA
ShapeMemory
Designed for AMI Designed for SFA
AMITY is not available for sale. Clinical trial is required for AMI indication.AMITY is not available for sale. Clinical trial is required for AMI indication.
DESolve is CE Mark approved; not available for sale DESolve CX and DESolve NXT are not available for sale.DESolve is CE Mark approved; not available for sale DESolve CX and DESolve NXT are not available for sale.
PRAVA is not available for sale and developed by Akesys Medical.PRAVA is not available for sale and developed by Akesys Medical.
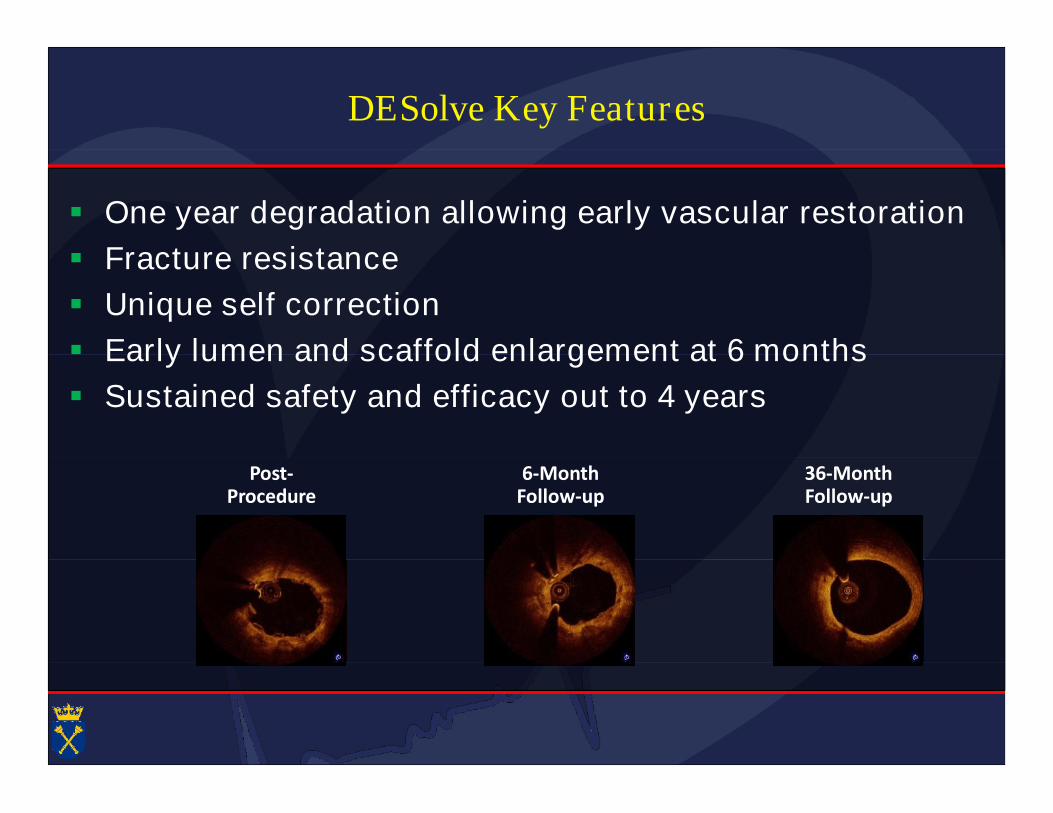
DESolve Key Features
One year degradation allowing early vascular restoration
Fracture resistance Fracture resistance
Unique self correction
Early lumen and scaffold enlargement at 6 months Early lumen and scaffold enlargement at 6 months
Sustained safety and efficacy out to 4 years
Post-Procedure
6-MonthFollow-up
36-MonthFollow-up
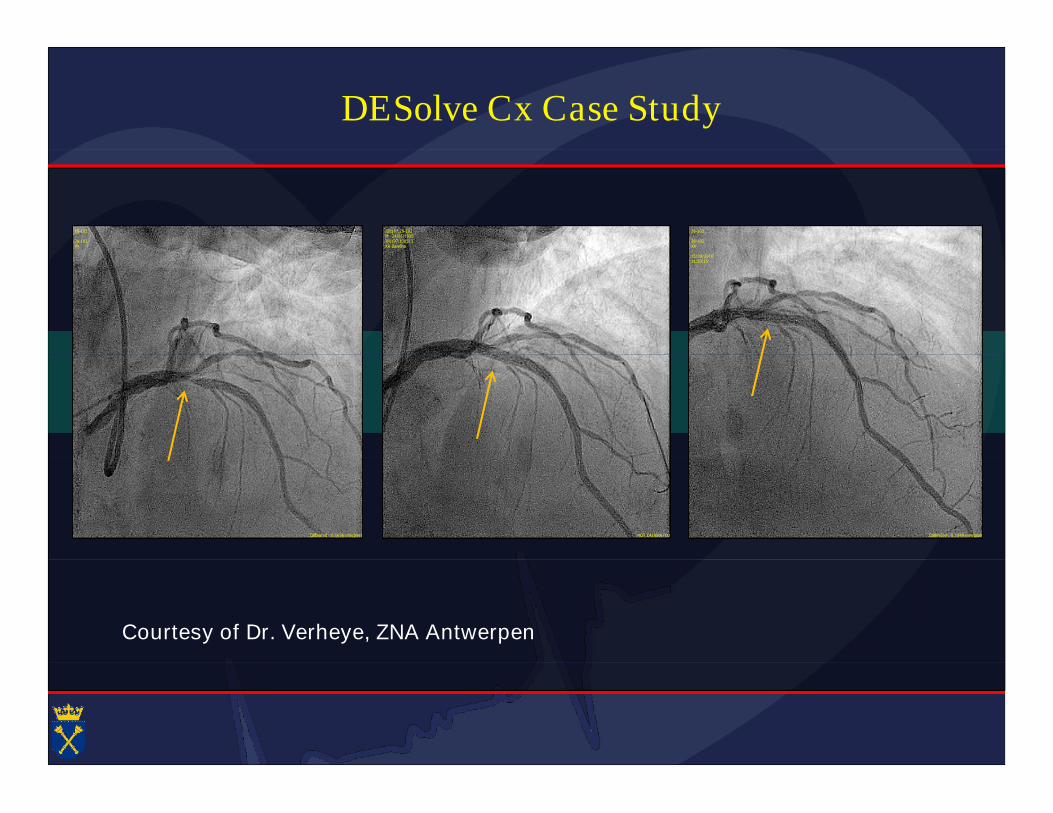
DESolve Cx Case Study
28-102
28-102XA
I00197.28-102M 24/05/1935I00197.138513XA Baseline
28-102
28-102XA
15/09/201611:20:15
Calibrated : 0.1636 mm/pixel NOT CALIBRATED Calibrated : 0.1849 mm/pixel
Courtesy of Dr. Verheye, ZNA Antwerpen
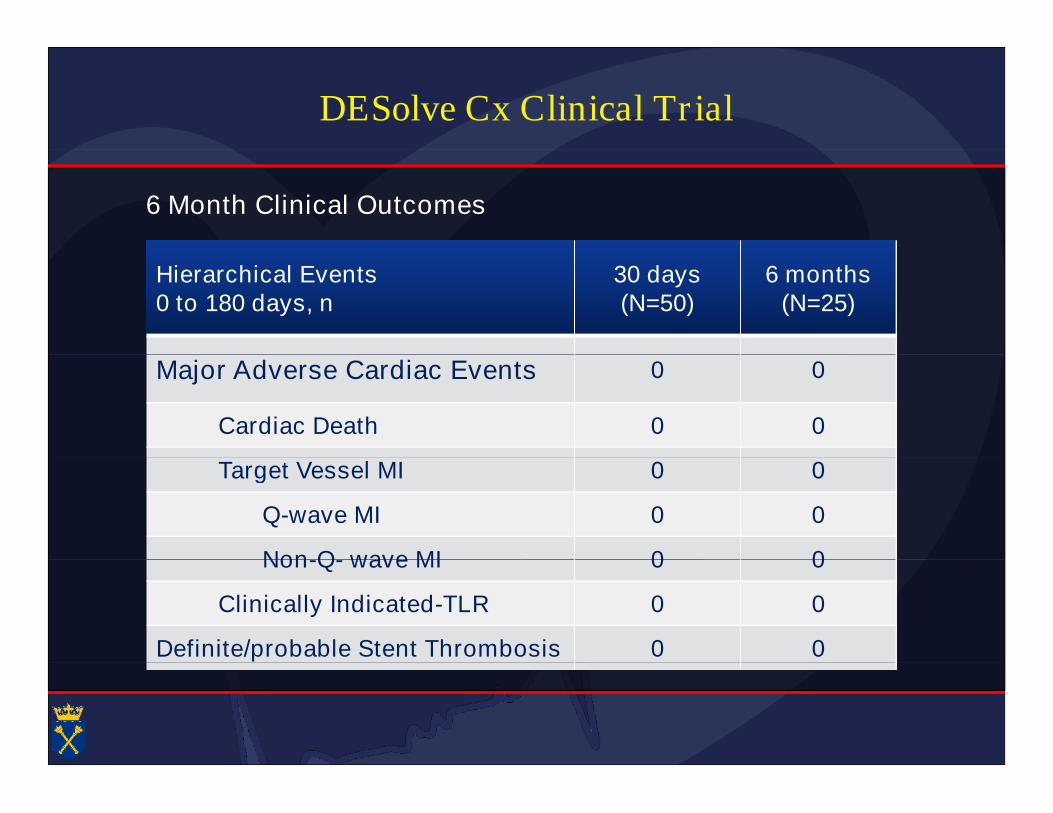
DESolve Cx Clinical Trial
6 Month Clinical Outcomes
Hierarchical Events0 to 180 days, n
30 days(N=50)
6 months(N=25)
Major Adverse Cardiac Events 0 0
Cardiac Death 0 0
Target Vessel MI 0 0Target Vessel MI 0 0
Q-wave MI 0 0
Non-Q- wave MI 0 0Non-Q- wave MI 0 0
Clinically Indicated-TLR 0 0
Definite/probable Stent Thrombosis 0 0
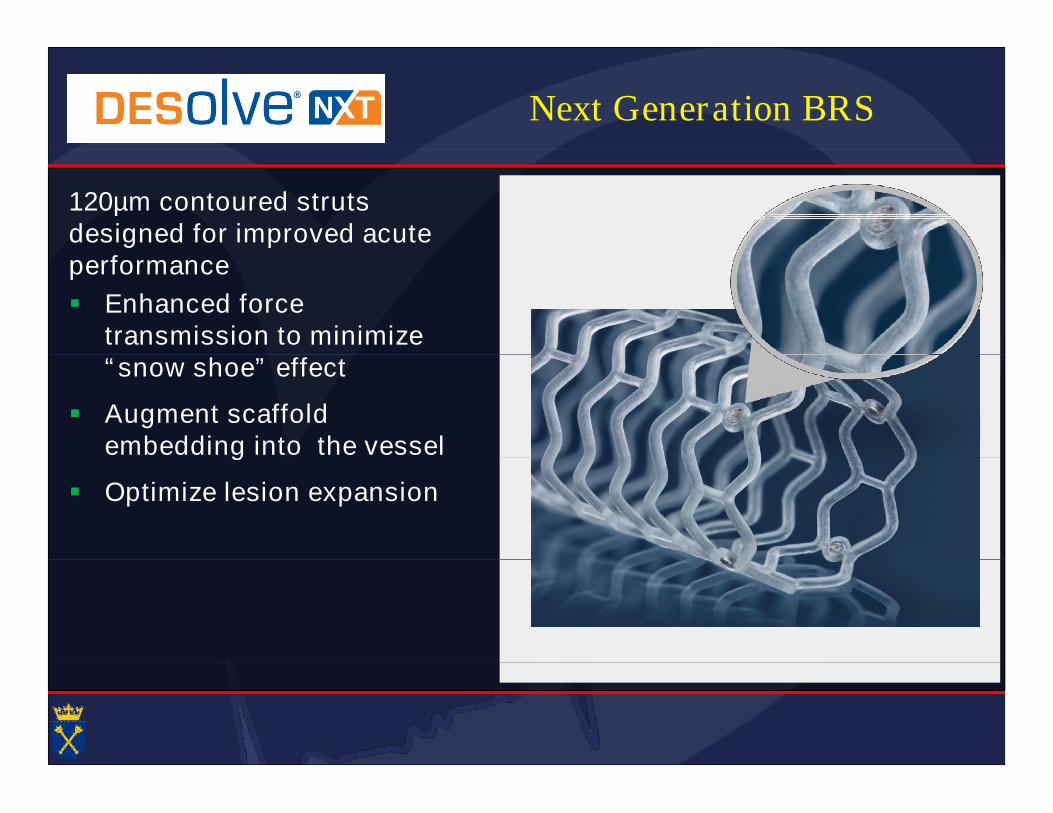
Next Generation BRS
120µm contoured strutsdesigned for improved acuteperformanceperformance
Enhanced forcetransmission to minimize“snow shoe” effect“snow shoe” effect
Augment scaffoldembedding into the vesselembedding into the vessel
Optimize lesion expansion
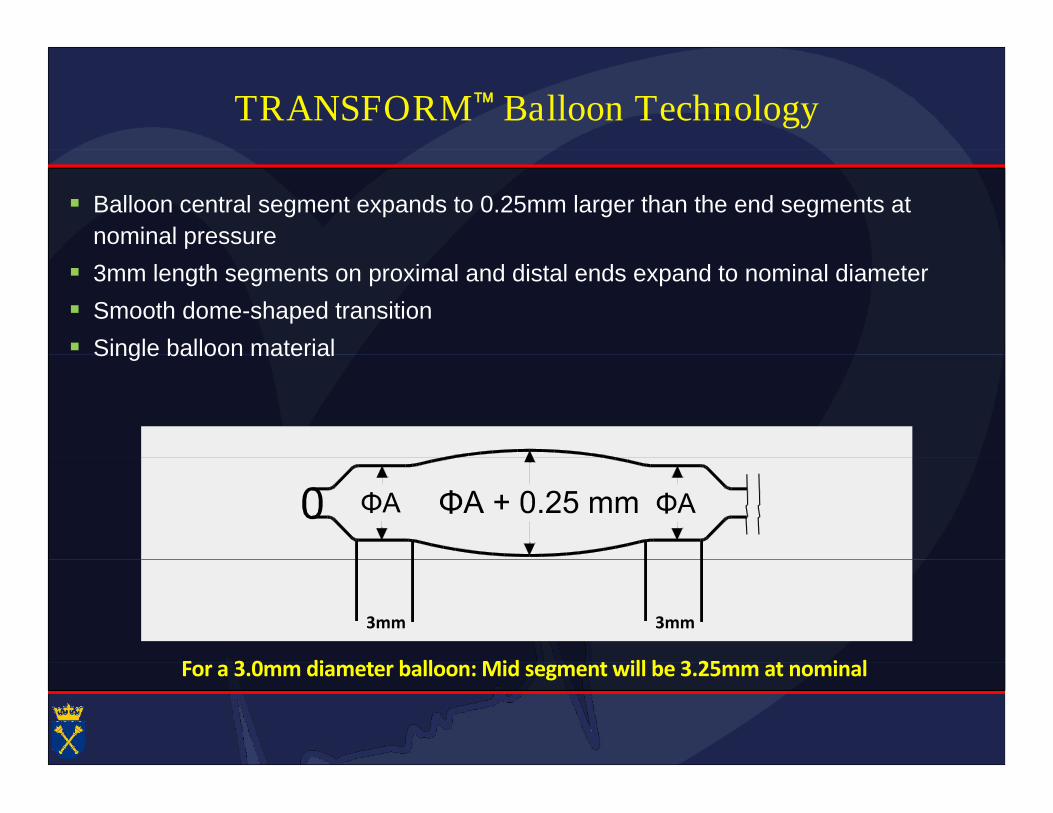
TRANSFORM Balloon Technology
Balloon central segment expands to 0.25mm larger than the end segments at
nominal pressure
3mm length segments on proximal and distal ends expand to nominal diameter
Smooth dome-shaped transition
Single balloon material Single balloon material
For a 3.0mm diameter balloon: Mid segment will be 3.25mm at nominal
3mm3mm
For a 3.0mm diameter balloon: Mid segment will be 3.25mm at nominal
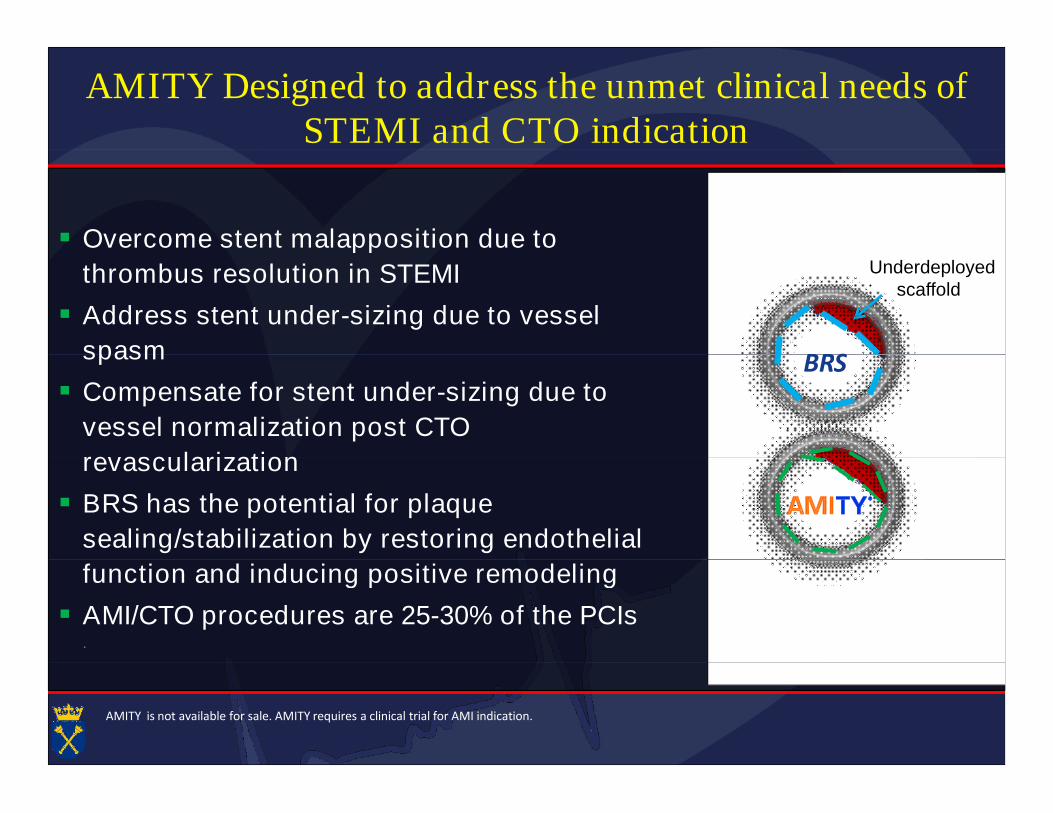
AMITY Designed to address the unmet clinical needs ofSTEMI and CTO indicationSTEMI and CTO indication
Overcome stent malapposition due to Overcome stent malapposition due to
thrombus resolution in STEMI
Address stent under-sizing due to vessel
spasm BRS
Underdeployedscaffold
spasm
Compensate for stent under-sizing due to
vessel normalization post CTO
revascularization
BRS
revascularization
BRS has the potential for plaque
sealing/stabilization by restoring endothelial
function and inducing positive remodeling
.
function and inducing positive remodeling
AMI/CTO procedures are 25-30% of the PCIs
AMITY is not available for sale. AMITY requires a clinical trial for AMI indication.
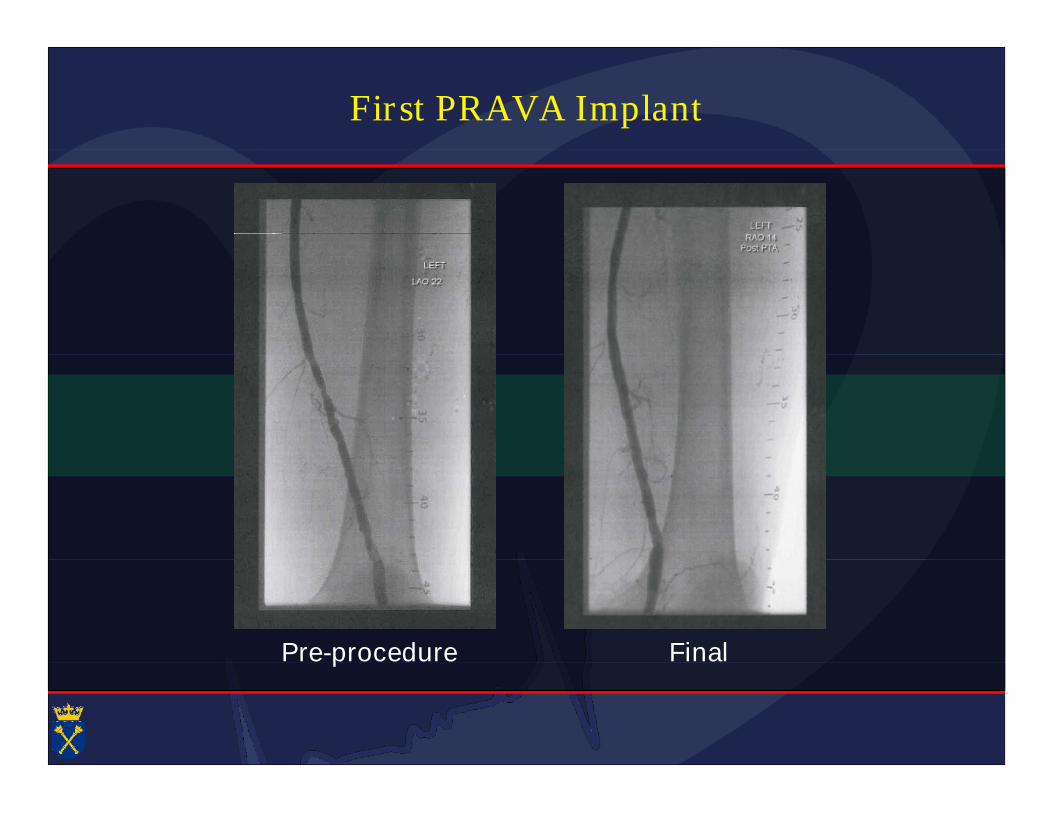
First PRAVA Implant
Pre-procedure FinalPre-procedure Final
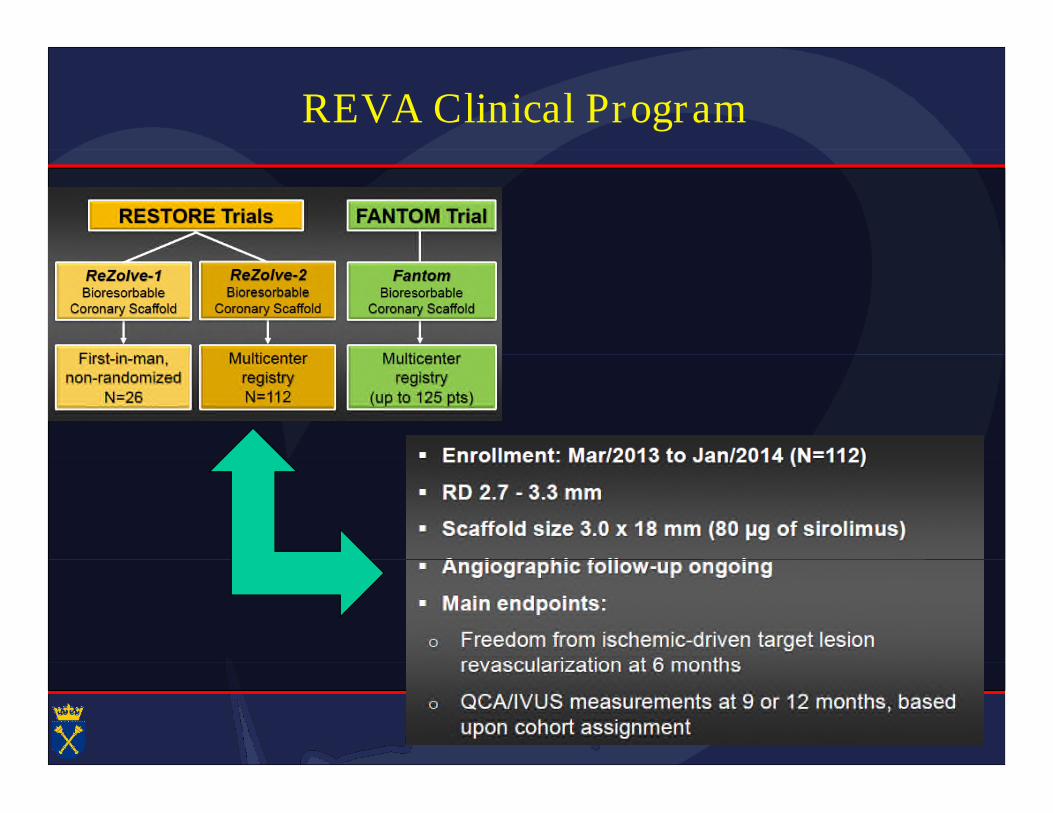
REVA Clinical Program
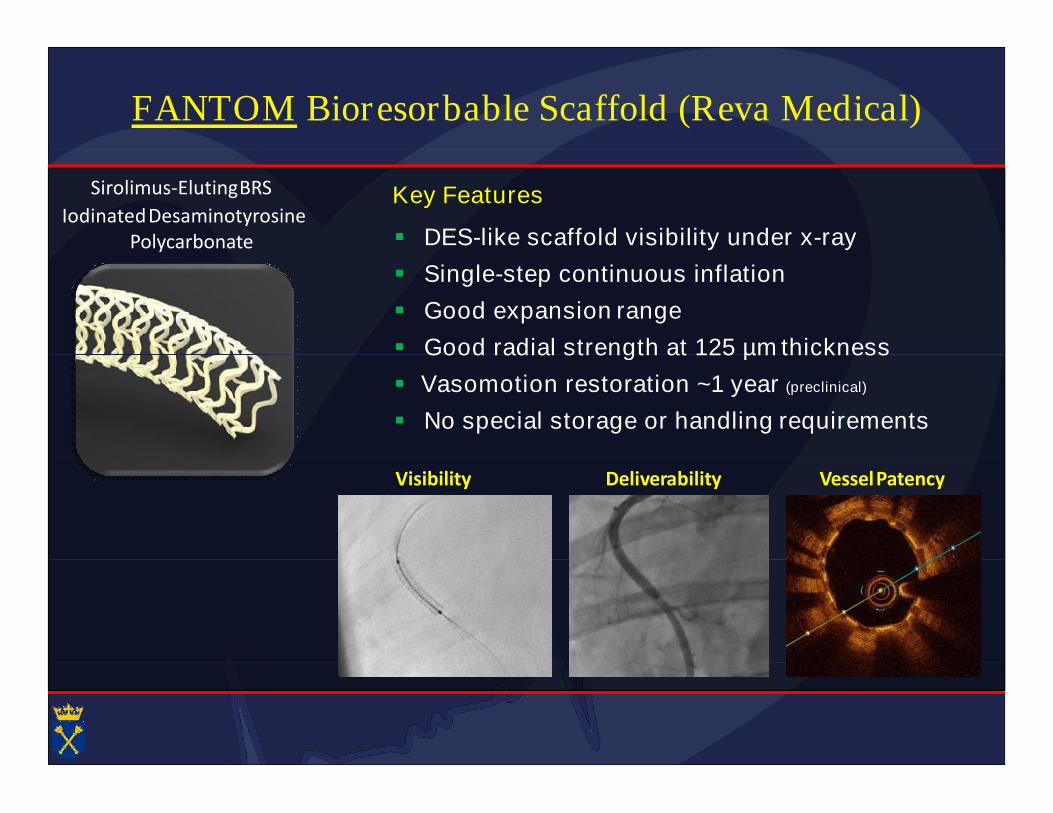
FANTOM Bioresorbable Scaffold (Reva Medical)
Sirolimus-ElutingBRS
IodinatedDesaminotyrosinePolycarbonate
Key Features
DES-like scaffold visibility under x-rayPolycarbonate
Single-step continuous inflation
Good expansion range
Good radial strength at 125 µmthickness Good radial strength at 125 µmthickness
Vasomotion restoration ~1 year (preclinical)
No special storage or handling requirements
Deliverability VesselPatencyVisibility
FANTOM BRS: Conclusions
Fantom offers new and clinically important features
Radiopacity Radiopacity
Deliverability
Single-step inflation
No special handling No special handling
Initial clinical data demonstrates:
Good acute performance Good acute performance
Enhanced device deliverability
Minimal residual stenosis and acute recoil (3%)
Sustained performance and safety through 6 months
Low MACE rate (2.1%) and scaffold thrombosis (0.4%)
Low late lumen loss (0.25mm) Low late lumen loss (0.25mm)
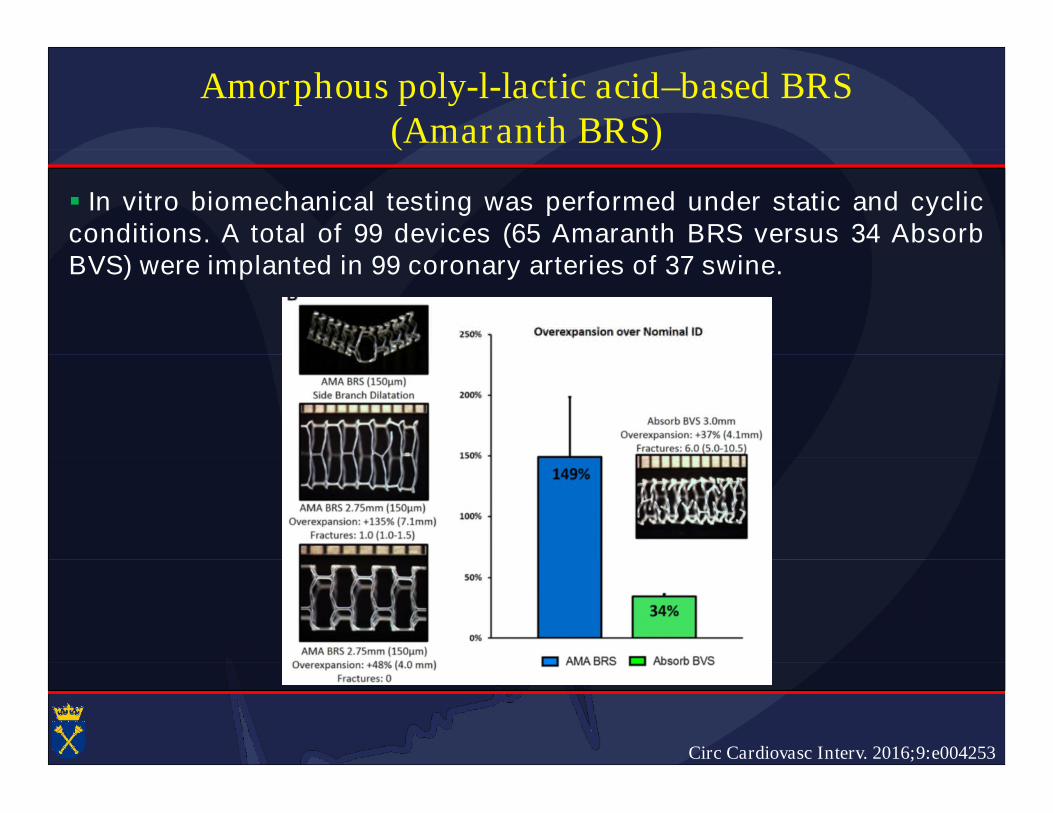
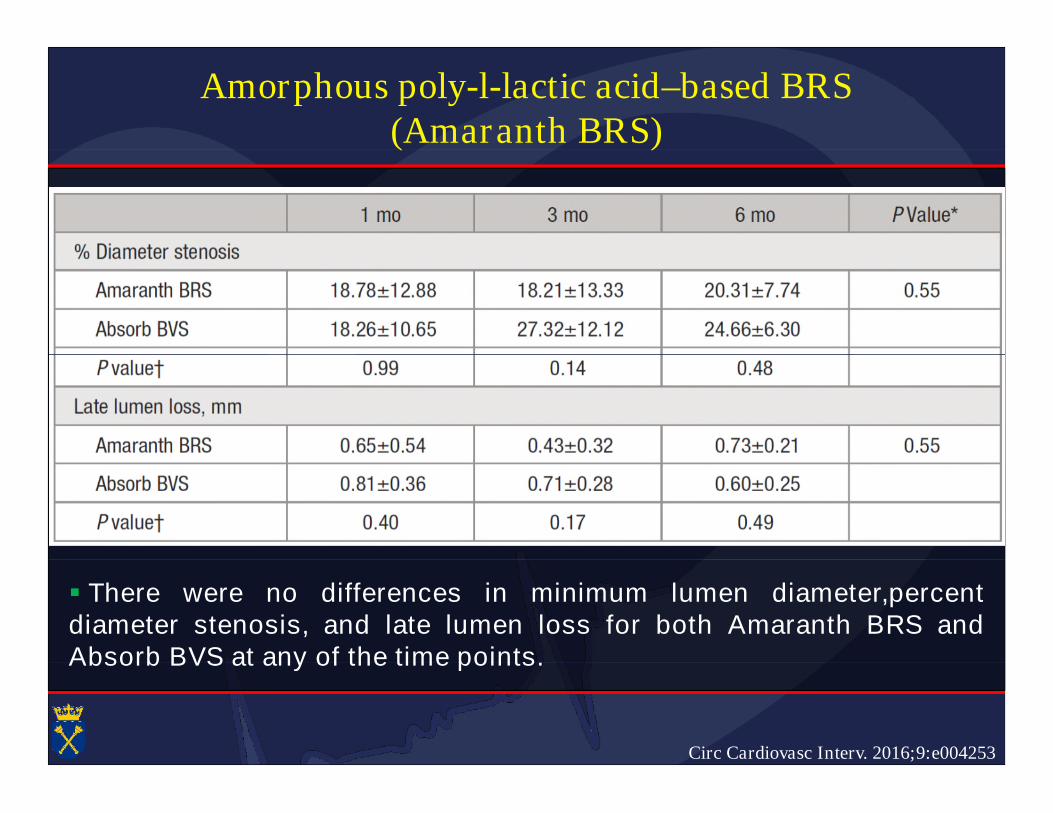
Amorphous poly-l-lactic acid–based BRS(Amaranth BRS)(Amaranth BRS)
In vitro biomechanical testing was performed under static and cyclicconditions. A total of 99 devices (65 Amaranth BRS versus 34 AbsorbBVS) were implanted in 99 coronary arteries of 37 swine.BVS) were implanted in 99 coronary arteries of 37 swine.
Circ Cardiovasc Interv. 2016;9:e004253
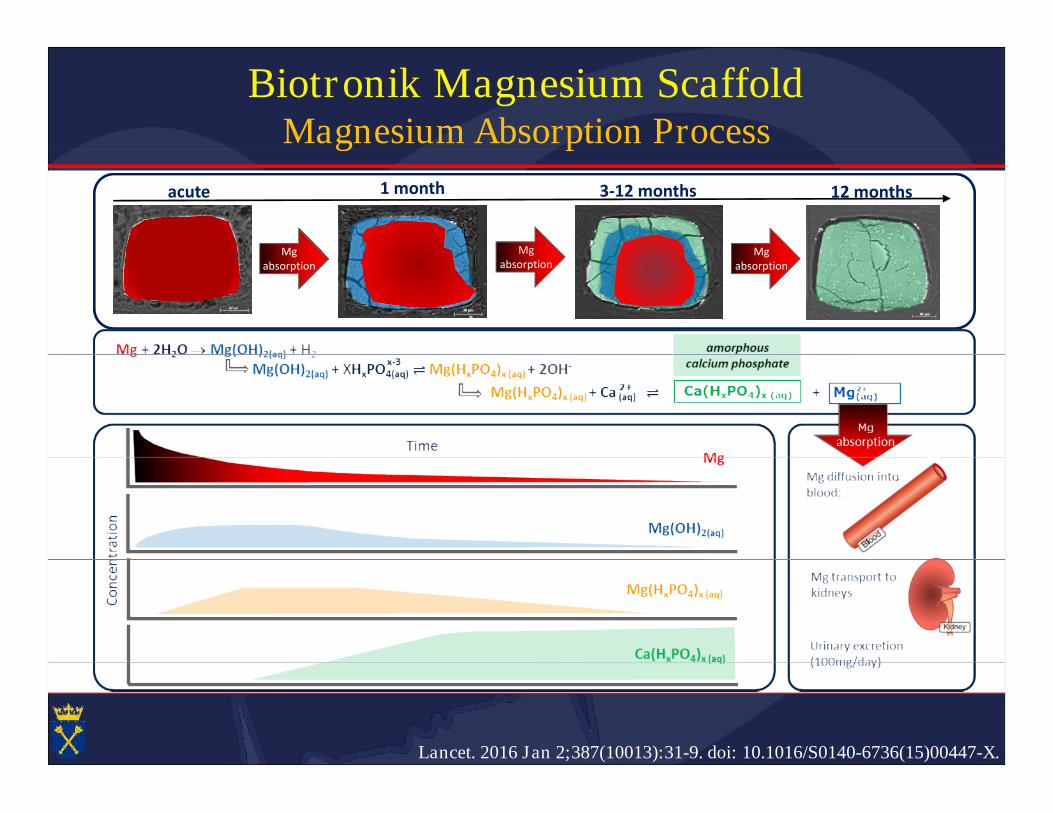
Biotronik Magnesium ScaffoldMagnesium Absorption ProcessMagnesium Absorption Process
acute 3-12 months 12 months1 month
Mg MgMg Mgabsorption
Mgabsorption
Mgabsorption
Lancet. 2016 Jan 2;387(10013):31-9. doi: 10.1016/S0140-6736(15)00447-X.
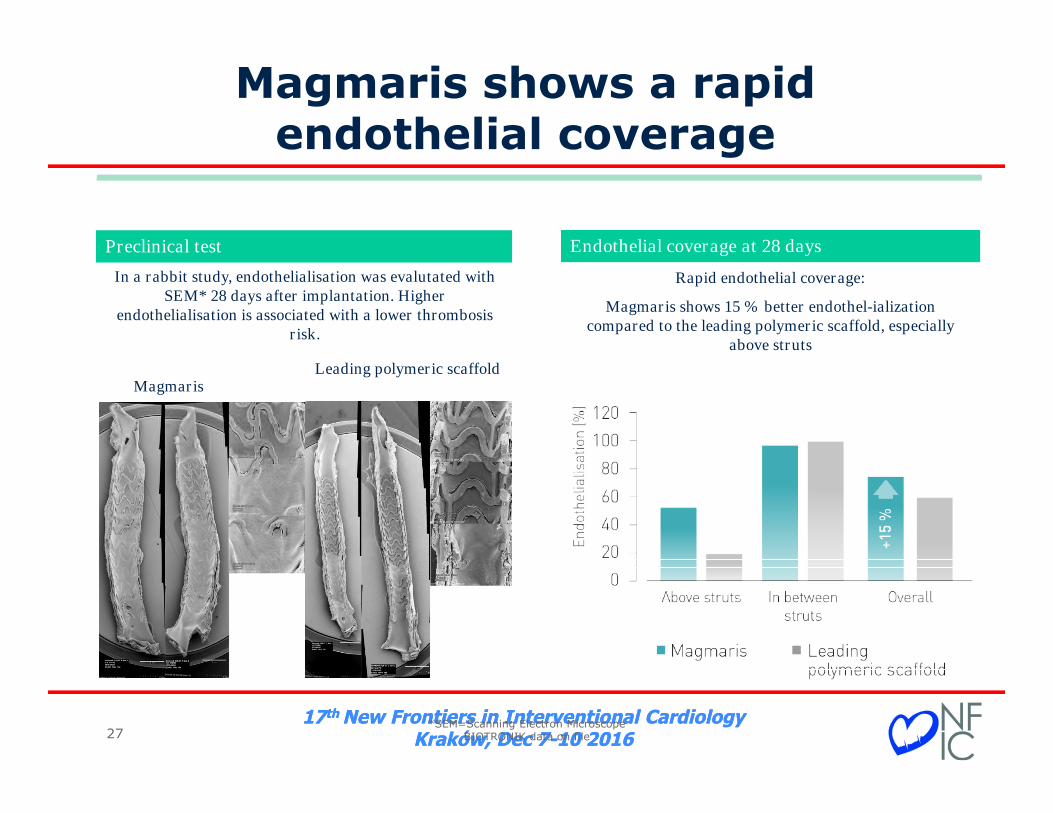
Magmaris shows a rapidendothelial coverageendothelial coverage
Endothelial coverage at 28 daysPreclinical test Endothelial coverage at 28 daysPreclinical test
Rapid endothelial coverage:
Magmaris shows 15 % better endothel-ializationcompared to the leading polymeric scaffold, especially
above struts
In a rabbit study, endothelialisation was evalutated withSEM* 28 days after implantation. Higher
endothelialisation is associated with a lower thrombosisrisk.
MagmarisLeading polymeric scaffold
17th New Frontiers in Interventional CardiologyKraków, Dec 7-10 2016
17th New Frontiers in Interventional CardiologyKraków, Dec 7-10 2016
CE mark pending
27*SEM=Scanning Electron Microscope
BIOTRONIK data on file
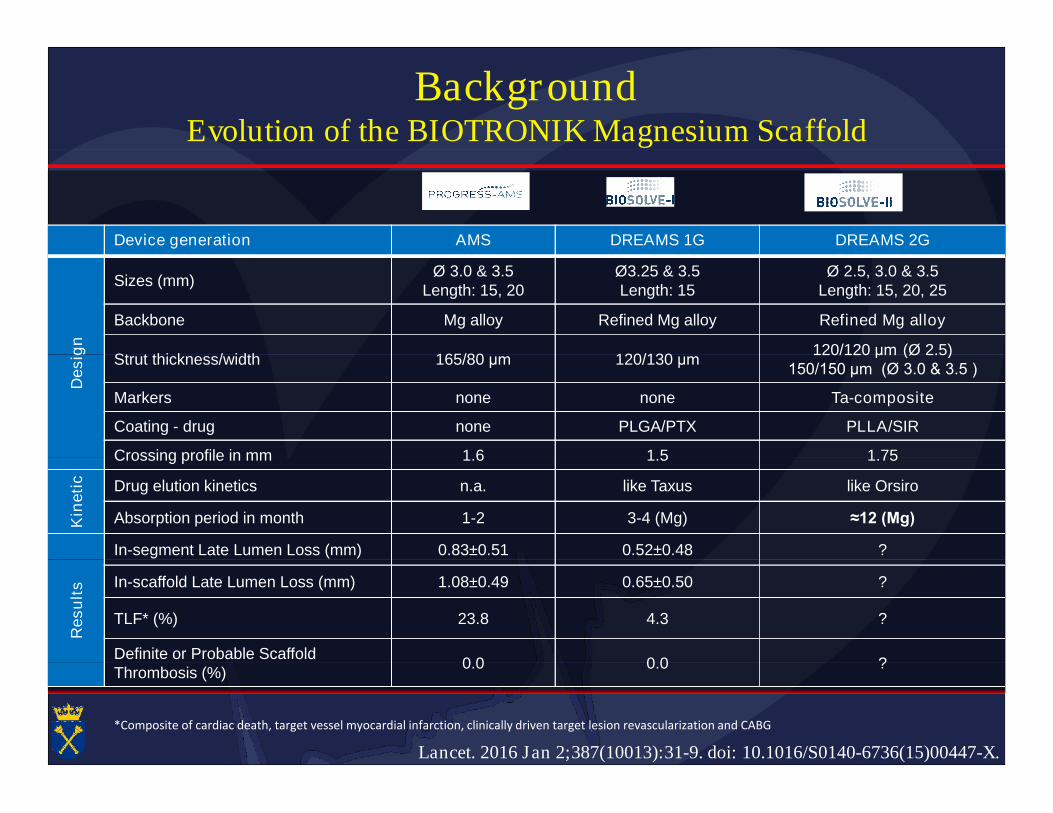
BackgroundEvolution of the BIOTRONIK Magnesium Scaffold
Device generation AMS DREAMS 1G DREAMS 2G
Desig
n
Sizes (mm)Ø 3.0 & 3.5
Length: 15, 20Ø3.25 & 3.5Length: 15
Ø 2.5, 3.0 & 3.5Length: 15, 20, 25
Backbone Mg alloy Refined Mg alloy Refined Mg alloy
Strut thickness/width 165/80 μm 120/130 μm120/120 μm (Ø 2.5)
Desig
n
Strut thickness/width 165/80 μm 120/130 μm120/120 μm (Ø 2.5)
150/150 μm (Ø 3.0 & 3.5 )
Markers none none Ta-composite
Coating - drug none PLGA/PTX PLLA/SIR
Crossing profile in mm 1.6 1.5 1.75Crossing profile in mm 1.6 1.5 1.75
Kin
eti
c Drug elution kinetics n.a. like Taxus like Orsiro
Absorption period in month 1-2 3-4 (Mg) ≈12 (Mg)
In-segment Late Lumen Loss (mm) 0.83±0.51 0.52±0.48 ?
Resu
lts In-scaffold Late Lumen Loss (mm) 1.08±0.49 0.65±0.50 ?
TLF* (%) 23.8 4.3 ?
Definite or Probable Scaffold0.0 0.0 ?
Lancet. 2016 Jan 2;387(10013):31-9. doi: 10.1016/S0140-6736(15)00447-X.
Definite or Probable ScaffoldThrombosis (%)
0.0 0.0 ?
*Composite of cardiac death, target vessel myocardial infarction, clinically driven target lesion revascularization and CABG
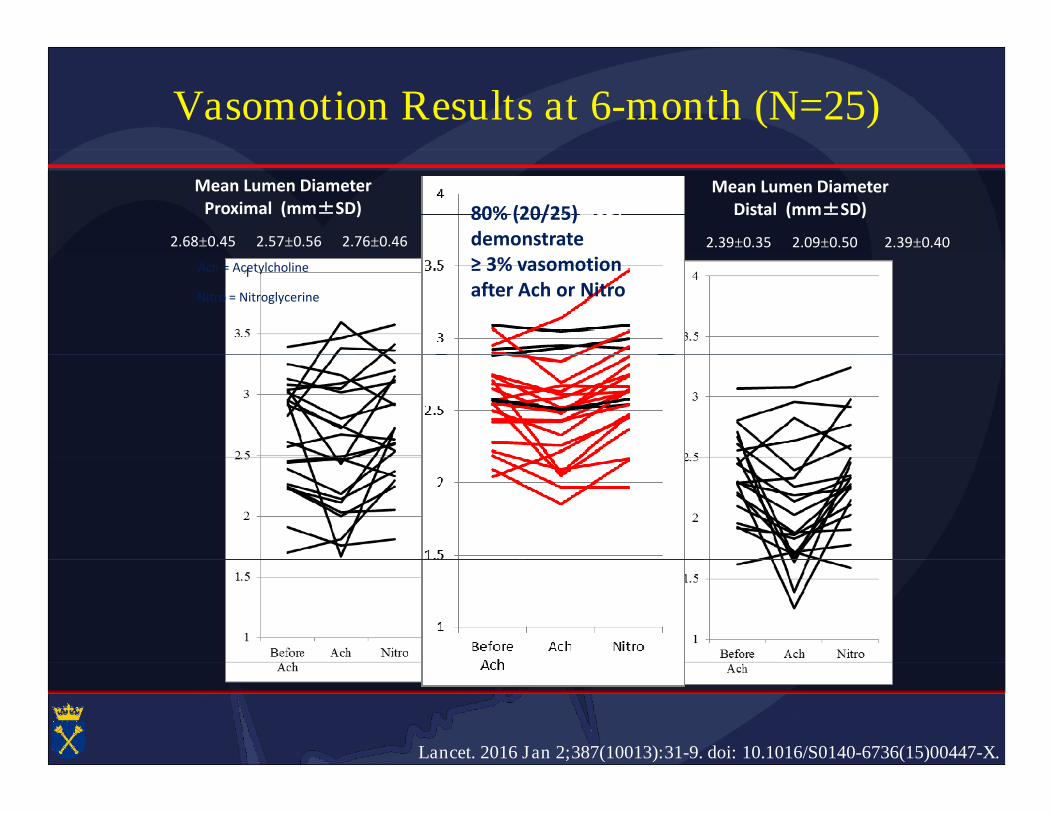
Vasomotion Results at 6-month (N=25)
Mean Lumen DiameterProximal (mm±SD)
Mean Lumen DiameterScaffold (mm±SD)
Mean Lumen DiameterDistal (mm±SD)
2.68±0.45 2.57±0.56 2.76±0.46 2.60±0.29 2.49±0.34 2.66±0.33 2.39±0.35 2.09±0.50 2.39±0.40
80% (20/25)demonstrate≥ 3% vasomotion ≥ 3% vasomotion after Ach or Nitro
Ach = Acetylcholine
Nitro = Nitroglycerine
Lancet. 2016 Jan 2;387(10013):31-9. doi: 10.1016/S0140-6736(15)00447-X.
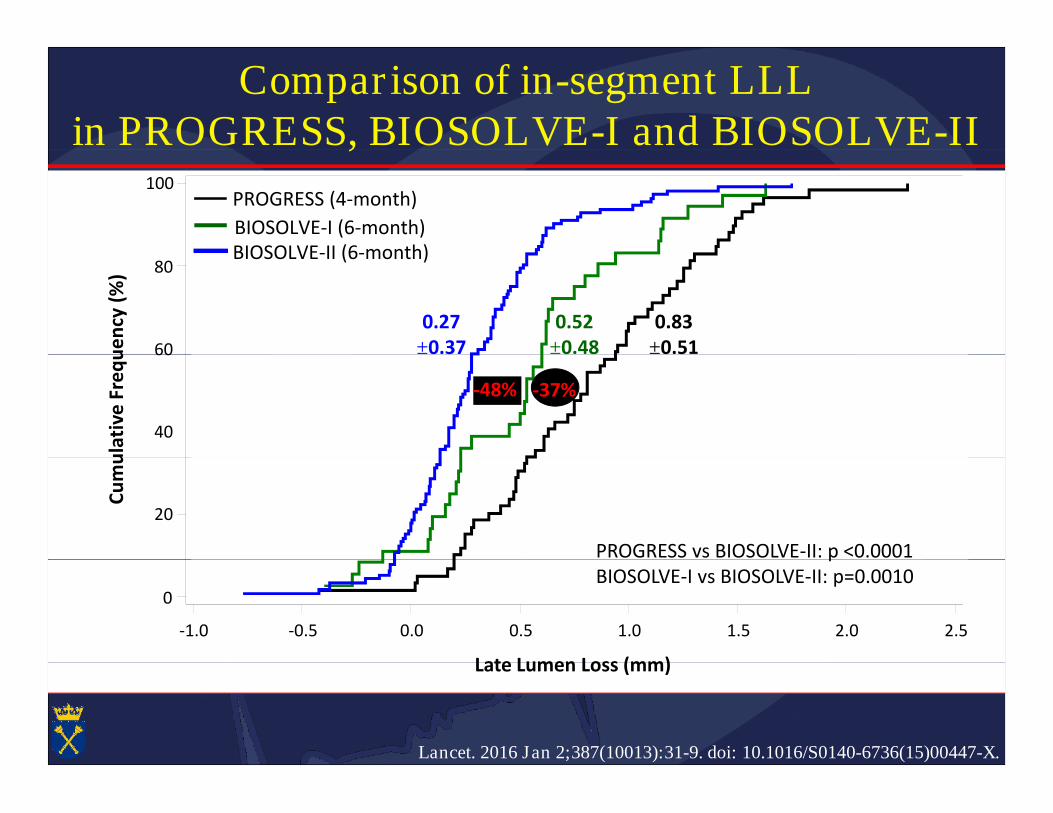
Comparison of in-segment LLLin PROGRESS, BIOSOLVE-I and BIOSOLVE-IIin PROGRESS, BIOSOLVE-I and BIOSOLVE-II
100
BIOSOLVE-I (6-month)
PROGRESS (4-month)
BIOSOLVE-II (6-month)
60
80
Cu
mu
lati
veFr
eq
ue
ncy
(%)
0.83±0.51
0.52±0.48
0.27±0.37
BIOSOLVE-II (6-month)
40
60
Cu
mu
lati
veFr
eq
ue
ncy
(%)
±0.51±0.48±0.37
-48% -37%
20
Cu
mu
lati
veFr
eq
ue
ncy
(%)
PROGRESS vs BIOSOLVE-II: p <0.0001
-1.0 -0.5 0.0 0.5 1.0 1.5 2.0 2.5
Late Lumen Loss (mm)
0
PROGRESS vs BIOSOLVE-II: p <0.0001BIOSOLVE-I vs BIOSOLVE-II: p=0.0010
Lancet. 2016 Jan 2;387(10013):31-9. doi: 10.1016/S0140-6736(15)00447-X.
Late Lumen Loss (mm)
Magmaris implantation NFIC 2016Magmaris implantation NFIC 2016
Institute of Cardiology, Jagiellonian University
Krakow, Poland
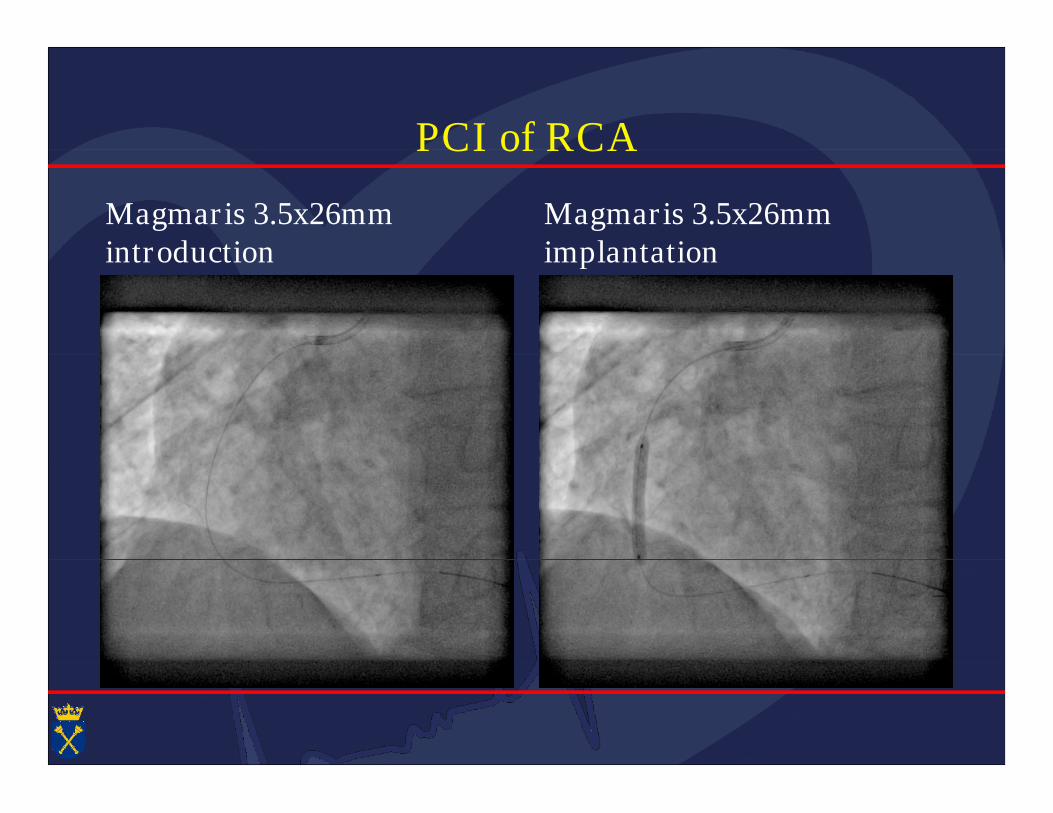
PCI of RCAPCI of RCA
Magmaris 3.5x26mmintroduction
Magmaris 3.5x26mmimplantationintroduction implantation
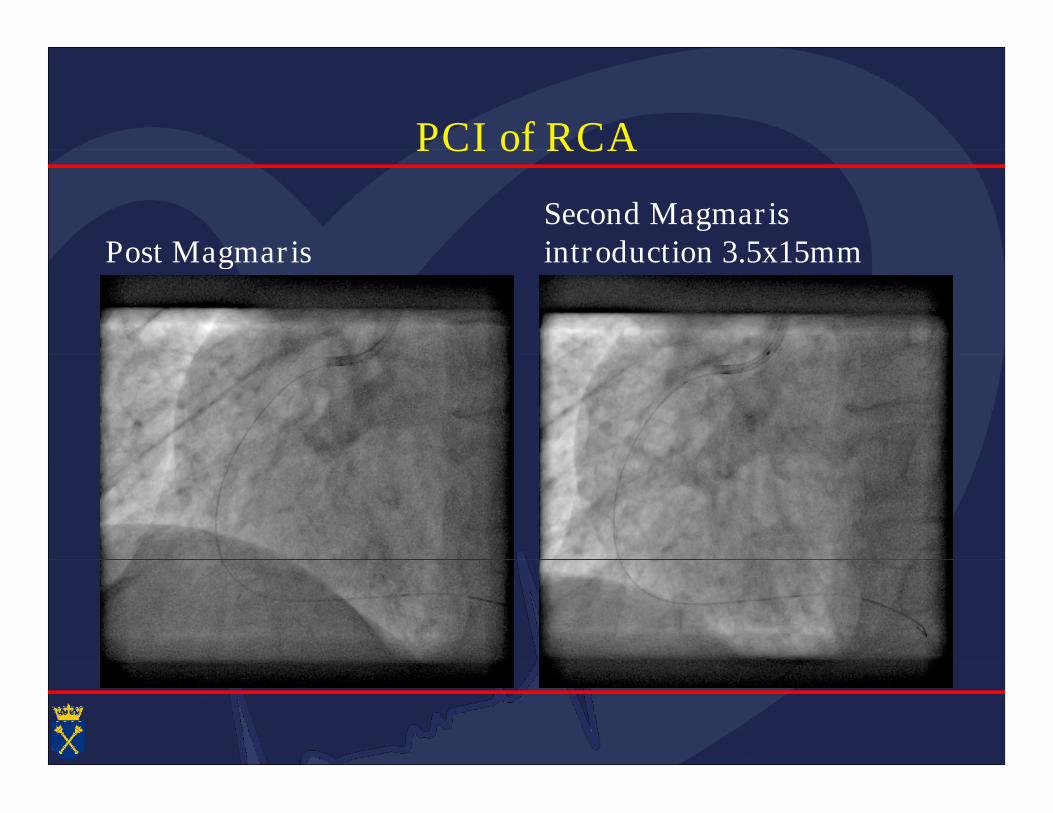
PCI of RCAPCI of RCA
Post MagmarisSecond Magmarisintroduction 3.5x15mmPost Magmaris introduction 3.5x15mm
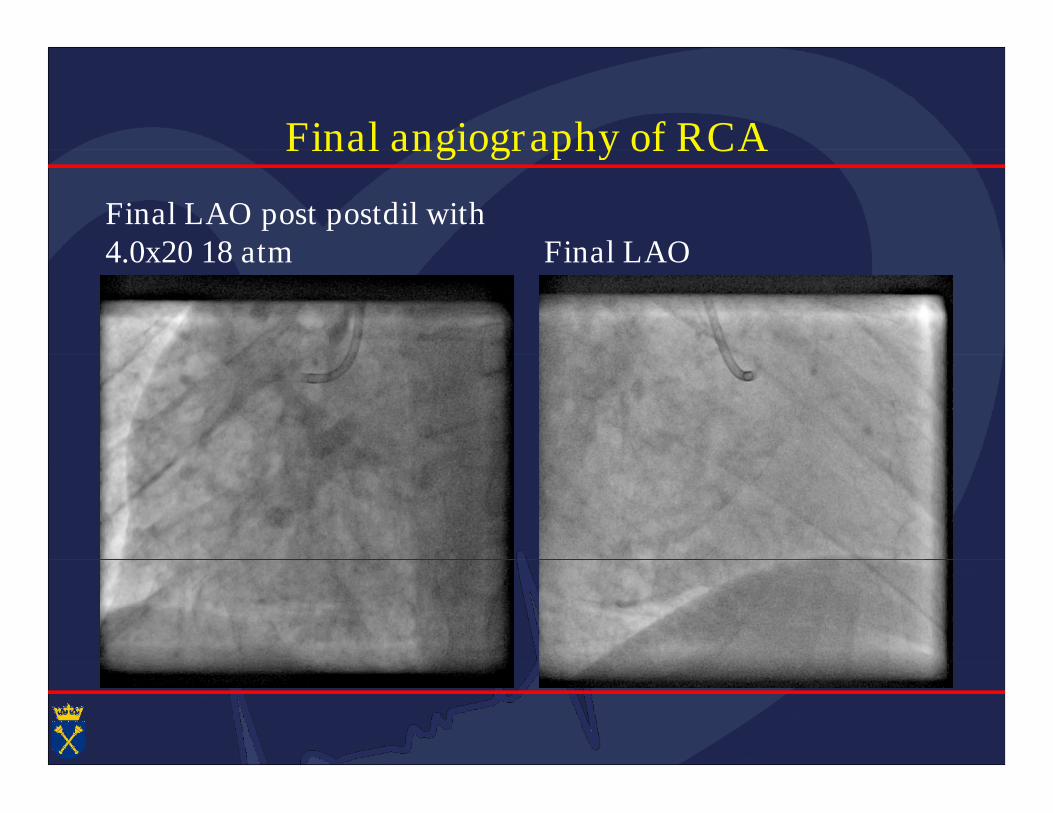
Final angiography of RCAFinal angiography of RCA
Final LAO post postdil with4.0x20 18 atm Final LAO4.0x20 18 atm Final LAO
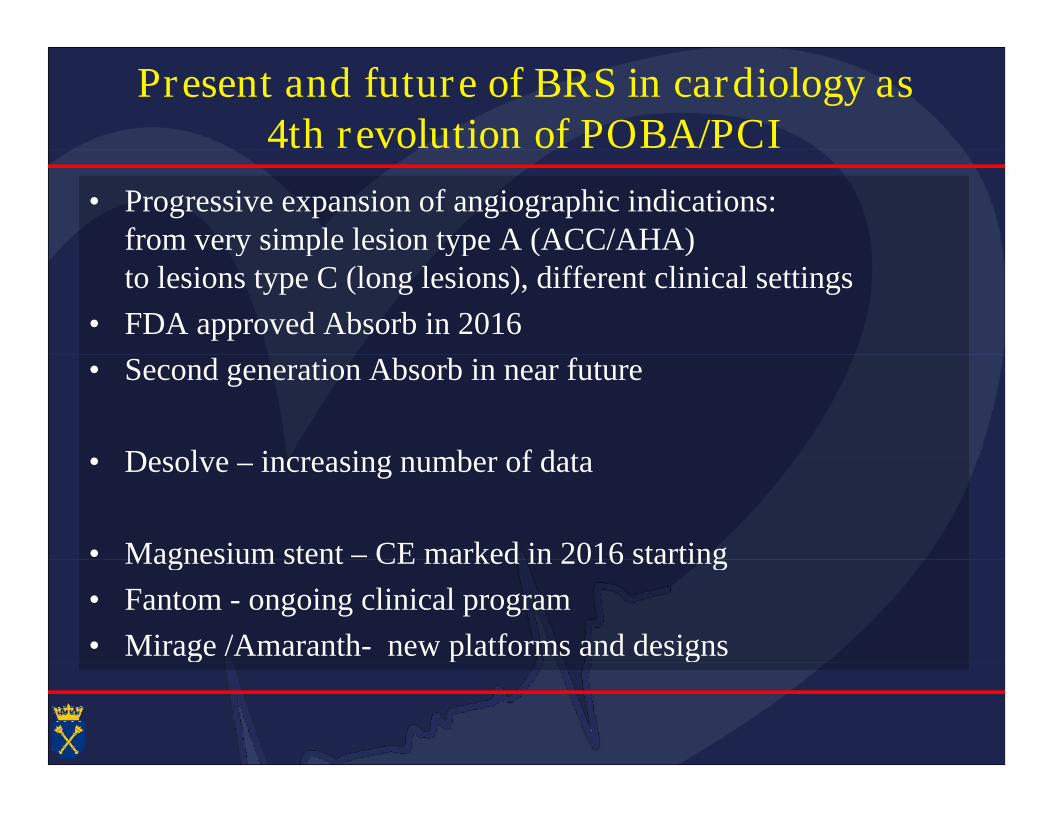
Present and future of BRS in cardiology as4th revolution of POBA/PCI4th revolution of POBA/PCI
• Progressive expansion of angiographic indications:from very simple lesion type A (ACC/AHA)from very simple lesion type A (ACC/AHA)to lesions type C (long lesions), different clinical settings
• FDA approved Absorb in 2016
• Second generation Absorb in near future• Second generation Absorb in near future
• Desolve – increasing number of data• Desolve – increasing number of data
• Magnesium stent – CE marked in 2016 starting• Magnesium stent – CE marked in 2016 starting
• Fantom - ongoing clinical program
• Mirage /Amaranth- new platforms and designs• Mirage /Amaranth- new platforms and designs
Amorphous poly-l-lactic acid–based BRS(Amaranth BRS)(Amaranth BRS)
There were no differences in minimum lumen diameter,percentdiameter stenosis, and late lumen loss for both Amaranth BRS andAbsorb BVS at any of the time points.
Circ Cardiovasc Interv. 2016;9:e004253
Absorb BVS at any of the time points.
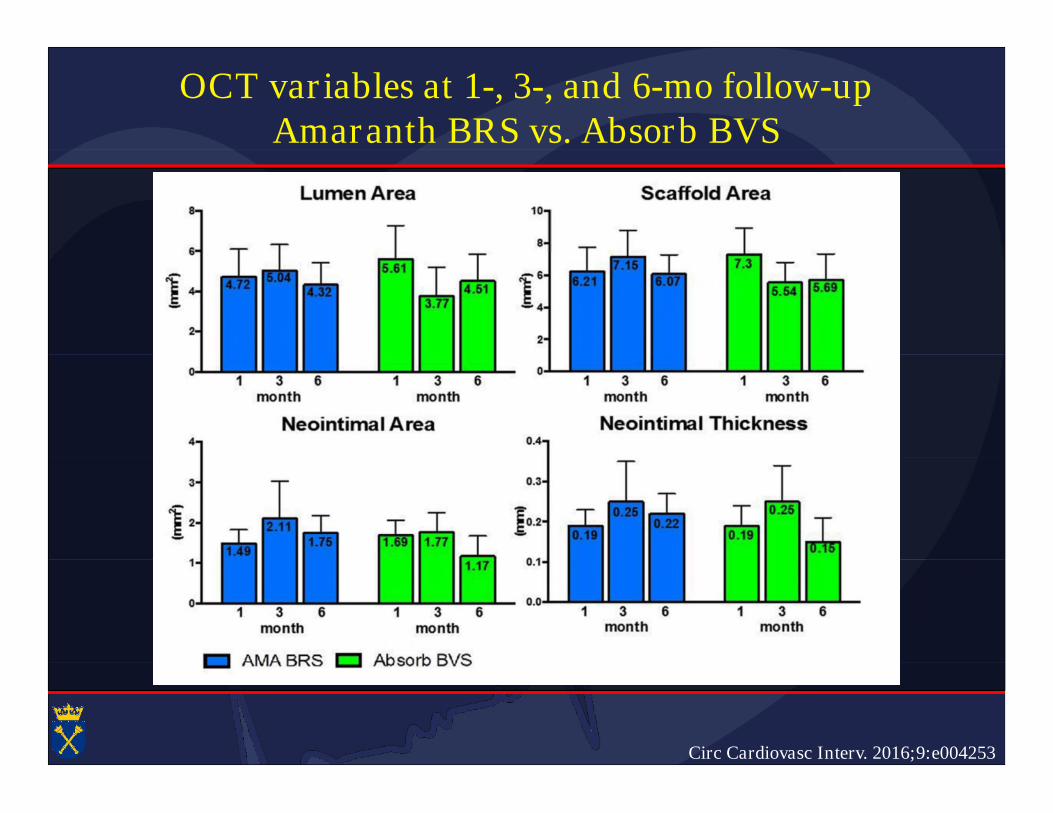
OCT variables at 1-, 3-, and 6-mo follow-upAmaranth BRS vs. Absorb BVSAmaranth BRS vs. Absorb BVS
Circ Cardiovasc Interv. 2016;9:e004253
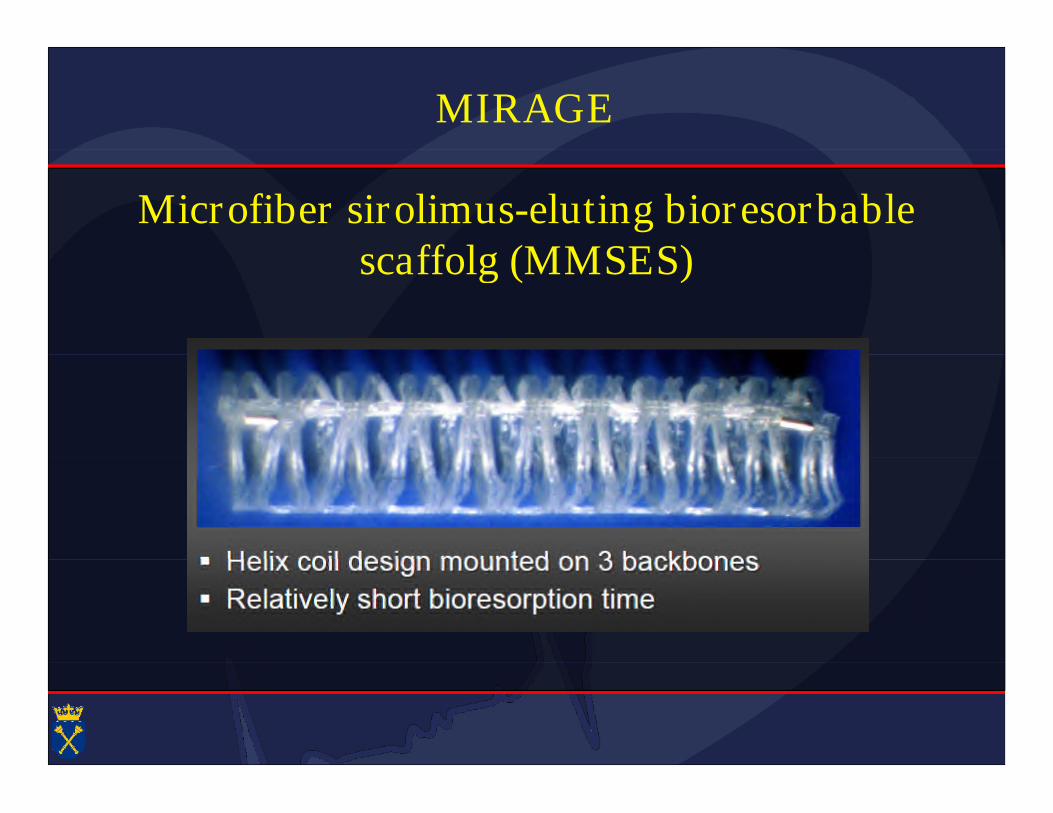
MIRAGE
Microfiber sirolimus-eluting bioresorbablescaffolg (MMSES)scaffolg (MMSES)
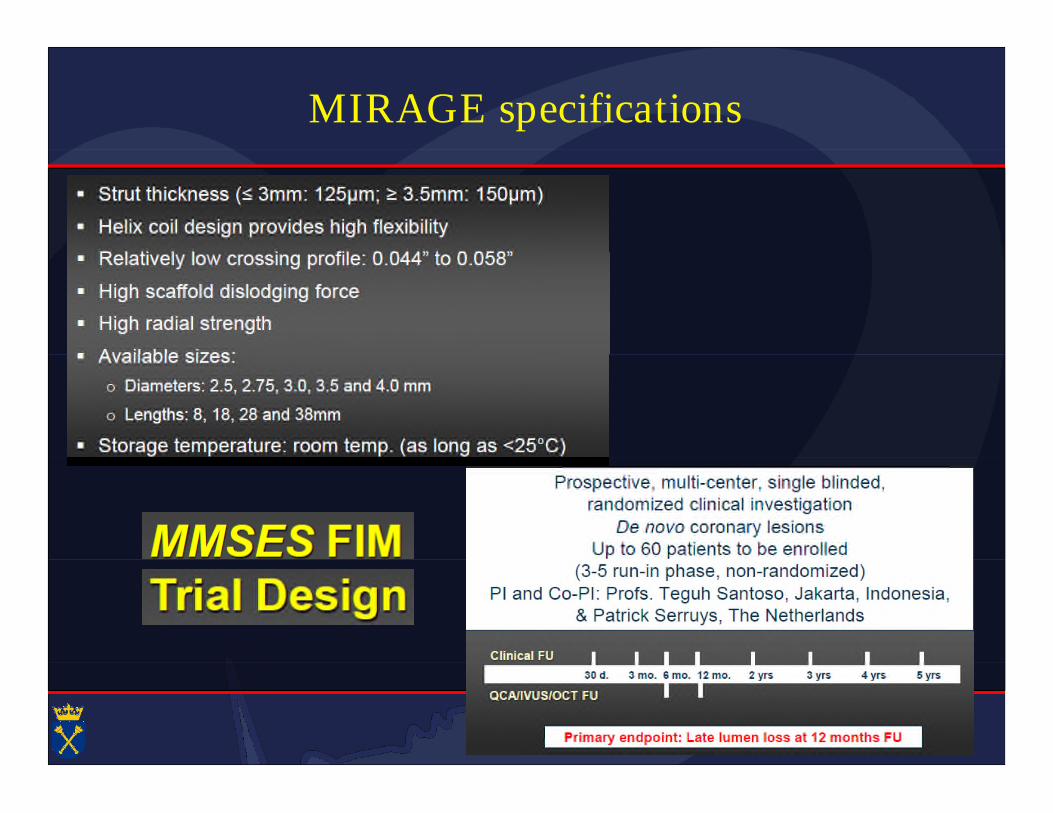
MIRAGE specifications
Conclusion
DREAMS 2G in BIOSOLVE-II demonstrates significantly improved in-segmentLLL (0.27±0.37mm) compared to it`s precursor devices tested in thePROGRESS (0.83±0.37mm) and the BIOSOLVE-I study (0.52±0.48mm)PROGRESS (0.83±0.37mm) and the BIOSOLVE-I study (0.52±0.48mm)
Vasomotion of the scaffolded vessel segment was demonstrated at 6 months
IVUS results in a subgroup of 30 subjects demonstrate a preservation of the IVUS results in a subgroup of 30 subjects demonstrate a preservation of thescaffold area with a low neo-intimal area at 6-month
No intra-luminal masses were observed by OCT at any time in a subgroup of25 subjects25 subjects
DREAMS 2G in BIOSOLVE-II demonstrates a low TLF (3.3%) and TLR (1.7%)rate at 6-month, which is comparable to other absorbable scaffolds andpermanent drug eluting stentspermanent drug eluting stents
No definite or probable scaffold thrombosis was observed with DREAMS 2Gtested in BIOSOLVE-II or any of it`s precursor devices tested in PROGRESSand BIOSOLVE-I in a total of 232 subjects
Lancet. 2016 Jan 2;387(10013):31-9. doi: 10.1016/S0140-6736(15)00447-X.
and BIOSOLVE-I in a total of 232 subjects
Magmaris implantation NFIC 2016Magmaris implantation NFIC 2016
Institute of Cardiology, Jagiellonian University
Krakow, Poland
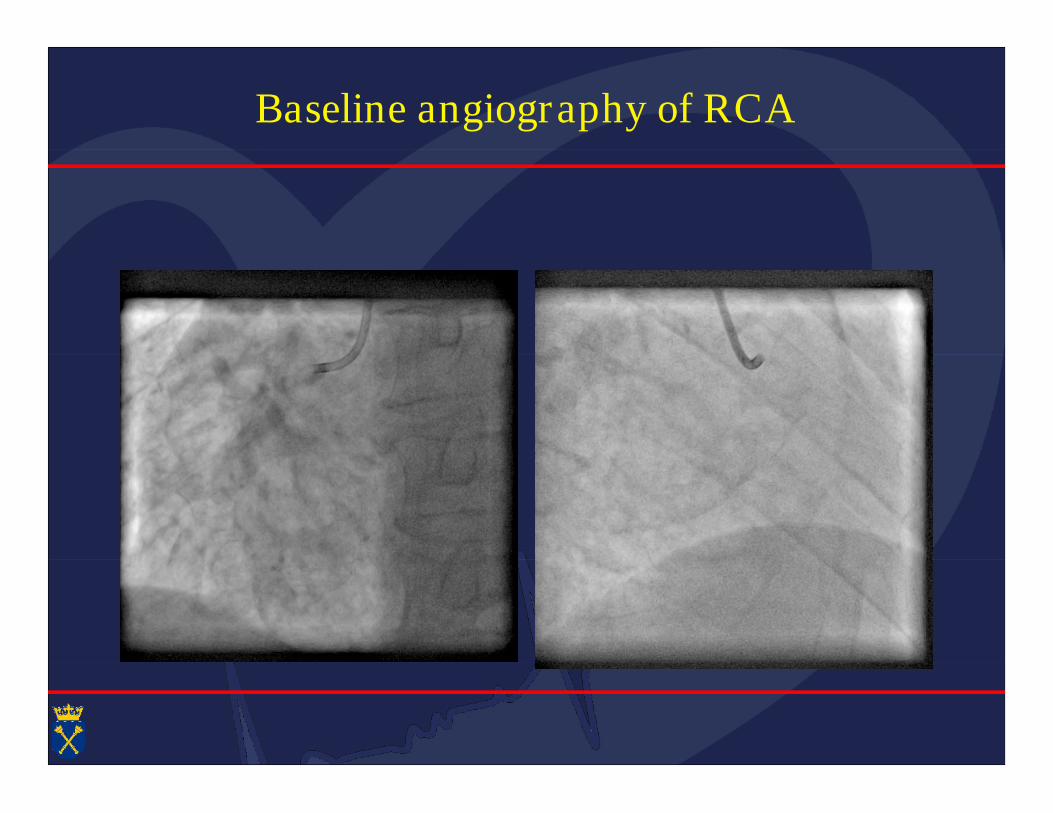
Baseline angiography of RCA
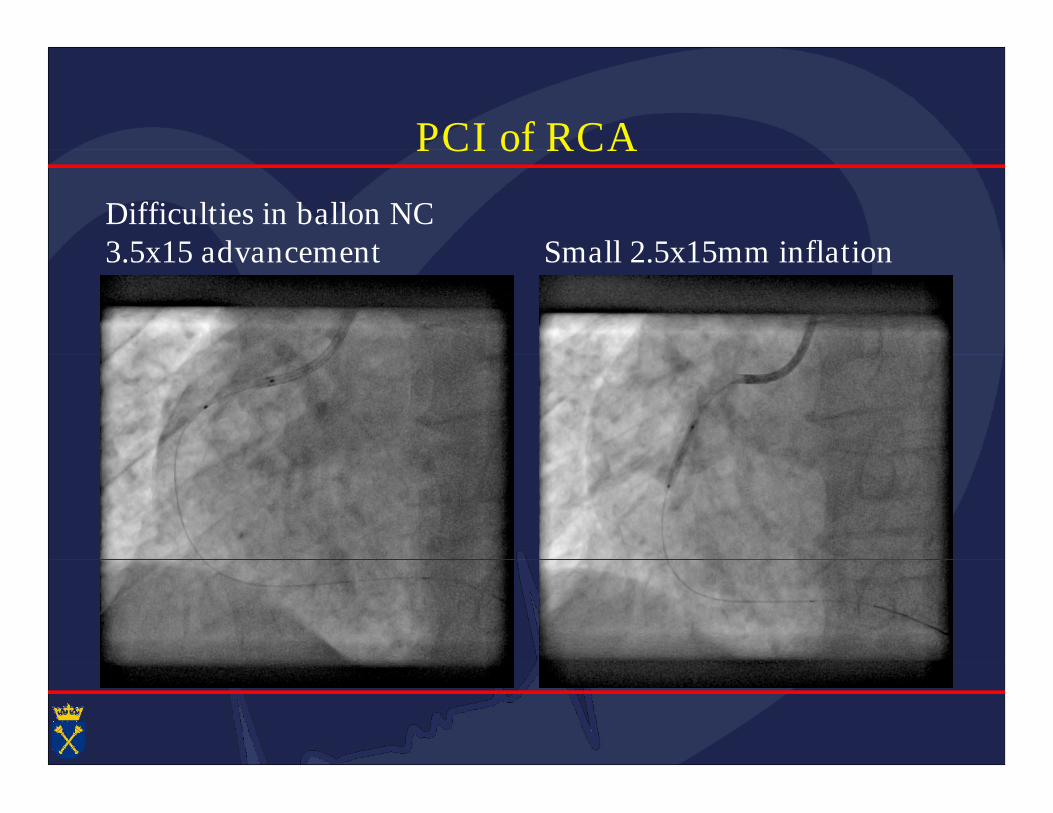
PCI of RCAPCI of RCA
Difficulties in ballon NC3.5x15 advancement Small 2.5x15mm inflation3.5x15 advancement Small 2.5x15mm inflation
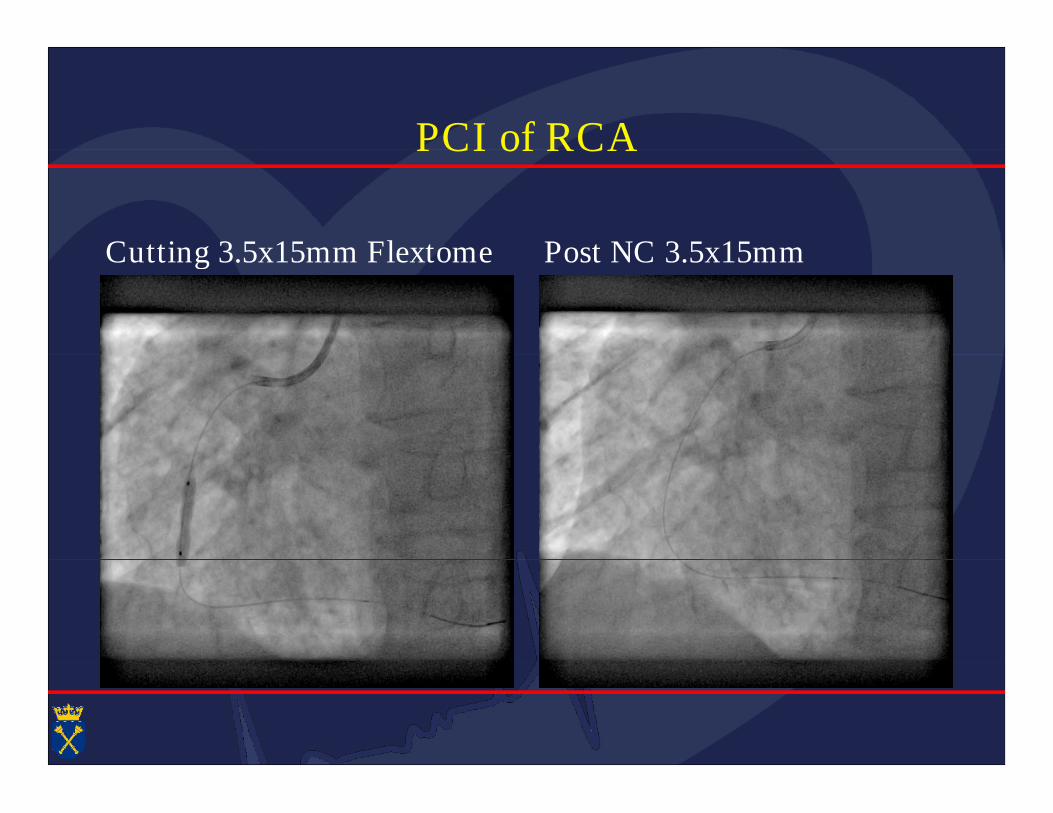
PCI of RCAPCI of RCA
Cutting 3.5x15mm Flextome Post NC 3.5x15mmCutting 3.5x15mm Flextome Post NC 3.5x15mm
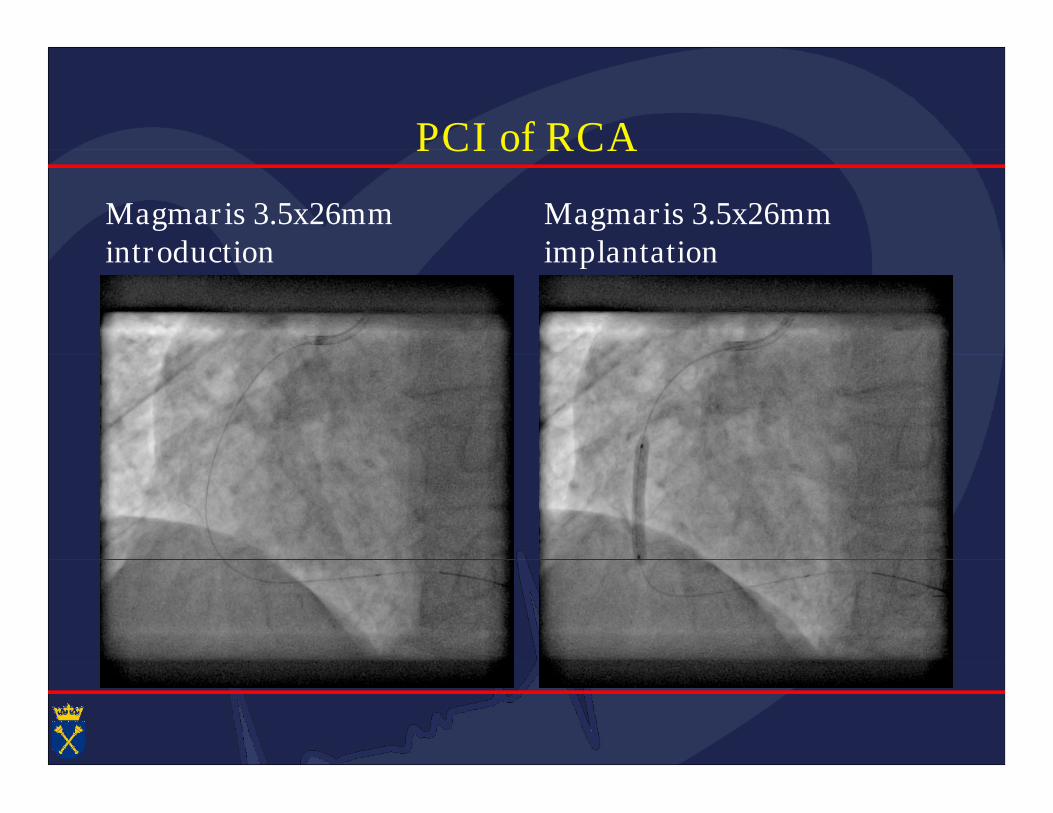
PCI of RCAPCI of RCA
Magmaris 3.5x26mmintroduction
Magmaris 3.5x26mmimplantationintroduction implantation
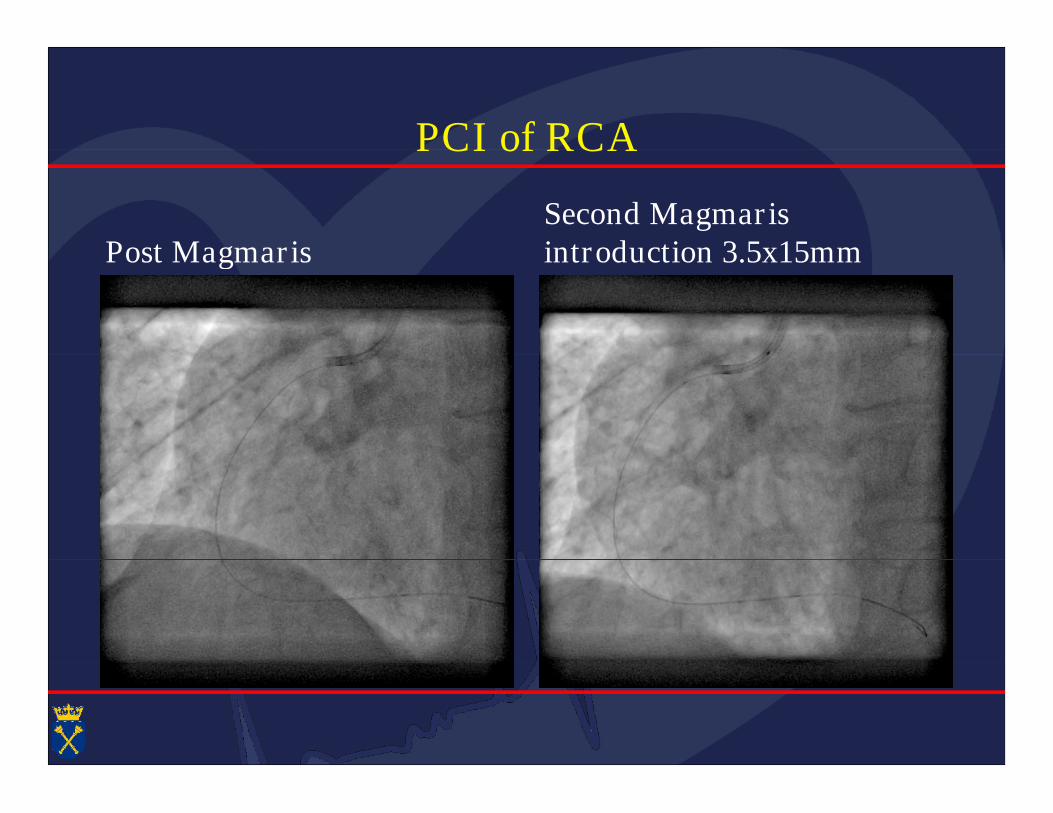
PCI of RCAPCI of RCA
Post MagmarisSecond Magmarisintroduction 3.5x15mmPost Magmaris introduction 3.5x15mm
Final angiography of RCAFinal angiography of RCA
Final LAO post postdil with4.0x20 18 atm Final LAO4.0x20 18 atm Final LAO
Present and future of BRS in cardiology as4th revolution of POBA/PCI4th revolution of POBA/PCI
• Progressive expansion of angiographic indications:from very simple lesion type A (ACC/AHA)from very simple lesion type A (ACC/AHA)to lesions type C (long lesions), different clinical settings
• FDA approved Absorb in 2016
• Second generation Absorb in near future• Second generation Absorb in near future
• Desolve – increasing number of data• Desolve – increasing number of data
• Magnesium stent – CE marked in 2016 starting• Magnesium stent – CE marked in 2016 starting
• Fantom - ongoing clinical program
• Mirage /Amaranth- new platforms and designs• Mirage /Amaranth- new platforms and designs











![ATTUALITA’ IN TEMA DI STENT BIORIASSORBIBILI? · BIOSOLVE-I n=46 BIOSOLVE-II n=123 BIOSOLVE-III n=63 12 month 36 month 12 month 6 month TLF[%] 23.8 6.8 3.4 3.3 Scaffold Thrombosi](https://img.pdfslide.us/doc/110x75/5edc41bfad6a402d6666d97b/attualitaa-in-tema-di-stent-bioriassorbibili-biosolve-i-n46-biosolve-ii-n123.jpg)