Embed Size (px)
Citation preview
![Page 1: Biomechanical Evaluation of AxiaLIF as Supplemental Hardware … · treating degenerative disc disease, instability and adult degenerative scoliosis [2]. The AxiaLIF¨ hardware, consisting](https://reader034.pdfslide.us/reader034/viewer/2022051604/600570bcfdb4a53ba20badc5/html5/thumbnails/1.jpg)
BIOMECHANICAL EVALUATION OF AXIALIF® AS SUPPLEMENTAL HARDWARE IN LONG FUSION CONSTRUCTS
+1Scheer, J.K.; 1Mulkerin W.; 1Nguyen, T.Q.; 1Tia, S.; 1Lotz, J.C.; 1Ames, C.; 1Buckley, J.M.; 1Burch, S. +1University of California at San Francisco, San Francisco, CA
[email protected] INTRODUCTION
The current practice in deformity surgery is to protect the inferior screws in long posterior fusion constructs by extending the fixation to the ilium or performing transforaminal and anterior lumbar interbody fusions (TLIF and ALIF, respectively) [1]. While these approaches lessen the potential for screw loosening, fracture, or non-union, they are associated with higher patient morbidity due to prolonged exposure (TLIF) or staged surgery (ALIF). AxiaLIF® (TranS1®) utilizes a novel percutaneous, presacral technique to access the L5/S1 disc space. Further, this novel technique has demonstrated successful clinical results treating degenerative disc disease, instability and adult degenerative scoliosis [2]. The AxiaLIF® hardware, consisting of a single threaded screw, can be inserted in the same operative setting as the original posterior fixation, thus minimizing exposure time and eliminating the need for patient repositioning [2]. The goal of this study is to determine whether it is biomechanically advantageous to use AxiaLIF® as supplemental anterior fixation in long fusion constructs. Bending rigidity will be quantified for constructs with and without AxiaLIF® terminating at the sacrum as well as the ilium. The efficacy of the device as a function of donor bone mineral density (BMD) will also be considered.
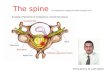
Figure 1: (left) Posterior screw-rod fusion with fixation to the ilium. (right) A lateral x-ray showing AxiaLIF® used as supplemental fixation at L5-S1 in a long fusion construct. Both images correspond to test specimens used in this study.
METHODS Intact lumbosacral spines with attached pelvis (N=6, L1-S1) were
harvested from fresh human cadavers (F=4, M=2; 54 ± 7 y.o.). BMD was assessed via standard dual x-ray absorptiometry (DEXA) lumbar scans (Hologic QDR). Planar x-ray scans (Philips BV Pulsera) were taken to exclude specimens with deformities or bridging osteophytes. Four sequential surgical treatments were applied to each specimen by a trained surgeon: 1) bilateral posterior rods with pedicle screws from L1-S1 (6.35mm Stainless Steel rods, 6.5x40mm pedicle screws, Medtronic), 2) extension of the posterior fusion to the ilium (7.5x70mm, Medtronic), 3) AxiaLIF® at L5-S1 with L1-S1 posterior fusion, and 4) AxialLIF® at L5-S1 with L1-ilium fusion.
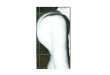
Figure 2: (left) Biomechanical test set-up for flexion testing of lumbosacral spines, (left) anterior view and (right) posterior view.
For each surgical configuration, specimens were tested non-destructively in flexion using a validated, cable-driven pure moment apparatus [3] (Figure 2, left) affixed to an industrial hydraulic press (Mini-Bionix 858, MTS). Prior to testing, the entire L1 vertebra and the superior ends of the two posterior rods were potted in quick-set resin (SmoothCast). This was done to simulate the rigidity of a long fusion
construct superior to L1. During testing, the pelvis was held in a custom-built three-point fixation clamp (Figure 2, right) that secured the pelvis while permitting unconstrained motion of the sacroiliac joint. Motion tracking targets were rigidly attached to L5 and S1, and these were used to monitor relative motion across that joint (Optotrak 3020, Northern Digital). In accordance with a standard protocol [4], bending tests consisted of preconditioning for 10 cycles between 2-7 Nm followed by one non-destructive loading cycle to 7.0 Nm. Maximum relative flexion across L5-S1 at 7.0 Nm was taken as the metric of interest for comparison across treatment groups. RESULTS
The efficacy of the AxiaLIF® device in preventing motion at L5/S1 was dependent on BMD (Figure 2). For normal to moderately osteopenic specimens (DEXA T-score > -2.0), maximum L5/S1 flexion angles decreased with addition of the AxiaLIF® hardware for both the L1-Sacrum and L1-Ilium constructs (mean 33% and 25%, respectively). L5/S1 motion with AxiaLIF® was slightly greater than L1-Ilium fixation alone for all normal/osteopenic specimens (0.25±0.18 degrees). Two specimens, one severely osteopenic (T-score = -2.3) and one osteoporotic (T-score = -2.6), showed increased flexion at L5/S1 with the addition of the AxiaLIF® device. This increase was more severe for L1-Sacrum fixation (approx. 0.4 & 0.8 degrees) than L1-Ilium fixation (approx. 0.1-0.2 degrees).
Figure 3: (left) Maximum flexion angle at L5-S1 for different surgical configurations for one normal (BMD = -0.4) and one severely osteoporotic specimen (BMD = -2.5). Error bars represent ±0.1 degree precision of motion tracking system [5]. (right) Change in maximum relative flexion across L5-S1 with AxiaLIF® as supplemental anterior fixation. CONCLUSIONS
The results of this study suggest that AxiaLIF® provides additional rigidity at the caudal base of long fusion constructs in individuals with normal bone mineral density. For a L1-Sacrum posterior screw-rod fusion, extension of the fusion to the ilium is on average more rigid than the addition of AxiaLIF®; however, the small difference in stability (approx. 0.3 degrees at L5/S1) between the two techniques may be outweighed by the lower morbidity associated with the AxiaLIF® product due to a compromise in bone integrity. For low bone density individuals, our data suggest that AxiaLIF® may actually destabilize caudal end of the long fusion construct. We hypothesize that this is caused by the inability of the relatively weak bone in the trabecular centrum to prevent migration of the AxiaLIF® device during forward flexion. Currently, the AxiaLIF® device is approved for use in patients with a Z Score > -1.5 with multiple published clinical studies demonstrating successful outcomes with respect to fusion incorporation and pain relief [2,6,7]. Future work will investigate the mechanisms by which the AxiaLIF® device fails to prevent motion at L5/S1 in osteoporotic bone, with research focused on improved fixation techniques. ACKNOWLEDGEMENTS Funding provided by TranS1 Medical, Inc. The authors thank Mr. Marshall Fong for his technical assistance. REFERENCES [1] Mummaneni PV, J Neurosurg Spine, 2004; [2] Ames CP, Minim Invasive Neurosurg. 2008; [3] Eguizabal J, SAS 2008; [4] Crawford Spine 1995; [5] Bozkus H, Spine 2004. [6] Anand 2008 SRS/IMAST; [7] Anand 2008 SRS/IMAST
Poster No. 1765 • 55th Annual Meeting of the Orthopaedic Research Society