Embed Size (px)
Citation preview

BioPharmThe Science & Business of Biopharmaceuticals
INTERNATIONAL
www.biopharminternational.com
INTERNATIONAL
Bio
Ph
arm
Intern
atio
nal
NO
VEM
BER 2
014
G
en
eric
Dru
gs I C
ellu
lar T
hera
py I S
am
plin
g P
lan
s V
olu
me 2
7 N
um
ber 1
1
November 2014
Volume 27 Number 11
GENE AND
CELL THERAPY
MANUFACTURING
FORMULATION
DESIGN OF EXPERIMENTS
PROVIDES BENEFITS
GLOBAL MARKETS
GERMANY POST AMNOG
SETTING STANDARDS FOR
BIOTECH THERAPEUTICS IN INDIA
TROUBLESHOOTING
VIRAL CLEARANCE
CHALLENGES
ES521015_BP1114_cv1.pgs 10.28.2014 23:16 ADV blackyellowmagentacyan

www.tosohbioscience.com
Tosoh Bioscience is a registered trademark of Tosoh Corporation.
TOSOH BIOSCIENCE LLC • Customer service: 866-527-3587 • Technical service: 800-366-4875, option #3
Hydroxyapatite resin for the purification of biomolecules
Available October 21st from Tosoh Bioscience
CaPure-HA
P
1527744.30
30.9742.1
[Ne]3s23p3
1.82 ±3,4,5
34685221
78.962.5
[Ar]3d104s24p4
4.79 -2,4,6
91
1600
231.0361.1
[Rn]5f26d7f2
4.79 4,5
881536700
2326.025
[Rn]7s2
5.0 2
2232891670
47.8671.6
[Ar]3d24s2
5.0 3,4
8-182.82-222.65
15.9993.5
[He]2s22p4
1.43 -2
7-195.65-209.86
14.0073.1
[He]2s22p3
1.25 2,±3,4,5
16444.75115.36
32.072.4
[Ne]3s23p4
2.07 2,±3,4,5
9241341132
238.0291.2
[Rn]5f36d7s2
19.0 3,4,5,6
7555963180
186.2071.5
[Xe]4f145d56s2
19.0 -1,2,4,6,7
U Re
Se Pa Ra Ti O N S
ES524450_BP1114_CV2_FP.pgs 10.30.2014 22:27 ADV blackyellowmagentacyan

INTERNATIONAL
BioPharmThe Science & Business of Biopharmaceuticals
EDITORIALEditorial Director Rita Peters [email protected]
Managing Editor Susan Haigney [email protected]
Science Editor Randi Hernandez [email protected]
Science Editor Adeline Siew, PhD [email protected]
Community Editor Ashley Roberts [email protected]
Art Director Dan Ward [email protected]
Contributing Editors Jill Wechsler, Jim Miller, Eric Langer, Anurag Rathore, Jerold Martin, Simon Chalk, and Cynthia A. Challener, PhD Correspondents Hellen Berger (Latin & South America, [email protected]), Jane Wan (Asia, [email protected]), Sean Milmo (Europe, [email protected]) ADVERTISING
Publisher Mike Tracey [email protected]
West/Mid-West Sales Manager Steve Hermer [email protected]
East Coast Sales Manager Scott Vail [email protected]
European Sales Manager Chris Lawson [email protected]
Senior Sales Executive Christine Joinson [email protected]
Direct List Rentals Tamara Phillips [email protected] 877-652-5295 ext. 121/ [email protected] Outside US, UK, direct dial: 281-419-5725. Ext. 121 PRODUCTION Production Manager Jesse Singer [email protected] AUDIENCE DEVELOPmENT Audience Development Rochelle Ballou [email protected]
Joe Loggia, Chief Executive Officer; Tom Ehardt, Executive Vice-President, Chief Administrative Officer & Chief Financial Officer; Georgiann DeCenzo, Executive Vice-President; Chris DeMoulin, Executive Vice-President; Rebecca Evangelou, Executive Vice-President, Business Systems; Julie Molleston, Executive Vice-President, Human Resources; Tracy Harris, Sr Vice-President; Dave Esola, Vice-President, General Manager Pharm/Science Group; Michael Bernstein, Vice-President, Legal; Francis Heid, Vice-President, Media Operations; Adele Hartwick,Vice-President, Treasurer & Controller
©2014 Advanstar Communications Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission in writing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specific clients is granted by Advanstar Communications Inc. for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: [email protected].
Advanstar Communications Inc. provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities that may be of interest to you. If you do not want Advanstar Communications Inc. to make your contact information available to third parties for marketing purposes, simply call toll-free 866-529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from Advanstar’s lists. Outside the U.S., please phone 218-740-6477.
BioPharm International does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.
BioPharm International welcomes unsolicited articles, manuscripts, photographs, illustrations, and other materials but cannot be held responsible for their safekeeping or return.
To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
EDITORIAL ADVISORY BOARDBioPharm International’s Editorial Advisory Board comprises distinguished specialists involved in the biologic manufacture of therapeutic drugs, diagnostics, and vaccines. Members serve as a sounding board for the editors and advise them on biotechnology trends, identify potential authors, and review manuscripts submitted for publication.
K. A. Ajit-Simh President, Shiba Associates
Rory Budihandojo Director, Quality and EHS Audit
Boehringer-Ingelheim
Edward G. Calamai Managing Partner
Pharmaceutical Manufacturing
and Compliance Associates, LLC
Suggy S. Chrai President and CEO
The Chrai Associates
Leonard J. Goren Global Leader, Human Identity
Division, GE Healthcare
Uwe Gottschalk Vice-President,
Purification Technologies
Sartorius Stedim Biotech GmbH
Fiona M. Greer Global Director,
BioPharma Services Development
SGS Life Science Services
Rajesh K. Gupta Vaccinnologist and Microbiologist
Jean F. Huxsoll Senior Director, Quality
Product Supply Biotech
Bayer Healthcare Pharmaceuticals
Denny Kraichely Associate Director
Johnson & Johnson
Stephan O. Krause Principal Scientist, Analytical
Biochemistry, MedImmune, Inc.
Steven S. Kuwahara Principal Consultant
GXP BioTechnology LLC
Eric S. Langer President and Managing Partner
BioPlan Associates, Inc.
Howard L. Levine President
BioProcess Technology Consultants
Herb Lutz Principal Consulting Engineer
EMD Millipore Corporation
Jerold Martin Sr. VP, Global Scientific Affairs,
Biopharmaceuticals
Pall Life Sciences
Hans-Peter Meyer VP, Special Projects Biotechnology
Lonza, Ltd.
K. John Morrow President, Newport Biotech
David Radspinner Global Head of Sales—Bioproduction
Thermo Fisher Scientific
Tom Ransohoff Vice-President and Senior Consultant
BioProcess Technology Consultants
Anurag Rathore Biotech CMC Consultant
Faculty Member, Indian Institute of
Technology
Susan J. Schniepp Vice-President
Quality and Regulatory Affairs
Allergy Laboratories, Inc
Tim Schofield Managing Director
Arlenda, USA
Paula Shadle Principal Consultant,
Shadle Consulting
Alexander F. Sito President,
BioValidation
Michiel E. Ultee Chief Scientific Officer
Laureate BioPharmaceutical Services, Inc.
Thomas J. Vanden Boom Vice-President, Global Biologics R&D
Hospira, Inc.
Krish Venkat CSO
AnVen Research
Steven Walfish Principal Statistician
BD
Gary Walsh Professor
Department of Chemical and
Environmental Sciences and Materials
and Surface Science Institute
University of Limerick, Ireland
ES521010_BP1114_003.pgs 10.28.2014 23:16 ADV blackyellowmagentacyan

4 BioPharm International www.biopharminternational.com November 2014
Contents
BioPharmINTERNATIONAL
BioPharm International integrates the science and business of
biopharmaceutical research, development, and manufacturing. We provide practical,
peer-reviewed technical solutions to enable biopharmaceutical professionals
to perform their jobs more effectively.
COLUMNS AND DEPARTMENTS
BioPharm International ISSN 1542-166X (print); ISSN 1939-1862 (digital) is published monthly by Advanstar Communications, Inc., 131 W. First Street, Duluth, MN 55802-2065. Subscription rates: $76 for one year in the United States and Possessions; $103 for one year in Canada and Mexico; all other countries $146 for one year. Single copies (prepaid only): $8 in the United States; $10 all other countries. Back issues, if available: $21 in the United States, $26 all other countries. Add $6.75 per order for shipping and handling. Periodicals postage paid at Duluth, MN 55806, and additional mailing offices. Postmaster Please send address changes to BioPharm International, PO Box 6128, Duluth, MN 55806-6128, USA. PUBLICATIONS MAIL AGREEMENT NO. 40612608, Return Undeliverable Canadian Addresses to: IMEX Global Solutions, P. O. Box 25542, London, ON N6C 6B2, CANADA. Canadian GST number: R-124213133RT001. Printed in U.S.A.
BioPharm International is selectively abstracted or indexed in: • Biological Sciences Database (Cambridge Scientif c Abstracts) • Biotechnology and Bioengineering Database (Cambridge Scientif c Abstracts) • Biotechnology Citation Index (ISI/Thomson Scientif c) • Chemical Abstracts (CAS) • Science Citation Index Expanded (ISI/Thomson Scientif c) • Web of Science (ISI/Thomson Scientif c)
ON THE WEBwww.biopharminternational.com
Social Media
Follow us on Twitter@BioPharmIntl
Join our BioPharmInternational Group
Single-Use Systems eBook Be sure to check out BioPharm InternationalÕs Secure Single-Use Systems eBook for articles on best practices, disposable chromatography
solutions, trends in single-use bioreactors, and more! Download the eBook at BioPharmInternational.com/eBook+Series
BioPharmThe Science & Business of Biopharmaceuticals
INTERNATIONAL
www.biopharminternational.com
INTERNATIONAL
November 2014
Volume 27 Number 11
Gene and
cell therapy
ManufacturinG
forMulation
DEsIgN Of ExpERImENTs
pROvIDEs BENEfITs
Global Markets
gERmANy pOsT AmNOg
sETTINg sTANDARDs fOR
BIOTEch ThERApEuTIcs IN INDIA
troubleshootinG
vIRAL cLEARANcE
chALLENgEs
6 From the Editor The US public catches Ebola hype, but lacks initiative for influenza prevention.Rita Peters
8 Regulatory Beat Manufacturers face regulatory overhaul, while brand-generic debates escalate over biosimilars and labeling changes.Jill Wechsler
12 Perspectives on Outsourcing European CDMOs want to get into the US market, but entry options are limited.Jim Miller
42 Troubleshooting Challenges remain for virus removal and validation. Cynthia A. Challener
45 Analytical Best Practices The ability to define a scientifically justified and statistically sound sampling procedure is a fundamental skill.Thomas A. Little
48 Ad Index
49 Product Spotlight
49 New Technology Showcase
50 The Word
GENE AND CELL THERAPY
Vector Manufacturing and Testing for Gene and Cell Therapy ApplicationsWolf Klump, Martin Wisher, Alison Armstrong, and Audrey ChangThe authors offer insight into cell
therapy manufacturing, vector
production, and the safety aspects
of testing for characterization. 14
Standardizing Practices for Cellular Therapy ManufacturingUplaksh Kumar and Naynesh R. KamaniCellular therapy developers learn
process development strategies
from pharma industry experiences. 24
FORMULATION DEVELOPMENT
DoE Provides Benefits, but Preparation Is NecessaryCynthia A. ChallenerDefining critical parameters and processing
large quantities of data can be a challenge. 28
GLOBAL PERSPECTIVES
Germany Post AMNOG: Insights for BioPharmaJill E. Sackman and Michael J. KuchenreutherThe authors take a look at some of the recent
developments in the German market. 30
Setting Standards for Biotech Therapeutics in IndiaRenu Jain, M. Kalaivani, Gunjan Narula, and G. N. SinghThe authors take a look at the
past and future impact of the
Indian Pharmacopoeia Commission. 35
Volume 27 Number 11 November 2014
FEATURES
Cover: REB Images/Getty Images
SecureSingle-uSe
SyStemS
November 2014
BioPharmINTERNATIONAL
The Science & Business of Biopharmaceuticals
e b o o k s e r i e s
www.biopharminternational.com
ES521018_BP1114_004.pgs 10.28.2014 23:17 ADV blackyellowmagentacyan

www.gelifesciences.com/BioProcess
Xcellerex XDR systems offer the benefi ts of single-use technology in a stirred-tank
bioreactor design. Developed for scalability and robustness, the XDR platform
provides the performance and fl exibility needed from process development to
large-scale biopharmaceutical manufacturing.
When you need a fl exible and scalable cell culture solution, we are a partner
like no other.
GE works.
Predictable process scaling.Xcellerex™ bioreactor platform.
upstream downstream single-use services
GE and GE monogram are trademarks of General Electric Company. Xcellerex is a trademark of General Electric Company or one of its subsidiaries.© 2014 General Electric Company - All rights reserved. First published Oct. 2014.GE Healthcare Bio-Sciences AB. Björkgatan 30, 751 84 Uppsala, Sweden
29-1333-79 AA 10/2014
ES524453_BP1114_005_FP.pgs 10.30.2014 22:27 ADV blackyellowmagentacyan

6 BioPharm International www.biopharminternational.com November 2014
From the Editor
The US public
catches Ebola hype,
but lacks initiative
for influenza
prevention.
Hype vs. Health
Ebola virus disease (EVD), which first appeared in Africa 38 years ago, gen-
erally was perceived by people in developed nations as a scary, deadly, but
distant illness far removed from their lives.
EVD is a severe, often fatal disease that is transmitted human-to-human
through bodily fluids. According to World Health Organization (WHO) data,
nearly 2000 people in Africa were infected with EVD from 1976 through 2013
with an average fatality rate of 50%. The latest outbreak began in March 2014 in
Guinea and spread to Sierra Leone, Liberia, Senegal, and Nigeria. As of Oct. 14,
WHO reported 9216 confirmed, probable, or suspected cases of EVD worldwide
and 4555 deaths.
When the first patient with EVD walked into a US hospital, the facility was
not prepared; two nurses treating the patient were infected. Despite initial mis-
steps, federal and local officials contained the outbreak to that single hospital.
But it was too late to contain overreaction by the public, press, and politicians,
which spread much faster and wider than the disease itself and distracted pub-
lic attention from real health threats.
While the afflicted nurses battled the disease, politicians lined up to
criticize the reaction of the federal government. Demonstrators outside the
White House called for a halt to flights from West Africa. Schools closed. In
one extreme example of undue caution, a school in Maine placed a teacher
on a 21-day leave after she attended a conference in Dallas in mid-October,
even though she had no contact with any people, transportation, or facilities
involved in three EVD cases diagnosed in that area.
The 2014 outbreak clearly illustrates there is a need for effective vaccines
and therapies for EVD; a handful of vaccines and treatments are in early devel-
opment and testing stages. Questions remain, however, about the bio/pharma
industry’s ability or desire to develop and produce therapies or vaccines cost-
effectively.
Viruses here and now
While EVD generated alarm, two other health issues presented serious medical
challenges for US patients.
Between mid-August and mid-October, the Centers for Disease Control
(CDC) and state public health laboratories confirmed that 825 people, mostly
children, in 46 states and the District of Columbia had respiratory illnesses
caused by enterovirus D68 (EV-D68); seven patients died. Enteroviruses and
rhinoviruses cause millions of respiratory illnesses in children each year; how-
ever, the 2014 outbreak of EV-D68 was much greater than that reported in pre-
vious years. There are no vaccines to prevent EV-D68.
Influenza is an annual threat to the health of the general public and
patients with compromised medical conditions in particular. The October
to March flu season is just underway and CDC estimates that 5–20% of
Americans get the flu each year. While most people recover, CDC estimates
that between 3000 and 49,000 Americans die from the flu or its complications
every year.
The flu virus is contagious and, unlike EVD, can be spread through airborne
transmission (a cough or sneeze) and by someone infected with the virus who
is not showing symptoms. Unlike EVD and EV-D68, however, vaccines to
protect against the flu are readily available; CDC says the vaccine reduces the
chance of getting the flu by approximately 60%. Still, less than half of the US
population gets innoculated.
Count me among those lining up for an annual flu shot. The vaccine does not
come with a guarantee that I will avoid the flu, but a shot of prevention is worth
more than a pound of paranoia. ◆
Rita Peters is the editorial director of
BioPharm International.
ES518360_BP1114_006.pgs 10.24.2014 02:32 ADV blackyellowmagentacyan

131.A1.0131.A © 2014 Eppendorf AG.
www.eppendorfna.com • 800-645-3050
Most CompactQbD-driven Process Development with the DASbox® Mini Bioreactor System
> Parallel set-up of 4, 8, 12 or more
bioreactors
> Perfectly suited for microbial
and cell culture applications
> Liquid-free exhaust condensation
> Fully mass flow-controlled gas mixing
> Available with single-use vessels
With working volumes of 60–250 mL
the DASbox is the optimal tool for
advanced cell culture and microbial
process development and Design
of Experiments (DoE) applications.
All critical parameters can be
precisely controlled.
ES524464_BP1114_007_FP.pgs 10.30.2014 22:28 ADV blackyellowmagentacyan

8 BioPharm International www.biopharminternational.com November 2014
Regulatory Beat
Vis
ion
so
fAm
eri
ca
/Jo
e S
oh
m/G
ett
y Im
ag
es
The 30th anniversary of the Hatch-
Waxman Act in September generated
widespread recognition of how the leg-
islation created today’s vibrant generic-drug
industry. Generic drugs now account for more
than 85% of US prescription drug use, and the
development of biosimilars promises to extend
this trend to large molecules. Such transforma-
tion was unanticipated back in 1984 by the
authors of the legislation, Sen. Orrin Hatch
(R-Utah) and Rep. Henry Waxman (D-Calif),
who is retiring from Congress but continues to
urge vigilance to ensure that Americans retain
access to low-cost quality medicines.
A September conference commemorating
Hatch-Waxman sponsored by the Food & Drug
Law Institute (FDLI) described the world with
few generic drugs prior to 1984 and how the
legislation was born of a compromise between
brand-name firms seeking patent extensions
and consumers demanding a clearer pathway for
bringing low-cost drugs to market. Former FDA
officials recalled the challenges in establishing
new policies for testing and evaluating generic
medicines and how the program’s success has
generated thousands of abbreviated
new drug applications (ANDAs) and
supplements that are requiring major
operational changes at FDA. Hatch-
Waxman also has generated a host of
legal, regulatory, and economic issues
that complicate generic drug oversight
and distribution.
User fees alter landscapeThe Hatch-Waxman anniversary
also coincides with the beginning
of year three of the Generic Drug
User Fee Act (GDUFA), the fee scheme
approved by Congress in 2012 to
speed up ANDA approvals. The pro-
gram expands FDA review staff, supports timely
field inspections, and funds research on devel-
oping more complex generic dosage forms. One
result is the elevation of the relatively small
Office of Generic Drugs (OGD) in the Center
for Drug Evaluation and Research (CDER) into a
“super office” to accommodate a larger cadre of
scientists, reviewers, and policy experts to sup-
port new regulatory approaches.
GDUFA requires OGD to meet certain time
frames for assessing and approving ANDAs
and supplements, while also whittling away at
a massive application backlog. Specific goals
for reviewing ANDAs kick in this year, and
manufacturers have concerns about OGD
meeting the schedule. An unanticipated prob-
lem is that more than 1400 applications were
filed this past year, many more than pro-
jected, making it even more necessary for
OGD to implement a new review process that
sets priorities based on product risk, medical
importance, review goal dates, and internal
workload factors.
Chemistry reviewers will provide “appropri-
ate scrutiny” to high-risk areas, while stream-
lining the review of lower-risk products,
explained Susan Rosencrance, then acting
deputy director for generic drug chemistry in
CDER’s Office of Pharmaceutical Science (OPS),
at the FDA/PQRI conference in September 2014.
The risk-based review approach has already paid
New Era for Generic DrugsManufacturers face regulatory overhaul, while brand-generic debates escalate over biosimilars and labeling changes.
Jill Wechsler is BioPharm
International’s Washington editor,
chevy chase, Md, 301.656.4634,
read Jill’s blogs at
pharmtech.com/wechsler.
the emergence of
biosimilars continues
to fuel debate over the
assessment of similarity.
ES518282_BP1114_008.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

10 BioPharm International www.biopharminternational.com November 2014
regulatory Beatregulatory Beat
off with a 50% reduction in chem-
istry review times this past year,
she noted.
A main strategy for speeding up
ANDA review and approval is to
reduce the number of application
review cycles. OGD is implement-
ing a “real-time communication”
program that allows staff to dis-
cuss minor deficiencies that can
be resolved quickly with manufac-
turers. The agency also is adopt-
ing a “block review” approach that
assigns a team to three or more
ANDAs with the same reference
listed drug or same drug mas-
ter file. This system moves away
from OGD’s random assignment
approach, established to avoid any
appearance of favoring one appli-
cation over another. Block reviews
aim to reduce repeated efforts, pro-
mote information sharing, and
produce more consistent decisions.
CDER also is working hard to
cut the massive backlog of some
5000 generic-drug manufactur-
ing supplements. An efficient sup-
plement review process is key to
encouraging product moderniza-
tion and quality improvements for
marketed drugs, and Rosencrance’s
office has almost halved the back-
log through a “strategic plan of
attack” by a special supplement
review team of external and inter-
nal chemistry reviewers.
Not all is rosy with FDA’s GDUFA
implementation process, though,
as seen in concerns raised by man-
ufacturers about still-slow ANDA
approvals at a GDUFA public hear-
ing in September. Small manu-
facturers asked FDA for reduced
annual facility and filing fees,
and several industry executives
urged more clarity in how new
guidance would be implemented.
They offered specific comments
on recent guidance documents
on ANDA content and format and
on the refuse-to-receive policy.
The loudest complaints focused
on OGD’s new communications
policy ending informal phone
conversations between FDA staff-
ers and industry representatives.
Manufacturers say such communi-
cation is key to resolving problems
quickly and helps them plan for
production changes and product
launches. FDA officials maintain
that constant queries are a burden,
lead to inconsistent practices, and
raise the specter of favoritism. But
they now plan to review and revise
the policy in response to industry
concerns.
liaBility and laBelsMeanwhile, the continued growth
in generic drug market share has
generated more legal challenges to
product development and market-
ing. Recent Supreme Court deci-
sions have raised questions about
the adequacy of safety information
in generic-drug labels, prompt-
ing FDA to propose a new rule
on labeling changes that generics
manufacturers strongly oppose as
likely to lead to different labels on
brands and generics. The Generic
Pharmaceutical Association (GPhA)
says FDA’s policy raises liability
issues that could curb development
of new low-cost medicines and
has sought Congressional support
for its position. The legal battle is
escalating as brand manufacturers
seek to avoid added liability for
patients harmed by generic drugs,
and generic-drug companies insist
they can’t have labels different
from the brand. GPhA has pro-
posed that FDA itself establish a
fast, efficient process for updating
labeling changes on both brand
and generic drugs, and to transmit
such updates electronically to pre-
scribers, dispensers, and patients.
Generic-drug makers also are
fighting innovators over allega-
tions that brands use risk evalu-
ation and mitigation strategies
(REMS) to block the development
and testing of new therapies.
GPhA backs legislation to make
it harder for innovator firms to
claim that a restricted distribu-
tion program required by a REMS
prevents it from making available
drug samples needed for bioequiv-
alence testing.
The emergence of biosimilars
continues to fuel debate over the
assessment of similarity between
reference products and follow-ons.
Although there is general agree-
ment that in-depth analysis of
product structure and function
plus pharmacology testing can
combine to document similarity,
there’s much disagreement over
extrapolation of data by a biosimi-
lar sponsor to support approval of
additional uses and over product
“naming” to distinguish innovators
from biosimilars, as brands look to
discourage interchangeability and
substitution of future biosimilars.
Successful biosimilar devel-
opment must consider manu-
fac t ur ing cost s and qua l it y
com m it me nt s , p o i nte d out
Parexel Vice-President Cecil Nick
at the September biosimilars con-
ference sponsored by the Drug
Information Association. In addi-
tion to assessing non-clinical and
clinical data requirements, spon-
sors must weigh the costs and effi-
ciencies of in-house production
versus contract manufacturing in
terms of production yield, media
costs, disposable versus fixed pro-
duction train, needed purification
steps, and fill/finish arrangements.
The generic-drug industry is “at
a crossroads,” commented Mylan
Senior Vice-President Carmen
Shepard at the FDLI conference.
GDUFA promises to provide more
predictable regulatory actions and
to encourage high quality pro-
duction. But manufacturers fear
that an over-emphasis on meeting
review goals could actually delay
final approvals and end up with
first filers losing exclusivity, under-
mining incentives for developing
new generic products. ◆
ES518278_BP1114_010.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

ES524466_BP1114_011_FP.pgs 10.30.2014 22:28 ADV blackyellowmagentacyan

12 BioPharm International www.biopharminternational.com November 2014
Perspectives on Outsourcing
Do
n F
arr
all/G
ett
y Im
ag
es
At the 2014 CPhI trade show, held Oct. 7–9
in Paris, executives from CDMOs and
contract labs whose operations are solely
in Europe expressed their desire to expand
their operations into North America. These
executives, however, were stymied about how
to do it.
Their interest in North America is not sur-
prising: opportunities there are much greater
than in Europe. There is far more venture
capital f inancing in North America than
in Europe and the level of drug develop-
ment activity is significantly greater. Many
European economies are contracting, and
government budgets to pay for drugs are
under stress. Further, with its large number
of former bio/pharma facilities converted to
contract services businesses, Europe experi-
ences price competition in the drug-devel-
opment market that seems more aggressive
than in North America.
Challenges in entering Us marketEuropean companies are challenged on sev-
eral levels to enter North America. For one
th ing , European cont rac tor s
don’t have a good understand-
ing of the North American mar-
ket. While some may have had
an FDA inspection, many haven’t
a nd don’t u nde r s t a nd F DA
requirements and how they differ
from European requirements.
Further, they have minimal
experience in trying to sell their
services in North America; some
may have one sales representa-
tive based in the US, but many
have none. Sales and marketing
in particular can be different in
North America versus Europe. For
instance, tradeshow marketing is important
in Europe and cold calling is uncommon, but
in North America it is the other way around.
Even if they have sales representation in
North America, European CDMOs suffer from
low brand recognition and can have a hard
time getting clients to travel overseas for ser-
vices that are readily available domestically.
Another cha l lenge for European con-
tractors is that there is a higher barrier to
market entry in North America than they
are used to. Most European CDMOs were
founded as buyouts of facilities that global
bio/pharmaceutical companies wanted to
get rid of. Facility closures are difficult in
Europe because of labor laws and because of
fears that mass layoffs could hurt companies
tendering for government drug supply con-
tracts. As a result, pharma companies have
been willing to offload unneeded facilities to
management teams or private equity inves-
tors at a fraction of their replacement value
and with contracts to continue to manufac-
ture legacy products for some period. This
has made it relatively easy to enter the con-
tract services business in Europe, although
the resulting overcapacity has hurt pricing
for contract manufacturing and development.
Opportunit ies to acquire faci l it ies on
such favorable terms are fewer and farther
sales and marketing in
particular can
be different in north
america versus europe.
Outside Looking In European CDMOs want into the US market, but entry options are limited.
Jim Miller is president of Pharmsource
information services, inc., and publisher
of Bio/Pharmaceutical Outsourcing
report, tel. 703.383.4903, twitter@
JimPharmsource, info@pharmsource.
com,www.pharmsource.com.
ES522820_BP1114_012.pgs 10.29.2014 22:40 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 13
Perspectives on Outsourcing
bet ween i n Nor t h A mer ica .
Because North America consists
of just two large markets, ver-
sus the 20 -plus small to mid-
size markets in Europe, there
weren’t so many facilities built
in the first place, so there have
been fewer facilit ies to divest.
As result, European companies
looking to enter North America
may have to “pay reta i l” to
acquire a fac i l it y or serv ices
business. Acquisition valuations
of CDMOs in recent years have
been especially high.
European CDMOs a re a l so
hindered by a lack of capital
necessary to acquire their way
into North America. They are
often poorly capitalized, given
that their initial buy-in to the
indust ry d idn’t require a lot
of investment. Fur ther, their
low profit margins mean they
haven’t been able to accumulate
a significant amount of equity
t h roug h r e t a i ne d e a r n i ngs .
A lso, some European CDMOs
are employee-owned and may
have particular challenges rais-
ing additional capital without
threatening thei r ownership
structure.
OPPOrtUnities existThe barriers to European entry
i nto t he US CDMO ma rke t
are high but not insurmount-
able . E xamples of European
contractors that have success-
fully established themselves in
North America in the past 10
years include CDMOs Vetter and
Almac as well as contract labs
l ike SGS and Eurof ins. Those
companies, however, had favor-
able ownership structures (fam-
ily trusts or publicly-traded) that
gave them access to adequate
capital.
Fu r ther, it i s occasiona l ly
possible to acquire facilities in
North America under favorable
terms. In 2013, European CMO
Unither acquired a dose manu-
facturing facility with contracts
in Rochester, New York, f rom
UCB Pharma; and Fareva was
able to acquire a manufactur-
ing and packaging facility with
contracts in Richmond, Virginia,
from Pfizer in 2011.
It ’s a lso worth not ing that
Nor t h A mer ica n compa n ie s
have challenges similar to the
Europeans’ when consider ing
entry into Europe. A common
problem has been the fa i lure
to realize that Europe is not a
single market—not even the
European Union—but rather a
collection of more than 20 coun-
tr ies with different languages
and cultures, and a wholly dif-
ferent concept of distance. So,
for instance, North American
compa n ies have e s tabl i shed
facilities in Ireland intended to
serve all of Europe, only to learn
that continental companies view
the Ir ish facilit ies as far away
and foreign.
As the bio/pharmaceut ica l
and contract services industries
consol idate, hav ing a global
network of facilities, at least in
North America and Europe, has
become increasingly important
for competitive success. Mid-size
European CDMOs and contract
labs must figure out how to over-
come the barriers to their entry
into North America if they intend
to succeed over the long term. ◆
north american
companies have
challenges similar
to the europeans’
when considering
entry into europe.
Pfizer Ireland Plant Receives ISPE Award
The International Society for Pharmaceutical Engineers (ISPE) recognized
Pfizer Ireland as the overall winner in the 2014 Facility of the Year Awards
(FOYA) category at the society’s annual meeting in Las Vegas, Nevada. FOYA
acknowledges the pharmaceutical manufacturing industry’s accomplishments
in construction and facility design and the pursuit of new technologies.
The focus of Pfizer Ireland’s Network Strategy Implementation (NSI)
Capacity project was the addition of a new vaccine suite and a drug
substance bioprocess suite. The new manufacturing suites included the
latest technologies, including electronic batch records, process analytical
technology, and disposable bag processing. Pfizer Ireland conducted the
project using a lean management strategy, a 5S program in the design
process, and a Six Sigma toolkit. The Pfizer Ireland Grange Castle plant that
won the award is located in Clondalkin, South County Dublin.
“The society was impressed with the NSI Capacity Expansion project and
the company’s ability to effectively manage the challenges of maintaining
supply with the demolition of existing facilities, new construction, and start-
up and integration activities,” said Chair of the FOYA Judging Panel James
Breen in a press release.
—Randi Hernandez
ES518279_BP1114_013.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

14 BioPharm International www.biopharminternational.com November 2014
RE
B Im
ag
es/
Gett
y Im
ag
es
Gene- and cell therapy-based
medicines are experiencing
resurgence due to the introduc-
tion of “next generation” trans-
fer vectors, which have demonstrated
improved safety and efficacy. Patient sam-
ples are often extracted, expanded, and
transduced using gene-therapy vectors,
and the modified cells are re-implanted in
the patient for therapeutic applications.
In this circumstance, the modified cell
is the drug product rather than the gene-
transfer vehicle, and it carries with it dis-
tinct regulatory challenges. An increase
in the number of candidate molecules
is anticipated due to the interest in the
cancer treatments based on recent suc-
cesses seen with chimeric antigen receptor
(CAR)-based cell therapies. Although the
end product of the manufactured viral
vector is considered a drug substance, in
the case of cell therapies, the scrutiny for
testing for adventitious agents is high. As
in many cases, the transduced cell prod-
ucts possess short shelf lives, often before
all release testing can be completed. In
addition, the use of plasmids for genera-
tion of viral vectors adds another layer of
compliance and testing.
Given the complexities associated with
new technologies, especially with “first-in-
class” applications, the technical and scien-
tific input can be the deciding factor in the
success of a testing and/or manufacturing
program. Both the manufacturing pro-
cess and the performance of routine (e.g.,
adventitious agent testing, mycoplasma,
sterility) and custom-designed (e.g., iden-
tity, potency) assays need to meet clinical
and regulatory compliance standards.
The authors offer insight into cell-ther-
apy manufacturing, vector production, and
the regulatory requirements and safety
aspects of testing for characterization.
To illustrate the manufacturing and
testing strategies for a complex cell-ther-
apy production process, the multilevel
production required to generate a CAR T
cell therapy product can serve as a good
example. This production process starts
with generation of cell lines and trans-
fection of these cells with plasmids to
produce a viral vector, which is then used
to transduce patient T cells, before these
Vector Manufacturing and Testing for Gene and Cell Therapy Applications
Wolf Klump, Martin Wisher, Alison Armstrong,
and Audrey Chang
The authors offer insight into
cell therapy manufacturing,
vector production, and the safety
aspects of testing for
characterization.
Wolf Klump, PhD, is senior manager
of Technical Services at SAFC; Martin
Wisher, PhD, is senior director, Quality
Assurance & Regulatory Affairs at
BioReliance; Alison Armstrong,
PhD, is senior director, Development
Services at BioReliance; and Audrey
Chang, PhD, is senior director,
Development Services at BioReliance.
Gene and Cell Therapy
ES518299_BP1114_014.pgs 10.24.2014 02:15 ADV blackyellowmagentacyan

sigma-aldrich.com/safc
Reduce risk with high-quality raw materials
Building QualityReducing Risk
Delivering Value
ES524465_BP1114_015_FP.pgs 10.30.2014 22:28 ADV blackyellowmagentacyan

16 BioPharm International www.biopharminternational.com November 2014
AL
L F
IGU
RE
S A
RE
CO
UR
TE
SY
OF
TH
E A
UT
HO
RS
are reintroduced into the patient.
This is a long and complicated path
that involves, in many cases, three
or more different manufacturers
(for cell banks, plasmids, lentiviral
vectors and patient cell manipula-
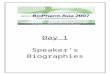
tion). The overall process is shown
in Figure 1.
In ex-vivo applications, gamma ret-
roviral vectors, derived from murine
leukemia virus (MLV), were the first
to be used; however, lentiviral vec-
tors, based on human immunode-
ficiency virus (HIV), have gained
attention due to their ability to
transduce non-dividing cells. While
MLV has a simple genome structure
(containing gag, pol, and env gene
sequences), lentiviruses have a more
complex one containing additional
accessory genes that are able to
manipulate host cell functions. The
general strategy in designing lentivi-
ral vectors for gene therapy is based
on the deletion and alteration of the
native viral sequences to prevent the
generation of replication-competent
retroviruses. To achieve this, the len-
tivirus components are segregated
into three or four different plasmid
constructs with the goal of pre-
venting the possibility of complete
recombination to a fully replication
competent lentivirus (RCL). The
viral vector genome contains at a
minimum the transgene expression
cassette, the long terminal repeats
(LTRs), and the packaging signal. In
most cases, three additional plasmids
provide the factors required for virus
production and packaging (e.g., gag,
pol, env). The envelope proteins are
typically replaced by a heterologous
viral glycoprotein, most commonly
vesicular stomatitis virus G-protein
(VSV-G), to modify the host range
of the vector. An important safety
feature is also the deletion of the
promoter-enhancer region from the
3’ LTR preventing transcription from
this region and subsequent viral rep-
lication (self-inactivating vector; SIN).
The essential steps of ex-vivo
gene therapy involve cell isolation
and in-vitro culture of the desired
cell type to allow the selection,
expansion, and differentiation
either before or after the cell has
been transduced with a viral vec-
tor. In the case of hematopoeitic
cells, most of these steps can be
performed in a closed system using
single-use blood collection and
processing bags.
For CAR T cell therapy, patient
blood cells are harvested, and the
desired T cell populations are selected
and grown to the required levels.
They are then transduced with a viral
vector carrying the CAR gene cassette,
followed by CAR T cell expansion to
the billion-cell level. Lentiviral vec-
tors have been shown to transduce T
cells more efficiently and are, there-
fore, the preferred vector for intro-
ducing CAR into patient target cells.
Expanded cells are then reintroduced
into the patient. To move quickly
into patients, the testing window is
relatively short, and administration
of cells may be initiated before all
testing is completed. This requires a
balance of product risk and timely
treatment of cancer patients.
LenTiViRAL VeCToR pRoDuCTion Lentiviral vector cGMP production
is frequently accomplished using
adherent HEK293 (human embry-
onic kidney cells immortalized
using sheared Adenovirus 5 DNA),
or HEK293T cells (HEK293 cells
containing the SV40 large T antigen
gene) transiently transfected with
plasmids providing the relevant vec-
tor components. The critical raw
materials usually needed for vector
production are the cells, medium
and serum, and the plasmids. Each of
these must be sourced from approved
suppliers and should have gone
through a rigorous testing program
to reduce the risk of introducing
adventitious agents into the produc-
tion process. Master and working cell
banks (MCBs and WCBs) and ani-
mal-derived media components are
also extensively tested.
If fetal bovine serum (FBS) and por-
cine trypsin are used in production,
they should be gamma irradiated to
reduce the risk of viral contamination.
FBS also carries the risk for bovine
spongiform encephalopathy (BSE)
contamination and, therefore, should
be restricted to negligible BSE risk
countries, such as the US, Australia,
and New Zealand. Plasmids being
Gene and Cell Therapy
Figure 1: Schematic of a representative manufacturing and testing strategy for a
cell therapy production process.
Identity
Saftey
Purity
Identity
Saftey
Purity
Identity
In-processtesting
Saftey
Purity
Identity
Saftey
Purity
Identity Saftey
Purity
Plasmids
Viralvector
Patientcell
Transducedpatient cell
Master cellbank (MCB)
Working cellbank (MCB)
ES518298_BP1114_016.pgs 10.24.2014 02:15 ADV blackyellowmagentacyan

With the largest network of harmonized bio/pharmaceutical
GMP product testing labs worldwide, Eurofins BioPharma
Product Testing is everywhere you are.
While delivering a true local lab experience, our
international presence ensures personal quality service
backed by a unique global breadth of harmonized
capabilities to solve all your testing challenges.
For the most complete range of global testing services,
harmonized quality systems and LIMS, you’ll never
need to look further than your own backyard.
Chemistry/Biochemistry
Cell Banking Services
Facility & Process Validation
Method Development & Validation
Microbiology
Molecular & Cell Biology
Raw Materials Testing
Release Testing
Residuals & Impurities Testing
Stability Testing & Storage
Viral Clearance & Viral Safety
Professional Scientific StaffingSM
Services
Belgium
Denmark
France
Germany
Ireland
Italy
Spain
Sweden
U.S.
Facilities
www.eurofins.com/biopharma
BioPharma
Product Testing
Right In Your Backyard.
The Largest Global
Footprint of Harmonized
Testing Labs...
ES524451_BP1114_017_FP.pgs 10.30.2014 22:27 ADV blackyellowmagentacyan

18 BioPharm International www.biopharminternational.com November 2014
produced in bacteria are tested for ste-
rility and endotoxin levels. Similarly,
the vector product requires testing for
adventitious agents, purity, genetic
identity, as well as potency before its
release as a drug substance for trans-
duction of cells ex vivo.
For lentiviral vector current good
manufacturing practices (cGMP)
manufacturing at the SAFC Carlsbad
location, several approaches for scale-
up are being pursued, including use
of cell factories, Corning cellSTACK
or HYPERStack. Depending on the
size of the facility and the available
incubator space, 20 to 40 cellSTACKs
or up to 20 HYPERStacks can be
incubated in parallel and still allow a
consistent and reliable vector produc-
tion. To allow consistent productivity,
the plasmid transfections are done
with polyethylenimine (PEI) as the
transfection reagent, which does not
require as high scrutiny with respect
to pH and buffer consistency as the
calcium phosphate based precipita-
tion method. In many cases, the cells
used for production are still grown
in the presence of serum, which
requires a higher scrutiny in testing,
and efforts to implement serum-free
production should be undertaken in
sight of commercialization. Overall,
efforts should be undertaken to move
toward animal-free components,
which apply to media components as
well as cell propagation.
In comparison with other virus
productions, where cell lysis is
involved, retroviral or lentiviral vec-
tors are harvested from supernatant,
which may, dependent on the pro-
duction system, also allow multiple
harvests and thereby increase the
overall yield. Supernatant volumes
can reach 100 L or more, and require
first a clarification and concentration
step followed by column purification.
The main criterion for purification is
to obtain an acceptable vector con-
centration and assurance that the
vector product has high transduction
efficiency and does not compromise
target cell functionality due to the
presence of contaminants.
ReGuLAToRy ReQuiReMenTS Manufacture of viral vectors, includ-
ing control of critical raw materials,
is governed by regulatory guidelines
issued by agencies such as FDA, the
European Medicines Agency (EMA),
and the Japanese Pharmaceuticals &
Medical Devices Agency (PMDA).
EMA has produced specific guid-
ance on the development and manu-
facture of lentiviral vectors (1). FDA
has provided guidance for the manu-
facture and ex-vivo use of retroviral
gene therapy vectors (2, 3). General
guidance on the manufacture and
quality control of gene therapy viral
vectors is given in the United States
Pharmacopeia (UPS) (4) and European
Pharmacopoeia (Ph. Eur.) (5).
Rigorous testing of viral vector
product, and the critical materi-
als used in its manufacturing, are
required to ensure the viral vector
product is free of adventitious agents,
and is fully characterized for its iden-
tity, purity, and activity. While cell
banks and plasmids can be generated
at qualified manufacturers or in-
house under cGMP, other raw mate-
rials, like media, FBS, Benzonase,
and PEI, must be scrutinized as well.
Yet the viral vector manufacturer
does not directly control production
of these materials. Here, qualifica-
tion of the relevant manufacturers,
good supply chain control, and addi-
tional testing contribute to another
level of complexity. Table I provides
an overview of the testing required
for cell banks, viral vector, and cell-
therapy product.
ASpeCTS oF SAFeTy TeSTinGSafety for clinical use is paramount,
and lentiviral vector preparations
must be formally and extensively
Gene and Cell Therapy
Maintaining an Efficient and Safe Cell-Therapy Supply Chain during Scale-Up and Scale-Out
By Matthew Lakelin, chief scientific officer at TrakCel
Unlike traditional pharmaceutical products that have linear supply chains, autologous therapies have circular supply chains where
the first step is to obtain cellular starting material from the patient. Should an error occur in an autologous therapy supply chain,
resulting in a patient receiving a therapy manufactured from another individual’s cellular starting material, there is a significant
risk of graft versus host disease and other unwanted responses. Supply-chain complexity is exacerbated when considering the
time and temperature-sensitive nature of these products.
The manufacture of allogeneic products does not require harvesting of tissue or cells for processing from the therapy’s
recipient; however, regulations state that it must be possible to trace the therapy to the original donor of the cellular starting
material. Typically, manufacturing of cell therapy products is labor-intensive, and requires continuous communication between
treatment centers and manufacturers to coordinate manufacturing and treatment. Products tend to be separated so that only
one patient’s therapy is contained within a cleanroom to prevent cross contamination. To efficiently scale-up and scale-out cell-
therapy products, clear strategies need to be developed for scheduling management, logistics management, product stability, and
closed systems manufacturing.
To read more on the steps required to develop an efficient manufacturing and supply system for cell therapies, please visit
www.biopharminternational.com/TrakCel.
ES518300_BP1114_018.pgs 10.24.2014 02:15 ADV blackyellowmagentacyan

Grow your cells with insulin from Novo Nordisk
We offer:
• Insulin from the largest manufacturer worldwide
• Pure & Animal Free cGMP product
• Ph.Eur. and USP compliance
• Full traceability
• Several manufacturing sites
• Safety stock at multiple secured locations
• Multi-ton scale production & capacity
• Robust risk mitigation strategy to secure supply safety
Contact us for more information.
www.fefchemicals.com
INSULIN HUMAN AF – THE KEY COMPONENT OF YOUR CELL GROWTH MEDIA
a Novo Nordisk company
ES525585_BP1114_019_FP.pgs 10.31.2014 23:22 ADV blackyellowmagentacyan

20 BioPharm International www.biopharminternational.com November 2014
Gene and Cell Therapy
tested to show they are absolutely
free of RCL. Various methods have
been proposed to detect RCL, which
report high specificity and sensitiv-
ity and can discriminate between
replication-defective virus and
RCL. Current testing recommen-
dations include testing of material
from multiple stages of the produc-
tion process and from transduced
patient cells. Both vector-producing
cells and supernatant from produc-
tion of an MCB should be tested for
RCL using a cell line permissive for
the RCL most likely to be generated.
Regulatory requirements are to test
1% of the total cells or 108 (whichever
is less) pooled vector-producing cells
by co-culture with a permissive cell
line. For supernatant, at least 5% of
the total production harvest must be
tested by amplification on a permis-
sive cell line. Infectivity assays on cell
supernatants or co-cultivation assays
for RCL require several passages of
detector cells and can take up to five
weeks to complete in the laboratory.
At present, most ex-vivo therapies
involve autologous donors where
no screening for adventitious agents
before transduction is done. After
transduction, cells are tested using
assays for sterility, absence of myco-
plasma, RCL, and endotoxin. If the
cell therapy product can be cryo-
preserved prior to administration
Table I: Assays to characterize cell lines and viral vectors. MCB is master cell bank. WCB is working cell bank.
AssaysHuman 293 producer cells Lentiviral
vector(Bulk harvest)
Lentiviral vector
(Purifed)
Ex vivo transduced
cellsMCB WCB
Identity
Isoenzyme analysis X X
DNA fingerprinting X X
Genetic identity by sequencing of transgene X
Genetic identity by restriction enzyme digest X
Absence of microbial contamination
Sterility assay X X X X x
Qualification of sterility assay X X X x
Mycoplasma assay X X X x
Qualification of mycoplasma assay X X x
Absence of adventitious viruses
In vitro assay for adventitious viruses (3 detector cell lines, 28-day assay)
X X X
In vivo assay for adventitious viruses (embryonated eggs, suckling and adult mice, GPs)
X X
Transmission electron microscopy X
PCR/RT-PCR assays for human viruses X
PERT assay X
Bovine virus assay X X X
Porcine virus assay X X X
Porcine circovirus X X X
Absence of replication competent vectors
Replication competent lentivirus X X X
Other tests
Titre of vector (infectivity and transducing efficiency)
X X X
Host cell DNA X
Host cell protein X
Residual bovine serum albumin X
Residual plasmids X
Osmolality X
pH X
Endotoxin X X
ES518296_BP1114_020.pgs 10.24.2014 02:15 ADV blackyellowmagentacyan

Guiding your high potency, solid oral dose drug project successfully
from early development to commercial scale requires world-class
assets and advanced expertise. Pfizer CentreSource applies a
complete end-to-end suite of industry-leading high-containment
services to move your project seamlessly from stage to stage and
get you to market faster.
Our facilities in Germany, Ireland and Italy are equipped with the
world’s most advanced processing assets, technology and
expertise. Included are award-winning engineered containment
platforms as well as segregation-based models, each with the
flexibility to support your specific needs and take promising new
molecules from early development, scale-up, and clinical supply to
commercial production. Our robust high-potency services include
sieving, milling and blending; high shear wet granulation and dry
granulation; core compression, encapsulation and aqueous film
coating; and complex packaging capabilities. We also apply
industry-leading development, analytical, and regulatory expertise
to accelerate your project and amplify your success.
High containment services from Pfizer CentreSource reflect Pfizer’s
uncompromised commitment to quality and compliance with
global standards, coupled with our dedication to 100% customer
satisfaction. So don’t trust your molecule to anything less than the
world’s leading high-containment processing resource. Call or visit
us online to start the conversation.
The Americas: +1.269.833.5844 Europe/Middle East/Africa: +32.2.714.6502 Asia Pacific: +65.6419.0248
[email protected] www.pfizercentresource.com
Unlock Worlds of PotentialWith Our End-to-End High Containment Expertise.
ES525893_BP1114_021_FP.pgs 11.01.2014 02:28 ADV blackyellowmagentacyan

22 BioPharm International www.biopharminternational.com November 2014
back into the patient, classical assays
for sterility and mycoplasma (which
can take up to 28 days to perform)
can be used.
However, in many cases, it is not
possible to freeze cells, and in these
cases, rapid tests must be used. This
could be PCR (polymerase chain
reaction) for mycoplasma, and
rapid-cell-growth-based micro-
biological assays that can take
less than three days, rather than
the 14-day sterility assay. When
transduced cells cannot be frozen,
regulatory authorities have asked
manufacturers to use a rapid assay
for replication competent retrovirus
(RCR) or RCL, such as PCR or PCR-
based reverse transcriptase assays,
which can be completed in days.
The longer assays for sterility and
co-cultivation assays for RCL should
also be run for initial studies—even
if final assay results are only avail-
able after the patient has been
treated with the cell therapy.
TeSTinG STRATeGieSSafety and other testing for charac-
terization purposes can be done at
select testing laboratories. The qual-
ity standard under which testing is
performed varies with geographic
region and stage of clinical devel-
opment. In the US, the testing of
starting materials such as cell banks,
process intermediates, and drug sub-
stance for Phase I/II clinical trials
may be performed to good labora-
tory practice (GLP). In the European
Union, even for materials for early
clinical trials, all manufacturing
and quality control testing must be
performed in licensed premises to
cGMP standards.
Assays to detect adventitious agents
need to be at least generically vali-
dated. All assays used for quality con-
trol of clinical material must be fit for
purpose, and information about the
specificity, sensitivity, and reproduc-
ibility of the assay system should be
available. The extent of this qualifi-
cation/validation data will increase
to support later-stage clinical trials
and product licensure. To navigate
through the regulatory guidance and
to implement a suitable testing strat-
egy, the support of experienced test-
ing laboratories can be valuable.
Testing of master and working
cell banks is focused on safety and
identity. For safety testing, absence
of microbes is tested in sterility and
mycoplasma assays. Testing to show
absence of viruses requires the use
of a number of different assays:
broad specificity assays that detect
a broad range of viruses by exami-
nation for cytopathic effects and
haemadsorption in vitro; mortal-
ity/morbidity on embryonated eggs,
mice and guinea pigs; and trans-
mission electron microscopy.
PCR and reverse transcription PCR
(RT-PCR) assays are used to detect
viruses that are not detectable in
the cells used for the in-vitro assay,
and PCR-based reverse transcriptase
(PERT) assays are used for the detec-
tion of endogenous and adventi-
tious retroviruses. In addition, cells
are tested for identity by isoenzyme
analysis and DNA fingerprinting.
Plasmids used for transfections to
produce viral vectors require test-
ing for sterility and endotoxin to
assure removal of all microbes used
in their production. It is also crucial
to confirm the viral vector specific
sequences to assure generation of
a homogeneous vector population.
Plasmid purity, as well as stability, is
essential to enable consistent trans-
fection efficiencies.
Cell-bank and viral-vector test-
ing have a strong focus on adventi-
tious agent testing, specifically when
using FBS or other animal-based
materials in the manufacturing pro-
cess. In addition, testing for replica-
tion competent viruses is required
for manufactured viral-vector lots to
ensure no infectious lentivirus was
generated via recombination events
during the manufacturing process.
More recently, the emergence
of massive parallel sequencing
(MP-Seq) technology provides the
opportunity of sequencing total cell
genomes quickly. This allows screen-
ing for the presence of unknown
adventitious agents, as well as the
analysis of the homogeneity and sta-
bility of vector populations. Already,
these methods are applied in evalua-
tion of unexpected test results in col-
laboration with regulatory agencies.
As a cGMP requirement, all raw
materials used in production should
be tested for identity. Bovine serum
should be screened for growth pro-
motion ability, absence of adventi-
tious bovine viruses, and levels of
anti-BVDV neutralizing antibodies.
Porcine trypsin should be screened
for absence of stable viruses such as
porcine parvovirus, porcine circovi-
rus, and porcine hepatitis E virus.
ConCLuSionAs the fields of gene and cell therapy
continue to evolve, new vectors and
applications are being explored, and
new adventitious agents are being
discovered. The testing strategies will
require adjustments, and will become
even more complex. However, new
testing technologies like MP-Seq will
add to the repertoire of testing, and
will eventually make the advancing
gene and cell therapy products safer,
and product progression more effec-
tive. In the case of the emergence
of the CAR T cell therapies, devel-
opment of novel treatments will
provide more options and drive the
development of gene and cell therapy
forward to cure patients.
ReFeRenCeS 1. EMA, CHMP/BWP/2458/03 (May 2005).
2. FDA, Guidance for Industry: Guidance
for Human Somatic Cell Therapy
and Gene Therapy (March 1998).
3. FDA, Supplemental Guidance on Testing
for Replication Competent Retrovirus
in Retroviral Vector Based Gene
Therapy Products and During Follow-
up of Patients in Clinical Trials Using
Retroviral Vectors (November 2006).
4. USP <1047> “Gene Therapy
Products” USP 37.
5. European Pharmacopoeia, 5.14
“Gene Transfer Medicinal Products
for Human Use” Jan. 2010. ◆
Gene and Cell Therapy
ES518297_BP1114_022.pgs 10.24.2014 02:15 ADV blackyellowmagentacyan

Presented by:
Sponsored by:
THE BENEFITS OF HIGH PERFORMING
CHROMATOGRAPHY RESINS INCLUDING
POROS® XQ, A NEW STRONG ANION EXCHANGER
LIVE WEBCAST: WEDNESDAY, OCT. 29; 9:00 AM & 2:00 PM (EDT) - 2 EVENTS
REGISTER FOR FREE AT WWW.BIopHArMINTErNATIoNAl.CoM/porosXQ
EVENT OVERVIEW:
poros® resins offer unique performance attributes and drive benefits to downstream processing. poros® XQ resin is the newest addition to our product portfolio. This high capacity, salt tolerant, high resolution anion exchanger enables unique selectivity, higher product yields through better separation, and reduced cost of goods. Applications data will be used to demonstrate the benefits of poros® resins to capture and polish chromatography, and process modeling will be used to demonstrate cost of goods improvements and process efficiencies that can be realized.
KEY LEARNING OBJECTIVES:
• learn how new approaches to the downstream purification process, with increased process flexibility and efficiency, help deliver improved purity and throughput
• Understand the benefits of a new strong anion exchanger with regard to resolution and capacity over a range of process conditions
• Use process modeling to show improved cost of goods and productivity
WHO SHOULD ATTEND:
large-scale bioproduction customers in the Biopharmaceuticals industry, biotech companies (early-phase clinical trials), and CMo’s (contract manufacturing organizations). or, any customer interested in the manufacturing/production of biomolecules such as monoclonal antibodies, therapeutic proteins, and vaccines.
PRESENTER:
Shelly Parra
M.S., Sr. Field
Application Scientist
Thermo Fisher Scientific
MODERATOR:
Sara Barschdorf
Multimedia Editor
Biopharm International
For questions contact
Sara Barschdorf at [email protected]
ES524463_BP1114_023_FP.pgs 10.30.2014 22:27 ADV blackyellowmagentacyan

24 BioPharm International www.biopharminternational.com November 2014
Cellular therapies are posi-
tioned to be the next revolu-
tion in the healthcare industry.
Disciplines such as bio-print-
ing and tissue engineering also require
high quality living cells and can be
considered a part of the overall cellular
therapy industry. Multiple diseases that
were traditionally incurable are being
addressed by cellular therapies with
promising early clinical results. Both
large and small companies are devel-
oping cellular therapies, and currently,
more than a thousand clinical trials are
being conducted (1).
Stem cells are unique in their ability
to divide and regenerate themselves and
in their ability to remain unspecialized
or differentiate into specialized cells
that can perform critical tasks in the
human body. Because of these unique
traits, these cells hold a great deal of
promise in helping researchers learn
about disease and develop treatments.
The regenerative properties of stem cells
are proving useful in developing treat-
ments for common conditions such as
diabetes, heart disease, Parkinson’s dis-
ease, spinal cord injuries, and strokes.
There are two primary categories of
cellular therapies: autologous and allo-
geneic. Autologous therapies are patient-
or donor-specific; allogeneic therapies
generally do not have a specific donor or
source requirement. Each therapy pres-
ents opportunities for treatments, but
also faces unique challenges to overcome
before it can get to the clinic. Autologous
therapies typically are not scalable; allo-
geneic therapies are scalable from a man-
ufacturing perspective. The number of
product doses that can be manufactured
or required for a single patient for an
autologous therapy are limited compared
to a scenario where multiple patients can
be treated using the same off-the-shelf
allogeneic therapy.
MANUFACTURING UNIT OPERATIONSAlthough recent scientific and techno-
logical advances in the cellular therapy
arena portend great therapeutic promise,
the final objective is to accelerate the
development path of these therapies to
the clinic and make them universally
available to all patients. Several steps
along the pathway are fraught with
challenges that institutions and bio-
pharma will face in the attempt to com-
mercialize these products.
One approach is to segment the
various steps of the development pro-
cess into discrete unit operations. This
approach has been successfully imple-
mented in the manufacture of chemi-
cals, automobiles, and food, as well as
other pharmaceutical industry sectors.
The lessons learned can be applied to the
development of cellular therapies. It is
here that cell biology meets engineering
with the application of sound manufac-
turing principles. These unit operations
range from science and discovery to
the successful execution of clinical tri-
als and commercialization of product.
This article focuses on the manufactur-
ing operations that include supply chain
management of raw materials, manufac-
turing processes with facility capabilities,
quality control, quality assurance release,
regulatory requirements, and shipping
and distribution.
Each unit operation needs to be scal-
able to effectively meet clinical demand.
The volume and complexity to make
product for an early-phase clinical trial
is different when compared to what is
required at commercial scale-up. There
is a need for process development
within each unit operation and while
Standardizing Practices for Cellular Therapy Manufacturing
Uplaksh Kumar and Naynesh R. Kamani
Cellular therapy
developers learn process development
strategies from pharma
industry experiences.
Uplaksh Kumar, PhD, MBA, is a cGMP
expert on the AABB Consulting Services
team. Naynesh R. Kamani, MD, is
the division director for the Center for
Cellular Therapies and Research at
AABB Center for Cellular Therapies.
Gene and Cell Therapy
ES518280_BP1114_024.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 25
the process starts out being flex-
ible, it needs to be locked in by
Phase III and before commercial
launch. An important component
of this overall strategy is to iden-
tify each of these requirements
early in the process.
Cost drivers increase as the
product moves through the dif-
ferent phases of clinical develop-
ment with the majority of the
costs closer to commercialization.
While safety and efficacy are pri-
mary drivers, the cost of the final
therapeutic product is also impor-
tant for therapies to be univer-
sally accessible; there should be no
limitations in getting these thera-
pies reimbursed and delivered to
patients (2).
Regulatory affairs
Regulatory requirements for dif-
ferent cell therapies are at differ-
ent stages of development, and
national and international regula-
tory agencies are discussing guid-
ance documents for the industry
to follow. The regulators are will-
ing to provide significant support
to drug developers and will work
with organizations to determine
the correct path forward, resulting
in a clear regulatory path to the
clinic. Japan’s regulatory agency,
for example, has recently retooled
its drug authorization framework
through legal reform to produce
the world’s fastest approval process
specifically designed for regenera-
tive medicine therapies (3).
Supply chain management
Supply chain management of key
materials is the first unit operation
within manufacturing. Cellular
therapies depend on the acquisi-
tion of the right source material
that, in most cases, is derived from
tissue or blood. A good donor
program needs to be established
to ensure that reproducible pro-
cedures are in place using stan-
dard methods to procure material.
While there are several options that
work well, there is limited stan-
dardization in approaches. Using a
standardized accreditation process
for blood and tissue sourcing, enti-
ties will help establish that the pro-
cess being followed is uniform and
consistent. Donor-to-donor vari-
ability will exist, so eliminating the
collection process as a variable will
improve reliability.
Another issue is a short supply
of serum, a critical raw material
in the supply chain. Projections
indicate that there is insufficient
serum to meet the commercial
demands for cell therapy (4). Using
synthetic biology approaches
with computational modeling can
identify substitutes to serum that
are more abundantly available. A
synthetic biology approach also
offers better characterization and
chemical definition, which will
help deliver a consistent prod-
uct and streamline the regulatory
pathway. Many media developers
have launched serum-free media,
which are also under evaluation to
address this bottleneck. Using raw
materials and consumables that
are well characterized and from
qualified suppliers is important.
Suppliers should have quality sys-
tems in place and open to an audit.
Facility design
The manufacturing facility needs
to be built and equipped with the
appropriate infrastructure and
environmental controls. Options
include building a facility, contract
manufacturing, and using modular
pods that are prefabricated and can
be implemented quickly to meet
requirements. Autologous cell-
therapy production may be biased
towards having a modular facility
for each product dose to minimize
cross contamination. Allogeneic
facilities can be designed in a ball-
room arrangement, as each pro-
duction lot represents multiple
doses made at larger scales.
Because terminal sterilization
for cellular therapies is limited, it
becomes important to minimize
open system processing where a
contaminant can be introduced
into the system and lead to failed
product batches. Open-system pro-
cessing requires a higher degree of
personnel training, aseptic process
validation, stringent environmen-
tal controls, and increased costs.
Using methods to ensure maxi-
mum closed-system manufacturing
with automation will reduce some
of the requirements on the facility.
Scale-up and manufacturing
Most manufacturing processes
start off being manual as they are
developed in a laboratory-based
environment with only small
quantities required for preclinical
testing. These processes are sel-
dom scale-up friendly and require
significant process development
efforts to get them ready for large-
scale production. Organizations
face this dilemma when they
review the process development
costs versus moving the process
as-is into clinical manufacturing.
Gene and Cell Therapy
Several steps along
the pathway are
fraught with
challenges that
institutions and
biopharma will face in
the attempt to
commercialize cellular
therapy products.
ES518281_BP1114_025.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

26 BioPharm International www.biopharminternational.com November 2014
Technology transfer of the labora-
tory based process may work in the
short term, but creates issues when
the only option available is scale-
out to achieve required product
volumes.
Research and development scien-
tists require insight into what scale-
up options exist with protocols
and application notes. These proto-
cols will provide early opportuni-
ties to identify processes that can
be easily translated into large-scale
formats with some process devel-
opment. Process development and
technology transfer will always be
required but using standard meth-
ods will streamline the process.
When developers are working with
T-flasks, they seldom think about
transitioning into multi layers ves-
sels and bioreactors. Producing 10
million cells can be achieved in a
laboratory environment but when
cells have to be produced at the bil-
lion to trillion scale, technology
requirements are different. Some
of this development can be done
via computational modeling or
small-scale experiments using well-
characterized methods that have
been qualified for their scalability
potential. Large-scale experiments
are expensive to run and while large,
well-funded organizations have the
resources, smaller organizations
will find it cost prohibitive. Cost-of-
goods modeling is required as the
drug products approach commercial
launch. By understanding the driv-
ers of cost early in the development
phase, the process can be optimized
while there still is some flexibility.
Once the process is locked down,
much work and expense is required
to establish equivalence with the
previous process.
Automation options should also
be evaluated to determine which
steps of the process can be auto-
mated. Several automation options
can be plugged in without exten-
sive customization and process
development. For example, auto-
mated and semi-automated filling
systems for the final dose of the
product are not only a faster and
scalable than manual processes,
they also minimize the oppor-
tunity for contamination. Other
options from the pharmaceuti-
cal industry and other ancillary
industries can be leveraged. Several
academic and industrial consortia
are being created to generate stan-
dardized platforms and methods to
be used across a wide spectrum of
requirements.
Quality control/assurance
Intermediates used in the manu-
facturing process and the final
product must go through quality-
control testing prior to release.
Multiple assays and methods are
available to address sterility, safety,
and efficacy. Many assays may
seem relevant but have no conse-
quence on the drug product. The
development of the acceptance
criteria should be relevant. Doing
more assays does not necessarily
impact outcome but doing the cor-
rect assays with the relevant accep-
tance criteria is important.
Shipping and distribution
The drug product must reach clini-
cal sites without compromising its
sterility, safety, and potency; there-
fore, bio-preservation and cold
chain management need to be
addressed. Standard off-the-shelf
bio-preservation options have been
successfully used with support-
ing regulatory documentation (5).
Evaluating existing options from
the industry is recommended before
designing custom options and will
help in the regulatory submission.
Most cel lular therapies are
shipped and distributed under liq-
uid nitrogen at -80°C or -20°C con-
ditions. Many vendors and service
providers meet national and inter-
national requirements. In addition,
new technologies stabilize these
cells at higher temperatures with-
out compromising viability, shelf
life, and efficacy. Final shipping
and distribution costs can consti-
tute more than 25% of the product
cost, a factor that should not be
underestimated during the budget-
ing process.
ThE PATh FORWARDChallenges will always exist when
launching new therapies and tech-
nologies. Established expertise
from other fields can be leveraged
and applied to cellular therapies.
Options and tools are available to
address each of these challenges.
Execution of a commercialization
strategy can be done in multiple
stages over time and, most impor-
tantly, when required. In some
cases, the investment needs to be
made early enough to be ready for
the next stage.
Accelerating a cellular therapy to
clinic can be executed by identify-
ing the relevant unit operations;
identifying the major components
within the unit operation and
those that need the most atten-
tion; leveraging existing expertise
or standards; implementing the
right solution; and validating the
implementation.
It is only a matter of time before
treatments become available for
diseases that were considered
difficult to cure. The industry is
focused on the promise of deliv-
ering effective cellular therapies
worldwide.
REFERENCES1. Alliance for Rengerative Medicine,
Regenerative Medicine State of the
Industry briefing (January 2014), http://
alliancerm.org/sites/default/files/ARM_
SOTI_PPT_2014.pdf, accessed Oct. 15,
2014.
2. R. Shaw, B. Hampson, C. Betz,
Bioprocessing Journal, 13 (2), 26-31
(2014).
3. D. Cyranoski, Nature Medicine. 11 (9),
510-513 (2013).
4. S. Jung, K.M. Panchalingam, R.D. Wuerth,
L. Rosenberg, L.A. Behie, Biotechnol Appl
Biochem. 59 (2), 106-120 (2012).
5. AJ Mathew, Cryobiology. 67 (3), 412
(2013). ◆
Gene and Cell Therapy
ES518277_BP1114_026.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

PREPARING FOR THE NEW
ELEMENTAL IMPURITIES GUIDELINES(Original air date Tuesday, October 14, 2014) ON-DEMAND WEBCAST
For questions, contact Sara Barschdorf at [email protected]
EVENT OVERVIEW:
The bio/pharmaceutical industry has long anticipated revised
guidelines for elemental impurities limits and testing. While
many questions about the fnal guidelines, as defned in the
International Conference on Harmonisation (ICH) in Q3D
Guideline for Elemental Impurities and the United States
Pharmacopeia (USP) in General Chapters <232> and <233>
still remain, organizations should begin to initiate plans to
transition to these new guidelines now.
In this webcast, experts from pharmaceutical and excipi-
ent manufacturers and analytical testing services will discuss
key areas of concern including risk assessment, proposed
test methods, and sample preparation techniques. Audience
members will have the opportunity to ask questions about the
pending implementation.
Key Learning Objectives
n Review expected requirements for ICH Q3D and USP <232>
and <233>
n Understand key areas is a risk assessment and factors that
afect risk
n Learn appropriate methods and procedures for sample
preparation.
Who Should Attend
Presenters
John Glennon
Stability Lab Team Leader
Supply Chain Stability Testing Hub
ZEB Quality
NA, Japan & Global Pharma Supply
GSK
Nikki Schopp
Team Leader
Analytical Laboratory Services
SGS Life Science Services
Moderator
Rita Peters
Editorial Director
BioPharm International
Presented by
Sponsored by
Register for free at www.biopharminternational.com/elemental
n QA/QC personnel
n Laboratory managers
n Formulation scientists
n Production and process
development managers
ES524479_BP1114_027_FP.pgs 10.30.2014 22:28 ADV blackyellowmagentacyan

28 BioPharm International www.biopharminternational.com November 2014
Co
lin A
nd
ers
on/G
ett
y Im
ag
es
Using a design-of-experiment
(DoE) approach a l lows a
formulat ion development
scientist to examine the for-
mulation design space in a statistically
significant manner from the beginning
of experimentation. In addition, a DoE-
driven approach meets the International
Conference on Harmonization Q8
guidelines for multivariate design space
and the subsequent justification of for-
mulation components when develop-
ing a drug product, according to Steven
R. LaBrenz, scientific director, pharma-
ceutical development and manufactur-
ing sciences with Janssen Research &
Development. At the same time, DoE
results depend on the selected criti-
cal parameters and the sample mate-
rial used in the studies. In addition, a
large amount of data is generated.
Consequently, reaping the benefits
requires a significant commitment to
DoE, including the training of research-
ers in study design and data-processing
techniques.
The benefiTs of DoeOne of the major advantages of the
DoE approach is the ability to study
the effects of multiple excipients and
their interactions in a formulation
at the same time, unlike in the tradi-
tional one-factor-at-time approach,
which is inherently flawed and biased,
according to Mark Yang, director of
fill/finish development for Genzyme.
Phuong Nguyen, a senior scientist with
Millennium Pharmaceuticals (The
Takeda Oncology Company) agrees with
Doe Provides benefits, but Preparation is necessary
Cynthia A. Challener
Defining critical parameters
and processing large quantities of data can be
a challenge.
Cynthia A. Challener is a contributing
editor to BioPharm International.
formulation Development
ES520993_BP1114_028.pgs 10.28.2014 23:15 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 29
this approach. “The quantitative
models for these multiple qual-
ity attributes can then be used for
global optimization of the formu-
lation, leading to more robust for-
mulation development,” she says.
Nguyen also notes that depend-
ing on the data that are generated
from an experimental design, it is
sometimes possible to gain some
mechanistic understanding of pro-
tein stabilization or behavior.
In addition, because multiple
variables can be explored at once,
fewer formulation studies are
required and, therefore, formula-
tion development is more efficient.
An added benefit of this efficiency,
Yang notes, is the reduced quantity
of material needed for formulation
development, which can be impor-
tant early in the development of a
biopharmaceutical product given
the limited availability of the bio-
logic API. Further, a DoE approach
can be particularly useful for com-
bination products that have device
attributes that must be considered
during formulation development,
says Nguyen.
The challenges of DoeWhile there clearly are numer-
ous advantages to using a DoE
approach in the formulation devel-
opment of biopharmaceuticals, it
is important to bear in mind that
there are also limitations to con-
sider with this method.
Two main challenges, asserts
LaBrenz, include the fact that sam-
pling of an adequate design space
is often difficult and there is an
overwhelming amount of data that
is generated with factorial design.
Yang agrees that the typical subset
of critical quality attributes of the
formulated product that are assayed
in a DoE study may not be com-
prehensive enough to cover some
of the quality changes that can
occur. Nguyen also warns that the
models used for DoE formulation
studies may include statistically
significant parameters that may
not be of any importance, such as
when the resulting change from an
input parameter range is within the
error of the method or is not large
enough to have a real effect.
In addition, Yang notes that the
API material used in DoE studies
comes from one or possibly a few
selected primary production lots
that are not necessarily completely
representative of later production
lots. “As a result, the conclusions
drawn based on DoE formula-
tion studies can be biased to some
degree,” he says.
LaBrenz believes that the chal-
lenges of a limited design space
and the management of large
quantities of data can be amelio-
rated with the adoption of high-
throughput sc reening (HTS)
techniques that provide both full
design space coverage and the abil-
ity to collect data in spreadsheets
and, eventually, databases.
Even with the use of HTS, how-
ever, implementation of DoE for
formulation development can be
time consuming and resource
intensive and can translate into
more extensive exper imenta-
tion than planned, according to
Nguyen. “It is a challenge to bal-
ance the number of experiments
required for a statistically robust
DoE study with the available sup-
plies, personnel, resources, and
time,” she says. In addition, user
training is a must, according to
Yang. “DoE study design and data
processing requires an understand-
ing of statistics theory and mod-
els, which can be challenging for
many new users,” he comments.
obTaining relevanT DaTaIn most DoE formulations studies,
data related to the critical quality
attributes and the stability of the
API, such as the protein melting
temperature, secondary or tertiary
structure, or other biochemical/
biophysical characteristics, are
generated. The ultimate goal for
formulation development is to
maintain the API in a stable state
with respect to both structure and
function during processing and
storage, according to Yang. Nguyen
points out that all of the previously
mentioned parameters may serve
as indicators for a stable state.
It is also important to reduce
the data to single-value results
as often as possible, such as the
percent monomer or aggregate as
determined using size exclusion
chromatography-high performance
liquid chromatography (SEC-HPLC),
or the percent purity. For spectral
data from characterization assays,
Janssen calculates the Center
of Spectral Mass Wavelength (or
Mean Center Mass), which allows
the creation of a relative stability
profile for a given spectrum-based
assay. “This single-point, continu-
ous, data-point strategy is readily
testable using most statistical meth-
ods,” LaBrenz explains. In addition,
Nguyen notes that the generated
stability data can be reduced down
to a reaction rate constant or an
output parameter used to develop
statistical models. “Overall,” she
summarizes, “data on quality attri-
butes are generated that will pro-
vide an understanding of how the
excipient or formulation within the
design space affect these attributes.”
Because DoE studies lead to the
production of large quantities of
data, it is important to ensure
that all of the data that are col-
lected are actually relevant. “A
thorough understanding of the
API and desired formulation char-
acteristics is necessary before ini-
tiating a DoE study,” says Yang.
“With such knowledge, a scientist
can make sound scientific judg-
ments and consider the potential
impact of new factors or excipi-
ents when designing a DoE study.”
formulation Development
Contin. on page 40
ES520998_BP1114_029.pgs 10.28.2014 23:15 ADV blackyellowmagentacyan

30 BioPharm International www.biopharminternational.com November 2014
We
st
en
d61P
re
miu
m/G
et
ty
im
aG
es
Manufacturers exploring
opportunities in global
markets face dynamic
demographic and disease
trends, changing market demands, and
evolving regulatory requirements—all
of which differ from one country to
another. While emerging markets con-
tinue to represent a new channel of
demand for pharmaceutical products,
manufacturers have quickly realized
that significant attention must still
be given to more established markets,
such as Germany. It’s no longer suf-
ficient to expect that regulatory data
from prospective randomized clinical
studies alone will be enough to con-
vince payers to provide a price pre-
mium for new products. In this article,
the authors take a look at some of the
recent developments in the German
pharmaceutical market, identify pric-
ing and reimbursement challenges, and
discuss strategies manufacturers should
consider for sustainable success.
Overview Of German market and amnOG Germany is the third largest phar-
maceutical market worldwide and
accounts for approximately 23% of
the European pharmaceutical market
(1). Of equal importance to manufac-
turers, drug prices in Germany are
often used as reference prices in 19
other countries. Taken together, gain-
ing access to this market at an accept-
able price has major implications
for long-term success. In a cost-con-
strained economy, the German gov-
Germany Post amnOG: insights for BioPharma
Jill E. Sackman andMichael J. Kuchenreuther
The authors take a look at some of the recent
developments in the German pharmaceutical
market.
Jill E. Sackman, DVM, PhD, is a
senior consultant, and Michael
Kuchenreuther, PhD, is a
research analyst, both at numerof
& associates, inc., St. Louis, mO,
www.nai-consulting.com.
european market report
ES521207_BP1114_030.pgs 10.28.2014 23:53 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 31
ernment has taken steps to
reduce healthcare spending, and
unfortunately for manufactur-
ers, one way they have sought to
do this is through The Act on the
Reform of the Market for Medical
P roducts (A rzneimit te lmarkt-
Neuordnungsgesetz—AMNOG).
This piece of leg islat ion was
enacted in 2011 and mandates a
more rigorous benefit evaluation
procedure for new pharmaceuti-
cals (and their subsequent label
expansions), thereby adding sig-
nificant challenges to the market
access process.
In AMNOG’s new system, manu-
facturers continue to set the ini-
tial price for new prescription
drugs after regulatory approval.
This price is valid for one year.
During this time, the manufac-
turer’s value dossier is reviewed
european market report
Table I. Decision criteria for G-BA’s/IQWiG’s beneft assessment.
Input CategorizationFactors shown to impact categorization decision
Qualitative
certainty of results
Proof, indication,
hint or no proof
Number of appropriate clinical studies available; use
of valid measurement instruments; risk of bias (e.g.,
non-blinding); endpoint type (e.g., hard, surrogate)
Quantitative extent
of added benefit
Major, considerable,
minor, non-quantifiable,
no added benefit, or
reduced benefit
Effect size at outcome level, confidence
interval associated with effect
Table II. G-BA decision breakdown on “Degree of Added Beneft” for new
pharmaceuticals within a specifc patient subpopulation (N=169).
Degree of added beneft Percent of cases
Major 0%
Considerable 10%
Minor 25%
Not quantifiable 7%
Lower 1%
Not proven 57%
For exhibit & sponsorship opportunities, contact:
Companies A-K:
Jason Gerardi
781-972-5452
Companies L-Z:
Carol Dinerstein
781-972-5471
Cambridge Healthtech Institute’s 14th Annual
CHI-PepTalk.comRegister by October 24 for Early-Bird Savings up to $400!Mention Keycode L56 and Save an Additional $100
January 19-23, 2015
San Diego, CATown and Country Resort
& Convention Center
20 Conferences, 300+ Speakers, 1,200+ Participants,
125+ Posters, 90+ Exhibitors, 1 Location
Be a Part of It!
ES521209_BP1114_031.pgs 10.28.2014 23:53 ADV blackyellowmagentacyan

32 BioPharm International www.biopharminternational.com November 2014
AL
L F
IGU
RE
S A
RE
CO
UR
TE
SY
OF
TH
E A
UT
HO
RS
by the Federal Joint Committee
(G-BA), which represents the
se l f-governance st r uc ture of
the German healthcare system.
With the help of the Institute for
Quality and Efficiency in Health
Care (IQWiG), an expert Health
Technology Assessment (HTA)
body, the G-BA determines the
level of added benefit of the new
drug relative to the appropriate
comparative therapy (ACT) cho-
sen by the G-BA as well as the
certainty of evidence presented
by the manufacturer. A br ief
description of these two inputs
that go into the G-BA’s final deci-
sion is included in Table I. Patient-
relevant criteria for additional
medical benefit include improv-
ing health, extending survival,
shortening the burden of i l l-
ness and reducing side effects, or
improving quality of life, and are
outlined in the IQWiG method-
ology paper (2). Originally, the
law was written to include the
possibility that patented products
already on the market would have
to undergo retrospective benefit
assessments; however, manufac-
turers were recently spared from
this potential headache (3).
Once the G-BA reaches a final
conclusion, pricing negotiations
begin with the statutory health
insurance (SHI) umbrella orga-
nization, GKV–SV (Gesetzliche
K r a n k e n v e r s i c h e r u n g –
Spitzenverband), which nego-
tiates on behalf of all SHIs and
also private sickness funds in
Germany. It is important to high-
light that the ACT is not only
used by the G-BA in its assess-
ment, it is also the price anchor
for these negotiations. For drugs
found to have no added benefit,
their price is capped in reference
to the price of the comparator.
Reference pricing to the compara-
tor can be either advantageous if
the ACT is already a high-priced
therapy or devastating if the ACT
is a generic drug. Thus, manu-
facturers looking to enter break-
through therapeutic areas where
the current standard treatment
is a generic will be particularly
challenged. Therapeutic prod-
ucts that demonstrate added ben-
efit are priced above the ACT but
may still face a minimum price
reduction of 7% (formerly 16%)
by law, unless it has been replaced
as part of the price negotiations.
Unfortunately for manufactur-
ers, while the number of prod-
ucts that have gone through the
entire assessment and pricing pro-
cess remains small since the law
was enacted three years ago, early
evidence suggests only limited
correlation exists between ben-
efit ratings and price reductions.
Rather, G-BA’s benefit rating has
primarily served as a door opener
for price negotiations (4).
SnaPShOt Of Benefit aSSeSSmentS and PricinG neGOtiatiOnS under amnOGAs of May 2014, 79 products have
been assessed by the G-BA within
169 patient subpopulations. More
than 50% of these early benefit
assessments have led to ‘no added
benefit’ rulings by the G-BA (see
Table II) (5). Not surprisingly, there
has been considerable variance
observed in the levels of addi-
tional benefit reported by phar-
maceutical manufacturers and the
G-BA. In contrast, the G-BA’s deci-
sions have more closely resembled
IQWiG’s recommendations with a
few notable exceptions (e.g., beli-
mumab, cabazitaxel, eribulin) (6).
Reasons the G-BA has offered for
‘no proven added benefit’ include
inadequate comparator, lack of
a relevant study to back claims
of benefit, lack of data on poten-
tial harms, and omission of data
for relevant patient subpopula-
tions. A more detailed breakdown
of the G-BA’s negative rulings as
of October 2013 is presented in
Figure 1 (7).
As Figure 1 i l lustrates, even
though the outcome of bene-
fit assessment is a key driver of
price negotiations, manufactur-
ers have not always prepared dos-
siers adequately. This, in turn,
compromises the outcome of the
assessment and subsequent price
that is agreed upon. Such prob-
lems with incomplete or inade-
quate evidence may be overcome
european market report
Figure 1. Reason for no proof of added beneft ruling for new pharmaceuticals
within a specifc patient subpopulation (N=113).
32%38%
20%
10%
Evidence inappropriate
Appropriate comparatornot considered
No beneft shown
Evidence incomplete
ES521206_BP1114_032.pgs 10.28.2014 23:53 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 33
european market report
as drug makers gain better under-
standing of the requirements.
To this end, the Federal Joint
Committee offers consultation
opportunities for manufacturers
to give advice on trial design (e.g.,
patient segmentation, compara-
tor selections, and endpoints). Not
all manufacturers, however, have
communicated with the G-BA to
discuss the technical issues and
challenges around preparation of
the benefit dossier, or earlier to
discuss the clinical trial (6).
Despite the market access
challenges that manufacturers
have experienced so far, only a
few products have been pulled
despite negative G-BA rulings and
demands for substantial rebates.
Novartis became the most recent
manufacturer to do this, with-
drawing its oral anti-diabetic
Galvus from the German market
after failing to secure a mutually
beneficial price with payers (8).
Given the size and revenue poten-
tial associated with this market-
place, the fact that few products
have been pulled is not surprising.
However, Hagen Pfundner, the
chairman of Germany’s pharma
lobby VFA and head of Swiss
drugmaker Roche’s German unit,
believes that a recent update to
the AMNOG legislation could lead
to “an increasing number of opt-
out decisions” (9). In the past, a
product’s original launch price in
Germany served as the published
list price for other markets. This
approach is no longer the case.
Since April 2014, the newly nego-
tiated reimbursement amounts
are published as visible ex-factory
prices, effectively replacing the
original list prices as source for
referencing. Drug makers fear the
information could challenge the
entire pricing framework within
Europe (and globally) either caus-
ing a downward spiral in reim-
bursement across the reg ion
or heavy parallel exports from
Germany to other countries. If
this new law is not overturned, it
poses a significant risk to profits
in the industry, especially consid-
ering that price discounts have
been as high as 70% following
G-BA’s benefit assessment and
range on average between 16–30%
(10). More broadly, the new rule
reinforces the importance of
manufacturers understanding the
nuances of this market and hav-
ing strategies in-place to achieve
successful market access.
recOmmendatiOnS fOr manufacturerSWhile Germany is certainly not
the only market that is enforc-
ing more stringent pricing and
reimbursement policies for new
therapeutic products, it is per-
haps scrutinizing the quality and
appropriateness of clinical data
more so than any other country.
Taken together with the fact that
other markets look to Germany to
determine pricing, manufactur-
ers should place a greater empha-
sis on G-BA’s recommendations
when structuring clinical studies.
To date, the majority of AMNOG
submissions did not have much
guiding input from the G-BA prior
to clinical study design and were
based on evidence generated on
Figure 2. Case summary of IQWiG’s beneft assessment of Kadcyla.
Drug
Indication
Subgroupsassessed by
G-BA
Comparatordefned by
G-BA
G-BA resolution
Notes
Kadcyla (trastuzumab emtansine, Roche)
Patients with unresectable, locally advanced or metastatic breast cancer that is HER2+
A. Patients with HER2+,locally advanced,unresectable breast cancer
Radiotherapy
No additional beneftproven (no relevantdata were available)
The company deviated from the G-BA’s specifcation by considering the total target population, for which it used lapatinib + capecitabine as comparator therapy.Thus, no added beneft was found for subpopulations A, C and D. For subpopulation B, there were positive effects in the outcome categories “mortality”, “health-related quality of life” and “serious/severe AEs”, and negative effect in the outcome category “non-serious/non-severe AEs.
No additional beneft proven(no relevant data were available)
No additional beneft proven(no relevant data were available)
Lapatinib + capecitabine
Indication of a major added beneft
Anthracycline (doxorubicin, epirubicin) Individual treatment under consideration ofthe respective approval of the drugs used
B. Patients with HER2+, metastaticbreast cancer, with prior treatmentwith anthracyclines, taxanes andtrastuzumab
C. Patients with HER2+, metastatic breastcancer, with prior treatment with taxanesand trastuzumab, but withoutanthracyclines
D. Patients with HER2+, metastatic breastcancer, with prior treatment with taxanesand trastuzumab, for whom treatment withanthracyclines is not an option
ES521205_BP1114_033.pgs 10.28.2014 23:53 ADV blackyellowmagentacyan

34 BioPharm International www.biopharminternational.com November 2014
a pre-AMNOG world. Moving
forward, proact ively consult-
ing with the G-BA to define the
comparator(s), clinical endpoints
and patient cohorts will be essen-
tial. Manufacturers need to do
this early in product development,
especially prior to starting Phase
III trials. Internally, manufactur-
ers should also enhance commu-
nication between regulatory and
market access teams to strategi-
cally plan for both market autho-
rization requirements and G-BA’s
requirements.
Even before G-BA consulta-
tions, manufacturers need to give
greater consideration to the prod-
uct’s indication. While the indica-
tion does not determine how the
benefit assessment is conducted,
completed assessments indicate
that it can influence the G-BA’s
comparator choice and a pivotal
trial’s relevance. For products with
broad indications, IQWiG and the
G-BA are demanding clinical data
for multiple patient subpopula-
tions and against multiple ACTs.
For example, these commission-
ing bodies recently distinguished
between four subpopulat ions
and ACTs for Roche’s Kadcyla
(see Figure 2) (11). Manufacturers
that have failed to anticipate and
include such data are seeing a
significant reduction in the over-
all level of added benefit granted
to their products (e.g., Pixuvri
and Inlyta) (12). Moving for-
ward, manufacturers will need to
ensure that all relevant subpopu-
lations have robust and statisti-
cally significant clinical endpoints
to support reimbursement, with
increasing demand for quality of
life data. If the resources required
to study multiple populations
using multiple comparators are
too great, pursuing a narrower
indication for a clearly defined
patient population and against a
single comparator serves as a via-
ble alternative.
Manufacturers will also have to
keep in mind that every new indi-
cation for a product will trigger
another round of benefit assess-
ment and a new price negotia-
tion. Here, attempts to negotiate
a higher price with subsequent
indications may be met with resis-
tance by the GKV-SV and prove
to be a significant challenge for
manufacturers. Thus, drug makers
should give greater consideration
to the trade-off between a fast
product launch and the highest
value launch.
Aside f rom data col lect ion
and defining a product’s indica-
tion, manufacturers must also
develop a solid pricing strategy
earlier on in the product devel-
opment process and have capa-
bilities to better predict a products
negotiated price. There is cur-
rently no formula regarding the
rebate amount the pharmaceuti-
cal company has to grant on its
retail price. Furthermore, while
evidence demonstrating added
benefit is required to avoid refer-
ence pricing, it is by no means the
sole determinant of pricing deci-
sions. Rather, the extent to which
a product’s price will be marked
down following a positive benefit
assessment is largely dependent
on its original launch price as well
as the market size and price of
the appropriate clinical compara-
tor. As more products go through
the product review and pricing
process and as more data become
available, manufacturers should
consider developing algorithms
to forecast the benefit assessment
outcomes and the product’s final
net price.
The f irst three years of the
AMNOG reform have proven that
demonstrating added benefit is
no small feat for manufacturers,
and while complaints continue
to be heard from pharmaceutical
stakeholders, the law shows no
signs of slowing down. AMNOG
has not only set new rules for
reimbursement and pricing of
pharmaceuticals in Germany, it
also forces the industry to adapt
at a global level, rethinking how
it brings new products to market.
Manufacturers that prepare thor-
oughly for benefit assessment and
the negotiation processes within it
will be best positioned for success.
aknOwLedGementThe authors would like to thank
Stefan Seliger, PhD, for his review
and insights.
referenceS 1. German Pharmaceutical Industry
Association/BPI, based on IMS World Review 2012.
2. IQWiG, General Methods Version 4.1. (Nov. 28, 2013).
3. G. Collier, A tweak or an outrage? Germany passes new pricing law. March 24, 2014, www.scripintelligence.com/home/A-tweak-or-an-outrage-Germany-passes-new-pricing-law-350844, accessed Aug. 8, 2014.
4. IMS Consulting, Pricing and Market
Access Outlook–2013 edition. 5. LEO Pharma Germany, It´s difficult to
meet HTA criteria according AMNOG – reason why? (June 10, 2014).
6. J. Ruof, et al., Eur J Health Econ. 15, pp 577–589 (2014).
7. PRMA Insights, PRMA Insights Focus:
Pricing and Reimbursement Success in
Germany under AMNOG (2013) 8. F. Kermani, “Novartis Pulls Galvus
From Germany After Failed Price Negotiations,” The Pink Sheet Daily (June 19, 2014).
9. L. Burger and T. Severin, “Germany’s stance on pricing threatens drug firm profits,” Reuters, Feb. 18, 2014, http://uk.reuters.com/article/2014/02/18/us-germany-drugs-analysis-idUKBREA1H09E20140218, accessed Aug. 14, 2014.
10. D. Bahr and T. Huelskoetter, “Comparing the Effectiveness of Prescription Drugs: The German Experience” (May 21, 2014), www.americanprogress.org/issues/healthcare/report/2014/05/21/90120/comparing-the-effectiveness-of-prescription-drugs-the-german-experience/, accessed Aug. 14, 2014.
11. Institute for Quality and Efficiency in Health Care, Trastuzumab emtansine – Benefit assessment according to §35a Social Code Book V
12. C. Henry, “Oncology drugs under AMNOG,” PMLive (May 7, 2014). ◆
european market report
ES521208_BP1114_034.pgs 10.28.2014 23:53 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 35
Yuji
Sakai/G
ett
y Im
ag
es
The past decade has seen con-
siderable growth in the Indian
pharmaceutical industry. India
has emerged as a key sup-
plier of high quality and affordable
medicines not only to the developing
world, but also to developed economies
as well (Figure 1A) (1). This sector has
recorded a compound annual growth
rate (CAGR) of 13.5% over the past five
years and is projected to reach $45 bil-
lion in 2020 (2). With the ongoing shift
from small molecules to biologics, the
Indian biopharmaceutical industry is
also set to replicate the success received
by the Indian pharmaceutical compa-
nies (Figure 1B) (1). The biopharmaceu-
ticals market has witnessed the fastest
growth in the 2013 financial year as
compared to other biotech markets
(e.g., Bio-Agri, Bio-Services, and Bio-
Informatics).
Growth in this sector has also bur-
dened the public institutions that
are responsible for ensuring that the
marketed products are safe and effica-
cious. In India, the Drug Controller
General of India (DCGI)-led Central
Drugs Standards Control Organization
(CDSCO) together with the State
Author it ies are pr imar i ly respon-
sible for ensuring the quality of bio-
tech therapeutics post-approval. The
Indian Pharmacopoeia Commission
(IPC), which creates and publishes
the Indian Pharmacopoeia (IP), how-
ever, plays a key role. The IP, as per
the Drugs and Cosmetics Act of 1940,
prescribes the standards for drugs pro-
duced and/or marketed in India and,
Setting Standards for Biotech Therapeutics in India
Anurag S. Rathore, Renu Jain, M. Kalaivani,
Gunjan Narula, and G. N. Singh
The authors take a look at the
past and future impact of the
Indian Pharmacopoeia
Commission.
Anurag S. Rathore* (pictured) is a
professor, Department of Chemical
Engineering, Indian Institute of
Technology, New Delhi, India. Renu
Jain is a scientist at National Institute of
Biologicals, NOIDA, India. M. Kalaivani
is a scientific assistant, Gunjan Narula
is a pharmacopoeial associate, and
G. N Singh is Secretary-cum-Scientific
Director at the Indian Pharmacopoeia
Commission, Ghaziabad, India.
*To whom all correspondence
should be addressed.
Global Perspective: Indian Pharmacopoeia Commission
ES521017_BP1114_035.pgs 10.28.2014 23:17 ADV blackyellowmagentacyan

36 BioPharm International www.biopharminternational.com November 2014
therefore, plays a significant role
in the control and assurance of
the quality of the pharmaceu-
tical products (3). Unlike a lot of
developing and developed coun-
tries, the standards stated in the
IP are authoritative and legally
enforceable by the Indian regu-
latory authorities (CDSCO and
State Drug Regulators). In this
31st article in the “Elements of
Biopharmaceutical Production”
series, the authors report on the
evolution and future of IPC. The
focus of the article is on biotech
therapeutics.
INDIAN PHARMACOPOEIA COMMISSIONThe IPC was constituted in 1948
with publication of IP defined as
its primary function. The first IP
was published in 1955 followed by
a supplement in 1960. This phar-
macopoeia contained both western
and traditional Indian pharmaceu-
tical products commonly used in
India.
Thereafter, the IP has been pub-
lished at frequent intervals. The
frequency has increased with time
due to the phenomenal growth
in the number of pharmaceutical
products over the past five decades
as well as the diversity in their ori-
gin and content. Over time, the
IP committee has deleted mono-
graphs for products that have
become obsolete and added mono-
graphs based on the therapeutic
merit and medical need (3).
The IPC was established in 2005
and the first addendum, which was
published by IPC in 2005, included
a large number of antiretroviral
drugs and raw plants commonly
used in making medicinal prod-
ucts not covered by any other
pharmacopoeias, which attracted
much global attention. Similarly,
IP 2007 contained 271 new mono-
graphs with focus on those drugs
and formulations that cover the
National Healthcare Programs
and the National List of Essential
Medicines. The addendum in 2008
contained 72 new monographs (4).
The commission had become fully
operational as an autonomous
body under the Ministry of Health
and Family Welfare, Government
of India in 2009 and released IP
2010 (5). IP 2010 contained mono-
graphs on antiretroviral, antican-
cer, antituberculosis, and herbal
drugs. It also included monographs
of biologically derived products
such as vaccines, immunosera for
human use, blood products, and
other biotech and veterinary (bio-
logical and non-biological) prepa-
rations. Addendum 2012 to the IP
2010 incorporated 52 new mono-
graphs (Table I) (3).
The primary objectives of IPC
include the following:
• Develop comprehensivemono-
graphs for drugs and upgrade
them as needed
• Accord pr ior it y to mono -
graphs of drugs included in
the National List of Essential
Medicines
• Collaborate with other phar-
macopoeia (e.g., United States
Pharmacopeia [USP ], Br it ish
Pharmacopoeia [BP], Chinese
Pharmacopeia [ChP], European
Pharmacopoeia [Ph. Eur.], World
Health Organization [WHO],
and Japanese Pharmacopeia [ JP])
to attempt harmonization with
global standards
• Prepare,certify,anddistributeIP
Reference Substances
• PublishNational Formulary of
India
• Organize educational programs
and research activities to gener-
ate awareness about the need for
quality standards for drugs and
related articles/materials (3).
MONOGRAPHS OF BIOTECH THERAPEUTICSThe scope of IPC has been
extended to include products of
biotechnological origin, indig-
enous herbs and herbal products,
veterinary vaccines, and additional
antiretroviral drugs and formula-
Global Perspective: Indian Pharmacopoeia Commission
Table I. Evolution of India Pharmacopoeia (IP) over the past fve decades. Source: Indian Pharmacopoeia (5).
IP Editions (By IP Committee) IP Editions (By IP Commission)
Year Edition Year Edition
1955 I 2005 Addendum
1960 Supplement 2007 V
1966 II 2008 Addendum
1975 Supplement 2010 VI
1985 III 2012 Addendum
1989 & 1991 Addendum 2014 VII (Recent)
1996 IV 2015 Addendum (To be published)
2000 Addendum
2000 Vet supplement
2002 Addendum
ES521011_BP1114_036.pgs 10.28.2014 23:16 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 37
Al
l f
Igu
rE
S c
ou
rt
ES
y o
f t
hE
Au
th
or
S
tions, inclusive of commonly used
fixed-dose combinations. IP 2014
had 577 new monographs and
included monographs of API [134],
formulations [161], excipients [18],
new drug substances [43], antivi-
ral [11] and anticancer [19], anti-
biotics [10], herbal [31], vaccine
and immunosera for human use
[5], insulin products [6], and bio-
technology products [7]. IP 2014
also included 19 new radiopharma-
ceutical monographs and a general
chapter on radiopharmaceutical
preparations (4). Table II presents a
comparison of monographs related
to biotech therapeutics across the
different international pharmaco-
poeial bodies. It can be seen that IP
compares well with other leading
global agencies. Figure 2 illustrates
the evolution and key milestones
of IPC since formation.
CHALLENGES AND POSSIBLE SOLUTIONSWhile significant advancements
have been made in the past decade
by the IPC since its formation, the
complexities of dealing with bio-
tech therapeutics raise the bar fur-
ther. The following are some of the
key challenges IPC faces today with
respect to successful creation and
implementation of monographs of
biotech therapeutic products.
• Li m i t e d e x p e ri e n ce w i t h b i o -
te c h pr o ce ss e s an d pr o duc t s .
Limited experience with bio-
tech processes and products is
a challenge faced by many gov-
ernment organizations in India
and across the world. Approval
of the first recombinant DNA
pro duc t , hu m a n i n s u l i n ,
occurred only in 1982. The
experience is even more lim-
ited in India. The government,
through agencies such as the
Department of Biotechnology,
actively funds events that allow
for training and sharing of best
practices and lessons learned.
Such activities are essential
for gradually building a strong
foundation of in-house experts.
For the interim, IPC will con-
tinue to rely on the scientific
panels that presently provide
scientific and technical super-
vision (6).
• L a c k o f i n - h o u s e l a b o r a t o r y.
While IPC has a laboratory for
characterization of reference
standards related to pharma-
ceutical products, it is in the
process of creating a state-of-
the-art laboratory for biotech
products. At present, IPC relies
on the National Institute of
Biological (NIB) for this set of
activities.
• Creation of reference standards
for biotech therapeutics. Biotech
products are complex in nature
and, therefore, no two products
are exactly the same (7). This
really complicates the task of
creating a reference standard
for a biotech therapeutic. So far
such reference standards are
offered for only a handful of
simpler biotech products, such
as interleukin and insulin. IPC,
together with NIB, is working on
creating a robust strategy for cre-
ation, characterization, storage,
and distribution of these stan-
dards to support the domestic
biotech industry.
• Collaborations with other global
pharmacopoeial agencies. The
scope of activities at IPC along
with the complexities associ-
ated with biotech therapeutics
make it a necessary require-
ment that the various pharma-
copeial agencies work together
with a col laborat ive spir it.
IPC and USP have been work-
ing closely together and orga-
nize an annual conference to
share updates and ideas. Similar
relationships need to be pur-
sued with other global agen-
cies such as National Institute
of Biological Standards and
Control (NIBSC), and European
Global Perspective: Indian Pharmacopoeia Commission
Figure 1. growth of the Indian (A) pharmaceutical industry and (B) biopharmaceutical industry.
50
45
40
35
30
25
20
15
10
5
0
1.4
1.2
1
0.8
0.6
0.4
0.2
0
2008 2009 2010 2011 2012 2013F
2003
-04
2004
-05
2005
-06
2006
-07
2007
-08
2008
-09
2009
-10
2010
-11
2011
-12
2012
-13
2014F2015F2016F2020F
USD
(B
illio
ns)
USD
(B
illio
ns)
YEARSYEARS
A BCAGR till now
CAGR expected
Export (billion dollars)
Domestic (billion dollars)
ES521013_BP1114_037.pgs 10.28.2014 23:16 ADV blackyellowmagentacyan

38 BioPharm International www.biopharminternational.com November 2014
Global Perspective: Indian Pharmacopoeia Commission
Directorate for the Quality of
Medicines (EDQM). As the IPC
grows in its capabilities, such
meaningful collaborations will
be mutually beneficial.
FUTURE PERSPECTIVEThe primary responsibil ity of
the IPC has been towards pub-
l ishing the IP at a f requency
that meets the requirement of
the industry and the country. IP
2014 included several biotech
monographs, and the next IP is
likely to include many new bio-
tech monographs as well in view
of the increasing dominance of
biotech therapeutics in the phar-
maceutical marketplace. IPC is in
the process of monograph verifi-
cation stage for rituximab drug
substance and drug product and
teriparatide drug substance and
drug product monographs. Many
new general chapters pertain-
ing to topics such as therapeu-
tic monoclonal antibodies, host
Table II: comparison of the status of monographs of biotech therapeutics across the various leading pharmacopeial
organizations across the world (8-12). IP is Indian Pharmacopoeia. chP is Chinese Pharmacopeia, uSP is United States
Pharmacopeia. BP is British Pharmacopoeia. Ph. Eur. is European Pharmacopoeia. JP is Japanese Pharmacopeia.
Biotech Monographs IP 2014 ChP 2010 USP 2013 BP 2014 Ph. Eur 2014 JP 2011
Erythropoietin Concentration Solution √ X X √ √ √
Erythropoietin for Injection √ √ X √ X X
Erythropoietin Injection √ √ X √ X X
Filgrastim Concentrated Solution √ √ X √ √ √
Filgrastim Injection √ X X X X √
Interferon Alpha 2 Concentration Solution √ X X √ √ X
Interferon Alpha 2a Injection √ √ X √ X X
Interferon Alpha 2b Injection √ √ X X X X
Interferon Beta 1a Concentration Solution √ X X √ √ X
Recombinant Streptokinase Bulk Solution √ X X X X X
Recombinant Streptokinase for Injection √ √ X X X X
Insulin Aspart √ X X √ √ X
Insulin Aspart Injection √ X X √ X X
Biphasic Insulin Aspart Injection √ X X X X X
Insulin Lispro √ X √ √ √ X
Insulin Lispro Injection √ X √ √ X X
Biphasic Insulin Lispro Injection √ X X X X X
Human Insulin √ X √ √ √ √
Insulin Injection Biphasic Isophane √ X √ √ √ X
Insulin Injection Isophane √ X √ √ √ X
Insulin Injection Soluble √ X √ √ √ X
Insulin Zinc Suspension √ X √ √ √ X
Insulin Zinc Suspension (Amorphous) √ X √ √ √ X
Insulin Zinc Suspension (Crystalline) √ X √ √ √ X
Insulin Glargine X X X X √ √
Human Glucagon X X √ √ X X
Human Glucagon for Injection X X √ X X X
Somatropin X X √ √ √ X
Somatropin Concentrated Solution X X X √ √ X
Somatropin for Injection X X √ √ √ X
Somatropin Injection X X X √ X X
Interferon Gamma 1b Concentrated Solution X X X √ √ X
Molgramostim Concentrated Solution X X X √ √ X
ES521012_BP1114_038.pgs 10.28.2014 23:16 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 39
Global Perspective: Indian Pharmacopoeia Commission
cell proteins and DNA, and viral
safety are in the works for the
next IP edition.
As mentioned previously, cre-
ating and implementing a pro-
cess for producing, storing, and
distributing reference standards
for biotech therapeutic products
is a key focus for IPC at present.
To establish these standards, can-
didate materials can be sourced
from multiple Indian manufactur-
ers (with certificate of analysis)
and calibrated against the origi-
nator product. Development of
reference standards for biotech
therapeutics can be done by col-
laborative studies involving the
manufacturers and other govern-
ment agencies such as the NIB.
The WHO International Standard
(WHO IS) could be considered
at the highest level of hierarchy
(primary standard) of reference
standard. The reference standard
should have the following key
components:
• Candidate materials sourced
from the manufacturers must
comply with the acceptance
criteria provided in the IPC
monograph. The cert i f icate
of analysis should be submit-
ted and should include the
critical quality attributes with
respect to identity, content,
and potency of the product.
Stability of the material should
be already established with
its formulation/presentation
defined by the manufacturer.
• Assessment of suitability of the
candidate material should be
evaluated by IPC with respect
to the content, formulation, and
final presentation of reference
standard material.
• A multi-centric collaborative
study should be planned to
verify the IP reference stan-
dard. The detailed study testing
protocol should include vali-
dated method to be followed
for analytical testing, storage,
and handling along with the
procedures for reporting and
submission of results.
Another major initiative for IPC
is establishing a laboratory for
verification of biological mono-
graphs and characterization of
the reference standards for bio-
logical products. The laboratory
will have state-of-the-art analyti-
cal instrumentation for testing/
analysis of biotechnology ther-
apeutics. The scope of the lab
includes:
• Development/verif ication of
methods and limits for biologi-
cal monographs
• Development of IP reference
standards for biotech therapeu-
tics
The success of these two initia-
tives is crucial for IPC to make a
meaningful contribution to the
Indian biotech industry.
SUMMARYWith biotechnology based thera-
peutics becoming increasingly
important to India, organizations
such as the IPC will need to evolve
to effectively do their part in the
process of bringing safe and effica-
cious therapeutic products to the
market. This article presents an
update on the challenges faced by
Figure 2. Evolution of Indian Pharmacopoeia commission over the past decade.
IP 2007(14 Monographs)
IP 2014(24 Monographs)
Next editionof IP
IP 2010
Addendum 2012(15 Monographs)
• Erythropoietin drug substance• Filgrsatim drug substance• Interferon alfa 2 drug substance• Streptokinase drug substance• Human insulin drug substance and drug products
• Erythropoietin drug substance• Filgrsatim drug substance• Interferon alfa 2 drug substance• Streptokinase drug substance• Human insulin drug substance and drug products
• Emphasis on Therapeutic Monoclonal antibodies and PEGylated products
• Erythropoietin drug substance and drug products• Filgrsatim drug substance and drug products• Interferon alfa 2 drug substance and drug products• Streptokinase drug substance and drug products• Human insulin drug substance and drug products• Insulin aspart drug substance and drug products• Insulin lispro drug substance and drug products
ES521019_BP1114_039.pgs 10.28.2014 23:17 ADV blackyellowmagentacyan

40 BioPharm International www.biopharminternational.com November 2014
LaBrenz adds that developing the
proper experimental design space
before sett ing up DoE experi-
ments ensures that the parameter
critical for the stability of an API
is identified. More specifically,
conducting a screening DoE to
determine which product quality
attributes (and the corresponding
output parameters used to rep-
resent them) are relevant in the
design space is helpful, accord-
ing to Nguyen. Accelerated stabil-
ity studies can also be performed
to determine relevant output
parameters.
Another key to generat ing
appropriate and relevant data is to
make sure that normal-distributed
data, obtained either directly or
after transformation, are used. If
there is a major process change,
it is necessary to evaluate and
understand any impacts on the
protein and the formulat ion,
according to Yang, which may
mean conducting comparability
or bridging studies.
MANAGING THE DATAFor DoE studies to be useful, the
generated data must not only be
relevant, but manageable. There
are different approaches to address-
ing this problem.
The solution for LaBrenz is
to use an open, read-only data-
base that can be shared between
mult iple groups, such as pre -
formulation, formulation, and
analytical development groups,
so that each unit can focus on
particular aspects of interest in
a DoE. “While a formulat ion
scientist needs to know where
the most stable space for an API
resides, an analytical chemist
may be more interested in the
variability and reproducibility
of results, both of which can be
obtained from a well-designed
DoE,” he says.
Nguyen remarks that using soft-
ware to automate data collection
and extraction of the relevant out-
put parameters for statistical analy-
sis is important. She also stresses
that having an understanding of
which output parameters to col-
lect and limiting the excipients
examined to a subset of approved
parenteral excipients can reduce
the amount of data that must be
analyzed.
Training on data processing is
also crucial, regardless of what
approach is used. LaBrenz uses
many different tools depending
on the level of complexity required
for a given project, and often the
choice of software is determined
by collaborators. “It isn’t the soft-
ware package that actually mat-
ters. It is all of the extra training
to develop my applied statistics
skills, including six-sigma training
and seminars, that helps me on the
job,” he states. ◆
Formulation DevelopmentÑContin. from page 29
the IPC and some of the significant
initiatives that the organization is
pursuing.
ACKNOWLEDGEMENTSThe authors would like to thank
the members of the IPC’s Expert
Committee on Biologicals and rDNA
Products. These include Dr. S.S.
Jadhav and Dr. Sunil Gairola (Serum
Institute of India), Dr. Venkata
Ramana (Reliance Life Sciences), Dr.
Anil Kukreja (Roche Products Pvt.
Ltd), Dr. Sriram Akundi (Biocon
Foundation), Dr. Jaideep Moitra
(Gennova Biopharmaceuticals),
Dr. Rahul Kulkarni (Gennova
Biopharmaceuticals), Dr. Himanshu
Gadgil (Intas Biopharmaceuticals),
Mrs. Kinnari Vyas and Dr. Susoban
Das (Intas Biopharmaceuticals), Dr.
Satyanarayana Subrahmanyam
(Dr. Reddy’s Laboratories Limited),
Dr. Sanjeev Kumar (Zydus Cadilla)
Dr. M. Kalaivani (IPC), Ms. Gunjan
Narula (IPC), and Dr. Renu Jain
(NIB). Prof. Anurag S. Rathore
(IIT Delhi) is the Chairman of the
Committee. Dr. G. N. Singh is pres-
ently the Drug Controller General
of India (DCGI) and is also the
Scientific Director of IPC.
REFERENCES 1. Association f Biotechnology
Led Enterprises, Industry
Insight, Biospectrum Asian
Edition, Vol. 1 (June 2013).
2. PricewaterhouseCooper, India Pharma
Inc.: Capitalizing on India’s growth
potential (PWC, November 2010).
3. Indian Pharmacopoeia (Ministry
of Health & Family Welfare),
Govt. of India (2014).
4. R.M. Singh, “Role of Indian
Pharmacopoeia for Quality Medicines
in India,” Spinco Biotech Cutting
Edge, 1 (6) (December 2013).
5. IPC, Indian Pharmacopoeia,
6th Edition (September
2010), www.ipc.gov.in.
6. A. S. Rathore, BioPharm Inter.
24 (11) (November 2011).
7. A. S. Rathore and I. S. Krull, LC
GC North America 28 (2010).
8. Pharmacopoeia of the People’s
Republic of China, 2010, The
state Pharmacopoeia Commission
of P.R. China, China Medical
Science Press, Beijing, China.
9. USP, USP 37 NF 32, United States
Pharmacopoeia Commission (Unite
Book Press Inc., Baltimore, MD 2014).
10. BP, British Pharmacopoeia, 2014
by The Stationary office on behalf
of The Medicines and Healthcare
Products Regulatory Agency (MHRA),
(London SW1W9SZ 2013).
11. Ph. Eur., The Europoean
Pharmacopoeia 8.0, Directorae
for quality of medicines and
healthcare of the Council of Europe
(EDQM), Council of Europe, 67075
Strasbourg, Cedex, France (2013).
12. JP, The Japanese Pharmacopoeia,
16th Edition, Pharmaceutical
and Medical Devices regulatory
Science Society of Japan,
Tokyo 150-002, Japan. ◆
Global Perspective: Indian Pharmacopoeia Commission
ES521016_BP1114_040.pgs 10.28.2014 23:17 ADV blackyellowmagentacyan

For questions, contact Kristen Moore at [email protected]
Presenter:
Ken CookEU Bio-separations Support ExpertThermo Fisher Scientifc
Moderator:
Mike TracyGroup PublisherBioPharm International
Sponsored by
Presented by
Who Should Attend: n Biopharmaceutical research
and development chemists and
laboratory managers
n Biopharmaceutical QC chemists and
laboratory managers
n Protein characterization chemists
n Fermentation production analysts
n Biotherapeutic protein clone
selection chemists
EVENT OVERVIEW:
Over the past decade, the number of monoclonal antibodies
(mAb) candidates entering the clinical pipeline has
grown signifcantly. In addition, the number of antibody
drug conjugates that use mAb specifcity to carry drug
payloads to target sites has increased. As a result, analytical
characterization is in high demand.
This webinar will discuss new innovations in sample
preparation, column technology, UHPLC, and high resolution
mass spectroscopy (HRMS) that allow the development of
analytical methods with run times of less than 5 minutes for
all routine methods.
Orbitrap technology has been established as the most
powerful MS technology for protein characterization. How
the new ultra high resolution Orbitrap technology can
be incorporated into a complete workfow for biopharma
analysis will also be presented.
LIVE WEBCASTThursday, November 13, 2014 at 8:00 am PST/ 11:00 am EST/ 4:00 pm GMT/ 5:00 pm CET
Register for free at http://www.biopharminternational.com/Innovations
Key Learning Objectives:
n Fast method development for charged variant analysis
and ADC characterization
n Rapid sample preparation for increased throughput and
precision
n Integration of ultra-high resolution LC-MS into the routine
biotherapeutic protein analysis workfow
ES524462_BP1114_041_FP.pgs 10.30.2014 22:28 ADV blackyellowmagentacyan

42 BioPharm International www.biopharminternational.com November 2014
Sve
ta D
em
ido
ff/G
ett
y Im
ag
es
Troubleshooting
Removal and inactivation of adventi-
tious and endogenous viruses have tra-
ditionally been achieved during the
downstream purification of biologics. Viral
clearance is assessed in small-scale tests, and
regulatory guidance documents provide a gen-
eral framework for how these tests should be
performed (1). Even with guidance, however,
demonstrating an appropriate level of viral
clearance can be challenging for biologics
manufacturers.
Upstream viral clearance Using media with a low level of viral contami-
nation can lead to major problems in biolog-
ics manufacturing. Cell-culture media and
other raw materials, particularly those derived
from animals, should be subjected to rigor-
ous testing and viral inactivation treatments,
according to S. Steve Zhou, director of virology
and molecular biology with the MicroBioTest
Division of Microbac Laboratories. In addi-
tion to treatment with heat and ultraviolet
radiation, virus retentive filtration is recog-
nized as one of the most efficient and robust
virus removal steps, and implementation in
the media feeding process could decrease the
risk of contamination significantly, accord-
ing to Horst Ruppach, senior director, viral
clearance with Charles River Biologics Testing
Solutions. “Current filters can be used in this
application, but they were not designed to
run under continuous and high throughput
conditions like those required for media sup-
ply,” he observes. Filter vendors are currently
being asked to modify the filter design for
this specific approach. Viral clearance stud-
ies will also need to be designed differently in
order to address the specific condi-
tions associated with media supply,
Ruppach adds.
Facility design and process monitoring Conditions throughout the commercial manu-
facturing process must be constantly monitored
to avoid viral contamination events. One major
concern for biologics production is the entry
of a small, non-enveloped, chemically resistant
virus into the manufacturing system, accord-
ing to Zhou. “Good facility design and strict
compliance with good manufacturing practice
is the best approach to avoiding this problem,”
he says. Equipment and process failures, such as
inadequate raw material screening or failure of
an upstream inactivation method, particularly
those that go undetected, are also a concern
with respect to potential viral contamination.
In these cases, close monitoring of the process,
preferably using automated systems, and a good
quality assurance/quality control program are
essential for preventing such problems, accord-
ing to Zhou.
minimizing manUFactUring costAs purification templates are established, the
cost of goods is of particular importance
because there is often pressure to limit oper-
ations to those that are necessary for bio-
therapeutic purification rather than include
operations that confer a marginal improve-
ment of product quality, according to Trish
cell-culture media and other
raw materials should be sub-
jected to rigorous testing and
viral inactivation treatments.
Viral Clearance Challenges in Bioprocessing Challenges remain for virus removal and validation.
Cynthia A. Challener is a contributing
editor to BioPharm International.
ES521009_BP1114_042.pgs 10.28.2014 23:15 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 43
troubleshooting
Greenhalgh, virology manager for
EMD Millipore. Processes with
fewer purification steps present
a challenge to virus clearance,
however, because higher removal
claims are expected with indi-
vidual unit operations. “Access to
high titer virus preparations in
testing labs is one way to achieve
high clearance levels, and i f
complete clearance is observed
across the unit operations, high
log reduction values (LRVs) will
be obtained,” says Greenhalgh.
“Meeting clearance targets by eval-
uating a minimal number of steps
that each deliver high removal
can be a risky approach, and a
more thorough evaluation of addi-
tional purification steps expected
to contribute to virus removal is
preferred by regulatory agencies,”
she continues.
More recently, there has been a
focus on understanding the impact
of small changes in the operating
window of individual unit opera-
tions on product quality. “There
is an expectation that the impact
of these changes on the virus
clearance capabilities for unit
operations, particularly chromato-
graphic purification steps, will be
understood,” Greenhalgh explains.
Historical virus clearance data with
the same template can be invalu-
able in setting realistic expecta-
tions for unit operation clearance.
Ideally, however, she notes that
clearance studies should also evalu-
ate conditions outside the process
center to more fully understand
the robustness for virus removal.
Comprehensive risk analysis is
often effective for highlighting
and prioritizing such evaluations
to streamline costly virus testing,
according to Greenhalgh.
process representationAnother challenge for viral clear-
ance validation is accurate process
representation. “In order to perform
high-quality viral clearance studies
and avoid unreliable, inaccurate, or
outdated viral clearance data, it is
necessary to regularly review the
manufacturing process and ensure
that the current manufacturing
process matches what was tested in
the viral clearance study,” accord-
ing to Zhou. A thorough definition
of full-scale process conditions is
particularly important so that they
can be assessed in small-scale viral
clearance tests.
These tests should also consider
process excursions, including inter-
ruptions, depressurization events,
and minor changes in feed quality
from chromatographic unit oper-
ations, according to Greenhalgh.
Zhou agrees: “In addition to hav-
ing a thorough understanding of
the process steps, particularly the
process parameters that are critical
for robust viral clearance, it is nec-
essary to consider worst-case sce-
narios in order to accurately define
the design space for viral clearance
testing.” He also believes that it
is important to update the design
space as new knowledge develops.
These assessments of process excur-
sions require open communication
between the biologics manufac-
turer and the testing laboratory to
develop comprehensive evaluation
plans, according to Greenhalgh.
For scale-down tests to provide
reliable viral clearance data, the
actual challenge feed must be rep-
resentative of that in the full-scale
process. Achieving this goal can be
difficult, because the test material
is typically frozen for shipping to
the testing lab, potentially leading
to changes in the process interme-
diates due to aggregation or prod-
uct degradation, which can result
in different performance for indi-
vidual unit operations compared
to that observed during process
development. “Understanding the
impact of shipping and extended
storage on performance and the
development of mitigation strat-
egies are important for ensuring
accurate virus clearance assess-
ments,” Greenhalgh says.
continUoUs processingInterest in continuous processing
of biologics using single-use sys-
tems is gaining traction because this
approach can significantly reduce
production costs, particularly for
smaller-volume APIs. Viral clear-
ance becomes even more impor-
tant under continuous production
conditions, according to Ruppach.
“Contaminants typically detected
during the fermentation process
may enter the purification process
under fully continuous produc-
tion conditions. Other questions
must also be addressed: How can
a potential contamination best be
mimicked in a process where virus
contaminants enter the downstream
process under a constant flow?
Will continuous processing impact
the viral inactivation and removal
capacities of downstream process
steps for which effective inactivation
or removal could be demonstrated
under standard conditions like low
pH inactivation, anion exchange
(AEX) chromatography, or virus-
retentive filtration? Further stud-
ies need to be performed to answer
these questions,” he states.
model virUs selectionPresently, according to Ruppach, the
same set of model viruses (murine
leukemia virus [MuLV], pseudora-
bies virus [PRV], reovirus [Reo-3],
and minute virus of mice/porcine
parvovirus [MVM/PPV]) is applied
for the viral clearance validation of
cell line-derived recombinant prod-
ucts. The achieved single reduction
factors are summed up to an overall
reduction factor that describes the
general virus inactivation/removal
capacity of the downstream pro-
cess. For instance, he notes that it is
accepted that AEX chromatography,
ES521014_BP1114_043.pgs 10.28.2014 23:16 ADV blackyellowmagentacyan

44 BioPharm International www.biopharminternational.com November 2014
troubleshooting
when run under certain conditions,
is highly effective in removing
this set of model viruses. It is also
known that low pH inactivation is
an effective inactivation step for
enveloped viruses when high reduc-
tion factors are demonstrated for
the two enveloped viruses MuLV
and PRV. “It is also known, however,
that other model viruses behave dif-
ferently. The Poliovirus, for instance,
is not effectively removed by AEX
chromatography under the same
conditions, and HIV-1 and bovine
viral diarrhea virus (BVDV) are
much more resistant to low pH
inactivation compared with MuLV
and PRV. These varying responses
raise questions about using the
same model viruses for all steps,
and a discussion should be initiated
regarding how robust viral clear-
ance can better be demonstrated,”
Ruppach asserts.
In addition, because nanofiltra-
tion is known to be the most effec-
tive virus removal step and can
remove both large (MuLV, PRV)
and small (MVM, PPV) viruses,
there is some discussion about the
use of these small model viruses
as surrogates for the larger viruses,
according to Ruppach. He points
out that some companies have in
fact claimed MVM removal data
as indicative of MuLV removal via
virus-retentive filtration or used
a fixed-reduction factor based on
internal experiments. “This practice
is not in full compliance with cur-
rent guidelines, but some agencies
have accepted this type of data for
IND applications of mAbs [mono-
clonal antibodies] derived from
CHO [Chinese hamster ovary] cell
lines. It remains uncertain, however,
whether all agencies will accept this
practice and if it can be applied for
late-stage viral clearance studies and
other products,” he comments.
Another issue with viral clear-
ance testing is the variable and often
unknown quality of the virus prep-
arations or spikes that are used in
these tests, according to Greenhalgh.
The Parenteral Drug Association
Technical Report 47 (2) provides a
framework for the preparation and
characterization of virus prepara-
tions, and individual testing labs
have developed their own descrip-
tions for virus preparations of differ-
ing purities. Generally, Greenhalgh
notes that virus purity has the big-
gest impact on the virus filtration
step: less purified preparations are
more likely to negatively impact the
virus filter performance by reduc-
ing the volumetric throughput and
ultimately resulting in over-sizing of
the filtration area and an increased
cost of goods for this dedicated virus
removal step. “Pre-studies to opti-
mize both the feed and the virus
spike level are critical prerequisites
for ensuring that expected perfor-
mance targets are met,” she states.
glp and/or gmp?Viral clearance studies, when per-
formed by contract research orga-
nizations (CROs), are frequently
performed following good labo-
ratory practices (GLP) principles.
Recently, however, the question
of whether viral clearance studies
should follow GMP rather than
GLP principles has been raised.
“Audits performed by customers at
CRO sites more often follow GMP
rather than GLP processes, and
typical GMP requirements, such
as corrective action and preven-
tive action (CAPA) procedures, are
requested,” says Ruppach.
This discussion is additionally
stimulated by the fact that viral
clearance studies are required at
different stages of the product
lifecycle, from before the clinical
phase through more comprehen-
sive studies for marketing autho-
rization. In the first case, a fully
validated production process is
typically not in place. In the lat-
ter case, a fully GMP-compliant
validated production process must
be in place. Accordingly, a GMP-
compliant viral clearance study
is more important for the late
stage rather than the early stage
of the product development pro-
cess, according to Ruppach. “It is
important, therefore, that CROs
offering viral clearance services
following GMP principles must
not apply all of the measurements
that are important for a production
site that manufactures and releases
pharmaceuticals for human use,”
he asserts.
importance oF commUnicationMeeting regulatory requirements
for virus safety depends on well-
designed studies that demonstrate
virus clearance across multiple
orthogonal steps with accurate
scale-down conditions, according
to Greenhalgh. “Comprehensive
test design resulting from thor-
ough process understanding and
communication between the bio-
logics manufacturer and the virus
clearance testing lab is essential to
meeting these goals.”
reFerences 1. ICH, Q5A. Guidance on Viral Safety
Evaluation of Biotechnology Products
Derived From Cell Lines of Human or
Animal Origin (1998).
2. Parenteral Drug Association,
Technical Report No. 47: Preparation
of Virus Spikes Used for Virus
Clearance Studies (2010). ◆
the question of
whether viral clear-
ance studies should
follow gmp rather
than glp principles
has been raised.
ES521020_BP1114_044.pgs 10.28.2014 23:17 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 45
Analytical Best Practices
Developing Representative Sampling Plans for Development, Problem Solving, and Validation The ability to define a scientifically justified and statistically sound sampling procedure is a fundamental skill in modern systematic drug development.
In all product and process development and
in all validation activities, developing a
representative sample and the correct and
defendable use of the statistical method used
are crucial. In all sampling activities, a scien-
tifically sound sampling plan should be devel-
oped, justified, and implemented. Sampling
activities include clinical trials, formulation,
stability (long term and accelerated), process
characterization, analytical method develop-
ment, method validation, process validation,
and release testing.
International Conference on Harmonization
(ICH) Q8, Q9, Q10, and Q11 (1–4) all require sta-
tistically valid sampling procedures in test and
product and process development. Specifically
Q8, Q9, and Q10 Questions and Answers (R4),
states (5):
“Q6: Do traditional sampling approaches apply to real
time release (RTR) testing?
A6: No, traditional sampling plans for in-process and
end-product testing involve a discrete sample size
that represents the minimal sampling expectations.
Generally, the use of RTR testing will include more
extensive on-line/in-line measurement. A scientifically
sound sampling approach should be developed, justi-
fied, and implemented. (Approved April 2009) process-
ing, in-process materials, and drug product quality can
provide an opportunity to shift controls upstream and
minimize the need for end product testing.”
The purpose of this paper is to organize
a logical framework and identify the appro-
priate tools that aid in the development of
a statistically valid sampling protocol. Due
to the complexity of the kinds of issues and
the types of problems to be solved, each sam-
pling procedure will be somewhat unique;
however, there are common issues and ques-
t ions that each sampling pro-
tocol will need to consider and
address.
sTATIsTIcAL MeTHODs fOR PRODUcT DeVeLOPMenTThe following are generally key steps for using
statistical methods for problem solving and
product development.
Define the business case
The business case explains the development
objective, how each activity relates to qual-
ity objectives, quality target product pro-
f i les (QTTPs), cr it ical quality attr ibutes
(CQAs), timelines or product development
requirements, and why the activity needs to
be completed. The business case gives con-
text to development and validation activities
and helps CMC teams understand how each
activity fits into overall business and qual-
ity imperatives. Failure to understand the
business case for development and validation
activities causes discontinuity in development
activities and the logic of what, why, and how
much becomes hard to justify and or file to the
appropriate health agencies.
Define the problem
Problem definitions describe what we don’t
know and or what is wrong with our current
performance. Problem definitions are essen-
tial for problem sampling plan development
and rationalization. Limitations and/or scope
failure to understand the
business case for develop-
ment and validation activi-
ties causes discontinuity.
Thomas A. Little is president of Thomas
A. Little Consulting, [email protected].
ES520995_BP1114_045.pgs 10.28.2014 23:15 ADV blackyellowmagentacyan

46 BioPharm International www.biopharminternational.com November 2014
Analytical Best Practices
ALL F
IGU
RE
S C
OU
RT
ES
Y O
F T
HE
AU
TH
OR
associated with each problem
definition is critical in defining
the associated population of units
associated with the problem.
Also associated with the problem
definition, there should be clar-
ity on what is the sampling unit
(batch, vial, drum etc.)
Define all objectives,
goals, and study questions
From the problem def init ion,
objectives, goals and study ques-
t ions must be def ined. Goals
come in four forms: maximize,
minimize, match target, and
none. Limits and acceptance cri-
teria should also be defined. The
sampling plan will be designed
to ensure all study questions are
answered, goals are achieved, and
questions are sufficiently precise
and accurate relative to the limits
and tolerances of the acceptance
criteria.
D e t e r m i n e a l l f a c t o r s a n d
responses and analytical methods
Based on the study questions and
goals, what must be measured to
meet the business case and solve
the problem? All factors that
influence the problem and study
questions must be defined. All
responses and analytical meth-
ods associated with the problem
need to be clarified. In many cases,
the factors and/or responses that
are currently measured in batch
records or in on-line data systems
do not address the problem to be
solved or the process to be charac-
terized. Care should be exercised
to assure there are no missing mea-
surements or the business case will
not be met or the problem will not
be addressed correctly.
Define the population
Based on the study questions,
unit def init ion, and problem
statement, what is the popula-
t ion of units that need to be
understood? Population defini-
tion is crucial prior to sampling
plan formalization. For R&D, the
population is often a function
of formulation and or configura-
tion. Another term that is often
associated with the population is
“volume.” How will the product
perform in volume and at scale
versus the limited product test-
ing that is performed in small-
scale studies?
Define the sample that will rep-
resent the population, study
quest ions , and t he de f ine d
problem
A sampling plan needs to be for-
mally defined and scientifically
justified to assure it is representa-
tive of the population and it meets
the all defined study objectives
and acceptance criteria.
Figure 1: Partition of variation analysis for sampling method determination.
Partition of varation (POV) crossed, dependent analysis
. . . . .Between total 0.000021 4.55 0.004601 0.5900 0.9622 Between sublot-fill/orientation 0.000002 0.43 0.001422 0.2498 0.9721 Between lot number 0.000016 3.41 0.003981 1.1415 0.3247 Between sublot-fill/orientation*lot number 0.000003 0.71 0.001814 0.2370 0.9964 . . .Within total 0.000444 95.45 0.021080 Within sublot-fill/orientation 0.000107 22.94 0.010334 Within lot number 0.000253 54.27 0.015895 Within sublot-fill/orientation*lotnumber 0.000042 9.01 0.006476 Common 0.000043 9.24 0.006559 . . .Total 0.000466 100.00 0.021577
PopVariance
Sqrt(varComp)% of TotalComponent F Ratio
Perc
en
t o
f to
tal
vari
ati
on
100
80
60
40
20
0
Variance components
Wit
hin
lo
t n
um
ber
Wit
hin
su
blo
t-fi
ll/o
rien
tati
on
Co
mm
on
Wit
hin
su
blo
t-fi
ll/o
rien
tati
on
*lo
t n
um
ber
Betw
een
lo
t n
um
ber
Betw
een
su
blo
t-fi
ll/o
rien
tati
on
*lo
t n
um
ber
Betw
een
su
blo
t-fi
ll/o
rien
tati
on
Prob>F Sig.
2 Level POV analysis: sublot-Fill/orientation, lot number
ES520997_BP1114_046.pgs 10.28.2014 23:15 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 47
Analytical Best Practices
WHO guidelines for representa-
tive sampling state (6): “Representat ive sample, Sample
obtained according to a sampling pro-
cedure designed to ensure that the dif-
ferent parts of a batch or the different
properties of a non-uniform material
are proportionately represented.”
The FDA process validation
guideline states (7):
“The sampling plan, including sampling
points, number of samples, and the
frequency of sampling for each unit
operation and attribute. The number of
samples should be adequate to provide
sufficient statistical confidence of qual-
ity both within a batch and between
batches. The confidence level selected
can be based on risk analysis as it
relates to the particular attribute under
examination. Sampling during this
stage should be more extensive than is
typical during routine production.”
All statistically justifiable sam-
pling plans require two primary
considerations: sampling method
and sample size.
Define the sampling method
The sampling method is defined
to clarify “how” samples are taken,
“where” they are taken, and “how
often.” How many samples are taken
is sample size. To determine the sam-
pling method, care must be exer-
cised to assure the samples are taken
from the primary sources of varia-
tion. Partition of variation (POV) or
components of variation (COV) anal-
ysis are used to determine the pro-
portion of variation within/between
batch for example. In Figure 1, 54%
of the variation occurs within the lot,
so at least 54% of the measurements
need to be allocated to the within lot
sampling to be representative. The
batch-to-batch variation is only 3%
so many batches are not needed in
this example. If 90% of the variation
was between batches, then 90% of
the samples should be from multiple
batches.
Define the sample size
Sampling method must be defined
first, then sample size. There are
many International Organization
for Standardization (ISO) standards
for variables and attributes sam-
pling for lot acceptance (8-10), and
there are also the National Institute
of Standards and Technology
(NIST) standards for determining
the sample size (11). SAS/JMP and
other statistical packages have their
own sample size and power cal-
culators. Every sampling protocol
involves risk. The risk should be
known rather than unknown.
To use a sample size calculator, the
confidence interval (1-alpha), the
power of the test, how reliably you
want to detect a change (1-beta), and
the practical change to observe (delta)
must be known. For example: alpha =
0.05, the power =0.95, and the delta
in pH that we want to detect is 0.2
and the standard deviation of pH at
the point of evaluation is 0.125 from
historical measurements. What is the
sample size? Eight samples will do
it. Sample size does not address sam-
pling method. Sampling method tells
you how to take the sample; sam-
ple size tells you how many. Power
curves are used when the delta is
unknown (see Figure 2).
Collect data per the sampling plan
Follow the sampling plan and col-
lect data and all associated data
tags (e.g., time, date, analyst, etc.)
during sampling.
Summarize data into statistics for
the sample and confidence inter-
vals for the population
Statistics and graphs are used to
summarize and aggregate the data.
The statistics describe the sample,
and the confidence intervals are
used to describe the population.
Confidence intervals control for
risk (95%, for example), varia-
tion in the data, and sample size.
Confidence intervals should be in
every graph and in every table.
Draw conclusions and inference
Based on the data and all associ-
ated confidence intervals, models,
and graphs, draw conclusions rela-
tive to acceptance criteria, limits,
CQAs, and the business case.
Verify conclusions, solve the prob-
lem, meet quality requirements,
and achieve the business case
Verify the conclusions and pre-
diction made from the sample
are subsequently observed in the
population. Demonstrate that
solutions are generally applica-
ble though on-going longitudi-
nal monitoring and continuous
validation protocols. Verification
Figure 2: Sample size and power curve.
Sample sizeOne mean
Difference to detect 0.2
Sample size 8
Power 0.95
Testing if one mean is different from
the hypothesized value.
Alpha 0.05
Std Dev 0.125
Extra Parameters 0
Supply two values to determine the
third.
Enter one value to see a plot of the
other two.
One mean
Sam
ple
siz
e
Difference
0.125
0.00 0.05 0.10 0.15 0.20
100
80
60
40
20
0
0.95 0.05
Sample size
PowerError
Std Dev Alpha
ES520996_BP1114_047.pgs 10.28.2014 23:15 ADV blackyellowmagentacyan

48 BioPharm International www.biopharminternational.com November 2014
Analytical Best Practices
indicates earlier estimates taken
from the representative sample
are correct. Failure to verify con-
clusions and inferences generally
indicates additional uncontrolled
factors are at play and need to
be understood and/or controlled
before the business case can be
achieved.
Summary
The ability to define a scientifi-
cally justified and statistically
sound sampling procedure is a
fundamental sk i l l in modern
systematic drug development. It
impacts every aspect of devel-
opment and validation. A struc-
tured approach using the key
considerations outlined in this
paper will aid in assuring it has
a defendable technical basis for
sampling method and sample
size selection and controls and
addresses risk relative to a clearly
def ined business cases, CQAs,
problem statements, and study
questions.
RefeRences 1. ICH, Q8 Pharmaceutical
Development (ICH, August 2009).
2. ICH, Q9 Quality Risk Management
(ICH, Nov. 9, 2005).
3. ICH, Q10 Pharmaceutical Quality
System (ICH, June 4, 2008)
4. ICH, Q11 Development and
Manufacture of Drug Substances
(Chemical Entities and
Biotechnological/Biological Entities)
(ICH, May 1, 2012).
5. ICH, Q8, Q9, and Q10 Questions and
Answers (R4) (ICH, November 2011).
6. WHO, Annex 4, WHO Guidelines for
Sampling of Pharmaceutical Products
and Related Materials (WHO, 2005).
7. FDA, Guidance for Industry, Process
Validation: General Principles and
Practices (January 2011).
8. ISO, ISO 10725, Acceptance
sampling plans and procedures for
the inspection of bulk materials
(ISO, 2000).
9. ISO, ISO 3951:1989, Sampling
procedures for inspection by
variables (ISO, 1989).
10. ISO, ISO 2859-1, Sampling
procedures for inspection by
attributes. Sampling schemes
indexed by acceptance quality limit
for lot-by-lot inspection (ISO, 1999).
11 NIST, “Sample Sizes Required,”
Engineering Statistics Handbook,
www.itl.nist.gov/div898/handbook/
prc/section2/prc222.htm, accessed
Oct. 16, 2014. ◆
Ad IndexCompany Page
AGILenT TecHnOLOGIes 51
BIO RAD LABORATORIes cover Tip
cAMBRIDGe HeALTH InsTITUTe 31
cATALenT PHARMA sOLUTIOns 52
eMD MILLIPORe 9
ePPenDORf nORTH AMeRIcA 7
eUROfIns LAncAsTeR LABORATORIes 17
fef cHeMIcAL 19
Ge HeALTHcARe LIfe scIences 5
LIfe TecHnOLOGIes 23
PfIZeR cenTResOURce 21
sAfc BIOscIences sIGMA ALDRIcH 15
sARTORIUs sTeDIM n AMeRIcA Inc 11
sGs LIfe scIence seRVIces 27
THeRMO fIsHeR scIenTIfIc 41
TOsOH BIOscIence 2
Verification
indicates earlier
estimates taken from
the representative
sample are correct.
ES523404_BP1114_048.pgs 10.30.2014 01:39 ADV blackyellowmagentacyan

November 2014 www.biopharminternational.com BioPharm International 49
SpotlightSpotlight
Tosoh Bioscience inTroduces
hydroxyapaTiTe resin
CaPure-HA was developed for the chromatographic separation of biomolecules. This resin has binding capacities of greater than 20 g/L for lysozyme at residence times as low as one minute and greater than 30 g/L for human IgG at residence
times as low as two minutes. CaPure-HA has been sintered at high temperatures for increased mechanical and chemical stability. Tosoh Bioscience, tel. 484.805.1219, www.tosohbioscience.com
insulin human aF
FeF Chemicals specializes in the supply of ingredients for the biopharmaceutical and pharmaceutical industries. We supply insulin for use in cell culture media from the largest manufacturer worldwide, Novo Nordisk.
Our Insulin Human AF product fulfils the definition for an animal-free product and is manufactured under cGMP compliance with the International Conference on Harmonization (ICH) Q7 guidelines and distributed from Denmark.
We provide consistent high quality and full traceability with multiple storage locations and a large safety stock, assuring guarantee of supply and flexibility in delivery options.
FeF Chemicals, tel. 0045 5667 1091, www.fefchemicals.com
sTarT imaging Fluorescence
WiThouT a darkroom
The ZOE™ Fluorescent Cell Imager is a complete digital imaging system that uses an intuitive touch-screen user interface to control brightfield, three fluorescence imaging channels,
and an integrated digital camera. Users can capture and store images and create multicolor merges with minimal training, and a light shield allows fluorescence imaging in ambient light. Bio-Rad
Laboratories, tel. 877.246.7231, www. bio-rad.com/info/zoe
neW agilenT
advanceBio rp-mab
columns
The only reversed-phase columns focused on the
unique challenges of mAb characterization. Superficially porous particles (3.5 µm) with wide pores (450Å) increase mAb resolution and provide shorter analysis times compared to fully porous particles. The robust Poroshell packed bed and 2 µm inlet frit extends column lifetime by preventing inlet blockage. A range of chemistries is available for flexible method development. Agilent Technologies, Inc., tel. 877.424.4536, www.agilent.com/chem/advancebio-RP
Cell Culture Consumables
Prevent Contamination
Eppendorf’s Cell Culture Consumables have an ISO class/GMP class C clean room production standard and a sterility assurance level of 10-6.
The flasks feature air filter technology, with improved ergonomic design to increase handling efficiency. Each flask is given a 100% in-line pressure test
for leaks. The resealable-top dishes include a corrugated ring to improve handling and transportation, with a SplashProtect ring inside the dish to protect against cross-contamination. The plates have been designed to minimize the “edge effect” with a chimney-well design in the outer moat of the 96-well plate.
Eppendorf
www.eppendorf.com
New Technology Showcase
ES518276_BP1114_049.pgs 10.24.2014 02:14 ADV blackyellowmagentacyan

50 BioPharm International www.biopharminternational.com November 2014
THE WORD
INDUSTRY BRIEFS
• FDA’s Dermatologic and Ophthalmic Drugs Advisory
Committee voted 7-0 to recommend approval of Novartis’
AIN457 (secukinumab) for the treatment of plaque pso-
riasis for patients who are candidates for systemic therapy
or phototherapy. The panel determined the drug was
highly efficacious and the 300 mg dose was determined to
provide the greatest benefit to patients. When compared
with Enbrel (etanercept) in a head-to-head trial last year,
secukinumab demonstrated significantly superior efficacy
over Enbrel in patients with moderate-to-severe plaque
psoriasis.
• Pall ForteBio announced the launch of a new solution
for quantifying contaminating residual host cell proteins
(HCPs) in Chinese hamster ovary (CHO) cells, the most
commonly used mammalian hosts for industrial produc-
tion of recombinant protein therapies. The new tool, the
Dip and Read Anti-CHO Host Cell Protein Detection Kit,
helps with the detection and reduction of residual HCPs
that are left behind by CHO cells. The residual products
can negatively affect the efficacy and safety of a final drug
product. The kit accelerates the drug delivery timeline by
providing better assay precision and complements Pall’s
ForteBio Octet Platform.
• FUJIFILM Diosynth Biotechnologies announced the
release of “Apollo,” a new technology solution for the man-
ufacture of therapeutic proteins. The platform, designed to
create a robust cell line to be used for preclinical material
through to commercial production, will feature a new
Chinese hamster ovary DG44-derived cell line, a novel
expression vector, a cell-line development process, and
optimized media and feed components. The Apollo plat-
form allows production of a representative material within
10 weeks of receiving a gene sequence and enables a clonal
cell line within 25 weeks from transfection. The expres-
sion system complements FUJIFILM’s pAVEway advanced
protein expression for microbial-based biopharmaceuticals.
• Many biopharmaceuticals such as antibody therapy
require subcutaneous injections or infusions for proper
absorption in the body. This type of administration is
usually required because, if taken orally, many of the
products become degraded in the stomach before uptake.
Researchers at the Massachusetts Institute of Technology
announced that they have devised a novel drug capsule
coated with tiny needles to deliver large-molecule biophar-
maceuticals. This drug-delivery method would effectively
prevent the breakdown of biologics in the stomach and
inject the drug payload directly into the lining of the gas-
trointestinal tract.
NEW FACILITIES
• Roche announced that it plans to expand its Basel
office complex to “bring it into line with modern effi-
ciency standards and building infrastructure require-
ments,” according to a press release from the company.
The multibillion-dollar investment will help to upgrade
existing infrastructure and will allow the site to satisfy
standards for energy consumption, safety, and GMP.
• IDT Biologika completed and certified the construction
of a large-scale production facility dedicated to filling
and lyophilization of biologics and vaccine products.
The fully integrated facility in Dessau, Germany, uses
a sterile liquid-filling line engineered to handle up to
24,000 vials per hour. Certified to biosafety levels 1
and 2 for live vaccines, the facility has been designed
and commissioned to be used for a range of advanced
biomedical technologies required in medium to large
clinical-stage and commercial-stage volumes.
MOST TWEETED
• How scientists are harnessing the power of modified T
cells to treat cancer. bit.ly/ZIjPzS
• Novartis announced positive results for secukinumab in
Ankylosing Spondylitis trials. bit.ly/ZP8rSS
• EMA encourages companies to apply for orphan-drug
status for Ebola treatments. bit.ly/1x1k3ge
EVENTS
2014 Lyophilization WeekDecember 1–4, 2014Bethesda, MD Risk-based Qualif cation of Sterile Drug Product Manufacturing SystemsDecember 8–10, 2014
Bethesda, MD
JOIN OUR ONLINE COMMUNITY
www.BioPharmInternational.com/LinkedIn
Twitter@BioPharmIntl
ES518361_BP1114_050.pgs 10.24.2014 02:32 ADV blackyellowmagentacyan

Limited time:Get a special deal on an Agilent A-Line Quick Connect Fitting
with your RP-mAb column at www.agilent.com/chem/advancebio_RP
BIG NEWS for scientists characterizing mAbs using reversed-phase
U/HPLC. The new AdvanceBio RP-mAb column uses Poroshell technology
to provide faster diffusion and higher resolving power for intact and reduced
mAb characterizations.
• BIG mAb resolution and speed – 3.5 µm particles with 450Å pore size
• Flexible method development with SB-C8, C4 and Diphenyl chemistries
• Assured reproducibility with Agilent manufacturing, end-to-end QC
ss
ss
ES524485_BP1114_CV3_FP.pgs 10.30.2014 22:28 ADV blackyellowmagentacyan

Every molecule has a challenge.
We have a smart biologics solution.
Call: + 1 888 SOLUTION (765-8846)
Email: [email protected]
Visit: www.catalent.com/biologics
smart biologics. integrated solutions. better treatments.
DEVELOPMENT DELIVERY SUPPLY
biologics
SPEED TO CLINICAccelerated development with one partner. Optimized cell line expression with GPEx‰ technology. Integrated analytical, fill/finish and clinical supply.
S
MORE PRODUCTS TO CLINICState-of-the-art clinical biomanufacturing facility.Innovative solutions for difficult-to-express proteins.Increased flexibility through single-use systems.
M
ADVANCED TECHNOLOGIESSMARTag™ technology for more efficacious ADCs. GPEx‰ and CAP‰ cell lines for biologics and biosimilar development. OptiGel Bio™ and ZydisBio™ technologies, plus glass-free injectable innovation with Advasept™ technology.
A
RIGHT THE FIRST TIMEHigher yields, stability and expression rates.More successful regulatory submissions.Reliable on-time delivery.
R
TRIED & TESTEDProven results with 400+ antibodies, 60+ recombinant proteins and a robust portfolio for biosimilar development. Established regulatory pathway with 25+ clinical trials across 6 continents.
T
As your strategic partner for
biologic development success, we
have the technology platforms and
integrated services to create smart,
tailored solutions that enable you
to get more products and better
treatments to clinic, faster.
ʺ 2
014
Cata
len
t P
harm
a S
olu
tio
ns.
All
rig
hts
rese
rved
.
CA
P is
a r
egis
tere
d t
radem
ark
of C
evec
Pharm
ace
utica
ls G
mbH
ES524452_BP1114_CV4_FP.pgs 10.30.2014 22:27 ADV blackyellowmagentacyan