Embed Size (px)
Citation preview

correspondence
n engl j med 368;21 nejm.org may 23, 2013 2043
couraging, but given that regorafenib also tar-gets angiogenesis, could it be just reexposure to an antiangiogenic drug that is effective? 5
Raffaella Bracci, M.D.Ospedali Riuniti di Ancona Ancona, Italy [email protected]
Elena Maccaroni, M.D. Stefano Cascinu, M.D.Università Politecnica delle Marche Ancona, Italy
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
1. Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointesti-nal stromal tumour after failure of imatinib: a randomised con-trolled trial. Lancet 2006;368:1329-38.2. Blay JY. Pharmacological management of gastrointestinal stromal tumours: an update on the role of sunitinib. Ann Oncol 2010;21:208-15.3. Zama IN, Hutson TE, Elson P, et al. Sunitinib rechallenge in metastatic renal cell carcinoma patients. Cancer 2010;116:5400-6.4. Bergers G, Hanahan D. Modes of resistance to anti-angio-genic therapy. Nat Rev Cancer 2008;8:592-603.5. Demetri GD, Reichardt P, Kang YK, et al. Randomized phase II trial of regorafenib in patients with metastatic and/or unre-sectable gastrointestinal stromal tumor (GIST) progressing de-spite prior treatment with at least imatinib and sunitinib: GRID trial. J Clin Oncol 2012;30:Suppl:LBA 10008. abstract.
DOI: 10.1056/NEJMc1301237
Bioresorbable Airway Splint Created with a Three-Dimensional Printer
To the Editor: Tracheobronchomalacia in new-borns, which manifests with dynamic airway collapse and respiratory insufficiency, is difficult to treat.1,2 In an infant with tracheobronchoma-lacia, we implanted a customized, bioresorbable tracheal splint, created with a computer-aided design based on a computed tomographic image of the patient’s airway and fabricated with the use of laser-based three-dimensional printing, to treat this life-threatening condition.
At birth at 35 weeks’ gestation, the patient did not have respiratory distress and otherwise appeared to be in normal health. At 6 weeks of age, he had chest-wall retractions and difficulty feeding. By 2 months of age, his symptoms pro-gressed and he required endotracheal intubation to sustain ventilation. The workup revealed the following: an anomalous origin and malposition of the pulmonary arteries, with crisscross anat-omy; right pulmonary-artery hypoplasia; com-pression of the left mainstem bronchus between an abnormally leftward-coursing ascending aorta and an anteriorly displaced descending aorta; air trapping; and postobstructive pneumonia. Despite placement of a tracheostomy tube, mechanical ventilation, and sedation, ventilation that was sufficient to prevent recurring cardiopulmonary arrests could not be maintained.
We reasoned that the localized tracheobron-chomalacia was the cause of this physiological abnormality and made a custom-designed and
custom-fabricated resorbable airway splint. Our bellowed topology design, similar to the hose of a vacuum cleaner, provides resistance against collapse while simultaneously allowing flexion, extension, and expansion with growth. The splint was manufactured from polycaprolactone with the use of a three-dimensional printer (Fig. 1A through 1D).
The institutional review board of the Univer-sity of Michigan consulted with the Food and Drug Administration and approved the use of the device under the emergency-use exemption, and written informed consent was provided by the patient’s parents. After transposition of the right pulmonary artery and failed aortopexy, sutures were placed around the circumference of the malacic left bronchus and tied through inter-stices of the splint, and the bronchus was ex-panded (Fig. 1E). Subsequent bronchoscopy re-vealed normal patency of the bronchus without dynamic collapse (Fig. 1F) and normal ventila-tory variation in the size of the left lung. The partial pressure of carbon dioxide in venous blood decreased from 88 to 48 mm Hg. Seven days after placement of the airway splint, wean-ing from mechanical ventilation was initiated, and 21 days after the procedure, ventilator sup-port was discontinued entirely and the child was discharged home with the tracheostomy in place. One year after surgery, imaging and endoscopy showed a patent left mainstem bronchus (Fig.
The New England Journal of Medicine Downloaded from nejm.org on May 23, 2013. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 368;21 nejm.org may 23, 20132044
A
G
B
DC
E FTrachea
Carina
SVC
Aorta
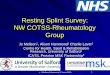
Figure 1. Placement of the Printed Airway Splint in the Patient.
Panel A shows the airway in expiration before placement of the splint; the image was reformatted with minimum- intensity projection. Panel B shows the patient-specific computed tomography–based design of the splint (red). Panel C shows an image-based three-dimensional printed cast of the patient’s airway without the splint in place, and Panel D shows the cast with the splint in place. Panel E shows intraoperative placement of the splint (green arrow) overlying the malacic left mainstem bronchial segment. SVC denotes superior vena cava. Panel F shows the bronchoscopic view, from the carina, of the left mainstem bronchus after placement of the splint. Panel G shows the airway in ex-piration 1 year after placement of the splint; the image was reformatted with minimum-intensity projection.
The New England Journal of Medicine Downloaded from nejm.org on May 23, 2013. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.

n engl j med 368;21 nejm.org may 23, 2013 2045
notices
1G). No unforeseen problems related to the splint have arisen. Full resorption of the splint was estimated to occur in 3 years.
This case shows that high-resolution imag-ing, computer-aided design, and biomaterial three-dimensional printing together can facili-tate the creation of implantable devices for con-ditions that are anatomically specific for a given patient.David A. Zopf, M.D. Scott J. Hollister, Ph.D.University of Michigan Ann Arbor, MI
Marc E. Nelson, M.D.Akron Children’s Hospital Akron, OH
Richard G. Ohye, M.D. Glenn E. Green, M.D.University of Michigan Ann Arbor, MI [email protected]
Supported by a grant (FD0003787) from the Food and Drug Administration.
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
1. Masters IB, Chang AB. Interventions for primary (intrinsic) tracheomalacia in children. Cochrane Database Syst Rev 2005;4:CD005304.2. Carden KA, Boiselle PM, Waltz DA, Ernst A. Tracheomalacia and tracheobronchomalacia in children and adults: an in-depth review. Chest 2005;127:984-1005.
DOI: 10.1056/NEJMc1206319Correspondence Copyright © 2013 Massachusetts Medical Society.
instructions for letters to the editor
Letters to the Editor are considered for publication, subject to editing and abridgment, provided they do not contain material that has been submitted or published elsewhere. Please note the following:
• Letters in reference to a Journal article must not exceed 175 words (excluding references) and must be received within 3 weeks after publication of the article.
• Letters not related to a Journal article must not exceed 400 words.
• A letter can have no more than five references and one figure or table.
• A letter can be signed by no more than three authors.
• Financial associations or other possible conflicts of interest must be disclosed. Disclosures will be published with the letters. (For authors of Journal articles who are responding to letters, we will only publish new relevant relationships that have developed since publication of the article.)
• Include your full mailing address, telephone number, fax number, and e-mail address with your letter.
• All letters must be submitted at authors.NEJM.org.
Letters that do not adhere to these instructions will not be considered. We will notify you when we have made a decision about possible publication. Letters regarding a recent Journal article may be shared with the authors of that article. We are unable to provide prepublication proofs. Submission of a letter constitutes permission for the Massachusetts Medical Society, its licensees, and its assignees to use it in the Journal’s various print and electronic publications and in collections, revisions, and any other form or medium.
notices
Notices submitted for publication should contain a mailing address and telephone number of a contact person or depart-ment. We regret that we are unable to publish all notices received. Notices also appear on the Journal’s website (NEJM.org/medical-conference). The listings can be viewed in their entirety or filtered by specialty, location, or month.
OncOlOgy cOnfEREncEsThe following conferences will be held: “Expanding Targets
in Lung Cancer” (Chicago, June 2); “12th International Con-gress on the Future of Breast Cancer” (Huntington Beach, CA, July 18–12); “14th International Lung Cancer Congress” (Hun-tington Beach, CA, July 25–27); “11th International Congress on Targeted Therapies in Cancer” (Washington, DC, Aug. 16 and 17); and “31st Annual Miami Breast Cancer Conference” (Miami Beach, FL, March 6–9).
Contact Physicians’ Education Resource, 666 Plainsboro Rd., Suite 356, Plainsboro, NJ 08536; or call (888) 949-0045; or fax (609) 257-0705; or e-mail [email protected]; or see http://www.gotoper.com/conferences.
MAyO clinic scOTTsdAlEThe following courses will be offered: “Neurology in Clini-
cal Practice” (Santa Barbara, CA, July 11–14); “Mayo Clinic Di-agnostic Imaging Update and Self-Assessment” (Dana Point, CA, July 29–Aug. 2); “Mayo Clinic Cardiology Update 2013: The Heart of the Matter” (Sedona, AZ, Aug. 2–4); “16th Annual Mayo Clinic Internal Medicine Update: Sedona 2013” (Sedona, AZ, Oct. 10–13, Oct. 24–27); “Mayo Clinic Hospital Medicine: Managing Complex Patients” (Tucson, AZ, Nov. 6–9); and “Multidisciplinary Update in Breast Disease” (Scottsdale, AZ, Nov. 13–16).
Contact Mayo School of Continuous Professional Develop-ment, Mayo Clinic, 13400 E. Shea Blvd, Scottsdale, AZ 85259; or call (480) 301-4580; or fax (480) 301-8323; or e-mail [email protected]; or see http://www.mayo.edu/cme.
76Th AnnuAl cOlOn And REcTAl suRgERy cOnfEREncE
The conference will be held in Minneapolis, Oct. 23–26. It is sponsored by the University of Minnesota Division of Colon and Rectal Surgery.
Contact Susan Crolla, 5353 Wayzata Blvd., Suite 350, Minne-apolis, MN 55416; or call (850) 212-6477; or e-mail info@ colonrectalcourse.org; or see http://www.colonrectalcourse.org.
TwElfTh AnnuAl PRiMARy fOcus syMPOsiuMThe symposium will be held in Marco Island, FL, June 21–23.Contact Baptist Health South Florida, 8900 N. Kendall Dr.,
Miami, FL 33176; or e-mail [email protected]; or see http://primaryfocus.baptisthealth.net.
The New England Journal of Medicine Downloaded from nejm.org on May 23, 2013. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.