Embed Size (px)
Citation preview

Acta of Bioengineering and Biomechanics Original paperVol. 18, No. 1, 2016 DOI: 10.5277/ABB-00248-2014-02
Biomechanical simulation of needle insertion into corneabased on distortion energy failure criterion
PENG SU, YANG YANG*, LEIYU ZHANG, LONG HUANG
Department of Mechanical Design and Automation, BeiHang University, Beijing, China.
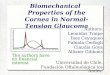
Purpose: This paper is mainly about biomechanical behavior of needle insertion into cornea, and proposes a failure criterion tosimulate the insertion process which has attracted considerable attention due to its importance for the minimally invasive treatment.Methods: In the process of needle insertion into cornea, tiny and complex insertion force is generated due to contact between needle andsoft tissue. Based on the distortion energy theory, there is proposed a failure criterion of corneal material that can solve contact problembetween rigid body and biological tissue in insertion simulation, where Cauchy stress of corneal material is the key to numerical calcula-tion. A finite element model of in vivo cornea is built, and the cornea constrained by sclera is simplified to two layers containing epithe-lium and stroma. Considering the hyper-viscoelastic property of corneal material, insertion simulation is carried out. Results: By insertionexperiment, the insertion force increases with insertion depth accompanying obvious fluctuations. Different insertion forces are gener-ated at different speeds. The punctured locations are obvious in the force-displacement curves. The results of insertion simulation aregenerally consistent with experimental data. Maps of von Mises stress reflect the tissue injury of the cornea during insertion process, andpunctured status corresponds to the point in the curves. Conclusions: The ability of this study to reproduce the behavior of needle inser-tion into cornea opens a promising perspective for the control of robotic surgery operation as well as the real-time simulation of cornealsuture surgery.
Key words: cornea, biomechanics, insertion force, suture, mathematical simulation
1. Introduction
The first step of suture surgery operation is theneedle insertion into soft tissue. Currently, physi-cians rely solely on tactile perception and tissue sur-face distortion to determine the progress of surgicalsutures. The judgement is subjective and cannot beused to control the robot-assisted surgery. Becausethere are many difficulties in the analysis of theinternal action of needle insertion into biologicaltissue, including deformation, relaxation, and pa-rameter settings in mathematical simulation, etc.,biomechanical study about the needle insertion intosoft tissue has become a bottleneck in the intersec-tion of medicine and mechanics, and it is also a ma-jor constraint of robotics development in the medicalfields.
Many scholars explored the biomechanics of nee-dle insertion into soft tissue, and pointed out that in-sertion force could be used for identifying tissue lay-ers as needle inserted into tissues [1]. Naturally,needle deflection and tissue deformation are majorproblems for accurate needle insertion. Roesthuis etal. [23] considered the needle to be a cantilever beamsupported by springs which have needle-tissue inter-action stiffness during an insertion. Van Gerwen et al.[27] proposed a law where insertion forces were af-fected by numerous factors, such as needle type, in-sertion speed, and tissue characteristics. Davis et al.[7] experimentally measured and theoretically mod-eled the force required to insert microneedles intoliving skin and the force needles can withstand beforefracturing, and the results provide the ability to predictinsertion and fracture forces. Although the cornea hasdifferent mechanical properties, insertion theories and
______________________________
* Corresponding author: Yang Yang, School of Mechanical Engineering and Automation, Beihang University, XueYuan RoadNo. 37, Hai Dian District, Beijing 100191, China. Phone number: +86 01082338386, e-mail: [email protected]
Received: December 5th, 2014Accepted for publication: April 14th, 2015

P. SU et al.66
modeling methods of these studies can serve as a use-ful reference for biomechanical study of needle inser-tion into cornea.
The insertion force distribution may be used forreal-time simulations of graphic location and tactilefeedback, and the numerical simulation can becomea valuable tool to plan ophthalmo-surgical procedures[25]. Marshall et al. [20] presented a suturing simula-tor for surgery operating on spring-mass surfacemeshes, and when the needle pierced the deformablemodel, the surface mesh was subdivided at the contactpoint using a novel subdivision algorithm. Di Maio etal. [8] developed a two-dimensional linear elastostaticmaterial model to quantify the needle forces and softtissue deformations. Similarly, Berkley et al. [4] havedeveloped a contact mechanism that applies con-straints to linear elastic models, and it emphasizeshigh model resolution, multipoint contact, rapid pre-processing, etc.
Main manipulator
End-effector
The needle insertion experiment
Auxiliary manipulator
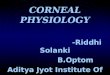
Fig. 1. The cornea-suturing robot. An end-effectorwith needle mounted on the main manipulator, and the first stepis the needle inserts into cornea in the corneal suture [30], [31]
Currently, most of the insertion studies focused onskin and internal organs, while the study is much lessin the field of corneal microsurgery that requires moreaccuracy and precision. In the previous study, we havedesigned a cornea-suturing robot that has a main ma-nipulator and an auxiliary manipulator, as shown inFig. 1. By comparing with the conventional manualsurgery, we found that robotic suturing has some ad-vantages: more stable suturing, smaller distortiontorque and fewer invasions to tissues [30], [31]. Therewere some key points that affected the success in con-ducting robot-assisted microsurgical suture, for exam-ple, the motion path of robot-end. If using the tradi-tional displacement control, the needle might causetissue damage due to a lack of force feedback fromrobot-end. However, surgery would be safer if therobot were controlled by references to the needle force
[1], [31]. Therefore, the study objective of this paperis to research biomechanical behavior of needle inser-tion into cornea that is an efficient reference to ensurethe success of robot-assisted surgery, and verify in-sertion modeling because it is one of the key tech-nologies to simulate the process of corneal surgery.
This paper proposes a distortion energy failurecriterion of corneal material in insertion simulation,and the element will lose carrying capacity if the con-dition of yield failure is met. Then insertion experi-mentation and simulation have been done to verify thefailure criterion. In the simulation, corneal materialproperties are accurately described by a hyper-visco-elastic corneal model deduced in the previous study[26], and a finite element model of the cornea simpli-fied to two layers containing epithelium and stroma isbuilt. Mesh elements of the insertion contact area arelocally refined in the finite element analysis to adaptto the distribution characteristics of calculation data.The results show that the failure criterion proposed iseffective in insertion simulation by comparisons withthe relationships between the insertion force and depthin experiment.
2. Materials and methods
2.1. Biological structureand material behavior
The cornea has the macroscopic structure of a thinshell in front wall of the eye. Assuming corneal sur-face is substantially spherical, it has a different thick-ness at each position, and pupillary zone is the thin-nest. In this paper, porcine cornea is taken as theresearch object, and geometric parameters of the cor-nea are shown in Table 1 [2], [9], [24].
Table 1. Corneal geometric parameters (mm) [2], [9], [24]
Parameter Value Parameter ValueAxial length 26.50 Horizontal diameter 11.20Corneal meanthickness 0.67 vertical diameter 11.00
Central thickness 0.55 Pericentral thickness 0.72
Peripheral thickness 1.00 Corneal anteriorradius 7.80
Corneal posteriorradius 6.80
At the micro level, the cornea is mainly composedof collagen fibrils embedded within a matrix of pro-teoglycans, and this construction leads to difficulties

Biomechanical simulation of needle insertion into cornea based on distortion energy failure criterion 67
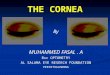
in understanding the material behaviour. The corneacan be divided into five layers, including epithelium,lamina elastica anterior, stroma, lamina elastica poste-rior, and endothelium, as seen in Fig. 2 [3], wherein,stroma is the main load-bearing part, accounting forabout 90% of the corneal thickness. The biomechani-cal properties of the cornea are primarily derived fromthe stroma [16]. Epithelium, located outermost layerof cornea, is generally considered to be a corneal bar-rier that is harder than the other layers, but it is onlya small contribution to the corneal tensile strength asit hardly bears the loads [13]. Lamina elastica anteriorhas no actually elasticity, which serves as the basis ofthe epithelium, and some scholars believe that it haslower contribution to the biomechanical properties ofcornea [9]. Lamina elastica posterior is a transparentfilm that is flexible and resistant, and it can buffer theeffect of IOP (i.e., Intra-ocular pressure) for cornea.Endothelium also hardly bears the load whose densityis consistent with epithelium.
Normally cornea is in a tensioned state, and itis difficult to quantitatively describe the cornealbiomechanical properties because there are manyfactors that can affect them, e.g., age, gender, andIOP, etc., [10], [11], [19] Besides, in the originaldata reported by different authors, some differencesbetween the sets of test results are observed becauseof different testing conditions or testing protocols[26]. Naturally, the results are consistent as to thescope and trend.
Stroma
Endothelium
Lamina elastica anterior
Lamina elastica posterior
12 mμ
500 mμ
10 12 mμ−
5 mμ
Epithelium35 55 mμ−
Fig. 2. Corneal micro-structure diagram [3]
Corneal material has two significant characteris-tics: hyperelastic and viscoelastic, and we have devel-oped a corneal model in the previous study [26].Firstly, the Mooney–Rivlin hyperelastic model ofcornea obtained based on stored-energy function canbe simplified as a linear equation with two unknownparameters. Then, modified Maxwell viscoelasticmodel of the cornea whose analytical form is consis-tent with the generalized Prony-series model is pro-posed from the perspective of material mechanics.
Parameters of the model are determined by the uniaxialtensile tests and the stress-relaxation tests.
The Mooney–Rivlin hyperelastic constitutive modelof the cornea may be described as
)3(20.11)3(59.10 21 −⋅−−⋅= IIW , (1)
where 132
1 IJI−
= and 234
2 IJI−
= represent the firstand second invariant of isochoric part C of the rightCauchy–Green deformation tensor C. The expansion
ratio 21
3IJ = represents volume ratio of deformation.I1, I2, and I3 are three basic invariants of tensor C.
The modified Maxwell viscoelastic model of thecornea may be described as
5/
4
1
)( EeEtG t
ii += −
=∑ τ , (2)
where Ei is relaxation modulus (unit: MPa), and τi isrelaxation time (unit: s), expressed by
)43.0,40.0,31.0,43.0,69.0(),,,,( 54321 =EEEEE
and
)1084.2,93.876,33.65,83.8(),,,( 34321 ×=ττττ .
The hyperelastic model and viscoelastic model ofthe cornea are established respectively. The hyper-elastic property of deformation-recovery and time-dependent viscoelastic property should be consideredat the same time under loading conditions. In general,it can be attributed to the non-linear hyper-viscoelasticproblem. It is a complex problem in the field of solidmechanics because the relationship between the de-formation rate and time rate is a series of energy con-version behavior.
2.2. Finite element model
According to the description above, a model ofneedle insertion into cornea can be established inABAQUS, as shown in Fig. 3 (a). Due to a smalldifference in the properties of the two orthogonaldirections, the corneal model simplified as an axi-symmetry one is verified by extrusion in vivo cornea[22], [26]. Many researchers have studied the corneaas a whole, but they did not indicate specific struc-tural layer relative to the measured biomechanicalparameters. It is necessary to distinguish the struc-tural layer on simulation because the layers of the

P. SU et al.68
cornea may affect the insertion force. Undoubtedly,stroma is essential in a simulation model. Epitheliumthat is the second thicker layer of the cornea after thestroma has a greater cell density, so it should be con-sidered in simulation model. Finally, other layers areso thin that we ignore their impact on the simulationresults. According to Table 1 and Fig. 2, cornealcentral thickness is 0.55 mm in the model wherestroma-thickness is 0.5 mm and epithelium-thicknessis assumed to be 0.067 mm.
X
Y
Stroma 0.5mm
Epithelium 0.067mm
0.2mm
2m
m 0
.5m
m
ConstraintNeedle
Sclera
Cornea
IOP=17.5mmHg
Insertion area
Contact areaSym
met
ry a
xis
Cornea
Needle
(a)
(b)
20º
0.01mm
Fig. 3. (a) The model of needle insertion into cornea,(b) meshing of local area
The material model is established based on cor-neal hyper-viscoelastic parameters above. The de-struction intensity of the cornea increases with age
[19], so it is difficult to determine a precise value ofthe failure stress. This paper found the predictionresults of numerical simulation were basically inagreement with experimental results when the failurestresses of epithelium and stroma are set to 10 MPaand 5 MPa which are estimates based on cornealbiomechanical study of laser in situ keratomileusis(LASIK) [12]. The lower hemisphere of the model ishinged constraints, and the needle, seen as a rigidbody, is constrained in the x direction, as shown inFig. 3 (a). In the previous study, the in vivo model ofthe cornea is validated by experiment and simulationof extrusion in vivo cornea [26]. Based on the actualstate of the eye, the cornea is constrained by sclerawhich is simplified as an elastomer, and materialbehaviors of the sclera can be described by elasticmodulus E = 3.08 MPa and Poisson’s ratio μ = 0.49[5]. It is an effective way to deal with constraintproblem of the cornea. Besides, the value of IOP is17.5 mmHg (i.e., 2.33 × 10–3 MPa), which is proveneffective value by extrusion simulation under differ-ent IOP.
Considering factors like computational accu-racy, efficiency, displacement coordination, andconvergence, etc., the model is divided into 16923mesh elements, where the element type is CAX4R,a 4-node bilinear axisymmetric quadrilateral in axi-symmetric stress family, element controls includereduced integration, distortion control, and enhancedhourglass control. In order to ensure accuracy of thecalculation, the meshes of corneal contact areashould be refined, wherein the insertion area is di-vided into 11683 mesh elements that accounts fornearly 70% of total elements in order to adapt to thedistribution characteristics of calculation data, asshown in Fig. 3 (b). During insertion, the contactsurface between the needle and corneal is changing,so surface-to-surface (explicit) contact is created,where needle is set to be the first surface and contactarea is the second surface. Interaction parameters areas follows: mechanical constraint formulation is pen-alty contact method, sliding formulation is finitesliding, and pressure-over closure normal behavior ofthe hard-contact. In addition, friction tangential be-havior of insertion cornea is related with the viscousof biological tissue, and it will change with insertionspeed. Based on the modified Kamopp friction model[21], Xuan et al. have established a friction modelthrough a series of sine loading tests, and when in-sertion speed ≥x 0.84 mm/s, the friction can begiven by [28]
xxxf 1171.0)sgn(371.0)( +−= . (3)

Biomechanical simulation of needle insertion into cornea based on distortion energy failure criterion 69
2.3. The distortion energyfailure criterion
In the finite element analysis, a failure criterionshould be set to control element deletion. There arethree common failure criterions: the maximum princi-pal strain, the maximum principal stress, and von-Mises stress failure criterion. The first two are mainlyused for failure analysis of brittle materials [14]. Be-sides, the von Mises stress criterion is widely used inpolymeric materials, such as strength and failureanalysis of plastics and rubber [15], [29].
The von Mises stress failure criterion, also knownas distortion energy failure criteria, originated in thedistortion energy theory (i.e., the fourth strength the-ory), and it is suitable for small strain. Based on therelationship of stress-strain in the previous study, themean value of corneal strain in the normal physiologi-cal stage is about 0.17 [26]. When the criterion is met,relevant elements of the model are damaged and inva-lid due to the loss of carrying capacity. In this paper,distortion energy theory was chosen as the failuretheory of needle insertion into cornea because of thesimilar material properties between cornea and otherhyperelastic materials.
Firstly, von Mises stress of corneal material shouldbe determined as it is the key to numerical calculation.Constitutive model (1) above may be represented as
,)1(1)3()3(
),,(
2201110
21
−+−+−=
=
JD
ICIC
JIIWW
(4)
where volume ratio J = det(F), and F is the materialdeformation gradient tensor (i.e., stretching tensor).
FJF 31
−= is the modified deformation gradient, and
there are three tensors: left Cauchy–Green tensorB = FFT, modified left Cauchy–Green tensor
BJFFB T 32
−== , and modified right Cauchy–Green
tensor .FFC T= B and C have the same charac-
teristic value, and 132
1 IJI−
= and 234
2 IJI−
= are in-variant tensors of the symmetric modified Cauchy–Green tensor [17]. There are partial derivatives
.2
and
),I(,I
1
132
21
−
−
=∂∂
−=∂∂
=∂∂
CJCJ
CIJCI
CI
(5)
According to the above definition, equation (5)can be further described as
.2
and
,31I)I(
,31I
1
111
34
2
11
32
1
−
−−
−−
=∂∂
⎟⎠⎞
⎜⎝⎛ −−=
∂∂
⎟⎠⎞
⎜⎝⎛ −=
∂∂
CJCJ
CICIJCI
CIJCI
(6)
There is a potential energy function W in hyper-elastic material, which is the potential energy of thesecond Piola–Kirchhoff stress tensor S, is given by
.22 2
2
1
1⎟⎟⎠
⎞⎜⎜⎝
⎛∂∂
∂∂
+∂∂
∂∂
+∂∂
∂∂
=∂∂
=CJ
JW
CI
IW
CI
IW
CWS (7)
According to equations (4) and (7), tensor S can bedescribed as
.)1(2
31
342
31I2
1
1111
34
01
11
32
10
−
−−
−−
−+
⎟⎠⎞
⎜⎝⎛ −−+
⎟⎠⎞
⎜⎝⎛ −=
JCJD
CCIIIIJC
CIJCS
(8)
The relationship between von Mises stress σ (i.e.,Cauchy stress) and stress S can be expressed by
TFSFJ1
=σ . (9)
Therefore, the expression of von Mises stress σ is
,)1(2
312
312
01
10
IJD
BBTTITBCJ
TIBCJ
−+
⎟⎠⎞
⎜⎝⎛ −−+
⎟⎠⎞
⎜⎝⎛ −=
34
σ
(10)
where T is the matrix trace of tensor C, i.e.,T = trace )(B . The expression (10) is the Cauchystress that can be applied to the material failure crite-rion.
Secondly, James Clerk Maxwell and Richard vonMises et al. specified von Mises criterion 100 yearsago, and some scholars have described that strain en-

P. SU et al.70
ergy density ρε consisted of volume change energydensity ρV and distortion energy density ρD in thestudy of mechanics of materials [18]. In the complexstress state, ρV and ρD are given by
].)()()[(6
1
,)(6
21
213
232
221
2321
σσσσσσμρ
σσσμρ
−+−+−+
=
++−
=
E
E
D
V
(11)
For calculating strain energy, the cornea is simpli-fied as an incompressible elastic material whose mate-rial parameters can be described by elastic modulusE = 1.8 MPa and Poisson’s ratio μ = 0.49 [6], [10].The expression of ρε can be rendered in the form
)].(2[21
13322123
22
21 σσσσσσμσσσρε ++−++=
E(12)
Distortion energy density is considered as the mainfactor causing material failure in the distortion energytheory. As long as the distortion energy density ρD
reaches its limit 0Dρ , the material is damaged [14],
20 ])([6
)1(2 σμρED+
= (13)
where [σ] is the limiting stress, i.e., breaking strength,which can be obtained by uniaxial tensile test. Theyield limit of material can be expressed as
0DD ρρ = . (14)
Therefore, defining state variable as δ, the yieldcondition can be expressed as
].[])()()[(21 2
132
322
21 σσσσσσσδ ≤−+−+−=
(15)
The material failure criterion of the cornea will bedefined using VUMAT, one of ABAQUS subroutines,and its implementation flowchart is shown in Fig. 4.In material integration points for each time increment,ABAQUS will call VUMAT to perform the calcula-tions about the material. The type of the variable δ isreal before comparing with [σ], and then it is defined asa constant to determine the state including Failure andNormal. If δ < [σ] in the calculation, state variable δ isdefined as 0 (i.e., δ = 0) that means the material isfailure. Otherwise, the material is normal when δ = 1.In the next time increment, the program will calculatethe next step if the initial state variable δ0 ≠ 0. The
parameters of different nonlinear model can be inputfrom the main program because the interface parame-ters have been set in VUMAT.
Normal
Material parameters
Interface parameters
VUMAT
Epithelium
Stroma
Material
ABAQUS
volume ratio J
Stretch tensor F
Deformation gradient
Left Cauchy-Green tensor
Mises stress
Bulk modulus Shear modulus
State variables
Strain increment
Stress increment
Failure
Breaking strength
Insertion layer
0G 0K
F
B
σ
δ
εΔ
σΔ
[ ]σ0δ = [ ]δ σ>
1δ =
0 0δ =
Normal
Section
Model
Assembly
Analysis step
Interaction
Boundary condition
Load Job
Output
Yes
Yes
No
No
Fig. 4. Implementation flowchartof the distortion energy failure criteria
2.4. Insertion experimentationand simulation
Because cornea is a very complex flexible body,the force is complicated in the process of needle in-sertion into cornea. The process can be divided intothree stages, including contact stage, trajection stageof needle-tip, and trajection stage of needle shaft, asshown in Fig. 5. Firstly, when the needle contacts withthe cornea, insertion force is surface contact force,i.e., stiffness force, generated due to the elasticity oftissue before cell units are damaged. After a steadyincrease, the force reaches a peak value. Secondly,when needle penetrates the top surface of cornea, theinsertion force shows sudden drop, and it is consti-tuted of the friction force and cutting force at trajec-tion stage of needle-tip. Finally, when the needlepenetrates the underside, entering the trajection stageof needle shaft, the insertion force is mainly consti-tuted by the friction force [1], [21].

Biomechanical simulation of needle insertion into cornea based on distortion energy failure criterion 71
(a)
(e)
(d)(c)
(b)
O A
B
Contact stage
Trajection stage of needle-tip
Trajection stage of needle shaft
Contact
Inserted top surface
Inserted underside
Fig. 5. The process of needle insertion into soft tissue,where O, A, and B are three critical conditions [21]
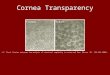
In order to study the insertion force, and providea judgment basis for the insertion simulation, experi-ments of needle insertion into cornea are done usingInstron 5848 Micro Tester, as seen in Fig. 6 (a). Consid-ering the accuracy of the data, insertion experimentsshould be carried out under the same condition that isconsistent with the previous experiments on cornealmaterial behavior [26]. The porcine eyes are slaughteredwithin eight hours. Measurement accuracy of the tester is±0.4% (load) and ±0.5 μm (displacement). The medicalneedle No. 2 is selected, 0.2 mm in diameter. In theexperiments, the needle is inserted into the cornea ata speed of 1 mm/s or 5 mm/s. In each insertion speed,10 eyeballs are used and vertical puncture is performedin each eyeball, as shown in Fig. 6 (b). Notably, IOPvalue of each eyeball is measured with a tonometerin the experiment. The eyeball should be injectedwith saline to make IOP value reach the ideal value(17.5 mmHg) when the measured value is less. The aimis to maintain the consistency of the internal pressure andremove a cause of experimental variability in the me-chanical response.
The process of needle insertion into cornea can besimulated, where the material failure criterion of thecornea is used for all mesh elements. When they reachthe failure distortion energy, they lose carrying capac-ity in the system, and this would be important to thedeformation gradient F. The failures of the elementsignore the volume loss that affect volume ratio J. Ap-plying insertion speed 1 mm/s and 5 mm/s at needle-end, the needle is inserted into the cornea, verticallydownward along the y-axis. Dynamic explicit step isset, where the simulation time is 0.7 s and the targettime increment is 2.0 × 10–5 s.
Workbench
Needle
Micro Tester
Eyeball
Cornea
Inst
ron
5848
Mic
ro T
este
r
(a) (b)
Fig. 6. (a) Instron 5848 Micro Tester;(b) A experiment of needle insertion into cornea
3. Results
Figure 7 shows insertion force-displacement curvewhen insertion speed v is 1 m/s, which is obtained by10 experiments. Analysing the mean value curve, theforce shows a stable upward trend with the insertiondepth, but there are two relatively distinct inflectionpoints shown as A and B points in the figure. Point Ais the puncture of the needle into entire cornea (i.e.,the punctured location), where the force will fluctuatesignificantly if the needle is inserted deeper. Consid-ering the position of point B, some reasons may causefluctuation of the force such as corneal deformation,tissue friction, etc. Symmetric error bar of standarddeviation shows statistical dispersion of 10 experi-mental data items in the insertion depth, and standarddeviation increases with the depth.
Fig. 7. Experimental data curve of insertion forcewhen insertion speed v is 1 m/s

P. SU et al.72
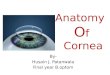
The force-displacement curves obtained in thesimulation are shown as curve a and b in Fig. 8, wherethe fitting curve a is given by third-order Gaussianinterpolation function F(x), shown in equation (15).Usually, the first drop is often used to signal thepuncture of the needle into the corneal top layer. Thecurve b is obtained by sample data, i.e., raw simula-tion result that can reflect small changes for insertionforce. So based on curve b, points C and D show epi-thelium and stroma has been punctured respectivelyconsidering the corneal model and corneal deforma-tion. Admittedly, there are some errors between aand c in Fig. 8 because the reality organisms alwayshave some factors that cannot be simulated, such aslocal deformation and unequal force. But trend andrange of insertion force data are generally the samebetween simulation and experiment. In addition,experimental result has an obvious hysteresis due totissue deformation that could lead to more friction.For example, considering the sudden drops of theforce on the curves and central thickness of the cor-nea in Table 1, the punctured position should be atabout 0.57 mm (near point E), which is smaller thanthe actual punctured position (point A). Undoubtedly,these puncture positions are of major importancewhen using the simulation for robot-surgery, we canmodify these differences according to the similartrend in practice. Statistics on the force of needle in-sertion into cornea are shown in Table 2, which con-sists of the mean value of experimental data and fit-ting value of simulation data at some insertiondisplacement.
]7.0,0[,exp)(23
1
∈⎟⎟
⎠
⎞
⎜⎜
⎝
⎛⎟⎟⎠
⎞⎜⎜⎝
⎛ −−=∑
=
xc
bxaxFi
i
ii (16)
where
⎥⎥⎥
⎦
⎤
⎢⎢⎢
⎣
⎡=
⎥⎥⎥
⎦
⎤
⎢⎢⎢
⎣
⎡
17.0,36.0,22.020.0,86.0,40.015.0,61.0,46.0
,,,,,,
333
222
111
cbacbacba
.
Besides, the comparison plot of different speedis shown in Fig. 9 (b). Comparing the curves at v =5 mm/s (curves d and e), the experimental results havesignificant fluctuations caused by the tissue defor-mation, and the punctured position in experiment(point A) is lagging relative to the simulation position(point E). Overall, higher insertion speed tends toincrease friction [27] and it is one of the reasons whyhigher speeds create greater interaction forces in theprocess. At the larger insertion speed, the fluctuationof simulation force is smaller than experimental force.
Obviously, the results of simulation are broadly con-sistent with experimental data at different speed.
Fig. 8. Insertion force-displacement curves when insertion speed vis 1 mm/s. a is the mean value curve of experimental data;b is the fitting curve of simulation results by equation (15);
c is the sample data curve of simulation results
Fig. 9. Insertion force-displacement curvesat different insertion speeds. a and b are the curvesshown in Fig. 8; d and e are the experimental curve
and simulation curve when insertion speed v is 5 mm/s
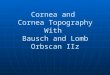
Maps of von Mises stress reflect the tissue injuryand deformation of the cornea during insertion proc-ess, as shown in Fig. 10, where figures (a), (b), (c),and (e) correspond to points O, C, D, and E of Fig. 8,respectively. Wherein, it is clearly seen from figure (c)that the boundary of two layers is due to differentfailure stresses. In figure (e), it can be consideredthat the whole cornea was punctured completely. Infigure (f), significant elastic deformation occurred atthe insertion position, whole cornea, and uncon-strained sclera.

Biomechanical simulation of needle insertion into cornea based on distortion energy failure criterion 73
Table 2. Statistics on the force of needle insertion into cornea,where experimental data is the mean value and simulation data is the fitting value
Insertion speed v is 1 m/s Insertion speed v is 5 m/sDisplacement(mm) Experimental
data (N)Simulation
data (N)Experimental
data (N)Simulation
data (N)0 0 0 0 0.02
0.05 0.01 0.01 0.02 0.030.1 0.03 0.02 0.06 0.05
0.15 0.06 0.05 0.10 0.090.2 0.09 0.09 0.15 0.13
0.25 0.12 0.15 0.22 0.190.3 0.18 0.20 0.30 0.26
0.35 0.24 0.24 0.31 0.340.4 0.22 0.26 0.38 0.41
0.45 0.26 0.31 0.15 0.490.5 0.36 0.38 0.55 0.57
0.55 0.44 0.48 0.58 0.630.6 0.51 0.56 0.64 0.62
0.65 0.62 0.57 0.60 0.530.7 0.63 0.53 0.64 0.55
(a) Mises stress at d=0mm
(b) Mises stress at d=7×10-2mm
(c) Mises stress at d=0.12mm
(d) Mises stress at d=0.16mm
(e) Mises stress at d=0.57mm
(f) Mises stress at d=0.7mm
Epithelium
Stroma
Deformation
S.Mises+ 9.785+ 8.970+ 8.154+ 7.339+ 6.532+ 5.708+ 4.893+ 4.077+ 3.262+ 2.446+ 1.631+ 8.154×10-1
+ 2.262×10-8
S.Mises+ 8.787+ 8.054+ 7.322+ 6.590+ 5.858+ 5.125+ 4.393+ 3.661+ 2.929+ 2.197+ 1.464+ 7.322×10-2
+ 2.311×10-8
S.Mises+ 9.566+ 8.769+ 7.972+ 7.174+ 6.377+ 5.580+ 4.783+ 3.986+ 3.189+ 2.191+ 1.594+ 7.972×10-1
+ 2.472×10-9
S.Mises+ 0+ 0+ 0+ 0+ 0+ 0+ 0+ 0+ 0+ 0+ 0+ 0+ 0
S.Mises+ 9.974+ 9.143+ 8.311+ 7.480+ 6.649+ 5.818+ 4.987+ 4.156+ 3.325+ 2.493+ 1.662+ 8.311×10-1
+ 1.627×10-11
S.Mises+ 9.495+ 8.704+ 7.913+ 7.122+ 6.330+ 5.539+ 4.748+ 3.956+ 3.165+ 2.374+ 1.583+ 7.322×10-1
+ 8.701×10-10
Deformation
Fig. 10. Maps of von Mises stress for insertion simulation when insertion speed is 1 mm/s, where d is insertion depth.(a) corneal pre-deformed status; (b) corneal epithelium has been punctured; (c) the stroma has been punctured; (d) punctured status
of stroma at d = 0.16 mm; (e) the lower surface of the cornea has been punctured; (f) broken status of the cornea at d = 0.7 mm

P. SU et al.74
4. Discussion
The process of needle insertion into cornea isa complex nonlinear problem including material non-linearity, geometric nonlinearity and boundary non-linearity. In the process, the insertion force, an im-portant parameter, would be generated owing to theinteractions between rigid body and viscoelastic ob-ject, which could be used to determine insertion depth.Although the force has been measured in previousreports [21], [31], biomechanical simulation of theprocess has not achieved the desired results due to thecomplexity.
Many scholars have done a lot of works in meas-urement of corneal biomechanical properties, but theproperties of cornea are different under differentphysiological conditions or test specifications [10].The previous study describes a corneal constitutivemodel that is a relatively simple material model in-cluding hyperelastic and viscoelastic ones [26]. It isimportant to ensure the authenticity and validity ofinsertion simulation. Material parameters of themodel, obtained by uniaxial tensile test and stressrelaxation test, are broadly in line with the results ofprevious publication, even though there are some dif-ferences in the accurate results due to different testingconditions.
Although some scholars had studied microscopicstructure of the cornea [3], few distinguished struc-tural layer during insertion simulation of the cornea.In this paper, the cornea is divided into two structurallayers including epithelium and stroma accordingto corneal structures and biomechanical properties.The idea to distinguish structural layer is the first tobe applied to insertion simulation of the cornea. Asa cell-based membrane, epithelium is believed to offera larger hardness to needle puncture. The cornea isconfined by external tissues, which contribute to theinternal stress and to the actual configuration of thecornea, where there is close association between cor-nea and sclera, and they together constitute the outerwall of the eye. On this basis, corneal constraint isconsidered in finite element model.
Insertion force-displacement curves are obtainedbased on experiment of needle insertion into cornea.Analyzing the curves, we found that the force is non-linearly increasing with the insertion depth before thecornea was punctured completely, and there is fluc-tuation of force caused by tissue deformation. Whenthe eyeball is extracted from the body, the confine-ment disappears and this leads to an “expansion” ofthe eyeball because a confinement is missing, and the
IOP is reduced correspondingly. Although it cannotcompensate the expansion of the eye, IOP value is tomaintain the ideal value (i.e., 17.5 mmHg) by inject-ing saline to the eyeball in order to ensure the consis-tency and remove experimental variability in the me-chanical response.
Finally, applying the distortion energy failurecriterion of corneal material, the process of needleinsertion into cornea is simulated in ABAQUS. Ac-cording to the relationship between the insertionforce and depth, obtained by simulation, we couldfind that the larger insertion speed tends to increaseinsertion force and decrease fluctuation of the force.Although the simulation describes the biomechanicalbehavior in ideal conditions, the correctness of thesimulation is verified by comparisons with the ex-perimental results.
Admittedly, there are some limits and drawbacksabout the approach. For example, the paper studies theinsertion force, but it can be subdivided as a summa-tion of stiffness, friction, and cutting forces to obtainmore accurate results [21]. The final structural modelof the corneal shell which is a simplification is in dis-cord with the theoretically advanced description, soa more accurate model with the physical nonlinearityshould be built as the technology improves. Besides,porcine corneas are taken as the test subjects due tothe difficulty in obtaining human ones, but they can-not completely substitute human ones because of dif-ferent mechanical behaviors [6], [11].
We are evaluating the possibility of performingthe surgery of robot-assisted corneal suturing basedon the results from this study. With further biome-chanical research we will explore the indicators ofthe force feedback which can be used to determinethe progress of robot-assisted surgery, and explorethe ways to implement real-time simulation of cor-neal suture surgery combining robotics and finiteelement methods.
Acknowledgement
The author wishes to thank the Natural Science Foundation ofChina (Grant No. 50675008 and Grant No. 51175013) that sup-ported this work.
References
[1] ABOLHASSANI N., PATEL R., MOALLEM M., Needle insertioninto soft tissue: A survey, Med. Eeg. Phys., 2007, 29(4),413–431.
[2] ALTMAN D.A., HOETZEL D.A., BUZARD K., CHOE K., Stripextensiometry for comparison of the mechanical response ofbovine, rabbit and human corneas, J. Biomech. Eng., 1992,114(2), 202–215.

Biomechanical simulation of needle insertion into cornea based on distortion energy failure criterion 75
[3] ANDERSON K., EL-SHEIKH A., NEWSON T., Application ofstructural analysis to the mechanical behaviour of the cor-nea, J. R. Soc. Interface, 2004, 1(1), 3–15.
[4] BERKLEY J., TURKIYYAH G., BERG D., GANTER M.,WEGHORST S., Real-time finite element modeling for surgerysimulation: An application to virtual suturing, IEEE T. Vis.Comput. Gr., 2004, 10(3), 314–325.
[5] BISPLINGHOFF J.A., MC-NALLY C., MANOOGIAN S.J., DUMA S.M.,Dynamic material properties of the human sclera, J. Biomech.,2009, 42(10), 1493–1497.
[6] BOSCHETTI F., TRIACCA V., SPINELLI L., PANDOLFI A.. Mechani-cal characterization of porcine corneas, J. Biomech. Eng.,2012, 134(3), 031003.
[7] DAVIS S.P., LANDIS B.J., ADAMS Z.H., ALLEN M.G., PrausnitzMR. Insertion of microneedles into skin: measurement andprediction of insertion force and needle fracture force,J. Biomech., 2004, 37, 1155–1163.
[8] DIMAIO S.P., SALCUDEAN S.E., Needle insertion modelingand simulation, IEEE Trans. Robot. and Autom., 2003,19(5), 864–875.
[9] EHLERS N., HJORTDAL J., Corneal thickness: measurementand implications, Exp. Eye. Res., 2004, 78(3), 543–548.
[10] ELSHEIKH A., ALHASSO D., RAMA P., Biomechanical proper-ties of human and porcine corneas, Exp. Eye. Res., 2008,86(5), 783–790.
[11] ELSHEIKH A., KASSEM W., JONES S.W., Strain-rate sensitiv-ity of porcine and ovine corneas, Acta Bioeng. Biomech.,2011, 13(2), 25–36.
[12] FANG X., XU Y., Corneal stress-strain relation and struc-tural equation of porcine eye after LASIK, Int. J. Ophthal-mol., 2006, 6(6).
[13] FRATZL P., MISOF K., ZIZAK I., RAPP G., AMENITSCH H.,BERNSTORFF S., Fibrillar structure and mechanical proper-ties of collagen, J. Struct. Biol., 1998, 122(1), 119–122.
[14] GERE J.M., GOODNO B.J., Mechanics of Materials, CengageLearning, 2009.
[15] GENT A.N., Engineering with rubber: how to design rubbercomponents, Carl Hanser Verlag GmbH Co., KG, 2012.
[16] HATAMI-MARBINI H., Viscoelastic shear properties of thecorneal stroma, J. Biomech., 2014, 47(3), 723–728.
[17] HOLZAPFEL G.A., Nonlinear solid mechanics, Chichester,Wiley, 2000.
[18] JONES R.M., Mechanics of composite materials, CRC Press,1998.
[19] LI L., TIGHE B., The anisotropic material constitutivemodels for the human cornea, J. Struct. Biol., 2006,153(3), 223–230.
[20] MARSHALL P., PAYANDEH S., DILL J., Suturing for surfacemeshes, CCA, 2005, 31–36.
[21] OKAMURA A.M., SIMONE C., O'LEARY M.D., Force modelingfor needle insertion into soft tissue. IEEE Trans. Biomed.Eng., 2004, 51(10), 1707–1716.
[22] PANDOLFI A., MANGANIELLO F., A model for the humancornea: constitutive formulation and numerical analysis,Biomech. Model. Mechan., 2006, 5(4), 237–246.
[23] ROESTHUIS R.J., VAN-VEEN Y.R., JAHYA A., MISRA S.,Mechanics of needle-tissue interaction, IROS, 2011,2557–2563.
[24] STITZEL J.D., DUMA S.M., CORMIER J.M., HERRING I.P.,A nonlinear finite element model of the eye with experimentalvalidation for the prediction of globe rupture, Stapp carCrash Journal, 2002, 46, 81–102.
[25] STUDER H.P., RIEDWYL H., AMSTUTZ C.A., HANSON J.V.,BUCHLER P., Patient-specific finite-element simulation of thehuman cornea: A clinical validation study on cataract sur-gery, J. Biomech., 2013, 46(4), 751–758.
[26] SU P., YANG Y., XIAO J., SONG Y., Corneal Hyper-viscoelastic Model: Derivations, Experiments, and Simula-tions, Acta Bioeng. Biomech., 2015, 17(2), 73–84.
[27] VAN-GERWEN D.J., DANKELMAN J., VAN-DEN-DOBBELSTEENJ.J., Needle–tissue interaction forces – A survey of experi-mental data, Med. Eng. Phys., 2012, 34(6), 665–680.
[28] XUAN X., YANG Y., WANG Z., DENG S., LIU X., Force modelingfor needle insertion into corneal tissue, Chinese High Tech-nology Letters, 2009, (9), 951–956.
[29] YAN J., STRENKOWSKI J.S., A finite element analysis of or-thogonal rubber cutting, J. Mater. Process. Tech., 2006,174(1), 102–108.
[30] YANG Y., LIU X., FU H., Finite Element Simulation of NeedleInsertion into Cornea, Chin. J. Mech. Eng., 2008, 44(12),24–29.
[31] YANG Y., XU C., DENG S., XIAO J., Insertion force in manualand robotic corneal suturing, Int. J. Med. Robot. Comp.,2012, 8(1), 25–33.