Embed Size (px)
Citation preview
Biopharmaceutics
Route of Administration,Anatomy & physiology affecting absorption and
Transit of Drugs
Lec:2
Ali Y Ali BSc Pharmacy, MSc Industrial Pharmaceutical Sciences
Dept. of Pharmaceutics School of Pharmacy
University of Sulaimani 1
Overview
• Introduction • Routes of drug administration • Physiological factors affecting oral drug absorption • Transit of Pharmaceuticals in the GIT
• Barriers to Drug Absorption
2
IntroductionPhysicochemical
properties
Dosage form Route of
Administration
Bioavailability(Rate & Extent)
3
Introduction
Factors affecting bioavailability depends on • The route of the administration.
– IV (100 %)
– Other routes: Oral, dermal, pulmonary, rectal• Absorption
4
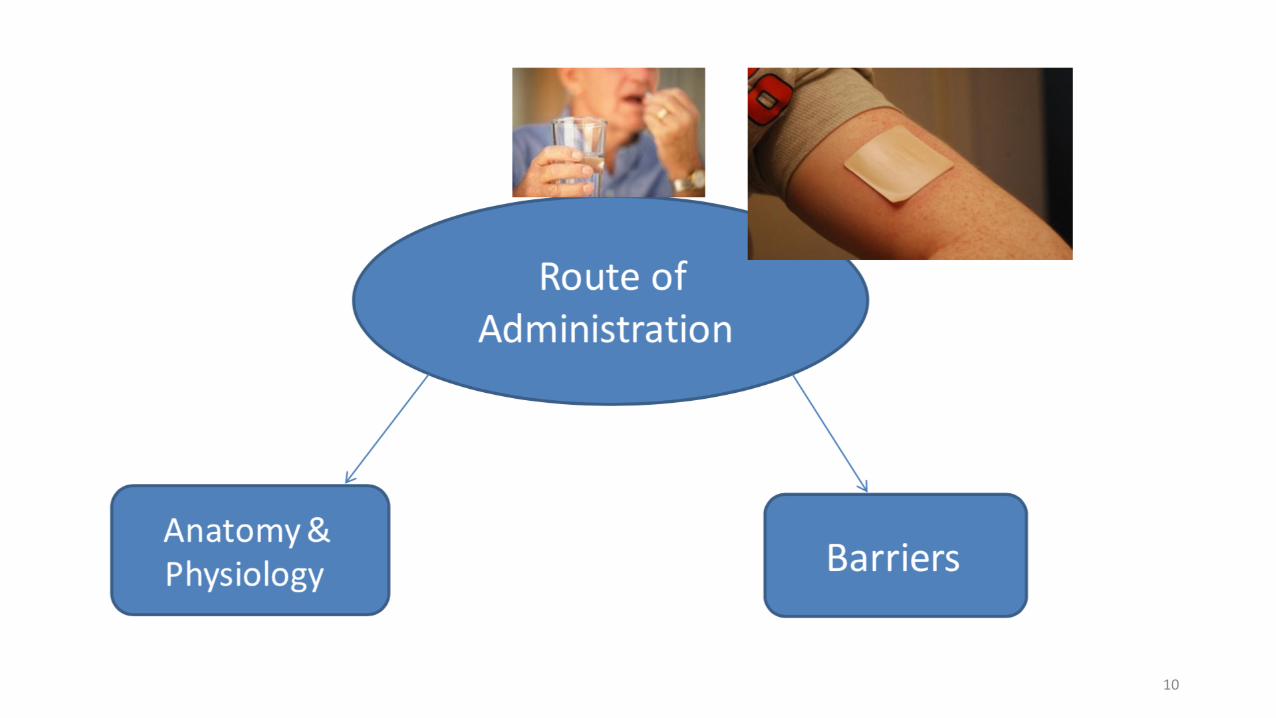
Routes of Drug Administration
1. Parenteral
2. Enteral
3. Miscellaneous
5
Parenteral
• Intravenous (IV) Bolus:• Bioavailability:
• Extent: 100 % systemic absorption • Rate: instantaneously in the blood
• IV infusions • Extent: 100 % systemic absorption • Rate: controlled by the rate of infusion
6
Parenteral
• Intramuscular (IM)• Bioavailability:
• Rapid absorption rate is rapid from aqueous solution • Slow absorption form oily based solution (Depot)
• Subcutaneous (SC): • Bioavailability:
• Rapid absorption from aqueous solution • Slow absorption form repository formulations
7
Enteral
• Buccal or sublingual(SL)• Rapid absorption for lipid soluble drugs
• Oral (PO)• Absorption may vary • Slower than fast parenteral like IM and IV bolus
• Rectal (PR)• Absorption may vary from suppository• More reliable from enema (solution)
8
Miscellaneous
• Transdermal • Slow absorption • Rate of absorption varies
• Inhalation and Intranasal • Rapid absorption • Total amount absorbed varies
9
10
Oral route
• Most popular• Natural and convenient for patient• Relatively easy to manufacture oral dosage forms
• Compact• Not sterilized• Inexpensive
• https://www.youtube.com/watch?v=GtZm4Iyb_Mo
11
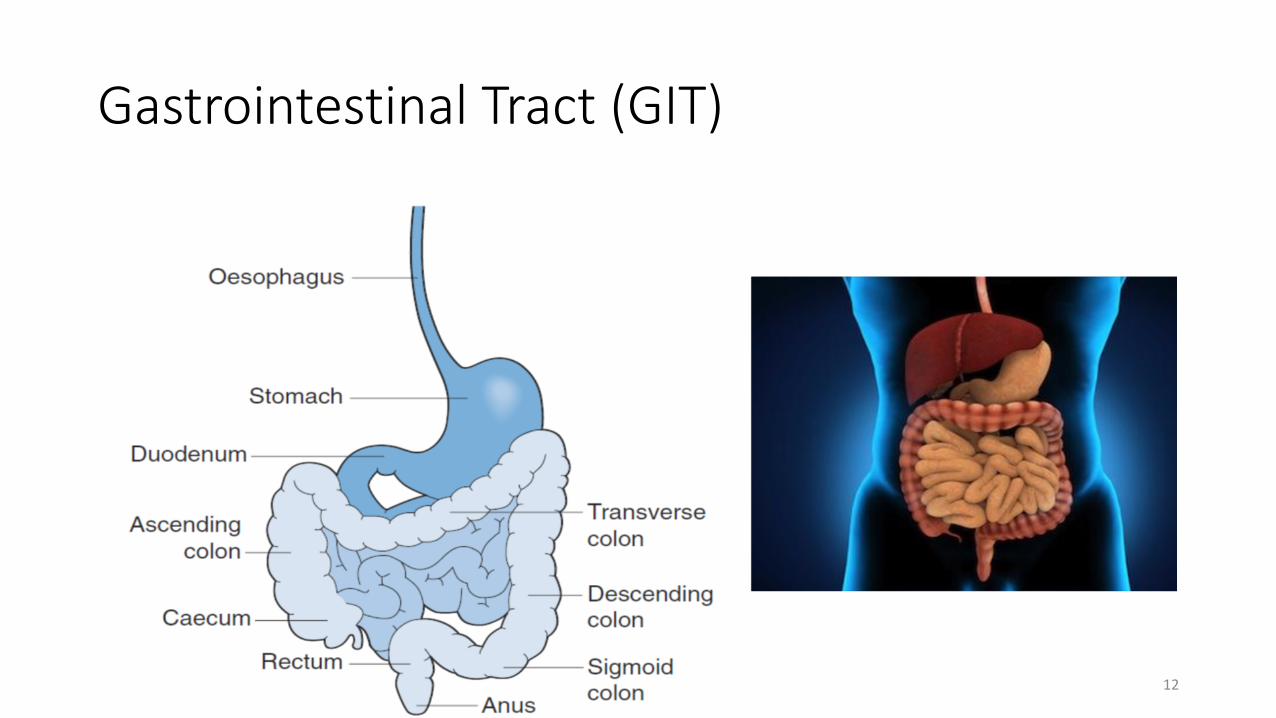
Gastrointestinal Tract (GIT)
12
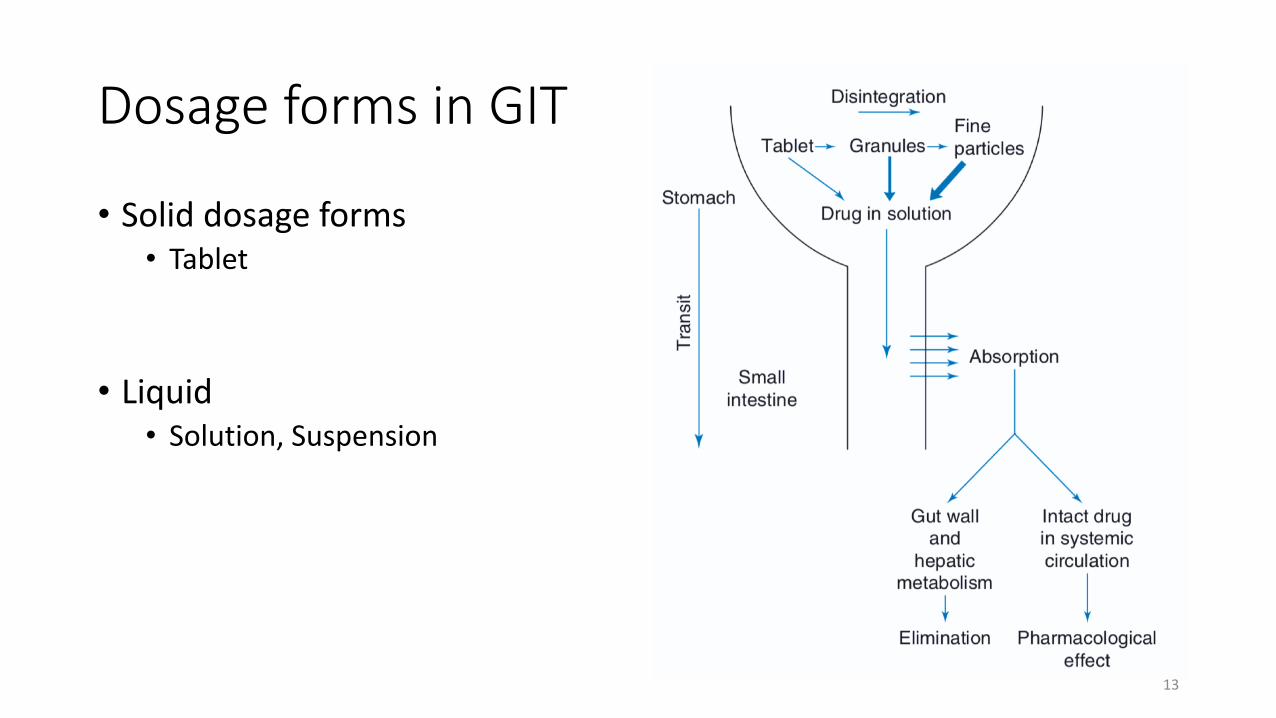
Dosage forms in GIT
• Solid dosage forms • Tablet
• Liquid • Solution, Suspension
13
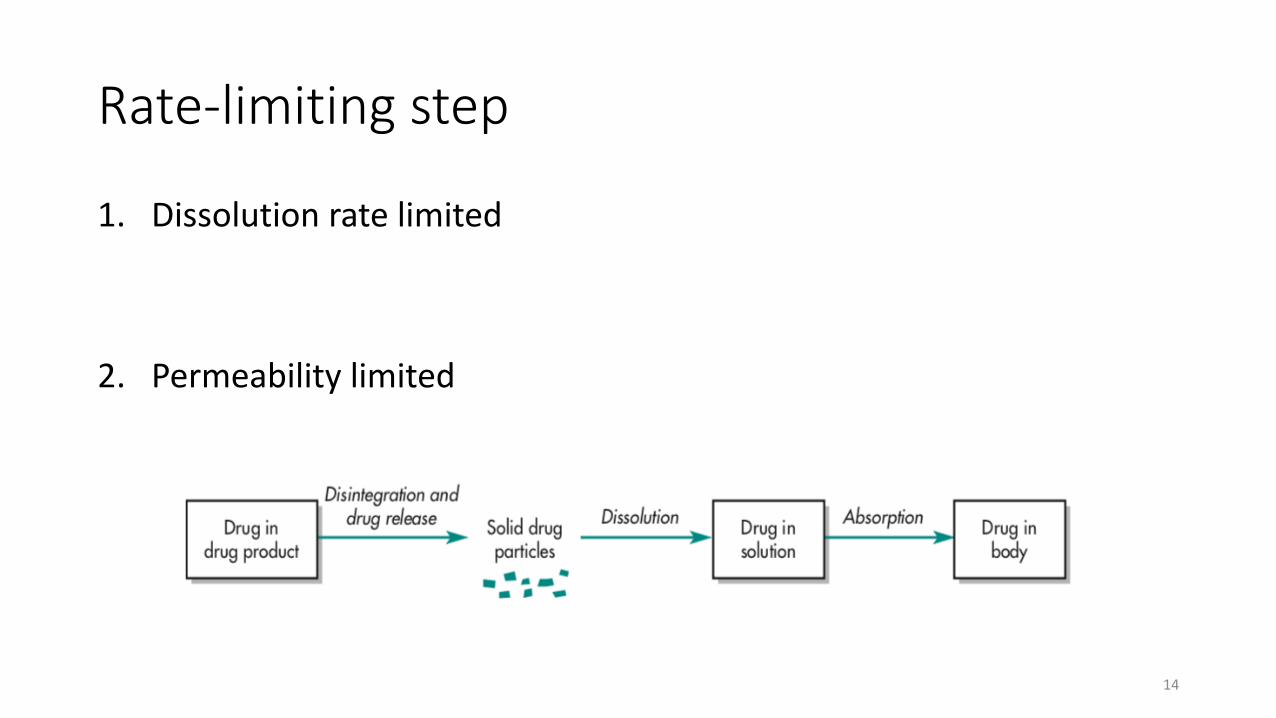
Rate-limiting step
1. Dissolution rate limited
2. Permeability limited
14
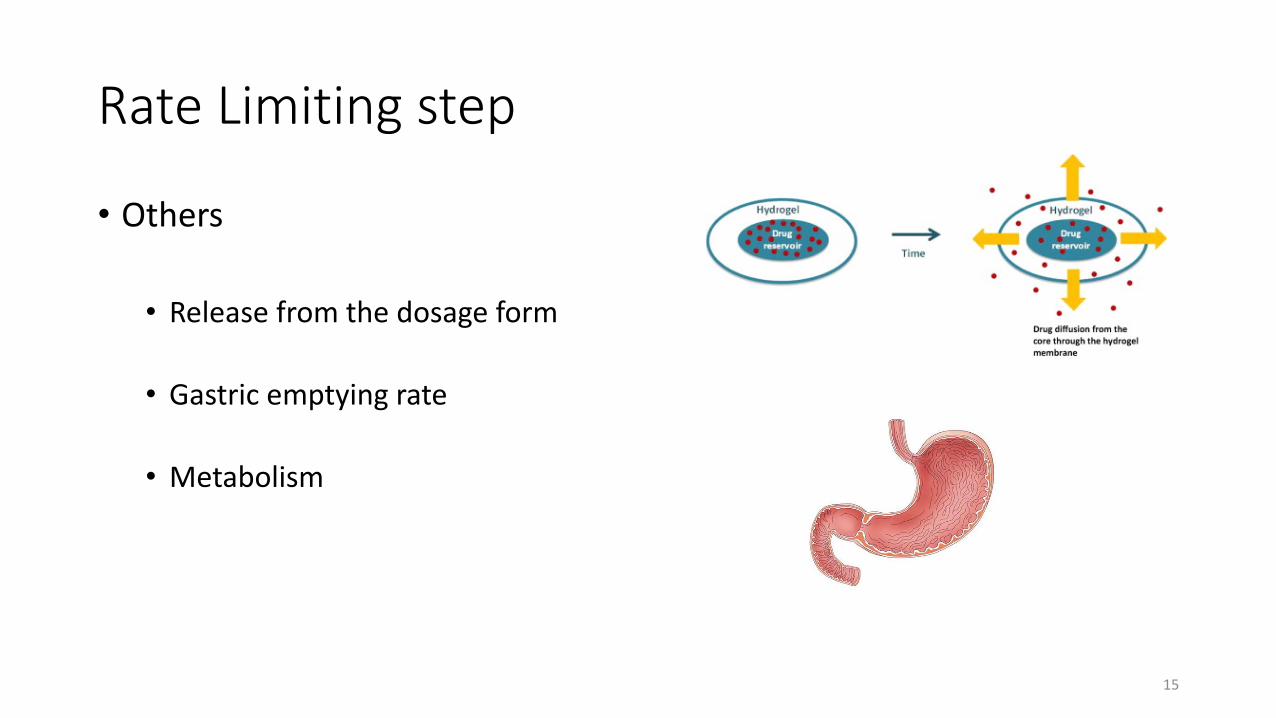
Rate Limiting step
• Others
• Release from the dosage form
• Gastric emptying rate
• Metabolism
15
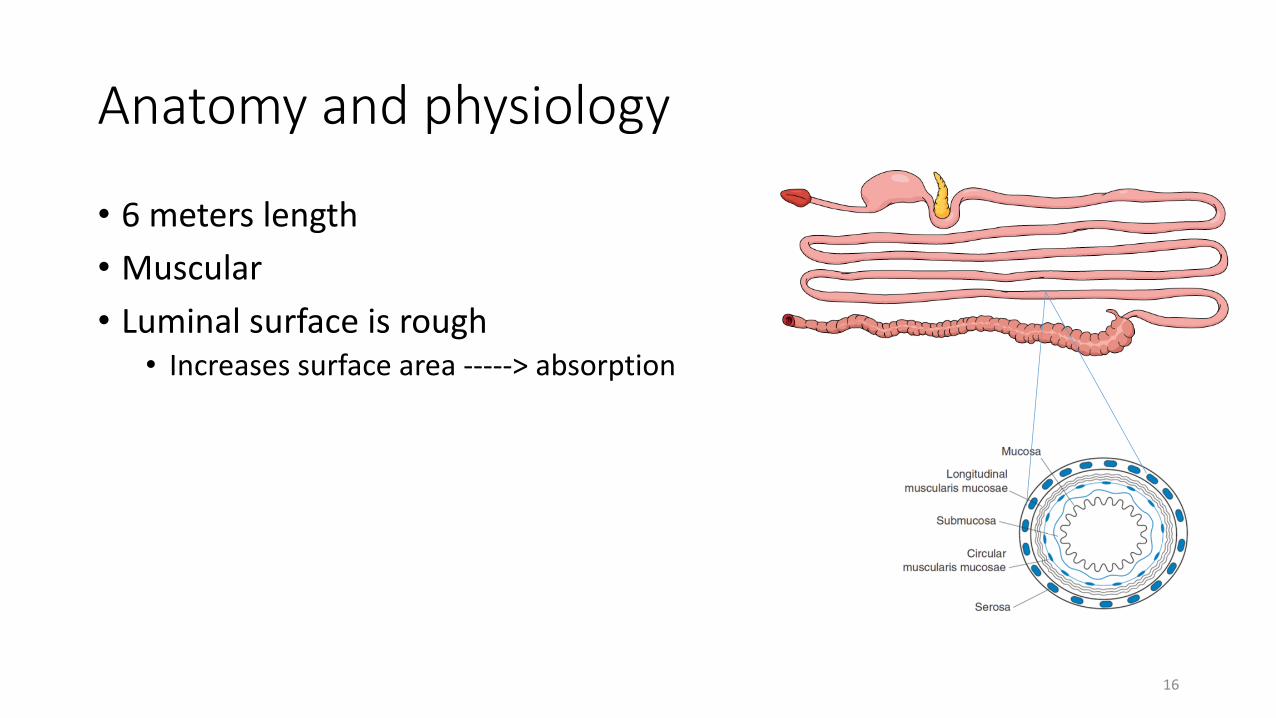
Anatomy and physiology
• 6 meters length • Muscular • Luminal surface is rough• Increases surface area -----> absorption
16
Mucus
• Secreted by GIT • Covers majority of GIT (Continuous in stomach and Duodenum)
• Functions • Protective
• Composition;• Water (95%)• Mucin (large glycoprotein)
17

Oral cavity
• Portal • pH = 7 • Saliva • Amylase
• Mucin
• Oral dispersing tablets (ODT)• Aripiprazole discemelt®
18
Oesophagus
• Links oral cavity to the stomach• Length 25cm and 2 cm diameter
• Mostly covered by epithelial cells
19
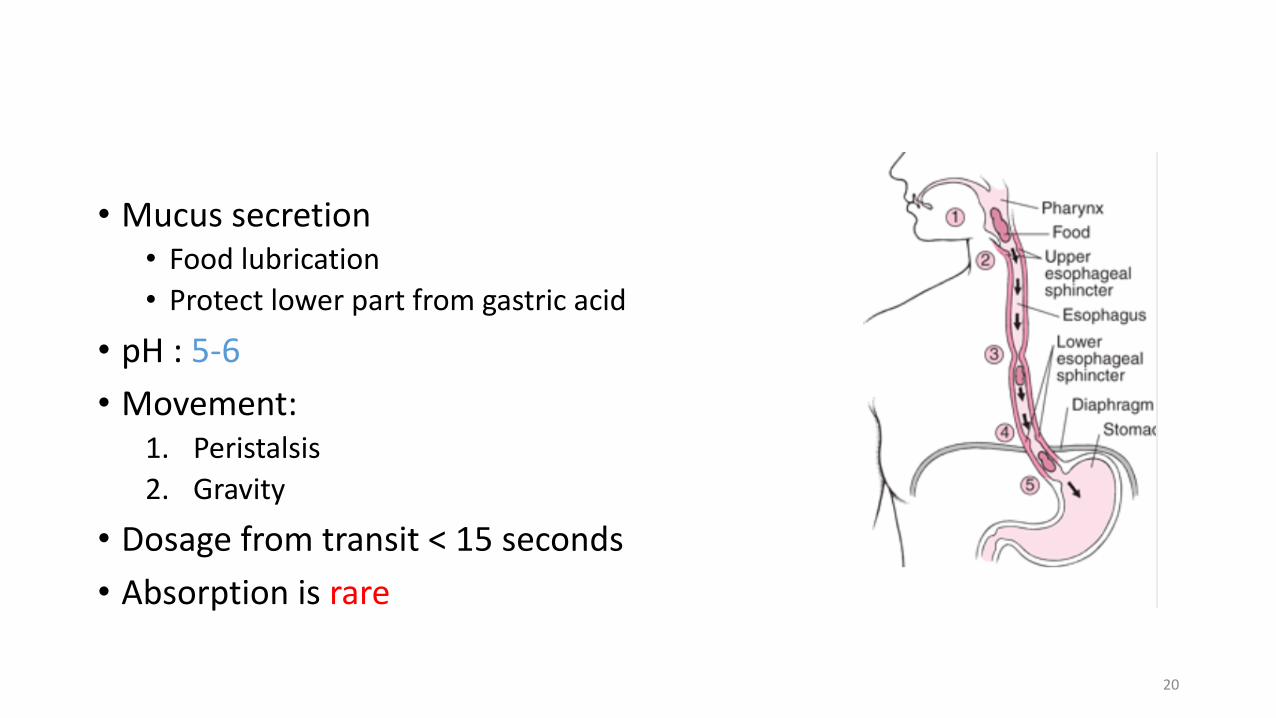
• Mucus secretion • Food lubrication • Protect lower part from gastric acid
• pH : 5-6• Movement:
1. Peristalsis 2. Gravity
• Dosage from transit < 15 seconds • Absorption is rare
20
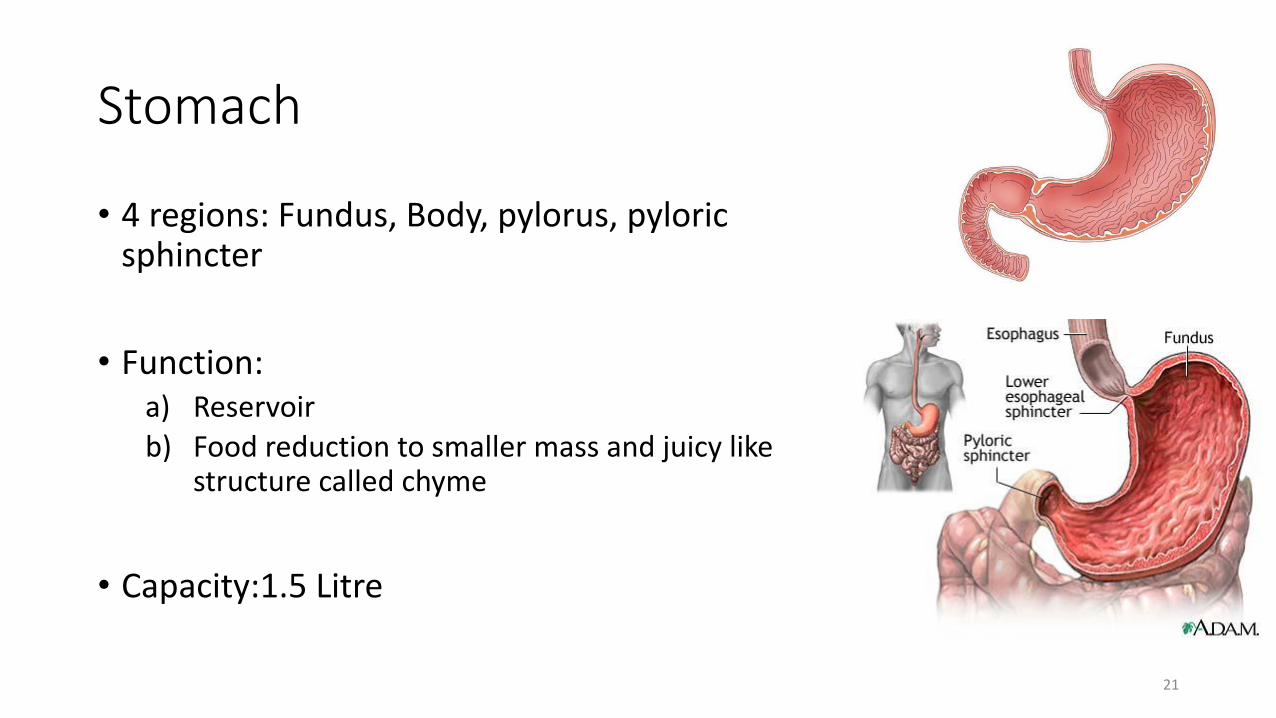
Stomach
• 4 regions: Fundus, Body, pylorus, pyloric sphincter
• Function:a) Reservoir b) Food reduction to smaller mass and juicy like
structure called chyme
• Capacity:1.5 Litre
21
Fasting State
• Gastric juice 1. Acid: parietal cells
2. Gastrin hormone; stimulates acid secretion, in response of presence of proteins and peptides
3. Pepsin: pepsinogen converted at low pH pepsin to break down small peptides
4. Mucus: protection
22
Stomach
• Absorption ?
23
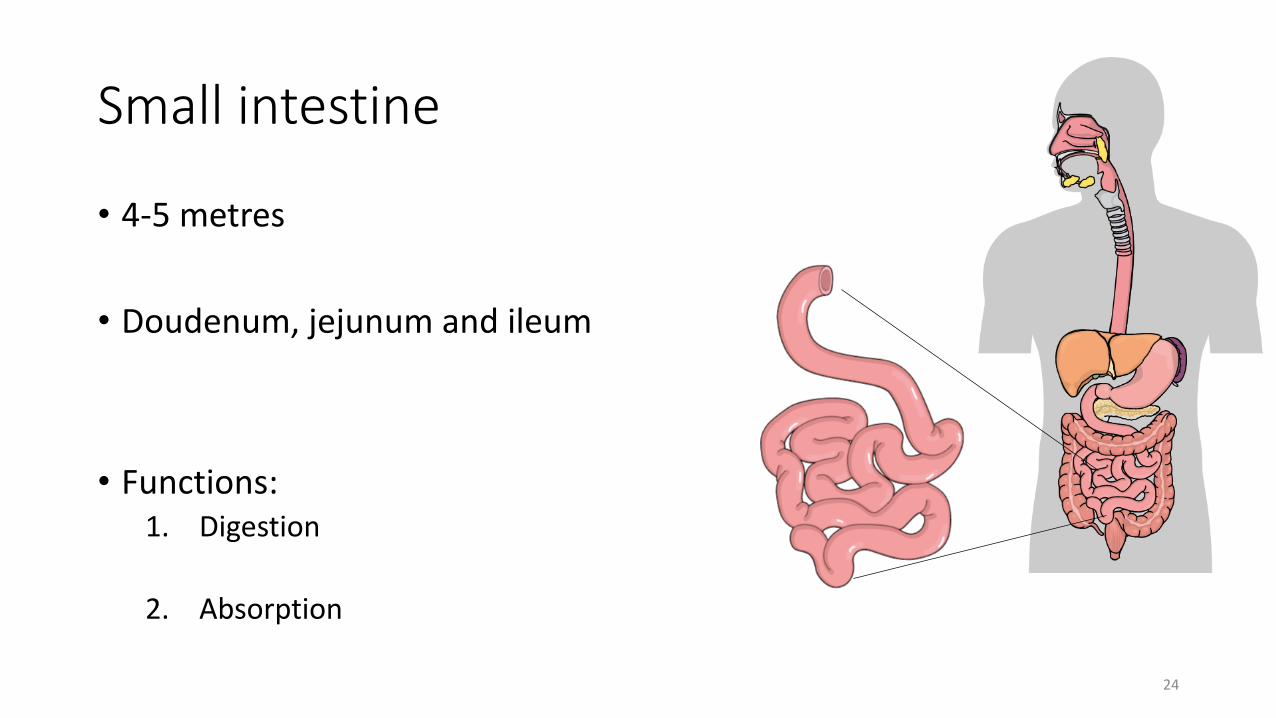
Small intestine
• 4-5 metres
• Doudenum, jejunum and ileum
• Functions:1. Digestion
2. Absorption
24
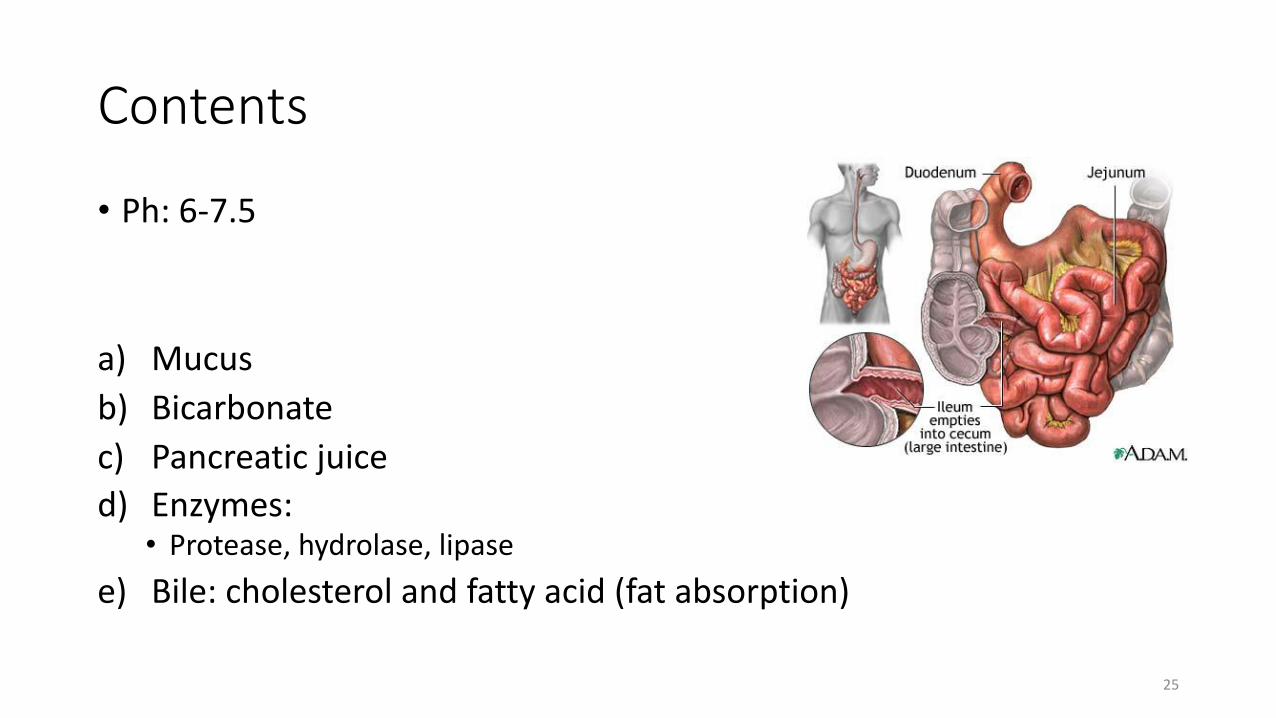
Contents
• Ph: 6-7.5
a) Mucus b) Bicarbonate c) Pancreatic juice d) Enzymes: • Protease, hydrolase, lipase
e) Bile: cholesterol and fatty acid (fat absorption)
25
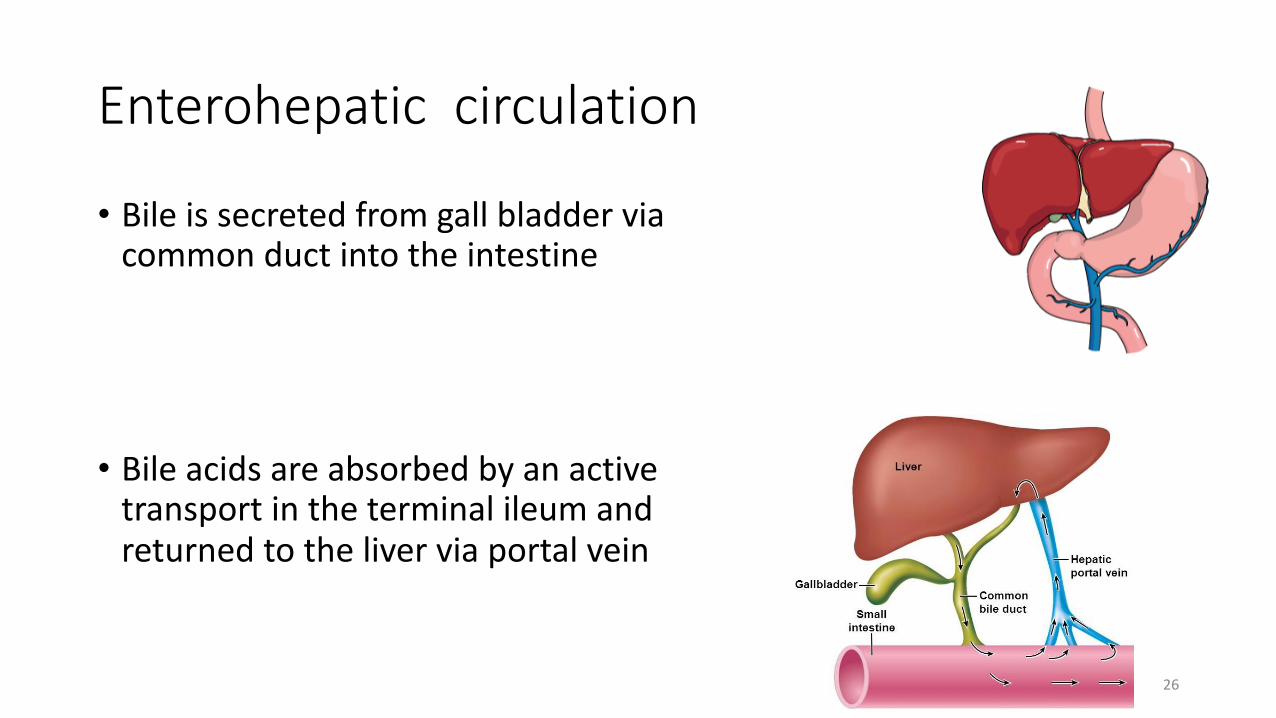
Enterohepatic circulation
• Bile is secreted from gall bladder via common duct into the intestine
• Bile acids are absorbed by an active transport in the terminal ileum and returned to the liver via portal vein
26
Small Intestine
• Absorption ?
• Major site ?
27
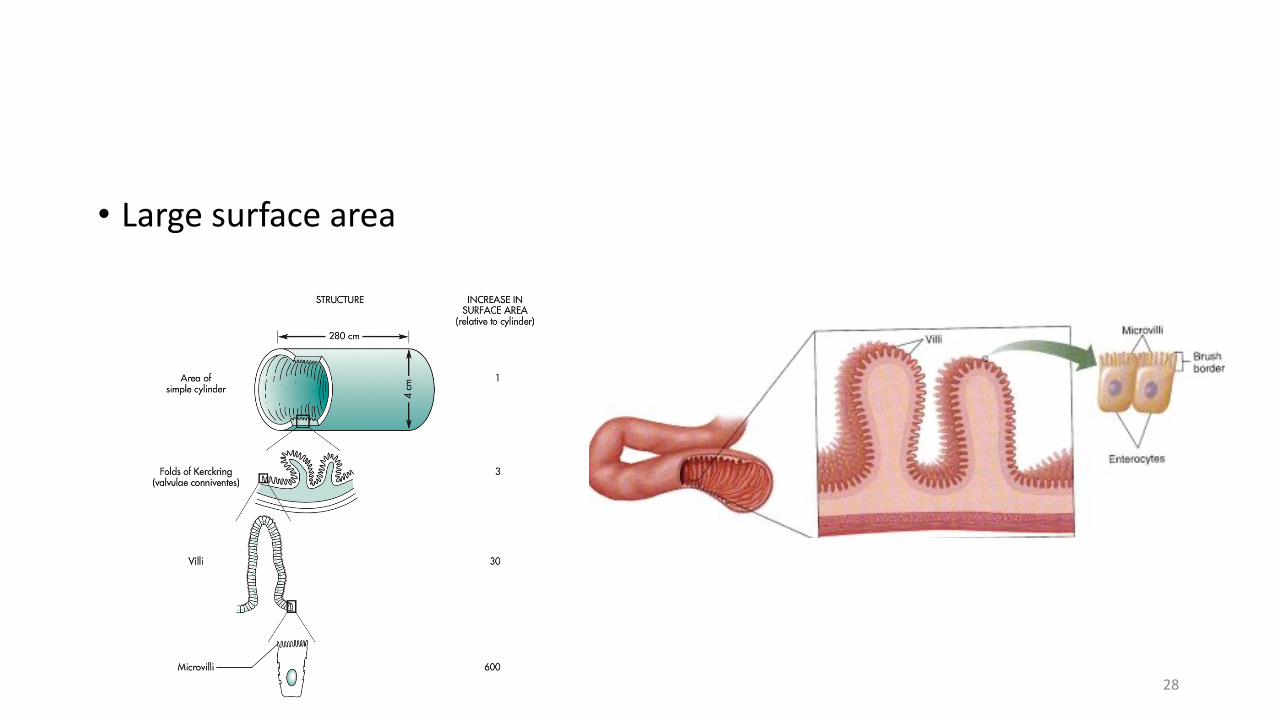
• Large surface area
28
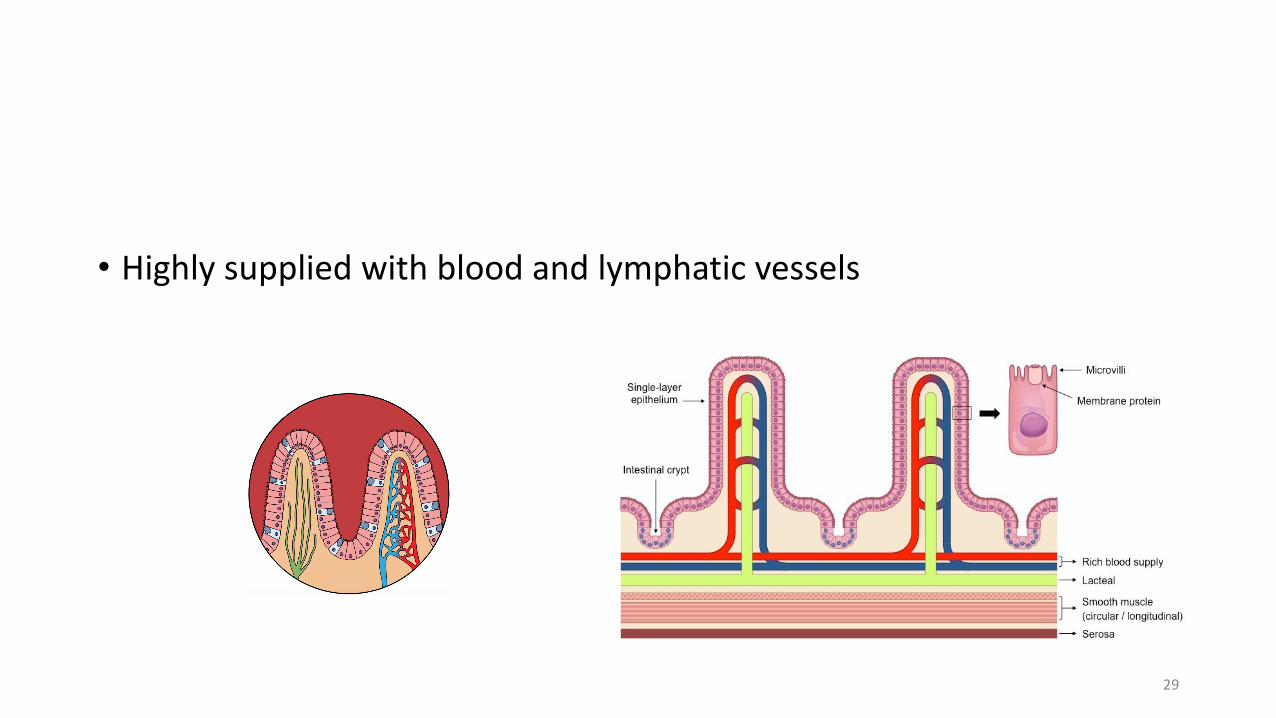
• Highly supplied with blood and lymphatic vessels
29
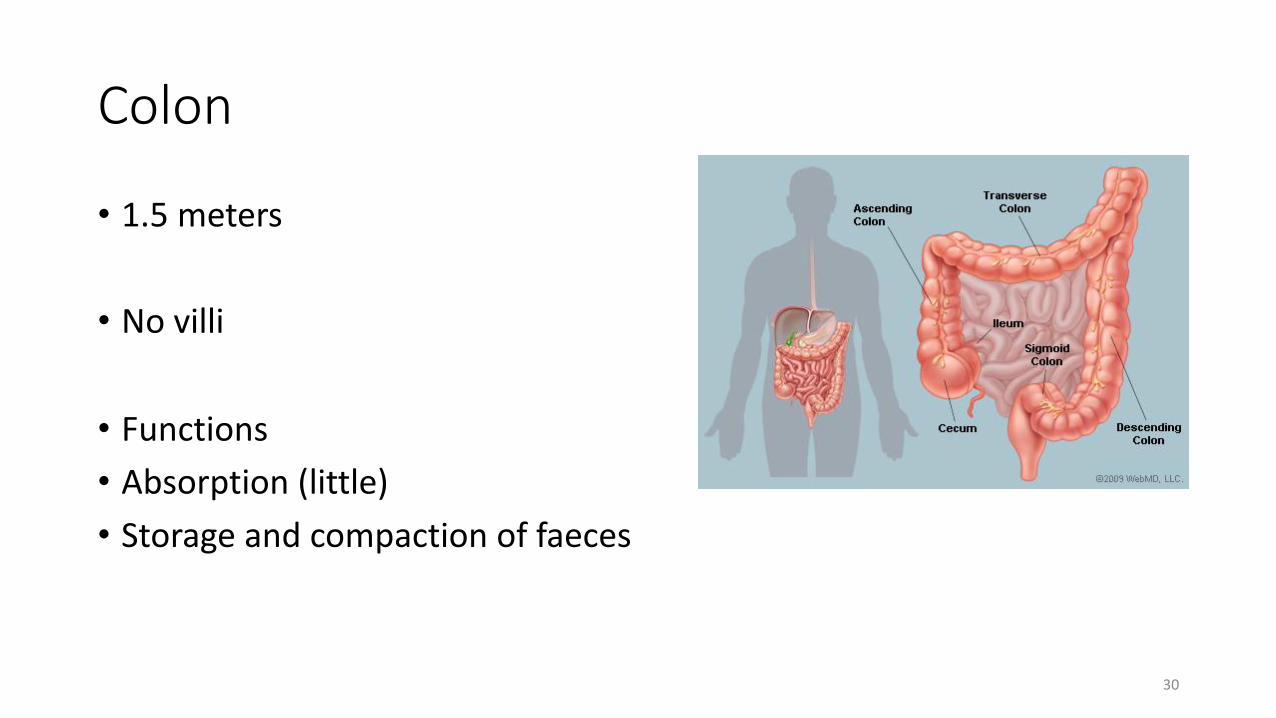
Colon
• 1.5 meters
• No villi
• Functions • Absorption (little)• Storage and compaction of faeces
30
Colon
• Bacteria:• Permanently colonized
• Capable of metabolic reactions
31
Transit of drugs in the GIT
• How long does a drug take to stay in the whole GIT ?
• 0.4-5 days
• Most of the drugs are absorbed from the intestine• time drug takes to the site do absorption is
important as it defines the onset of action
32
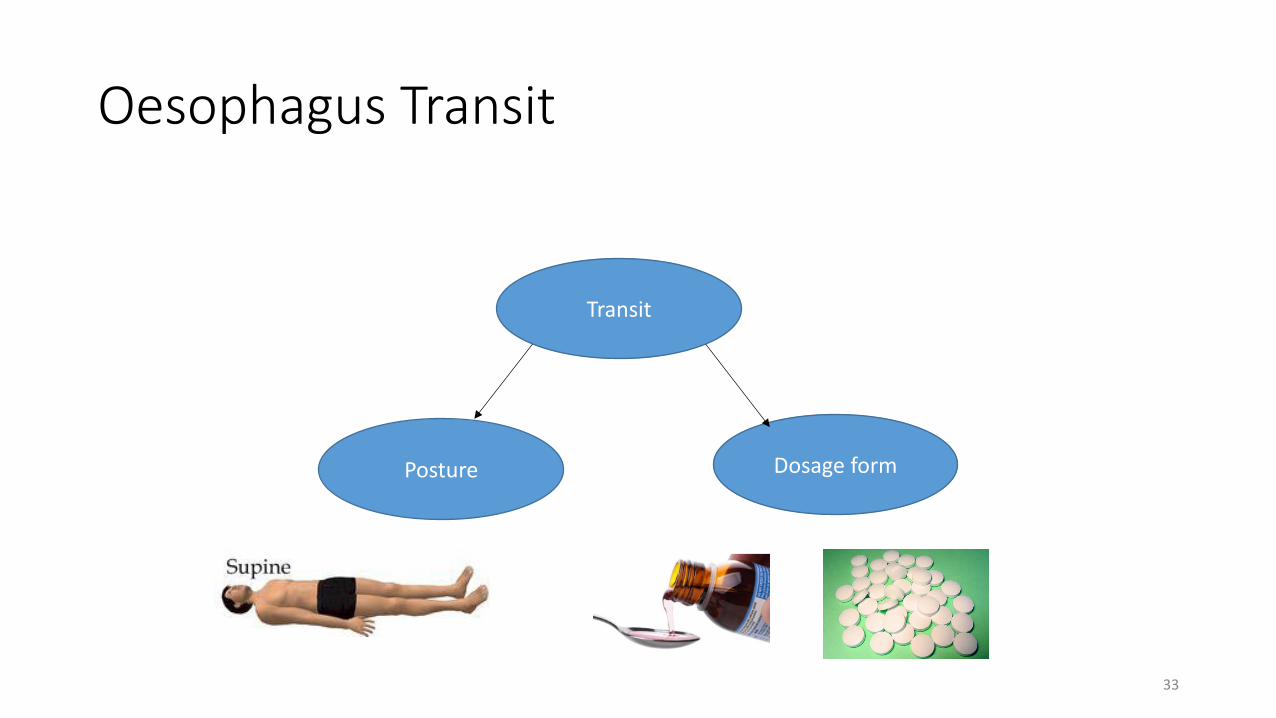
Oesophagus Transit
Transit
Posture Dosage form
33
Oesophagus Transit
• A person in supine position and taking a solid dosage form, it might lodge in the oesophagus and by dehydration adhesion and forming of a gel might occur.
34
Oesophagus Transit
• Consequences: 1. Delay in effect 2. Irritation and ulceration of the oesophagus
e.g. KI tablets and NSAIDs.
35
Stomach transit
Gastric Emptying Rate (GER)
• The time taken by dosage form to transit stomach.
• 5 minutes to 2 hours
36
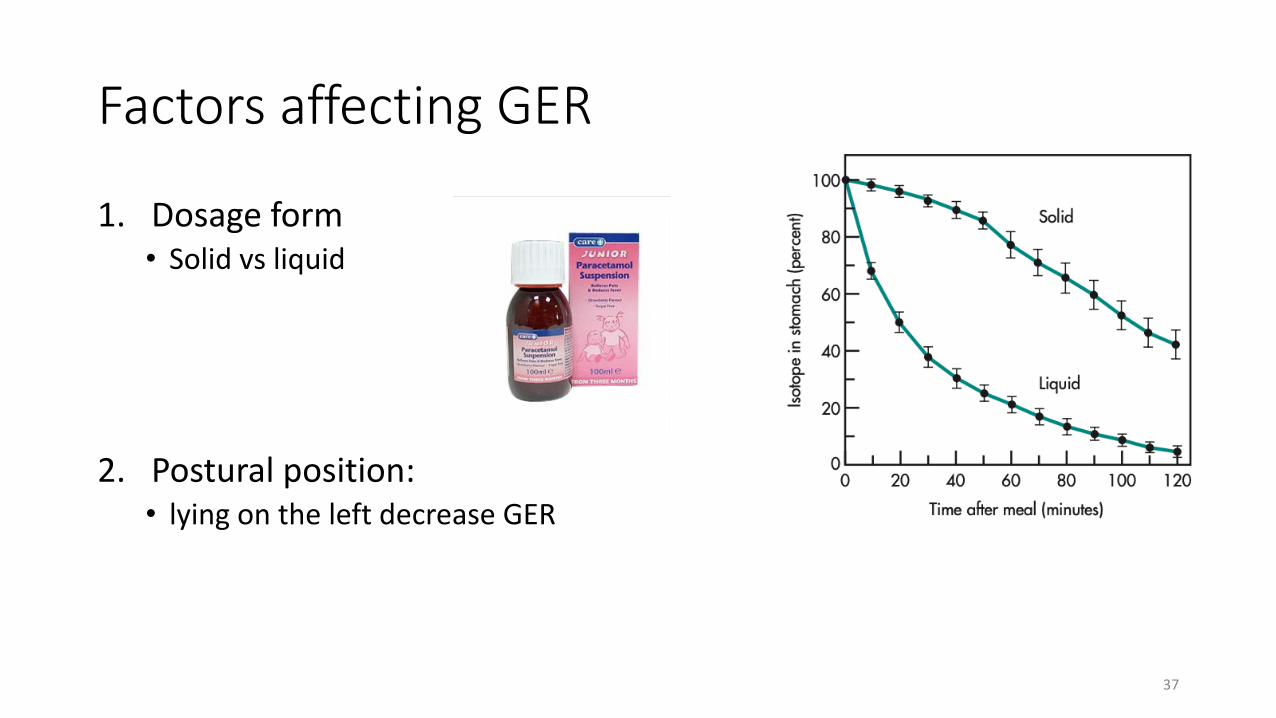
Factors affecting GER
1. Dosage form • Solid vs liquid
2. Postural position:• lying on the left decrease GER
37

Factors affecting GER
3. Fasted/fed state
4. Composition of food:• Fatty food decrease GER
38
Factors affecting GER
5. Effect of drugs• Anticholinergics and ethanol
6. Disease states:• Decrease GER: some diabetics, local pyloric lesion, Hypothyroidism• Increase GER: Hyperthyroidism
39
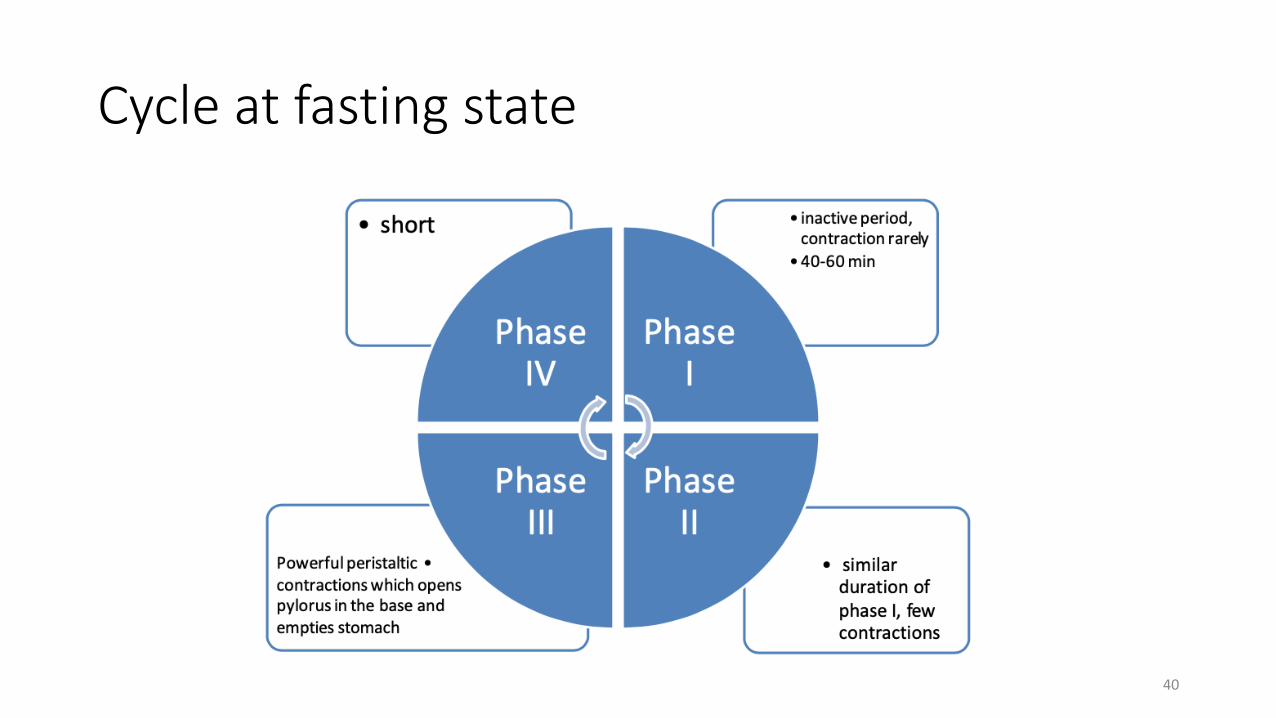
Cycle at fasting state
40
• The discrimination between dosage forms is not found in the fasted state.
41
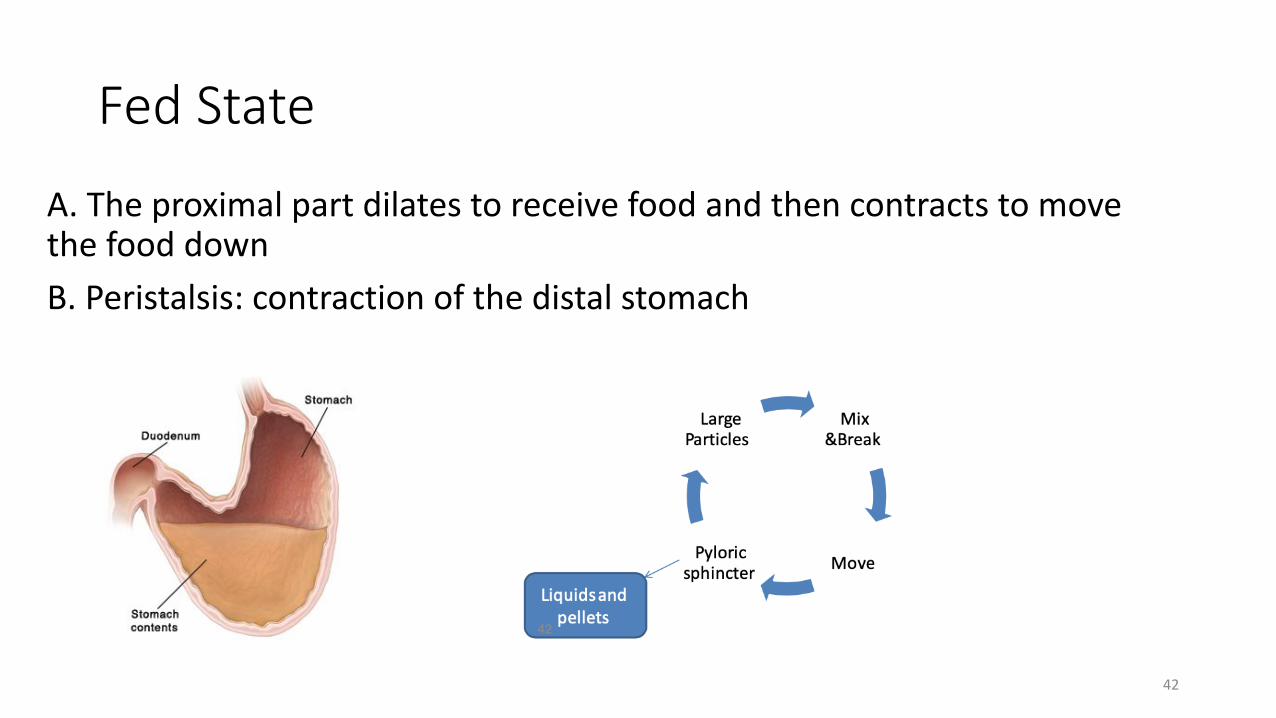
Fed State
A. The proximal part dilates to receive food and then contracts to move the food down B. Peristalsis: contraction of the distal stomach
42
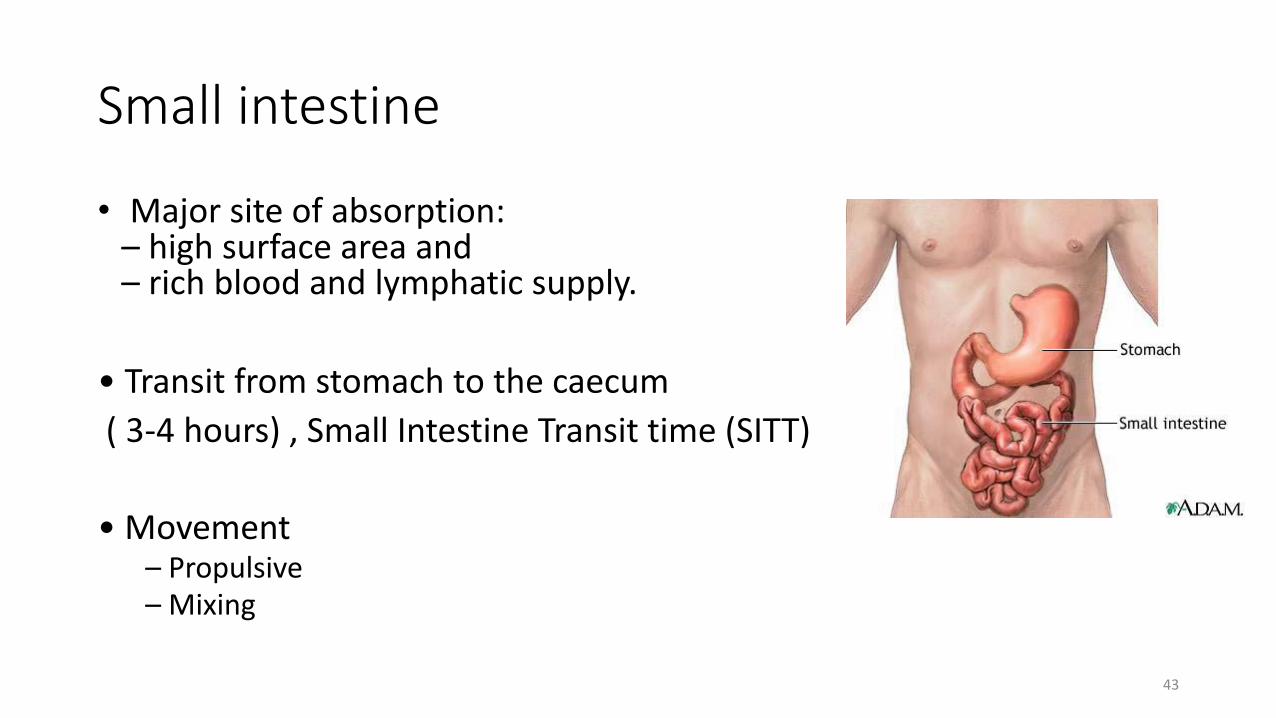
Small intestine
• Major site of absorption:– high surface area and– rich blood and lymphatic supply.
• Transit from stomach to the caecum( 3-4 hours) , Small Intestine Transit time (SITT)
• Movement – Propulsive – Mixing
43
• No discrimination:
1. Dosage forms
2. Fed and fasted state.
44
Intestinal transit time importance
1. Controlled release and sustained release
2. Enteric coated tablet
45
3. Drugs dissolve slowly in the intestinal fluid- Dissolution Rate limited
4. Drugs absorbed by intestinal carrier-mediated transport
46
Colon Transit
• Long and variable (2- 48 hours)
Depending on: • Dosage form• Diet • Disease state
47
Colon Transit
• Example:• Metoprolol • Theophylline
• Good candidates for an oral sustained-release dosage form.
48
Further readings
• Aulton, M. E. and K. M. Taylor (2013). Aulton's pharmaceutics: the design and manufacture of medicines, Elsevier Health Sciences.• Shargel, L., S. Wu-Pong and A. B. Yu (2007). Applied biopharmaceutics
& pharmacokinetics, McGraw-Hill.• Fleisher, D., B. Sweet, A. Parekh and J. Boullata (2010). Drug
Absorption with Food. Handbook of Drug-Nutrient Interactions. J. I. Boullata and V. T. Armenti, Humana Press: 209-241.
49





























