Questions?Return to General/Principles IndexE-mail OTA about
Questions/CommentsIf you would like to volunteer as an author for
the Resident Slide Project or recommend updates to any of the
following slides, please send an e-mail to [email protected]
**Material Properties: fundamental behaviors of a substance
independent of its geometry.Structural Properties: the ability of
an object to resist bending under torsion, axial load, or bending
is a function of its shape and distribution of material around the
cross section.*Force applied to a body causes a deformation. If one
plots a graph of displacement due to the force applied to a
material, the slope of the curve represent the materials
stiffness.*Stress: is the force applied per unit area (F/A).Strain:
is the change in a materials length due to an applied stress
relative to its original length = L/ L0.*If one graphs the
resulting strain (L/ L0) due to the applied stress (F/A), the slope
of the Stress-Strain curve is the Elastic Modulus.*Review the
elastic modulus of common materials encountered in orthopaedic
surgery relative to each other.*Elastic Deformation: In the elastic
region, the relationship of displacement to the applied force in
linear. In this region, the material returns to its resting state
if the force is removed (elastic), like a rubber band.Stiffness:
again, is the slope of the elastic portion of the
force-displacement curve.Plastic Deformation: As more force is
applied, the materials behavior becomes plastic, and permanent
deformation occurs. The material will not return to its original
state after the force is removed (like when you bend a plastic ice
cream spoon to far it stays bent).Energy: The area under the curve
represents energy absorbed into the material during the deformation
process (work).*Stiffness: The steeper the slope, the stiffer the
material. A material with a flat slope is flexible.Yield Point: the
point on the force-displacement curve where the material changes
from elastic to plastic deformation is the yield point.Failure
Point: At some point the material will break; this point due is the
materials Failure Point.Brittle: a material which experiences
little plastic deformation before it fails is said to be brittle
(glass for example).Ductile: if a material with a large plastic
deformation region before it fails is said to be ductile (copper
for example).Toughness: a material which can absorb more energy
prior to failure (large area under the curve) is said to be
tougher.Weakness: a material which can absorb little energy prior
to failure (small area under the curve) is said to be weak.
*Compare the two types of failure: Load to Failure: Continuous
application of force until the material breaks (failure point at
the ultimate load). Bone usually fractures by load to
failure.Fatigue Failure: Cyclical sub-threshold loading may result
in failure due to fatigue.Load to failure testing often reported in
the orthopaedic literature: however, clinically, failure fracture
fixation constructs or implants often due to fatigue failure.
*Anisotropic: some materials (bone) have different mechanical
properties dependent upon the type of load applied (transverse,
longitudinal, shear).Viscoelastic: many biological materials to
include bone reveal different stress-strain curves depending upon
the speed at which the force is applied.*Bone is anisotropic-its
modulus is dependent upon the direction of loading. Bone is weakest
in shear, then tension, then compression. This can help us
understand the fracture produced (failure) from various mechanisms
(applied loads).Review the values of the Ultimate Stress at Failure
of cortical bone based upon the different direction of loading for
cortical bone.*Bone is viscoelastic, the force-deformation curve
will be different for different rates of loading.Trabecular bone
becomes stiffer in compression the faster it is loaded. It is
hypothesized that at high rates of loading the marrow elements do
not have time to be push out, and act like a fluid filled shock
absorber.*Bone, as a living material, can experience changes in its
density. Subtle density changes can have great effects upon the
material properties of the bone. Graph shows a marked change in the
stress/strain curve of trabecular bone when its density is
decreased by a factor of 3. These changes occur with normal aging,
disease, use and disuse.Figure from: Browner B., Jupiter J., Levine
A., Trafton P., Skeletal Trauma 2nd Edition, W.B. Saunders, 1998,
figure 4-5, pg. 101 *These bending, torsion, tensile and
compressive forces are applied to bones, and if excessive, may lead
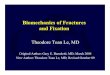
to fracture.*The nature of the applied force is often evident by
the nature of the fracture.Tension TransverseBending - Butterfly
Compression - Oblique Torsion - SpiralFigure from: Browner B.,
Jupiter J., Levine A., Trafton P., Skeletal Trauma 2nd Edition,
W.B. Saunders, 1998, figure 4-9, pg. 103.
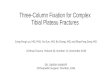
*As the bone is subjected to a bending load, one side is placed
under compression, the other is placed under tension. Since the
bones compressive strength is greater than its tensile strength,
the bone fails first on the tension side.Figure from: Tencer A.,
Johnson K., Biomechanics in Orthopaedic Trauma, J.P. Lippincott,
1994, figure 3.6 (a), (b), pg. 39.
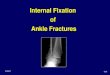
*TORSION: The diagonal in the direction of the applied force is
in tension cracks perpendicular to this tension diagonalSpiral
fracture 45 to the long axisFigures from: Tencer A., Johnson K.,
Biomechanics in Orthopaedic Trauma, J.P. Lippincott, 1994, figure
3.8 (a), pg. 41.
*Combined bending & axial loads result in oblique fractures
or those with a butterfly fragment.Figure from: Tencer A., Johnson
K., Biomechanics in Orthopaedic Trauma, J.P. Lippincott, 1994,
figure 3.7 (a), pg. 40.
*Resistance to bending, twisting, axial compression or tension
of an object is a function of its cross-sectional shape with
respect to a given axis. The relationship of resistance to applied
forces to the distribution of mass (shape) with respect to an axis
is related to the moment of inertia. These calculations based upon
the cross-sectional shape are useful in comparing the resistance to
applied forces of two different objects (solid vs. cannulated IM
nails, thin vs. thick cortical bone).Figure from: Browner B.,
Jupiter J., Levine A., Trafton P., Skeletal Trauma 2nd Edition,
W.B. Saunders, 1998, figure 4-6, pg. 101.
*Effect of fracture Callus: since the moment of inertia for a
cylindrical tube is proportional to r4 any small increase in the
radius by callus further away from the center greatly increases
moment of inertia therefore the stiffness of the structure.Figures
from: Browner B., Jupiter J., Levine A., Trafton P., Skeletal
Trauma 2nd Edition, W.B. Saunders, 1998, figure 4-6, pg. 101.Tencer
A., Johnson K., Biomechanics in Orthopaedic Trauma, J.P.
Lippincott, 1994, figure 4.6, pg. 62.
*Time of Healing: Callus increases with time, therefore the
stiffness increases with time. Near normal stiffness achieved at 27
days due to the callus formed further away from the axis. This
increased strength does not correspond to the radiographs.Figure
from: Browner B., Jupiter J., Levine A., Trafton P., Skeletal
Trauma 2nd Edition, W.B. Saunders, 1998, figure 4-15, pg. 109.
*Recall that for a cylindrical tube, the moment of inertia is
proportional to the radius to the 4th power. Small changes in the
radius can mean large changes in the stiffness.Figure from: Browner
B., Jupiter J., Levine A., Trafton P., Skeletal Trauma 2nd Edition,
W.B. Saunders, 1998, figure 4-6, pg. 101.
*IM Nail Diameter: As the diameter of the nail increases, so
does the torsional and bending moments of inertia (stiffness); a 16
mm nail is 2.5 x stiffer than a 12 mm nail. The large diameter can
accommodate larger holes for larger interlocking screws. The nail
size is limited by the diameter of the patients IM canal and the
amount of reaming performed. Figure from: Tencer A., Johnson K.,
Biomechanics in Orthopaedic Trauma, J.P. Lippincott, 1994, figure
9.21, pg. 263.
*SLOTTING: Placing a longitudinal slot in a nail makes the nail
moderately more flexible in bending (especially if slotted on the
compression side), and significantly more flexible in torsion. This
slot allows for radial compression of the nail during insertion
into the femur. The increased bending flexibility aids in allowing
an easier insertion and canal fit, but also decreases the fatigue
resistance of the nail (does not seem to be a clinical problem).
Figures from: Nail cross sections: Tencer A., Johnson K.,
Biomechanics in Orthopaedic Trauma, J.P. Lippincott, 1994, figure
9.20, pg 262.Stress diagrams: Rockwood and Greens 4th ed.
*Slotting-Torsion: A slotted nail is about 2% as stiff as an
intact femur in torsion, while a solid-section nail is about 50% as
stiff (Tencer, Tech Orthop 1988). Figures from: Bar graph: Tencer
A., Johnson K., Biomechanics in Orthopaedic Trauma, J.P.
Lippencott, 1994, figure 9.22, pg. 263.
*INTERLOCKING SCREWS: Control torsion and axial
loads.ADVANTAGES: The use of interlocking bolts expanded the use of
IM nails to more proximal, more distal, and unstable fractures
(highly comminuted, segmental), as well as adds rotational
stability with the non-reamed technique. DISADVANTAGES: Requires
some technical skill to place. The holes in the nail act as stress
risers (the weakest part of the nail to fatigue is at or just
proximal to the most proximal distal locking screw). There is an
increased rate of nail breakage if the fracture is within 5 cm of
these screws (Bucholz, JBJS 1987), or if the screw hole closest to
the fracture is left unfilled (Hahn, Injury 1996). LOCATION: Screw
holes closer to the end of the nail allow for the fixation of more
proximal or distal fractures, but at the expense of stability of
the construct. *Screw Anatomy: review screw terminology.Inner
diameter: the inner, core or root diameter determines the screws
strength.Outer diameter: the difference between the inner core
diameter and the outer diameter of the threads is the thread width.
Increasing the thread width increases the pull-out strength.Pitch:
threads per inch. Increasing pitch increases the pull out strength
of the screw.Figure from: Tencer A., Johnson K., Biomechanics in
Orthopaedic Trauma, J.P. Lippincott, 1994, figure 6.19 (a), pg.
133.
*Increasing the screws root diameter a factor of two allows it
to withstand torques eight times greater.The more volume of bone
caught between threads, the greater the pull out strength. This can
be achieved by increasing the thread width of the screw, or
increasing the number of threads in contact with the bone. Density
of the bone also affect pull out strength (young> than old bone,
cortical bone > cancellous bone).*Cannulated ScrewsIncreased
inner root diameter of a cannulated screw is large than a
comparable non-cannulated screw. This extra material is required to
compensate for the cannulation (mechanical effects of converting a
solid cylinder to a tube).This results in a relatively smaller
thread width and lower pull out strength.Figure from: Tencer A.,
Johnson K., Biomechanics in Orthopaedic Trauma, J.P. Lippincott,
1994, figure 6.30 (b), pg. 140.
*Bending stiffness proportional to the thickness of the plate to
the 3rd power, and directly to the elastic modulus. Therefore,
changing the plate thickness has more effect upon stiffness than
changing the material.This is expressed as the base (b) times the
height or thickness cubed over 12.*The primary function of the
plate is to maintain alignment as an internal splint, and to create
compression between the fracture ends such that bone can transfer
some of the applied loads itself. A compression plate, tension
band, or a lag screw does this by generating compression across the
fracture.In fixation constructs in which the plate-bone system can
carry load, the compressed fractured bone carries a major part of
the load. The bone, therefore, protects the implant (B.G. Weber).
*Unstable constructs: A construct in which compression cannot be
achieved across the fracture is unstable and at risk for failure.
Plates alone cannot tolerate the functional loads of a limb, and if
the fracture does not heal, the construct may eventually fail due
to fatigue under cyclical loading. This situation may be due
to:Severe comminution: consider bridge plating techniques.Bone
lossPoor quality bonePoor screw techniqueImproper choice of
implants*A gap at the fracture site such that there is no fracture
compression with applied loads allows bending or torsion of the
plate with the fulcrum at the level of the fracture. All of the
forces are transmitted through the plate alone instead of being
shared by the bone and the plate.*Fatigue Failure:Even stable
constructs may fail from fatigue if the fracture does not heal due
to biological reasons (infection, soft tissue loss, periosteal
stripping, smoking). The fracture surgeon must learn to balance the
desire for rigid fixation with the need to preserve the soft tissue
(biological fixation).
*Screw-Plate Relationship: When load is applied to the bone, a
portion of the load is transferred across the fracture line if the
construct allows compression. A portion of the load is also
transferred to the plate by bone-plate friction. A portion is
supported by the screw resisting bending and pull out.Lag Screw:
adding a compression lag screw across the fracture site greatly
increases the load transfer to the bone, further protecting the
screws and plate.
*The screws closest to the fracture see the most forces. The
screws further away experience progressively less force.The
construct rigidity decreases as the distance between the innermost
screws increases.A longer plate can increase the rigidity of the
construct.
*Through experience with failure the recommended strength of
plate and number of screws in each fragment has been determined.
These are general guidelines and more may be required with poor
quality bone. Anatomic constraints may limit also the construct.
Also it is important to note that the increased spread of screws is
more important than the number of screws (provided each screw has
equal purchase) for construct stability.
*It is uncertain how rigid an external fixation frame should be;
too rigid may be detrimental to fracture healing.*SIZE OF PINS:
RADIUS: Stiffness proportional to {radius}4, so small changes in
pin diameter greatly increases stiffness. **This is the most
significant factor affecting stability of the fixator. Larger pins
provide more rigid fixator, providing less bending stress at the
bone-pin interface and lower rate of loosening.However, the hole
size acts as a stress riser; if the pin diameter is greater than
30% the size of the bone the risk of fracture greatly increases
(McBroom, Orthop Res 88).
*NUMBER OF PINS:1] Two pins per fragment to prevent rotation,
usually in same plane.2] A third pin in the fragment adds slightly
to the resistance to bending and axial deviations, but little to
rigidity. A third pin does allow the subsequent removal of a loose
or infected pin without sacrificing the construct. *Deformation
perpendicular to the plane of two pins is best controlled with a
third pin in that perpendicular plane. A third pin (C) out of plane
of two other pins (A & B) stabilizes that segment.
*PIN LOCATION:1] Pin out of zone of injury if possible (avoid
infecting fracture):a] For stability, place pins as close to the
fracture site as possible (limited by anatomy and soft tissue
injury).b] For sterility place away location of incision for any
future, delayed ORIF, bone grafting, soft tissue coverage.2] More
stable if the second pin in a fragment is spread as far from the
first pin to best resist motion in the perpendicular plane.3] Wire
constructs most stable when at 90 to each other.
*PIN PRELOAD: BENDING PRELOAD: Previously thought that bending
(preloading) the pins would decrease pin loosening. However, the
pressure necrosis on the compression side of the pin leads to
earlier loosening (Hydahl, JOT 91).RADIAL PRELOAD: Can radial
preload the pin by using a pilot hole slightly smaller than the
pins root diameter or a tapered pin. This is thought to decrease
loosening and increase fixation. *BONE-FRAME DISTANCE: 1] ROD: The
closer the frame is to the bone the more stable is the construct.
Allow room for edema and wound care (2-3 cm).2] RING: Decreasing
the span that the wire travels increases the overall rigidity.3]
DYNAMIZATION: Can dynamize the frame easily by moving the rod
further away from the bone. *4In conventional plate fixation, as
the screws are tightened, and the screws displace the bone into
compression, a compressive force is generated between the plate and
the bone. This compressive force must be sufficient in order to
generate enough friction between the plate and the bone to maintain
stability of the fracture. As long as the resultant load from body
weight and muscles does not exceed what the frictional interface
can support, the construct will remain stable and prevent
collapse.*5Here is the initial stress in the bone due to tightening
(roughly 0). When the bone is loaded along the axes of the bone,
the bone around the screw is compressed on the load side of the
fracture. *7If we compare the stresses in the bone immediately
after implantation, the bone around the bi-cortical screws is
already stressed from tightening whereas the bone around the locked
screw is not subjected to any shear stresses. When the patient
starts to weight bear, the bone in the bi-cortical screws is more
highly stressed than the locked screws. *5Here is the initial
stress in the bone due to tightening. When the bone is loaded along
the axes of the bone, the bone around the screw is compressed on
the load side of the fracture. As the load is increased, and the
angle between the screw and the plate starts to change, the
resultant loading vector on the screw changes from pure compression
to a compressive and a tensile component. It is this additional
tensile component which, when the elastic limit of the bone is
exceeded, will cause toggling and eventual collapse across the
fracture gap.*Once the angular stability of one screw is lost [by
pulling thru 2nd cortex], the cycle begins and the inherent angular
stability of the construct is compromised.*Resistance of larger
area decreases this form of pullout. Rather the next form is
necessary [see next slide]. *Through experience with failure the
recommended strength of plate and number of screws in each fragment
has been determined. These are general guidelines and more may be
required with poor quality bone. Anatomic constraints may limit
also the construct. Also it is important to note that the increased
spread of screws is more important than the number of screws
(provided each screw has equal purchase) for construct
stability.
**Vorteil einer winkelstabilen Verschraubung*Mechanisch gesehen
entspricht das LIF einem Externen Fixateur, mit dem Vorteil, dass
er sehr nahe am Knochen liegt und dadurch stabiler ist. Es ist
jedoch wichtig, dass der Lngstrger (Platte), wie beim externen
Fixateur lange gewhlt wird******