Embed Size (px)
Citation preview

International Journal of Nursing Studies 46 (2009) 678–688
Contents lists available at ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
Biopsychosocial factors are associated with low back pain in femalenursing students: A cross-sectional study
Tim Mitchell a,*, Peter B. O’Sullivan a, Anne Smith a, Angus F. Burnett a,b, Leon Straker a,Jenny Thornton d, Cobie J. Rudd c
a School of Physiotherapy, Curtin University of Technology, Perth, Western Australia, Australiab School of Exercise, Biomedical and Health Sciences, Edith Cowan University, Western Australia, Australiac School of Nursing, Midwifery and Post-graduate Medicine, Edith Cowan University, Perth, Western Australia, Australiad School of Psychology, Curtin University of Technology, Perth, Western Australia, Australia
A R T I C L E I N F O
Article history:
Received 22 July 2008
Received in revised form 4 November 2008
Accepted 4 November 2008
Keywords:
Low back pain
Biopsychosocial
Physical
Psychological
Nurse
A B S T R A C T
Background: Occupational low back pain is a significant problem among nurses. Recent
literature suggests current occupational preventative strategies for nurses have not been
effective. Given low back pain is already prevalent before commencing employment,
nursing students should be the target of preventative interventions. Modifiable personal
factors which contribute to low back pain have proven difficult to identify, but are thought
to play an important role in the biopsychosocial nature of low back pain.
Objectives: To evaluate the contribution of personal biopsychosocial factors to low back
pain in nursing students.
Design: Cross-sectional study comprising physical testing and questionnaires.
Settings: Two university undergraduate nursing schools in Western Australia.
Participants: 170 female undergraduate nursing students.
Methods: Low back pain and control subjects were compared across social, lifestyle
(physical activity), psychological (stress, anxiety, depression, back pain beliefs, coping
strategies and catastrophising) and physical (spinal postures and spinal kinematics in
functional tasks, leg and back muscle endurance, spinal repositioning error and
cardiovascular fitness) characteristics. Low back pain was considered as either ‘‘minor’’
or ‘‘significant’’ depending upon pain severity, duration, impact and level of disability.
Results: Over 30% of all subjects (mean age 22.5� 4.5 years) reported ‘‘significant’’ low back
paininthepreceding12months. Univariate analysis: social measuresdid not distinguishbetween
groups. Subjects with ‘‘significant’’ low back pain were more physically active (p = 0.04), had
higher stress scores (p = 0.01) and used passive coping strategies (p < 0.001) more than other
subjects. ‘‘Significant’’ low back pain subjects held their lower lumbar spine in a more extended
posture during transfers at bed height than other subjects. No differences between groups were
found for sagittal spinal mobility, static spinal posture, muscle endurance, spinal repositioning
error, cardiovascular fitness or other psychological measures. Multivariate analysis: regression
analysis revealed stress, coping, physical activity, spinal kinematics, and age all contributed
independently to the presence of low back pain, representing a significant 23% of variance.
Conclusions: Modifiable lifestyle, psychological and physical factors were independently
associated with low back pain in nursing students. Targeting personal factors associated
with low back pain in nursing students, rather than occupational factors in working nurses
may help improve the impact of low back pain in nurses. Prospective studies are required
to confirm the relevance of these findings for risk of future low back pain in nurses.
Crown Copyright � 2008 Published by Elsevier Ltd. All rights reserved.
* Corresponding author at: School of Physiotherapy, Curtin University of Technology, GPO Box U1987, Perth, Western Australia 6845, Australia.
E-mail address: [email protected] (T. Mitchell).
0020-7489/$ – see front matter . Crown Copyright � 2008 Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.ijnurstu.2008.11.004

T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688 679
What is already known about this topic?
� O
ccupational low back pain is a significant problem innurses. � C urrent occupational low back pain preventative stra-tegies for nurses have not proven effective. Given lowback pain is already prevalent before commencingemployment, there may need to be a shift in the timingand focus of these interventions.
� C urrently, the best personal predictor of low back pain isprevious history. Therefore there is a need to identifyother modifiable personal factors that contribute to lowback pain in nurses before they commence employment.
What this paper adds
� O
ver 30% of nursing students experienced significant lowback pain in the previous 12 months, confirming them asan appropriate target population for preventative inter-ventions. � T his study identified modifiable personal lifestyle,psychological and physical factors were independentlyassociated with LBP in nursing students, which explaineda significant proportion of the variance.
� T hese factors could form the basis of a biopsychosocialprevention approach that targets personal, rather thanoccupational factors associated with low back pain.However, prospective research is required to furthervalidate these findings.
1. Introduction
Low back pain (LBP) is widely regarded as a biopsy-chosocial problem (Waddell, 2004). Occupations such asnursing, which involve physical (Mohseni-Bandpei et al.,2006; Smedley et al., 1997) as well as psychological (Feyeret al., 2000) stressors, are known to increase LBP risk(Violante et al., 2004; Yip, 2004). A recent review foundthere is no strong evidence regarding the efficacy ofworkplace interventions preventing LBP in nurses (Daw-son et al., 2007).
As LBP is already a significant problem among nursingstudents prior to commencing full-time employment(Mitchell et al., 2008; Videman et al., 2005), LBP preventionshould perhaps target nurses before their careers begin(Mitchell et al., 2008). This would require that interven-tions focus on personal, rather than occupational factorsassociated with LBP. However, modifiable personal factorsthat influence LBP need to be identified before successfulinterventions can be developed.
Currently, previous LBP history explains the largestproportion of group variance in previous studies (Feyeret al., 2000; Smedley et al., 1997), which does not informunderlying mechanisms or guide management. This maysuggest that identifying modifiable personal factorsassociated with non-disabling LBP in younger populationscould assist in guiding LBP interventions to prevent futureLBP in these populations. This notion is supported byrecent research demonstrating that LBP can be preventedby a physiotherapy intervention that targets personalfactors in female adolescents (ref). It is proposed that this
approach may help to reduce the likely cumulative in-fluence of these personal factors and occupational factorson subsequent chronic LBP development in older workingpopulations.
Current evidence of psychological factors associatedwith LBP development in nursing staff identifies occupa-tional factors such as interpersonal workplace stress andjob satisfaction (Eriksen et al., 2004; Yip, 2004). In terms ofpsychological factors outside the workplace however,there is some evidence that pre-existing psychologicaldistress is linked with future LBP episodes in youngerpopulations including nursing students (Feyer et al., 2000;Power et al., 2001).
Other personal psychological factors such as fear anddistress are linked to LBP chronicity, disability and sickleave patterns rather than the development of LBP(Boersma and Linton, 2006). Other factors include cata-strophising (Peters et al., 2005), and passive copingstrategies (Mercado et al., 2005). The role of these factorsin the development of LBP remains unclear.
Most physical risk factors for LBP in nurses are focussedon occupational factors such as volumes of bending andlifting (Mohseni-Bandpei et al., 2006; Yip, 2004). A range ofpersonal physical including poor back muscle endurance(Moffroid et al., 1994), reduced cardiovascular fitness (Cadyet al., 1979), altered motor control patterns (Cholewickiet al., 2005), poor spinal posture (Dankaerts et al., 2006), andreduced sagittal range of motion (Wong and Lee, 2004) havebeen found in various LBP populations. However, it isunclear whether these factors are important in nursingstudents. There is also a lack of consensus regarding theinfluence of other personal (such as gender, age, and weight)and social (such as alcohol, smoking and injury history)factors on LBP (Dempsey et al., 1997). Further, lifestylefactors such as physical inactivity (Wedderkopp et al., 2008)and high levels of vigorous physical activity (Kujala et al.,1999) have been associated with LBP.
Non-modifiable predictors such as previous LBP historyand genetic factors explain over 40% of LBP variance(Hestbaek et al., 2004; Shelerud, 2006). However, emer-ging evidence of altered movement and spinal postures inLBP subjects when performing pain provocative tasks(Dankaerts et al., 2006), along with differences in regionallumbar spine function (Gill et al., 2007), may help explain agreater proportion of modifiable physical LBP risk.Furthermore, it is likely that factors associated with LBPcannot be generalised across different populations (Schenket al., 2007) and within a biopsychosocial model, no singlefactor can explain LBP (Adams et al., 2002).
2. Aims and objectives
The purpose of this study was to comprehensivelyevaluate the influence on LBP of personal biopsychosocialfactors including task-specific individual physical factorsrelevant to pain provocation in female nursing students.
3. Methods
This cross-sectional study examined a range of personalpsychological, physical and social/lifestyle characteristics

T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688680
in female undergraduate nursing students with andwithout a history of LBP as part of a larger prospectivestudy.
3.1. Sample
Data were collected on female undergraduate nursingstudents from two undergraduate university nursingprograms with approximately 1660 enrolled students.Ethical approval to conduct the study was granted fromboth universities involved, and written informed consentwas obtained from subjects. Subjects attended a singletesting session of 60–90 min duration, which involvedcompletion of both questionnaires and a range of physicalassessments (listed below).
Subjects aged between 18 and 35 in their second orthird year of the programs were recruited by personalinvitation during lectures at both universities. A total of196 students registered interest in the study and of these175 subsequently agreed to participate. Sample sizecalculations were based on statistical requirements forthe prospective component of this study, which indicatedminimum group sizes (LBP and Control) of 30 subjectswould provide sufficient statistical power to detectprimary associations of interest.
All nursing students with or without LBP (symptomsfrom the region of the back between L1 and the glutealfolds) were invited to participate. However, based on ourprevious survey of LBP in a similar nursing student sample(Mitchell et al., 2008), we expected the majority ofstudents (approximately 80%) to already have had someexperience of LBP (ache pain or discomfort) and that mostLBP subjects would have episodic rather than chronic,disabling LBP. This population was chosen to fulfil theobjective of investigating personal factors associated withLBP in a cohort at high-risk of future chronic LBP in theirworking life.
Subjects were excluded if they had; an inability tounderstand written or spoken English; other conditionsaffecting the spine or lower limbs including inflammatorydisorders, neurological diseases or metastatic disease;pregnancy or less than 6 months post-partum; inability tocomplete all physical tests; or pain greater than 3 out of 10on a VAS at the time of testing (one subject). Pregnancyexcluded two subjects, one had an active spondyloarthro-pathy and one subject had a forearm fracture, resulting in astudy sample of 170 subjects.
Subjects who had acute LBP that limited theirperformance of the test procedures were excluded. Asacute LBP has been shown to influence spinal posture(Harrison et al., 1998) and motor control (Hodges et al.,2003) as well as physical performance due to psychologicalinfluences (Swinkels-Meewisse et al., 2006), includingthese subjects would potentially limit the conclusions,which could be drawn from the findings of this study. Bycomparing matched groups of subjects with differentlevels of LBP in the preceding 12 months (but not acutepain influencing their performance at the time of testing),differences found between the groups could therefore bemore strongly linked to the presence of recent (or current)LBP. It is proposed that intervention directed at such
identified factors could have strong implications forprevention of future LBP episodes.
3.2. LBP sub-groups
To investigate the influence of LBP, subjects weredivided into three LBP categories; No LBP, ‘Mild’ LBP and‘Significant’ LBP. Considering the multifactorial influ-ences on LBP (Waddell, 2004), and variance in LBPprevalence based on LBP definition (Marras et al., 2007),Significant LBP group allocation was defined by a com-bination of indicators across a range of domains fromprevious LBP research. Fifty-three female subjects wereclassified as having significant LBP as they scored abovethe designated cut off score in at least three of thefollowing four criteria:
1. L
ifetime LBP severity > 4/10 for their worst ever LBP ona visual analogue pain scale (Bolton, 1999).2. D
uration of LBP in previous 12 months > 1 week (todifferentiate subjects with a single, very short episode ofLBP (Kuornika et al., 1987)).3. L
BP requiring treatment or medication or a reduction inactivity in the past 12 months (Adams et al., 1999).4. L
BP disability levels at the time of testing of >20% asmeasured by the Oswestry Disability Index (ODI)(Fairbank et al., 1980).The remaining LBP subjects who reported some pain inthe previous 12 months, but did not satisfy the criteriafor Significant LBP were considered as having Mild LBP(Table 1).
3.3. LBP screening questionnaires
The Nordic Low Back Pain Questionnaire (Kuornikaet al., 1987) was used to determine LBP history, severityand impact, and to exclude subjects according to theinclusion/exclusion criteria. A visual analogue scale mea-sured highest lifetime LBP severity. The Modified CoreNetwork Low Back Pain Medical Screening Questionnaireassessed subject’s general health status and screen forconfounding ‘‘red flag’’ medical conditions (Committee,1997).
3.4. Social and lifestyle factors
Demographic and social data (socio-economic, maritalstatus, compensation history, alcohol consumption andsmoking), were obtained using a questionnaire based onprevious research (Brasic, 2003). The InternationalPhysical Activity Questionnaire (IPAQ) self-report longform was used to record average physical activity levelsof subjects over the last 7 days (Booth, 2000). Subjectsestimated average light, moderate and vigorous weeklyphysical activity levels across a range of domainsincluding Occupational, Transport and Leisure time. Datawere summed across the domains to give weeklyaverages (in hours) of time spent doing vigorous andmoderate physical activity as well as total time spentsitting and walking.

Table 1
Group comparisons of age, BMI and LBP characteristics [mean � S.D., %, or median (interquartile range)].
No LBP (n = 36) Mild LBP (n = 81) Significant LBP (n = 53) p-Value
Age (years) 21.7 � 3.5 22.0 � 4.2 23.9 � 5.1 0.06
BMI (kg/m2) 21.9 � 2.8 23.3 � 4.3 23.1 � 3.4 0.18
Lifetime highest VAS (/10) 0 3.9 � 2.3a 6.6 � 1.6b,c <0.001
Annual LBP duration (% >7days) 0 33.3a 92.5b,c <0.001
Significant LBP impact (%) 0 44.4a 96.2b,c <0.001
Oswestry Disability Index (%) 0 10.4 � 6.6a 21.2 � 9.2b,c <0.001
VAS = visual analogue scale, BMI = body mass index, significant LBP impact = requiring treatment, medication or activity reduction in the past 12 months.a Significant between No Pain and Mild Pain groups.b Significant between No Pain and Significant Pain groups.c Significant between Mild Pain and Significant Pain groups.
T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688 681
3.5. Psychological factors
Four reliable and valid questionnaires were used toevaluate psychological characteristics. The DepressionAnxiety Stress Scales (DASS) are a set of three self-reportscales used to measure depression, anxiety and stress(Lovibond and Lovibond, 1995). The Back Beliefs Ques-tionnaire (BBQ) is a 14-item self-administered question-naire which determines individual beliefs regarding theimpact of back pain (Symonds et al., 1996). The GeneralShort Form 19-item Coping Scale for Adults (CSA)investigates coping and the development of copingstrategies (Frydenberg and Lewis, 2004). It provides sub-scale scores for four coping styles; Dealing with theProblem; Non-productive Coping; Optimism (focus onpositive); and Sharing (social interaction and support fromothers). The relationship between degree of LBP severityand coping was assessed at the level of coping style as wellas four individual items (Play Sport, I Get Sick, ConsciouslyBlock out the Problem, and Worry About What WillHappen to Me) chosen by the authors as they reflectdifferent strategies commonly described by patients asways of dealing with different concerns. The PainCatastrophizing Scale (PCS) (Sullivan et al., 1995) contains13 items regarding past pain experiences and provides atotal and three sub-scale scores assessing Rumination,Magnification and Helplessness.
3.6. Physical factors
Body Mass Index was calculated as an index of weightrelative to height to provide an indication of adiposity.
3.6.1. Spinal angles
Lumbar spine sagittal plane (flexion/extension)angles (measured in degrees) were derived from sensorsplaced over T12, L3 and S2 using 3-Space1 FastrakTM
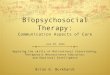
(Polhemus, Kaiser Aerospace, Vermont). Spinal posturesmeasured were usual sitting and usual standing. Sagittalspinal angles were measured in maximal slumpedsitting, sway standing, and maximal forward bendingand maximal backward bending in standing. Peaksagittal angles during a series of functional tasks werealso examined in an attempt to replicate specific aspectsof spinal loading in common nurse duties. Test posturesare shown in Fig. 1. All tests, except picking up a pen,were performed three times.
3.6.2. Sitting (usual and slumped)
It is acknowledged that measuring true ‘‘usual’’posture is difficult in the laboratory setting. However,subjects were covertly observed when completing ques-tionnaires prior to physical testing to gain an idea of their‘‘usual’’ sitting posture, and to ensure a similar posturewas adopted during testing. Further, subjects were notaware when the ‘‘usual’’ standing and sitting measureswere being recoded, as they performed a number of tasksthat involved sitting or standing as the starting position.Usual and slumped sitting postures were measured asfollows using a previously described protocol (Dankaertset al., 2006):
1. S
ubjects were asked to sit on a stool, which was selectedto allow their thighs to be parallel with the floor andknees flexed at 908. No direction of how to sit or anindication of what was being measured was provided.This position was recorded for five seconds as their usualsitting posture (defined as the sitting posture theywould usually adopt during unsupported sitting).2. S
ubjects were then assisted into their end of rangelumbar flexion sitting posture for five seconds by anexperienced therapist using standardised cues ofasking the subject to ‘‘slouch’’ and using hand cueson the lateral shoulder and pelvis to guide posteriorpelvic tilting.3.6.3. Standing (usual, sway, and maximal forward and
backward bending)
1. S
ubjects were asked to stand comfortably at a pre-determined position. Whilst no specific instruction ofhow to stand was given, all subjects stood with their feetparallel. This position was recorded for five seconds astheir usual standing posture (defined as the standingposture they would usually adopt during habitualunsupported standing).2. S
way standing posture was defined as subject’s relaxedstanding posture with the pelvis translated anteriorlyrelative to the trunk. All subjects were guided into thisposition for five seconds by the same experiencedtherapist. Excellent reliability of positioning subjects insway posture has been shown previously (O’Sullivanet al., 2002).3. S
ubjects were then asked to bend forwards as far aspossible with their knees straight, and a five second
Fig. 1. Test postures.
T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688682
recording in this position was defined as maximalforward bending.
4. S
imilarly, maximal backward bending was measured byasking subjects to then bend backwards as far aspossible for five seconds, keeping their feet stationary.3.6.4. Lifting (pen drop, box lift and pillow and box transfer)
1. W
hile in the standing position, a pen was placed in frontof subjects and they were asked to pick it up. Subjectswere directed to pick up the pen as if they had justdropped their own pen on the floor and needed toretrieve it. This test was performed only once.2. S
ubjects were then directed to pick up a moderate 5 kgload in a box with handles 20 cm above floor height. Nocues were given regarding how to pick up the box.3. A
height adjustable bed was then set at a height 10 cmabove each subject’s superior patella margin as astandardised height. The task involved transferring apillow from left to right a distance of 75 cm, then backto the starting position. Subjects initially stood at themid point between the pillow and target positionmarked on the bed, then were asked to transfer thepillow, with no specific directions regarding how tolift.
4. T
he task involving transferring a pillow was thenrepeated using a 5 kg box. Hand position was 20 cmabove bed surface (analogous to box handle height).3.6.5. Squatting (lower limb muscle endurance)
A measure of generalised lower limb muscle endurancewas taken using a single trial semi-squat static hold test,which has been described previously and shown todiscriminate between female rowers with and withoutLBP (Perich et al., 2006). Subjects were seated on a stoolwith thighs parallel and knees flexed at 908 and their armsfolded across their chest. Subjects were then asked toadopt a squat position with their buttocks just clear of the

T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688 683
stool, by an experienced therapist using standardised cues.Subject’s lumbar spine posture was recorded throughoutthe squat test, with a five second FastrakTM data sampletaken as their squat posture once their position was stableafter rising from the stool. The hold time was measured inseconds using a hand held stopwatch.
3.6.6. Back muscle endurance
Subject’s back muscle endurance was measured usingthe Biering-Sorensen test (Biering-Sorensen et al., 1989).The length of time in seconds the subject was able tomaintain neutral trunk alignment without deviating morethan 108 into flexion or extension was recorded during asingle trial.
3.6.7. Spinal repositioning sense (proprioception)
Spinal repositioning accuracy was determined usingthe 3-Space1 FastrakTM. Repositioning accuracy wasevaluated with subjects attempting to reproduce a criterionposition of neutral lumbar lordosis in sitting, using criteriareported elsewhere (O’Sullivan et al., 2003). Repositioningaccuracy in degrees was recorded as the angle from thecriterion position the subject holds during each reposi-tioning trial.
3.6.8. Cardiovascular fitness
The Astrand-Rhyming ergometer sub-maximal cardi-orespiratory fitness test (Astrand and Rodahl, 1986)was used to estimate VO2 (max) score and compare tonormative values to determine a fitness rating.
3.7. Data management
Analysis of spinal angles was conducted using customsoftware written in LabVIEW V8 (National Instruments,Texas, USA). Lower lumbar (LLx) (L3–S2), upper lumbar(ULx) (T12–L3), and total lumbar angles (T12–S2) werecalculated for each movement trial, as previously definedand shown to possess excellent inter-trial reliability insitting (Dankaerts et al., 2006). Reliability and validity ofthe FastrakTM system for measuring spinal range ofmotion has been demonstrated (Jordan et al., 2004;Pearcy and Hindle, 1989). For this study, only LLxangles were reported in the analysis. LLx spinal segmentsare most often the source of LBP (Beattie et al., 2000)and this study was examining spinal posture andkinematics relative to pain. Extension in the sagittalplane was assigned a positive value, and flexion anegative value.
Inter-trial reliability (from three trials for each subject)for all LLx measures in this study was excellent. The meanLLx ICC was 0.97 (range: 0.93–0.99) and mean LLx SEM was2.08 (range: 0.5–2.58). The mean angle of three trials(averaged over 5 s of data collection) was calculated foreach of; usual and maximal slumped sitting, usual andsway standing and maximal forward and backwardbending in standing. The mean peak sagittal angles werecalculated for the functional tasks. As there was nosustained hold during these tasks (except for the squat),the customised analysis software determined the point ofpeak sagittal flexion (or least sagittal extension) angle
reached between the manually tagged start and finish ofthe task.
Further analysis was conducted on how far subjectsheld their LLx spine from their maximal end of rangeflexion angle during different postures. For sitting, usualsitting angle was compared to maximal slump sittingangle. The maximal forward bending angle in standing wasused as the end of range reference angle to compare with;picking up the pen and box from the floor, transferring thepillow and box at bed height and squatting angle.
3.8. Statistical analysis
All basic statistical analyses were performed usingSPSS Version 13 (SPSS Inc., Chicago: USA) and IntercooledStata 9.2 for Windows (Statacorp LP, College Station: USA).Differences in psychological, physical and social char-acteristics between the three pain groups were testedusing chi-square analysis and one-way ANOVAs. Hoch-berg’s GT2 and Games–Howell post hoc analyses wereused, dictated by Levene’s test for homogeneity ofvariances. Kruskal–Wallis test was used for non-para-metric variables. A critical alpha probability of .05 wasused, with no adjustment for multiple comparisons tobalance Type I and Type II errors.
A logit ordinal regression model (proportional oddsmodel) was used to assess the independent association ofvariables from the physical and psychosocial domains withpain group membership, with pain group assumed to be athree level ordinal variable from No Pain to SignificantPain. The parallel regression assumption for each variablein the model was tested using the Brant test. Analysis ofresiduals was performed to check for cases with undueinfluence over model estimates. A two-step model selec-tion procedure consisted of (i) identifying those variableswithin each domain that were significantly and indepen-dently associated with pain group membership afteradjusting for age, and (ii) simultaneously entering thosevariables identified from step 1 into a final model, with ageincluded as a covariate. Model fit was assessed using themodel chi-squared likelihood ratio test and the substantivesignificance of the model was assessed by McKelvey andZavoina’s R2, which has been suggested as the closestanalogue to linear regression R2 (Scott Long and Freese,2006).
4. Results
The highest proportion of subjects (48%) was in the MildLBP group, with Significant LBP being experienced by 31%of subjects and only 21% of the subjects reporting noprevious history of LBP (Table 1).
4.1. Social and lifestyle factors
No differences between LBP groups were found for anyof the social factors including alcohol consumption orcigarette smoking (p-value range 0.17–0.90). Subjectswith Significant LBP were involved with more hours ofmoderate plus vigorous activity per week [median 17.5 h(IQR 14.3)] than subjects with Mild LBP [median 9.0 h

Table 2
Group comparisons of psychological variables [mean � S.D., or median (interquartile range)].
No LBP (n = 36) Mild LBP (n = 81) Significant LBP (n = 53) p-Value
DASS total (/126) 8 (10) 12 (14) 16 (16)a 0.007
Depression (/42) 1 (2) 2 (4) 2 (4) 0.31
Anxiety (/42) 2 (4) 4 (4) 4 (4) 0.082
Stress (/42) 5 (6) 8 (10) 10 (10)b,a 0.004
Back Beliefs Questionnaire (/45) 28.9 � 4.5 30.4 � 4.9 29.3 � 5.6 0.28
Coping scale for adults
Dealing with problem (/105) 73.0 � 12.8 69.7 � 13.1 69.8 � 12.8 0.41
Non-productive coping (/105) 51.9 � 11.2 53.1 � 12.9 57.8 � 20.1 0.14
Sharing (/100) 53.2 � 16.5 45.4 � 13.8c 47.2 � 14.9 0.027
Optimism (/100) 64.7 � 15.3 60.4 � 12.8 61.2 � 13.6 0.23
Pain Catastrophizing Scale (/52) 9.5 (13.8) 7.5 (13) 9.0 (13.5) 0.24
Rumination (/16) 4.0 (6.5) 3.0 (5.75) 5.0 (8.0) 0.40
Magnification (/12) 1.0 (3.0) 2.0 (3.0) 2.0 (3.0) 0.24
Helplessness (/24) 3.5 (4.75) 2.0 (4.75) 3.0 (6.5) 0.28
a Significant between Mild Pain and Significant Pain groups.b Significant between No Pain and Significant Pain groups.c Significant between No Pain and Mild Pain groups.
T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688684
(IQR 14.0), p = 0.04]. There were trends for Significant LBPsubjects tending to sit less hours per week than othersubjects (p = 0.18).
4.2. Psychological factors
A summary of psychological variables is provided inTable 2. The DASS total score and Stress subscale scorewere higher in the Significant LBP group when comparedwith No LBP subjects. Of the four subscales within the CSA,the only difference was in the Sharing scale, with the scorebeing higher in the No LBP group, when compared with theMild LBP group. Of the individual CSA items tested, ‘‘I GetSick’’ was more frequently reported in the Significant LBPgroup, compared with both the No LBP and Mild LBPgroups (p = 0.02). There were no differences in back beliefsor pain catastrophising scores between groups.
4.3. Physical factors
There were no differences evident between the threegroups for leg muscle endurance, back muscle enduranceor spinal repositioning error (see Table 3). Across allsubjects, the median cardiovascular fitness rating was‘‘Average’’ (Astrand and Rodahl, 1986) and there were nodifferences in mean cardiovascular fitness (VO2 max)scores between the three groups.
There were no differences in usual standing posture orusual sitting posture between the three groups. Acomparison of LLx spinal angles in static postures andacross functional tasks is shown in Table 3.
Subjects with Significant LBP were further away fromtheir maximal forward bending angle when picking up a penfrom the floor and transferring a pillow at bed height, thansubjects with Mild LBP. Subjects with Significant LBP werealso further away from their maximal forward bendingangle when transferring a pillow and transferring a 5 kg boxat bed height than all other subjects. Significant LBP subjectshad a more extended mean LLx angle when transferringa 5 kg box at bed height than subjects with No LBP.
4.4. Multivariate model
After identifying those variables within each domain(physical/lifestyle, psychological and physical) that wereindependently associated with pain group membership,five variables remained in the final model. Older age; morehours of weekly vigorous activity; a higher stress score;more use of the coping strategy ‘‘I get sick’’; and holdingthe LLx spine further from end range spinal flexion whentransferring a 5 kg box at bed height were associated withLBP group membership. Table 4 presents the odds ratios foreach variable estimated in the final ordinal regressionmodel showing the unique association of variables fromthe different domain (i.e. holding all other variables in themodel constant) with pain group membership. TheMcKelvey and Zavoina’s R2 value of this model was 0.229.
5. Discussion
The results of this study support current views that LBPis multidimensional in nature (Turk, 2005), with modifi-able personal factors across different domains associatedwith LBP. Although not severely disabling, over 30% of thisrelatively young sample of female undergraduate nursingstudents had LBP in the preceding 12 months that wouldbe regarded as clinically significant. High LBP prevalencerates in undergraduate student populations highlights theimportance of targeting prevention interventions prior tothe commencement of full-time employment (Mitchellet al., 2008; Nyland and Grimmer, 2003).
In the multivariate model, 23% of the variance betweenLBP groups was explained by personal factors fromlifestyle, psychological and physical domains. This var-iance is considerably higher when compared to previousprospective studies on LBP personal risk factors (Adamset al., 1999; Papageorgiou et al., 1997) and supportsassertions that different domains contribute indepen-dently to LBP (Leeuw et al., 2007). Despite being includedin the final model, age did not contribute significantly,which may be explained by the small mean difference (2.2

Table 3
Group comparisons of spinal angles and physical variables between (mean � standard deviation).
No LBP (n = 36) Mild LBP (n = 81) Significant LBP (n = 53) p-Value
Sitting angles
Usual LLx sit angle (8) 2.3 � 9.4 4.2 � 8.0 5.1 � 9.6 0.33
LLx sit proximity to EOR (8) 2.7 � 4.4 1.8 � 3.4 3.2 � 4.5 0.13
Standing angles
Usual LLx stand angle (8) 23.2 � 12.4 22.6 � 10.2 24.7 � 11.8 0.56
LLx sway angle (8) 31.0 � 14.4 31.0 � 13.2 31.6 � 14.0 0.97
LLx extension angle (8) 45.4 � 19.4 44.2 � 7.4 42.6 � 21.6 0.80
LLx flexion angle (8) �11.7 � 8.4 �11.6 � 6.1 �12.1 � 6.8 0.91
Functional posture angles
LLx pen angle (8) �8.5 � 8.2 �8.6 � 6.5 �6.9 � 7.7 0.40
LLx pen proximity to EOR (8) 3.3 � 3.6 3.2 � 2.6 5.3 � 5.3a 0.005
LLx 5 kg lift angle (8) �6.1 � 9.1 �5.6 � 7.2 �4.4 � 9.2 0.61
LLx 5 kg lift proximity to EOR (8) 5.7 � 5.7 6.1 � 5.1 7.8 � 6.6 0.15
LLx pillow transfer angle (8) 1.8 � 9.0 2.7 � 7.8 5.7 � 9.3 0.06
LLx pillow transfer proximity to EOR (8) 13.5 � 7.0 14.3 � 7.1b 17.8 � 8.3c,a 0.01
LLx 5 kg transfer angle (8) 6.1 � 8.7 7.8 � 8.5 10.9 � 9.3c 0.027
LLx 5 kg transfer proximity to EOR (8) 17.8 � 7.6 19.3 � 8.1b 23.0 � 9.3c,a 0.008
LLx squat angle (8) �4.1 � 9.2 �3.3 � 8.5 �2.3 � 9.5 0.65
LLx squat proximity to EOR (8) 7.8 � 6.9 8.6 � 6.4 9.8 � 8.0 0.40
Performance measures
Squat time (s) 37.7 � 21.2 36.1 � 18.8 39.9 � 23.2 0.59
Sorensen time (s) 91.7 � 48.2 85.0 � 44.6 93.0 � 56.9 0.61
LLx sitting repositioning error (8) 0.7 � 3.2 0.9 � 3.1 1.5 � 3.3 0.39
Predicted VO2 max (L/min) 2.3 � 0.4 2.3 � 0.5 2.3 � 0.4 0.69
LLx = lower lumbar, EOR = end of range flexion angle, negative angle = lumbar flexion, positive angle = lumbar extension.a Significant between Mild Pain and Significant Pain groups.b Significant between No Pain and Mild Pain groups.c Significant between No Pain and Significant Pain groups.
T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688 685
years) in age between LBP groups. The strength of thesepreliminary findings is that a modest proportion of thevariance can be attributable to factors that have thepotential to change, providing some evidence towardsdeveloping more successful LBP interventions.
5.1. Social and lifestyle factors
Subjects with Significant LBP were involved in morehours of moderate and vigorous physical activity per weekthan other subjects, however this did not translate intohigher aerobic fitness levels. Other studies report norelationship between physical activity and LBP (Bru-
Table 4
Odds ratios, 95% CIs and p-values from multivariate ordinal logistic
regression model.
Odds ratioa 95% CI p-Value
Age (years) 1.06 0.99–1.14 0.104
Lifestyle: vigorous activityb 1.30 1.05–1.62 0.015
Psychological: stressb 1.37 1.09–1.72 0.007
Psychological: ‘‘I get sick’’b 1.52 1.12–2.07 0.007
Physical: 5 kg transfer at bed
height. LLx proximity
to end range flexionb
0.56 0.39–0.79 0.001
a The odds ratio represents the proportional increase in the odds of a
higher outcome (i.e. a more severe pain group) versus a lower outcome,
holding all other variables constant, for a unit increase in the independent
variable.b To enable meaningful comparisons of odds ratios between variables a
unit increase (approximating one standard deviation) in each indepen-
dent variable is represented as; ‘‘stress’’ = 5 points, ‘‘I get sick’’ = 1 point,
‘‘vigorous activity’’ = 5 h, and ‘‘5 kg transfer’’ = 108.
magne et al., 2000; Sanya and Ogwumike, 2005). Highlevels of physical activity may be a coping strategy for LBPin this sample of female nursing students and this is inagreement with previous research that found nurses withLBP did not show signs of physical deconditioning (Schenket al., 2007). Although speculative, it is possible that thisfinding relates to increased spinal loading and a lack ofpacing strategies in these subjects. Alternatively, as themeasure of physical activity considered componentsincluding household and gardening activity, increasedhours of moderate and vigorous activity may indicateincreased exposure to bending and lifting tasks.
There were no differences between groups for any ofthe social measures including household income andsmoking. There are contrasting findings for links betweensocial measures and LBP (Dempsey et al., 1997), possiblyindicating that such measures are important only inspecific populations. This otherwise young, healthy uni-versity sample may be an example of a population who’sLBP is not strongly influenced by such measures. Alter-natively, sample size or other social factors not measuredin this study may have influenced this finding.
5.2. Psychological variables
In terms of psychological measures, high stress and ‘‘Iget sick’’ scores were included in the final multivariatemodel, indicating the importance of psychological stressand aspects of coping strategies in LBP populations. Thereis some evidence that high psychological distress levels arepredictive of future LBP episodes (Croft et al., 1995; Feyer

T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688686
et al., 2000). Recent research supports a biochemical linkbetween psychological stress and spinal pain in a workingpopulation (Schell et al., 2008), possibly associated withchanges in the regulation of the hypothalamus–pituitary–adrenal (HPA) axis (Derijk and de Kloet, 2008).
Another proposed mechanism for the relationshipbetween stress and LBP may be via direct influences ofemotions on the autonomic nervous system, resulting inaltered tissue sensitivity in some individuals (Martinez-Lavin, 2007). Descending inhibitory pain modulationsystems are known to be influenced by forebrain activityincluding emotional responses (Zusman, 2002) and longerterm stress is thought to reduce central descending tonicpain inhibition (Ashkinazi and Vershinina, 1999). Higherpsychological stress among nursing students may alsocontribute to pain via increased mechanical spinal loadingdue to higher levels of muscle tension. Marras et al. (2000)have shown that psychologically stressful environmentsproduced higher trunk muscle co-activation responses incertain female subjects. They hypothesized that thismuscle co-activation could make them more susceptibleto increased spinal loading and low back disorder risk.Although this cross-sectional study cannot distinguishwhether high stress is a characteristic of the individual or iscaused by having LBP, given subjects with acute LBP wereexcluded, high stress was less likely to be related to currentpain. This may be supported by the fact that the SignificantLBP group had LBP beliefs within a normal range (Symondset al., 1996).
The coping strategy ‘‘I Get Sick’’ was used most amongSignificant LBP subjects, and least among the No LBPsubjects. It has been proposed that individuals with poorercoping strategies are more prone to a range of healthproblems, including LBP (Leboeuf-Yde et al., 2006). ‘‘I getsick’’ is a typical somatisation response. Somatisation is acognitive style, which has been linked with LBP (Baconet al., 1994), and there is some evidence of higherprevalence in females with LBP (Schneider et al., 2006).
Perhaps the most notable measure that was not relatedto LBP was pain catastrophising, which has been reportedto be consistently higher in chronic pain populationsstudies (Peters et al., 2005; Sullivan et al., 2005). This islikely to be explained by the population sample beingyoung, otherwise healthy nursing students, withoutchronic LBP. This may also explain the lack of differencein depression and anxiety scores between the groups.
5.3. Physical variables
The importance of measuring physical variables thatare related to specific functional or pain provocative tasksis highlighted by one such variable being retained in thefinal multivariate model. The position of the LLx spinewhen transferring a box at bed height was the mostimportant physical variable. Subjects who held their LLxspine further from end range flexion were more likely to bein the Significant LBP group. Guarded or protectivemovement patterns are also associated with high levelsof protective muscle tone, and may further contribute tocompressive joint loading and pain (Dankaerts et al., 2006).As Significant LBP subjects held their LLx spine further
from end of range flexion during a number of bendingrelated functional tasks, it is speculated that these subjectswere adopting guarded type movement patterns, possiblydue to previous pain experience. Further research utilisingEMG would be required to verify this.
Measures of physical performance (fitness and endur-ance) failed to distinguish between subject groups. This isconsistent with the lack of consensus in physical factorsassociated with LBP between different studies (Dempseyet al., 1997). It is unlikely that strong associations betweensuch variables and LBP in one study population (Readyet al., 1993), and a complete lack of association in anotherpopulation (Cady et al., 1979) can be explained entirely bymethod differences. It may be that physical performancemeasures are only relevant when they relate to themechanical exposures of the specific population underinvestigation, such as fire-fighters (Cady et al., 1979) andmanual workers (O’Sullivan et al., 2006). In nursingstudents, reduced back muscle endurance may be morerelevant later in their course when they increase theirpractical nursing exposure, or once they commence work.
5.4. Limitations
These preliminary findings on this moderate sizesample of young female nursing students cannot beconsidered representative of broader populations. This isimportant to consider not only from a socio-demographicperspective, but also in terms of LBP classification.Characteristics identified as being associated with clini-cally significant but not chronic, disabling LBP in thissample may not be generalisable in other population types,males or other LBP classification. Validation of thesefindings is required in a larger, representative sample ofnursing students. Further, sub-groups of LBP were notconsidered in this study, which may have revealed otherfactors associated with different sub-groups of studentswith LBP (McCarthy et al., 2004).
Defining multidimensional pain inventory profiles(Turk and Rudy, 1988) in this study would have helpeddetermine if the findings of this study were influenced byspecific psychologic profiles, and whether female nursingstudents at risk consist of one predominant profile. It ispossible that other factors not examined in this study maycontribute to LBP variance. These include muscle activa-tion levels (Cholewicki et al., 2005), fear avoidance(Thomas and France, 2007) and genetic factors (Battieet al., 1997). Prospective data is needed to determine if thefactors identified in this cross-sectional study are pre-dictive of future LBP recurrence in this population.
6. Conclusions
This study supports that LBP is a multifactorialbiopsychosocial problem, with modifiable personal char-acteristics being associated with LBP. Increased physicalactivity, stress and coping strategies other than catastro-phising were associated with LBP. Physical measures thatare related to specific functional or pain provocative tasks,rather than general measures of physical performance,were also associated with LBP.

T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688 687
These preliminary results support the concept oftargeting modifiable personal characteristics in nursingstudents as an alternative to occupational preventionstrategies in working nurses. The findings require moreextensive investigation in prospective studies. Further, thestrength of these associations may differ across specificsub-groups of LBP.
Competing interests
Nil.
Funding
Nil.
Ethical approval
Ethical approval was obtained from university HumanResearch Ethics Committees, and all relevant ethicalconsiderations were observed.
Acknowledgements
The authors would like to thank all participants andCurtin University School of Nursing and Midwifery, EdithCowan University School of Nursing, Midwifery andPostgraduate Medicine for their support. We also thankPaul Davey for software programming and technicalassistance.
Conflict of interest
There is no conflict of interest.
References
Adams, M., Bogduk, N., Burton, K., Dolan, P., 2002. The Biomechanics ofBack Pain. Churchill Livingston, Edinburgh.
Adams, M.A., Mannion, A.F., Dolan, P., 1999. Personal risk factors for firsttime low back pain. Spine 24 (23), 2497–2505.
Ashkinazi, I., Vershinina, E.A., 1999. Pain sensitivity in chronic psychoe-motional stress in humans. Neurosci. Behav. Physiol. 29 (3), 333–337.
Astrand, P., Rodahl, K., 1986. Text Book of Work Physiology: PhysiologicalBasis of Exercise. McGraw Hill, New York.
Bacon, N.M., Bacon, S.F., Atkinson, J.H., Slater, M.A., Patterson, T.L., Grant,I., Garfin, S.R., 1994. Somatization symptoms in chronic low back painpatients. Psychosom. Med. 56 (2), 118–127.
Battie, M.C., Videman, T., Levalahti, E., Gill, K., Kaprio, J., 1997. Heritabilityof low back pain and the role of disc degeneration. Pain 131 (3), 272–280.
Beattie, P., Meyers, S., Stratford, P., Millard, R., Hollenberg, G., 2000.Associations between patient report of symptoms and anatomicimpairment visible on lumbar magnetic resonance imaging. Spine25, 819–828.
Biering-Sorensen, F., Thomsen, C., Hilden, J., 1989. Risk indicators for lowback trouble. Scand. J. Rehabil. Med. 21, 151–157.
Boersma, K., Linton, S.J., 2006. Psychological processes underlying thedevelopment of a chronic pain problem: a prospective study of therelationship between profiles of psychological variables in the fear-avoidance model and disability. Clin. J. Pain. 22 (2), 160–166.
Bolton, J.E., 1999. Accuracy of recall of usual pain intensity in back painpatients. Pain 83 (3), 533–539.
Booth, M.L., 2000. Assessment of physical activity: an internationalperspective. Res. Q. Exerc. Sport 71, s114–s120.
Brasic, J., 2003. Documentation of demographic data. Psychol. Rep. 93,151–152.
Brumagne, S., Cordo, P., Lysens, R., Verschueren, S., Swinnen, S., 2000. Therole of paraspinal muscle spindles in lumbosacral position sense inindividuals with and without low back pain. Spine 25, 989–994.
Cady, L.D., Bischoff, D.P., O’Connell, E.R., Thomas, P.C., Allan, J.H., 1979.Strength and fitness and subsequent back injuries in firefighters. J.Occup. Med. 21, 269–272.
Cholewicki, J., Silfies, S.P., Shah, R.A., Greene, H.S., Reeves, N.P., Alvi, K.,Goldberg, B., 2005. Delayed trunk muscle reflex responses increasethe risk of low back injuries. Spine 30 (23), 2614–2620.
Committee, A.a.t.N.H., 1997. New Zealand Acute Low Back Pain Guide. NZ,Wellington.
Croft, P.R., Papagerorgiou, A.C., Ferry, S., Thomas, E., Jayson, M.I.V., Silman,A.J., 1995. Psychologic distress and low back pain: evidence from aprospective study in the general population. Spine 20 (24), 2731–2737.
Dankaerts, W., O’Sullivan, P., Burnett, A., Straker, L., 2006. Differences insitting postures are associated with nonspecific chronic low back paindisorders when patients are subclassified. Spine 31 (6), 698–704.
Dawson, A.P., McLennan, S.N., Schiller, S.D., Jull, G.A., Hodges, P.W.,Stewart, S., 2007. Interventions to prevent back pain and back injuryin nurses: a systematic review. Occup. Environ. Med. 64, 642–650.
Dempsey, P., Burdorf, A., Webster, B.S., 1997. The influence of personalvariables on work-related low-back disorders and implications forfuture research. J. Occup. Environ. Med. 39, 748–759.
Derijk, R.H., de Kloet, E.R., 2008. Corticosteroid receptor polymorphisms:determinants of vulnerability and resilience. Eur. J. Pharmacol. 583(2–3), 303–311.
Eriksen, W., Bruusgaard, D., Knardahl, S., 2004. Work factors as predictorsof intense or disabling low back pain; a prospective study of nurses’aides. Occup. Environ. Med. 61, 398–404.
Fairbank, J.C., Couper, J., Davies, J., O’Brien, J., 1980. The Oswestry low backpain disability questionnaire. Physiotherapy 66, 271–273.
Feyer, A., Herbison, P., Williamson, A., de Silva, I., Mandryk, J., Hendrie, L.,Hely, M., 2000. The role of physical and psychological factors inoccupational low back pain: a prospective cohort study. Occup.Environ. Med. 57, 116–120.
Frydenberg, E., Lewis, R., 2004. Coping Scale for Adults. Administrator’sManual, Research Edition. Australian Council for EducationalResearch, Melbourne.
Gill, K.P., Bennett, S.J., Savelsbergh, G.J., van Dieen, J.H., 2007. Regionalchanges in spine posture at lift onset with changes in lift distance andlift style. Spine 32 (15), 1599–1604.
Harrison, D.D., Cailliet, R., Janik, T.J., Troyanovich, S.J., Harrison, D.E.,Holland, B., 1998. Elliptical modelling of the sagittal lumbar lordosisand segmental rotation angles as a method to discriminate betweennormal and low back pain subjects. J. Spinal Disord. 11 (5), 430–439.
Hestbaek, L., Iachine, I.A., Leboeuf-Yde, C., Kyvik, K.O., Manniche, C., 2004.Heredity of low back pain in a young population: a classical twinstudy. Twin Res. 7 (1), 16–26.
Hodges, P.W., Moseley, G.L., Gabrielsson, A., Gandevia, S.C., 2003. Experi-mental muscle pain changes feedforward postural responses of thetrunk muscles. Exp. Brain Res. 151 (2), 262–271.
Jordan, K., Haywood, K.L., Dziedzic, K., Garratt, A.M., Jones, P.W., Ong, B.N.,Dawes, P.T., 2004. Assessment of the 3-dimensional Fastrak measure-ment system in measuring range of motion in ankylosing spondylitis.J. Rheumatol. 31 (11), 2207–2215.
Kujala, U.M., Taimela, S., Viljanen, T., 1999. Leisure physical activity andvarious pain symptoms among adolescents. Br. J. Sports Med. 33 (5),325–328.
Kuornika, I., Jonsson, B., Kilbom, A., Vinterberg, H., Biering-Sorensen, F.,Andersson, G., Jorgensen, K., 1987. Standardised Nordic question-naires for the analysis of musculoskeletal symptoms. Appl. Ergon.18, 233–237.
Leboeuf-Yde, C., Larsen, K., Ahlstrand, I., Volinn, E., 2006. Coping and backproblems: analysis of multiple data sources on an entire cross-sec-tional cohort of Swedish military recruits. BMC Musculoskelet. Dis-ord. 7, 39.
Leeuw, M., Goossens, M.E., Linton, S.J., Crombez, G., Boersma, K., Vlaeyen,J.W., 2007. The fear-avoidance model of musculoskeletal pain: cur-rent state of scientific evidence. J. Behav. Med. 30 (1), 77–94.
Lovibond, S., Lovibond, P., 1995. Manual For The Depression AnxietyStress Scales. Psychology Foundation, Sydney.
Marras, W.S., Davis, K., Heaney, C., Maronitis, A.B., Allread, W.G., 2000. Theinfluence of psychosocial stress, gender and personality on mechan-ical loading of the lumbar spine. Spine 25, 3045–3054.
Marras, W.S., Ferguson, S.A., Burr, D., Schabo, P., Maronitis, A., 2007. Lowback pain recurrence in occupational environments. Spine 32 (21),2387–2397.
Martinez-Lavin, M., 2007. Biology and therapy of fibromyalgia. Stress, thestress response system, and fibromyalgia. Arthritis Res. Ther. 9 (4),216.

T. Mitchell et al. / International Journal of Nursing Studies 46 (2009) 678–688688
McCarthy, C., Frances, A., Strimpakos, N., Freemont, A., Oldham, J., 2004.The biopsychosocial classification of non-specific low back pain: asystematic review. Phys. Ther. Rev. 9, 17–30.
Mercado, A.C., Carroll, L.J., Cassidy, J.D., Cote, P., 2005. Passive coping is arisk factor for disabling neck or low back pain. Pain 117 (1–2), 51–57.
Mitchell, T., O’Sullivan, P.B., Burnett, A.F., Straker, L., Rudd, C., 2008. Lowback pain characteristics from undergraduate student to workingnurse in Australia: a cross-sectional survey. Int. J. Nurs. Stud.,doi:10.1016/j.ijnurstu.2008.1003.1001.
Moffroid, M., Reid, S., Henry, S., Haugh, L., Ricamato, A., 1994. Someendurance measures in persons with chronic low back pain. J. Orthop.Sports Phys. Ther. 2, 81–87.
Mohseni-Bandpei, M.A., Fakhri, M., Bagheri-Nesami, M., Ahmad-Shirvani,M., Khalilian, A.R., Shayesteh-Azar, M., 2006. Occupational back painin Iranian nurses: an epidemiological study. Br. J. Nurs. 15 (17), 914–917.
Nyland, L., Grimmer, K., 2003. Is undergraduate physiotherapy a riskfactor for low back pain? A prevalence study of LBP in physiotherapystudents. BMC Musculoskelet. Disord. 4, doi:10.1186/1471-2474-1184-1122.
O’Sullivan, P., Burnett, A., Floyd, A., Gadsden, K., Loguidice, J., Miller, D.,Quirke, H., 2003. Lumbar repositioning deficit in a specific low backpain population. Spine 28, 1074–1079.
O’Sullivan, P., Grahamslaw, K., Kendell, M., Lapenskie, S., Moller, N.,Richards, K., 2002. The effect of different standing and sitting postureson trunk muscle activity in a pain free population. Spine 27, 1238–1244.
O’Sullivan, P., Mitchell, T., Bulich, P., Waller, R., Holte, J., 2006. Therelationship between posture and back muscle endurance in indus-trial workers with flexion-related low back pain. Man. Ther. 11, 264–271.
Papageorgiou, A.C., Macfarlane, G.J., Thomas, E., Croft, P.R., Jayson, M.I.V.,Silman, A.J., 1997. Psychosocial factors in the workplace—do theypredict new episodes of low back pain? Spine 22 (10), 1137–1142.
Pearcy, M., Hindle, R., 1989. A new method for the non-invasive three-dimensional measurement of human back movement. Clin. Biomech.4, 73–79.
Perich, D., Burnett, A.F., O’Sullivan, P.B., 2006. Low back pain and factorsassociated with it: examination of adolescent female rowers. In:XXIVth Symposium on Biomechanics in Sports. University of Salz-burg, Salzburg, pp. 355–358.
Peters, M.L., Vlaeyen, J.W., Weber, W.E., 2005. The joint contribution ofphysical pathology, pain-related fear and catastrophizing to chronicback pain disability. Pain 113, 45–50.
Power, C., Frank, J., Hertzman, C., Schierhout, G., Li, L., 2001. Predictors oflow back pain onset in a prospective British study. Am. J. Public Health91 (10), 1671–1678.
Ready, A.E., Boreskie, S.L., Law, S.A., Russell, R., 1993. Fitness and lifestyleparameters fail to predict back injuries in nurses. Can. J. Appl. Physiol.18 (1), 80–90.
Sanya, A.O., Ogwumike, O.O., 2005. Low back pain prevalence amongstindustrial workers in the private sector in Oyo State, Nigeria. Afr. J.Med. Med. Sci. 34 (3), 245–249.
Schell, E., Theorell, T., Hasson, D., Arnetz, B., Saraste, H., 2008. Stressbiomarkers’ associations to pain in the neck, shoulder and back in
healthy media workers: 12-month prospective follow-up. Eur. SpineJ. 17 (3), 393–405.
Schenk, P., Laubli, T., Hodler, J., Klipstein, A., 2007. Symptomatology ofrecurrent low back pain in nursing and administrative professions.Eur. Spine J. 16, 1789–1798.
Schneider, S., Randoll, D., Buchner, M., 2006. Why do women have backpain more than men? A representative prevalence study in the federalrepublic of Germany. Clin. J. Pain 22 (8), 738–747.
Scott Long, J., Freese, J., 2006. Regression Models for Categorical Depen-dent Variables Using Stata. StataCorp LP, College Station, TX.
Shelerud, R.A., 2006. Epidemiology of occupational low back pain. Clin.Occup. Environ. Med. 5 (3), 501–528.
Smedley, J., Egger, P., Cooper, C., Coggon, D., 1997. Prospective cohortstudy of predictors of incident low back pain in nurses. Br. Med. J. 315,550–551.
Sullivan, M., Bishop, S., Pivik, J., 1995. The pain catastrophising scale:development and validation. Psych. Assess. 7, 524–532.
Sullivan, M.J., Lynch, M.E., Clark, A.J., 2005. Dimensions of catastrophicthinking associated with pain experience and disability in patientswith neuropathic pain conditions. Pain 113, 310–315.
Swinkels-Meewisse, I.E., Roelofs, J., Oostendorp, R.A., Verbeek, A.L.,Vlaeyen, J.W., 2006. Acute low back pain: pain-related fear and paincatastrophizing influence physical performance and perceived dis-ability. Pain 120 (1–2), 36–43.
Symonds, T.L., Burton, A.K., Tillotson, K.M., Maine, C.J., 1996. Do attitudesand beliefs influence work loss due to low back trouble? Occup. Med.46, 25–32.
Thomas, J.S., France, C.R., 2007. Pain-related fear is associated withavoidance of spinal motion during recovery from low back pain.Spine 32 (16), E460–E466.
Turk, D.C., 2005. The potential of treatment matching for subgroups ofpatients with chronic pain: lumping versus splitting. Clin. J. Pain 21(1), 44–55.
Turk, D.C., Rudy, T.E., 1988. Toward an empirically derived taxonomy ofchronic pain patients: integration of psychological assessment data. J.Consult. Clin. Psychol. 56, 233–238.
Videman, T., Ojajarvi, A., Riihimaki, H., Troup, J., 2005. Low back painamong nurses. A follow up beginning at entry to the nursing school.Spine 30, 2334–2341.
Violante, F., Fiori, M., Fiorentini, C., Risi, A., Garagnani, G., Bonfiglioli, R.,Mattioli, S., 2004. Associations of psychosocial and individual factorswith three different categories of back disorder among nursing staff. J.Occup. Health 46, 100–108.
Waddell, G., 2004. The Back Pain Revolution. Churchill Livingstone,London.
Wedderkopp, N., Kjaer, P., Hestbaek, L., Korsholm, L., Leboeuf-Yde, C.,2008. High-level physical activity in childhood seems to protectagainst low back pain in early adolescence. Spine J..
Wong, T.K., Lee, R.Y., 2004. Effects of low back pain on the relationshipbetween the movements of the lumbar spine and hip. Hum. Mov. Sci.23 (1), 21–34.
Yip, V.Y., 2004. New low back pain in nurses: work activities, work stressand sedentary lifestyle. J. Adv. Nurs. 46, 430–440.
Zusman, M., 2002. Forebrain-mediated sensitization of central painpathways: ‘non-specific’ pain and a new image for MT. Man. Ther.7 (2), 80–88.