-
8/20/2019 Biopsy - Technique
1/25
Biopsy Techniques:Skin Lesions
-
8/20/2019 Biopsy - Technique
2/25
Indications (indikasi)
• To make or confirm histopathologic diagnoses
(utk membuat atau mengkonfirmasi diagnosishistopatologi )
• Definitive treatment of abnormal, malignant,
and atypical lesions
• Elective removal for cosmetic reasons
-
8/20/2019 Biopsy - Technique
3/25
Contraindications
• Infection at biopsy site• Bleeding disorder
• Allergy to local anesthetics
-
8/20/2019 Biopsy - Technique
4/25
Risks
• Bleeding– Avoid NSAIDs or ASA 10 days before large
excisions
– Switch from warfarin to heparin for large excisions
• Infection
• Scar– More common in children, young adults
– Higher risk areas: mandible, chest, neck, shoulders, hands,
feet
– Previous history of keloid formation• Nerve damage
– Face high risk area: facial motor nerve runs very close
todermal layer. Nerves run in subcutaneous fat plane.
-
8/20/2019 Biopsy - Technique
5/25
Risks
• Allergy to local anesthetics– Type I
• can occur w/o previous exposure. Rare
– Type IV: delayed hypersensitivity.• Needs previous
exposure
• Usually local reactions, rash, contact dermatitis.
– Amide agents• lidocaine, mepivicaine, bupivicaine,
etidocaine
• Most commonly used agents
• Allergy is EXTREMEMLY rare.
– Ester agents• procaine, tetracaine, chloroprocaine
– Bacteriostatic saline or injectable diphenhydramine• Mild
anesthetic effect. Lasts 15 minutes.
-
8/20/2019 Biopsy - Technique
6/25
Risks
• Allergy to topical antibiotics
– Neomycin. 3rd most common contact allergen in U.S.–
Bacitracin. 6th most common contact allergen in U.S.
-
8/20/2019 Biopsy - Technique
7/25
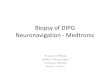
Description of Lesion
Flat
• Macule < 1 cm
• Patch > 1 cm
Raised
• Papule < 1 cm
• Nodule 1-2 cm
• Tumor > 2 cm
• Plaque. Flat,
elevated with
surface area >
height.
• Indurated. Firm
Pedunculated
-
8/20/2019 Biopsy - Technique
8/25
How to chose your biopsy type ?
• Flat– Punch or ellipse
• Raised– Punch or ellipse if worried about melanoma
– Shave in other cases
• Indurated– Punch or ellipse
• Pedunculated
– Shave or scissors
-
8/20/2019 Biopsy - Technique
9/25
Where should I biopsy?
• Pigmented lesion– Excise entire specimen. 1-3 mm margins
• Rash– Developed but not excoriated lesion
–Multiple biopsies– Biopsy at edge of lesions
– 4 mm punch
• Blistering disorder– Excise entire blister or at blister
edge
• Formalin for histopathology– Biopsy peri-lesional normal
skin
• Saline soaked gauze for Direct Immunoflorescence (DIF)
-
8/20/2019 Biopsy - Technique
10/25
How deep should you go?
• Punch & elliptical biopsies
• When concerned about melanoma
Prognosis based on depth
• Easier extraction of specimen
• Shave biopsies
• Raised or pedunculated
• Not worried about
melanoma
Through epidermis/dermis into
subcutaneous fat
Through epidermis &
dermis
-
8/20/2019 Biopsy - Technique
11/25
Supplies & Instruments
• Prep solution– Isopropyl alcohol, povidone-iodine,
chlorhexadine
• Drapes
• Gauze• Syringes• Needles
– 18 or 20 G to draw up. 25 or 30 G to inject.
• Anesthetic– Lidocaine (0.5, 1 or 2%) with or without
epinephrine– Epinephrine okay to use on digits/acral areas
-
8/20/2019 Biopsy - Technique
12/25
Supplies & Instruments
• Punch biopsy (3mm-8mm)
• # 15 blade scalpel
• Iris scissors, forceps with teeth, needle driver
• Suture– Nylon, absorbable or prolene (blue)
– 4-0 or 5-0 with P-3 or FS-3 needle. 6-0 on face.
• Hemostatic agent– Aluminum chloride (Drysol)
– Silver nitrate sticks. May stain skin brown• Processing
solution (formalin, saline, etc)
• Dressing supplies
-
8/20/2019 Biopsy - Technique
13/25
Shave biopsy
• Create wheal to elevatelesion
• Stretch & stabilize skin• #15 blade held parallel
to skin
• Smooth sweeping strokes
• Near end of excision, place forceps on top of lesion to
stabilize and prevent tearing with exit of blade
-
8/20/2019 Biopsy - Technique
14/25
Punch Biopsy
• Determine direction of skin tension
lines
• Stabilize skin with thumb/forefinger
• Consider stretching skin perpendicular
to skin lines to create ellipse
• Place punch perpendicular to skin
• Apply firm downward pressure with acircular motion until
reach sub-Q fat.
Will feel “give”
• Forceps to remove lesion. Cut at base
-
8/20/2019 Biopsy - Technique
15/25
Fusiform (Elliptical)
Excision
• Align long axis of excision parallel to skin tension lines•
Draw ellipse
– 2-5 mm wound margins– 30 degree angles at each apex– Length is
3-4 times the width
• #15 blade scalpel
• Undermine at level of sub-Q fat with scalpel or scissor• Place
stitch at one end of biopsy sample
– Helps to identify orientation of sample
• Undermine wound edges in preparation for suturing
-
8/20/2019 Biopsy - Technique
16/25
Processing biopsy specimens
• Histopathology– 10% buffered formalin
• Direct immunoflorescence
– Dx of blistering disease, SLE, etc.– Michel’s solution
– Saline soaked gauze. Do not let specimen dry out
• Bacterial or fungal cultures
– Sterile container with nonbacteriostatic saline• Viral
studies
– Viral transport media
-
8/20/2019 Biopsy - Technique
17/25
To suture or not to suture?
• Does this biopsy need a stitch?– RCT comparing primary
(suture) vs secondary healing
in 4 mm vs. 8 mm punch biopsies.• Doctors: no difference in
healing or cosmesis
in 4 mm or 8 mm biopsies.• Patients: no difference in healing or
cosmesis
in 4 mm biopsy. Better cosmesis with suture in 8 mm bx.
• Sutures-- Monofilament nylon (Ethilon)-- Polypropylene
(Prolene)
• What about absorbable sutures?– Some evidence: absorbable
polyglactin (Vicryl) suturesequal to nylon sutures in rates of
infection, redness,dehisence, scar hypertrophy, patient
satisfaction.
-
8/20/2019 Biopsy - Technique
18/25
Simple Suture
-
8/20/2019 Biopsy - Technique
19/25
Vertical Mattress Suture
-
8/20/2019 Biopsy - Technique
20/25
Post Procedure Care
• Wounds heel faster when moist– Vaseline or antibiotic
ointment
• Occlusive or semi-occlusive dressing• Remove bandage after
12-24 hrs
• Cleanse with soap/water twice daily
• Bandage for approx 5 days or until re-epithelialized
• Shower okay with sutures. Avoid soaking
• Avoid activities that will put stress on sutures
-
8/20/2019 Biopsy - Technique
21/25
Suture Removal
• Face
– 4-6 days; apply Steri-Strips
• Chest, abdomen, upper extremities, scalp
– 7-10 days
• Back, lower extremities– 12-20 days
-
8/20/2019 Biopsy - Technique
22/25
Pathology Forms: Essential Information
• The 6 D’s
Demographics: age, gender, ethnicity
Description:
-location, color, symptoms, other areas of involvement,previous
therapy or biopsy.
Diseases & Drugs
Duration of condition
Diameter of lesion or eruption
Diagnosis: in order of likelihood-Can be broad categories
such as malignancy,
dermatitis, infection.
-Avoid terms like “rule out”
-
8/20/2019 Biopsy - Technique
23/25
Documentation
• Diagnosis: Reason for procedure
• Description and location of lesion
• Procedure: Shave vs. Punch vs. Ellipse• Consent: Risks and
benefits reviewed
• Prep and Anesthesia
• Description of procedure
• Specimen disposition
• Patient education and follow-up
-
8/20/2019 Biopsy - Technique
24/25
Follow-up of pathology results
• No uniform recommendations
• Interpretation requires understanding ofclinical scenario
• Work closely with your dermatologist
• Get to know YOUR dermatopathologist
-
8/20/2019 Biopsy - Technique
25/25
The End