-
8/12/2019 Biomechanical Changes Associated With the
Osteoarthritic, Arthrodesed,
1/6
Review
Biomechanical changes associated with the osteoarthritic,
arthrodesed,
and prosthetic ankle joint
Tristan Barton *, Francois Lintz, Ian Winson
Department of Trauma and Orthopaedics, Avon Orthopaedic Centre,
Southmead Hospital, Bristol, United Kingdom
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 52
2. Spatialtemporal factors . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . 53
3. Ankle joint kinematics. . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . 53
4. Ankle joint kinetics . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . 55
5. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . 55
6. Future directions . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . 56
References . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . 56
1. Introduction
Degenerative joint disease of the ankle can result in loss
of
function as a consequence of pain, stiffness and deformity[1].
This
disease process can result in significant alterations not only
to the
biomechanics of the ankle joint, but to the foot and ankle
complex
as a whole. Analysis of the kinematics and kinetics of gait
helps to
improve our understanding of the biomechanics of the foot
andankle. As the technology and accuracy of gait analysis continues
to
develop, the importance of addressing the foot and ankle
complex
as a functional unit becomes increasingly apparent in order
to
successfully treat foot and ankle pathology [2].
It is now recognised thatit is inappropriate
toconsiderthefootas
a simple lever at the distal end of the tibia. Multi-segment
models
have been designed in an attempt to isolate the kinematics of
the
individual joints within thefoot andanklecomplex
[35].Anymodel
will however remain an over-simplification due to the vast
number
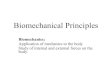
of articulations within the foot and ankle. Current motion
analysis
aims to group such articulating units into segments, with
skin
markersindicating the boundaries of each segment (Fig.1). The
four
segment models enable the movements of the hind-foot,
mid-foot
and forefoot to be measured relativeto thetibia in three
dimensions
and are producing more accurate modelling of foot and
anklekinematics. Such techniques have the benefit of being
non-invasive,
but do have a number of limitations. Firstly, as mentioned
above,
each foot segment is a composed of a number of articulations
and
therefore the individual influence of the each joint cannot not
be
defined. This is of particular relevance in the hindfoot, with
respect
to ankle and subtalar joint kinematics. A further problem is
that
utilising skin markers. Such markers are placed over the
bony
landmarks they represent during motion analysis. Relative
move-
ments of thefour segments aresmall,and anyinaccuracies in
marker
placement or marker movement relative to the underlying bony
structures will influence the overall analysis.
Foot and Ankle Surgery 17 (2011) 5257
A R T I C L E I N F O
Article history:
Received 26 October 2010
Received in revised form 23 December 2010Accepted 13 January
2011
Keywords:
Biomechanics
Kinematics
Kinetics
Ankle arthrodesis
Ankle replacement
* Corresponding author. Tel.: +44 7970 470533.
E-mail address: [email protected](T. Barton).
Contents lists available at ScienceDirect
Foot and Ankle Surgery
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m
/ l o c a t e / f a s
1268-7731/$ see front matter. Crown Copyright 2011 Eurpoean Foot
and Ankle Society. Published by Elsevier Ltd. All rights
reserved.
doi:10.1016/j.fas.2011.01.010
http://dx.doi.org/10.1016/j.fas.2011.01.010mailto:[email protected]://www.sciencedirect.com/science/journal/12687731http://dx.doi.org/10.1016/j.fas.2011.01.010http://dx.doi.org/10.1016/j.fas.2011.01.010http://www.sciencedirect.com/science/journal/12687731mailto:[email protected]://dx.doi.org/10.1016/j.fas.2011.01.010
-
8/12/2019 Biomechanical Changes Associated With the
Osteoarthritic, Arthrodesed,
2/6
More accurate modelling is achieved utilising methods such
as
invasive in vivo techniques and dynamic testing of cadaveric
specimens. Invasive testing using intra-cortical pins
certainly
provides more accurate data than utilising skin markers and
also
allows assessment of talar motion[6]. This technique is limited
by
surgical access to certain aspects of the foot, and the
question
remains as to whether the foot behaves normally when gait is
analysed with pins in situ. Studies do suggest that such
methods
are valid, and pre- and post-pin insertion pressure studies do
show
relative normality of gait despite the presence of
intra-cortical
pins[7]. Dynamic assessment of cadaveric specimens does
allow
access to all aspects of the foot and ankle complex and has
the
benefit of enabling assessment of movement both of
thearticulations and the soft tissues [811]. In vitro loading of
the
foot and ankle complex is unlikely however to accurately
re-create
in vivo gait and loading patterns.
Further tools for the assessment of foot and ankle
kinematics
utilise fluoroscopic and magnetic resonance imaging [12,14].
These techniques produce three-dimensional images of the
foot
and ankle complex in weight-bearing subjects and enables
motion
at individual jointsto be quantified. Using this technique,
magnetic
resonance images produces more accurate data, however the
stages of gait can only be reproduced in a static form.
Fluoroscopic
imaging allows dynamic analysis of the gait cycle, but the
data
obtained is less accurate than that obtained utilising
magnetic
resonance imaging.
These developments in the assessment of foot and
anklebiomechanics are enabling an improved understanding of the
kinematic and kinetic changes that occur in the diseased
ankle
joint. In addition, the effect of surgical treatments of foot
and ankle
pathology can now be studied from a biomechanical
perspective
and help guide future developments [15]. This is of
increasing
relevance in the treatment of degenerative changes within
the
ankle joint where traditionally ankle arthrodesis has provided
the
most reliable outcome in the operative treatment of
symptomatic
ankle arthritis. With continuing improvements in both the
understanding of the biomechanics and the technology of the
implants, the number of ankle replacements performed is
steadily
increasing. The outcome following ankle replacement is
improving
with respect to both revision rates and functional scores
[1619],
but the key to the continuing improvement in implant longevity
is
likely to be in the stable fixation of the prosthesis within a
well
balanced foot and ankle complex. Recent biomechanical
studies
suggest that if the prosthesis is misaligned, polyethylene wear
and
implant survival is likely to be compromised[2022].
2. Spatialtemporal factors
A painful ankle joint results in changes to both the pattern
and
velocity of gait. The majority of studies report both cadence
(steps/
minute) and stride length to be reduced,with patients
spendingless
time on the affected limb in stance[2325]. The overall effect
of
these changes is a reduction in walking speed with an
asymmetric
gait and resultant limp. This is likely to represent a
protective
mechanism in order to reduce the load passing across the
diseased
joint[26]. Interestingly,Dyrbyet al.foundcadenceto be
significantly
increased in patients witharthriticankles compared
withunaffected
controls, but this increase was not sufficient to normalise
walking
speed due to the reduced stride length[27].
Following ankle arthrodesis, there is a significant
improvement
in walking speed[2832]. This however does remain
significantly
reduced when compared with controls. Thomas et al. found the
reduction in walking speed to be a consequence of a reduction
in
both cadence and stride length[31]. Mazur et al. and Beyaert et
al.
however found cadence to be comparable with controls
post-arthrodesis, and the reduced walking speed to be a consequence
of
a significant reduction in stride length[28,29]. These studies
both
showed a normalisation in the proportion of gait spent in
stance
phase on the affected side. Wu et al. reported differing
findings
with an increase in cadence in the arthrodesed patient group
compared with controls, although this was not found to be
statistically significant. The authors of this paper also noted
a
significantlyincreased proportion of time spent in the swing
phase
of gait on the affected limb in the arthrodesed group [32].
The early studies looking at the spatialtemporal parameters
of
gaitfollowing ankle replacementshoweddisappointing
resultswith
minimal if any improvement in cadence, stride length and
walking
speed[24,33]. As a consequence of improvements in both
implant
and surgical technology, the results of more recent studies
usingsecond generation prosthetic designs are encouraging. Such
studies
report the majority of spatialtemporal variables to be
significantly
improved following ankle replacement. As following
arthrodesis
however, these remain significantly reduced when compared
with
controls [27,3437]. Valderrabano et al. reported in 2007 that
all
spatialtemporal factors were comparable with controls in 15
patients at 12 months following ankle replacement using the
Hintegra prosthesis [25]. Further gait studies have shown
the
improvement in post-operative walking velocity to be a result of
an
increase in cadence rather than stride length[35,37].
Interestingly,
Doets et al. found walking velocity to be comparable with
controls
following ankle replacement in rheumatoid patients, but to
remain
significantly reduced in treated patients with
osteoarthritis[36].
A proposed benefit of performing an ankle replacement asopposed
to an arthrodesis is that of reproducing a more normal
gait pattern. Interestingly, when comparing the two
modalities,
Piriou et al. noted walking speed to be closer to normal
following
arthrodesis than ankle replacement. This improved speed
follow-
ing ankle arthrodesis was at theexpense of thesymmetrical
timing
of gait and therefore patients walked with a more apparent
limp.
Ankle replacement was found to produce a gait pattern that
more
closely replicated that of controls, but with a slower
velocity[30].
3. Ankle joint kinematics
Kinematics is the study of movement of the body in space
without consideration of the forces that cause that movement.
Gait
analysis performed on normal individuals reveals that there
are
[
Fig. 1. Placement of skin markers for gait analysis [56].
T. Barton et al. / Foot and Ankle Surgery 17 (2011) 5257 53
-
8/12/2019 Biomechanical Changes Associated With the
Osteoarthritic, Arthrodesed,
3/6
large variations in the kinematics of the foot and ankle
[4,38,39].
This individuality of biomechanics therefore creates
problems
when tryingto surgically recreate what is considered to be
normal
biomechanics in patients with foot and ankle pathology. The
painful degenerate ankle joint has major implications on
joint
kinematics, and much work has focused on defining the effect
of
these changes. Early work on ankle biomechanics by Stauffer et
al.
reported a reductionin sagittal plane ankle joint motion in
patients
with a diseased ankle[24]. During gait, there was a reduction
in
dorsiflexion with the majority of ankle motion occurring in
a
plantarflexed positon through both the stance and swing
phases.
Valderrabano et al. recorded hindfoot kinematics in patients
with
ankle arthrosis and found a reduction in motion in all planes.
The
most noticeable reduction when compared to normal subjects
again occurred, as would be expected, in the sagittal
plane[25].
Khazzam et al. utilised the Milwaukee four segment foot model
to
analyse the kinematics of both the hindfoot and the forefoot
in
patients with ankle arthrosis compared with unaffected
controls
[23]. The authors reported affected patients to have a
global
decrease in the dynamic range of motion throughout all foot
and
ankle segments as compared to normal. In the hindfoot,
affected
patients demonstrated excessive external rotation throughout
gait, and were noted to have reduced hindfoot eversion from
load
response through to terminal stance. In the forefoot, a decrease
inmotion in all planes was noted, and in particular, there was
an
absence of varus rotation at toe-off which was present in
the
unaffected patients.
Leardini et al. [13] and De Asla et al. [12] have described
a
coupling between the ankle and subtalar joints during
hindfoot
motion [12,13]. Using combined magnetic resonance and dual
fluoroscopic imaging techniques, Kozenak et al. furthered this
work
andreported on thekinematicsof thetibiotalar andsubtalar joints
in
patients with ankle arthrosis. The authors reported that in
patients
witha degenerative ankle joint, in addition to a reduction in
subtalar
rotation,the direction of rotation wasreversed
whencomparedwith
normalindividuals [14]. As a consequenceof this, motioncoupling
of
the tibiotalar and subtalar joints is lost in patients with
ankle
arthosis, with both joints externally rotating during stance.
Theauthors confirmed the findings of Khazzam et al. in reporting
a
reduction in hindfoot internal rotation, which reached
statistical
significance in the subtalar joint from midstance to
toe-off.
As would be expected, ankle arthrodesis significantly
reduces
hindfoot movements in the sagittal plane [29,31,32,4042]. A
degree of hindfoot motion in this plane is preserved secondary
to a
mobile subtalar joint [2932]. Cadaveric work performed by
Valderrabano et al. found hindfoot motion to be
significantly
reduced in all planes following arthrodesis and these findings
have
been reproduced during gait analysis [911]. This reduction
in
hindfoot motion in the coronal and transverse planes is likely
a
consequence of either pre-existing or progression of
degenerative
changes within the subtalar joint[31,40,42,43].
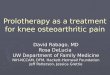
The second rocker of gait as defined by Perry is characterised
byforward progression of the tibia relative to the hindfoot
through
the stance phase of gait (Fig. 2) [44]. This motion is
reduced
following ankle arthrodesis, resulting in knee
hyper-extension
during late stance [28,29,32,42]. In addition to knee hyper-
extension, relative forward progression of thetibiais enabled by
an
early heel lift in order to increase the tilt of the tibia
relative to the
floor although not to the hindfoot [28,45,46]. If the ankle
is
arthrodesed in slight plantarflexion, knee hyperextension is
required to enable a foot flat to the ground[29,42].
Oneof theprinciple concerns following ankle arthrodesis is
that
of the adverse effect on the neighbouring joints of the foot
and
ankle complex. Clinical studies support the theory of
secondary
midfoot degenerative changes as a consequence of
compensatory
hyper-extension through the mid-foot. Gait analysis however
shows motion through the midfoot following ankle arthrodesis
to
be unpredictable with studies reporting both
increases[29,32,46
48] and decreases [31,49,50] in forefoot motion relative to
the
hindfoot. In reality, midfoot motion following ankle arthrodesis
is
likely to be dependent on a number of factors. These include
the
presence of pre-existing arthritic changes within the midfoot
joints
[43], the progression of degenerative changes as a result of
increased stresses, and the position of the arthrodesis itself.
The
employment of a variety of motion segment models and the
inherent inaccuracies of assessing the relative small movements
of
the forefoot may provide additional explanations for these
discrepancies.Gait analysis following the first generation of
ankle replace-
ments showed ankle movement to be preserved, although
failure
rates with the early constrained designs were found to be
unacceptable [24,33]. Cadaveric testing of the newer implant
designs showed recovery of plantarflexion (Agility, Hintegra)
and
inversion/eversion (Hintegra, STAR) when compared with
normal
specimens [9]. The first reports of gait analysis following
ankle
replacement with second generation designs were published in
2004. Brodsky et al. reported on eleven patients who
underwent
ankle replacement with the STAR prosthesis and found a
significantly improved range of ankle motion in the sagittal
plane
[34]. In the same year Dyrby et al. reported on pre- and
post-
operative gait analysis in nine patients, again with the
STAR
prosthesis, but found no significant improvement in ankle range
ofmovement, which remained significantly reduced when compared
with controls[27].
Doets et al. reviewed the gait analysis in ten patients
following
an ankle replacement with the BuechelPappas prosthesis and
found them to have a reduced range of dorsiflexion compared
to
controls but a similar degree of plantarflexion. During normal
gait
however, the extremes of movement in the sagittal plane were
not
required and the range of motion was found to be comparable
between the two groups[36]. More recent studies show motion
in
the sagittal plane to be improved post-operatively but to
remain
reduced when compared with controls. More importantly, they
report a more physiological pattern of gait in this plane,
particularly during the second rocker [25,37]. Coetzee et
al.
reported on radiographic assessment of ankle range of
motionfollowing ankle replacement and found this to be improved
following ankle replacement but to a lesser extent than
clinical
assessment would suggest [51]. The authors concluded that
clinical assessment of hindfoot motion is likely to include
both
hindfoot and midfoot movements, and that accurate assessment
of
tibiotalar motion requires radiographic measurements.
The assessment of hindfoot motion in the coronal plane
produce varying results, however the magnitude of readings
in
this plane are an order of magnitude lower that at the
tibio-talar
joint and therefore the significance of differing readings is
less
clear. Valderrabanoet al. and Doets et al. reported an
improvement
in the total range of motion of the hindfoot in the coronal
plane
following ankle arthroplasty to levels comparable with
unaffected
individuals [25,36]. Ingrosso et al. however found
conflicting
[
Fig. 2. Perrys rockers of gait[57].
T. Barton et al. / Foot and Ankle Surgery 17 (2011) 525754
-
8/12/2019 Biomechanical Changes Associated With the
Osteoarthritic, Arthrodesed,
4/6
results with no change in range of motion in this plane
post-
operatively [37]. With regards to mid-tarsal movement, no
significant differences were noted between controls and
patients
either pre- or post-arthroplasty [25,36]. The progression of
degenerative changes in the neighbouring joints of the foot
and
ankle has been reported following ankle replacement as well
as
ankle fusion, but to a lesser extent. Knecht et al. found that
at a
mean of 7.2 years following total ankle replacement with the
Agility prosthesis, the grade of arthritis within the subtalar
and
talonavicular subtalar increased by 19% and 15%
respectively[52].
4. Ankle joint kinetics
Kinetics is the study of movement and the forces that cause
that
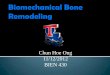
movement. The vertical ground reaction force (GRF) profile of
the
normal foot has the characteristic appearance of two peaks
representing heel strike and toe-off and a trough between
these
peaks representing mid-stance (Fig. 3). The vertical peaks are
at
approximately 115% of total body weight with the trough at
80%.
Fore-aft shear force in early stance is approximately 15% of
body
weight and represents a braking force with the centre of
gravity
falling behind the heel. As the centre of gravity moves forward
over
the anklejoint,a reversal ofthe shearforces isseenin anaft
direction
of a similar magnitude. In a medial to lateral direction, the
shear
force is initially medially before moving laterally for the
remainder
of stance with a maximal magnitude of 5% of body weight.
The pattern of ground reaction forces in patients with ankle
arthritis does not significantly differ from unaffected
patients, but
the magnitude of the vertical peaks is reduced. This change is
most
significant at the second vertical peak representing a reduction
in
the forces at toe-off. The shear forces have been shown to
be
similar between controls and affected patients [53]. There is
a
global reduction in moment forces in the arthritic ankle, with
the
most significant reduction the transverse plain (adduction
moment). The reduction in forces working across the
arthritic
ankle have been hypothesised to be a result of muscle
weakness
secondary to disuse atrophy [25] A further theory is that
the
reduced forces have a protective effect by reducing joint
loading
and shear forces[26,54].
Ankle arthrodesis results in a global reduction in the
vertical
ground reaction forces due to a combination of joint stiffness
and
muscle weakness. As confirmed by hindfoot kinematics, early
heel
lift is evident with an early drop in the first vertical GRF.
Beyaert
et al. analysed the location of the vertical GRF with respect to
the
ankle joint. The authors found that patients with an
arthrodesed
ankle demonstrated a forward shift of the GRF during the
stance
phase of gait compared with controls. In addition, the GRF
during
the third rocker was directed posterior to rather than through
the
line of the metatarsal heads. This change in orientation of
the
vertical GRF may provide a further biomechanical explanation
for
the increase in mid-tarsal symptoms in patients following an
ankle
arthrodesis[28].
Ankle replacement has been shown to improve the vertical
ground reaction force magnitude [55], but the second vertical
peak
does notreach normal levels [25,36]. One cause of this reduction
inthe vertical forces is likely to be a result of longstanding
weakness
of the triceps surae that is not fully recoverable
post-arthroplasty.
This theory has been re-enforced by EMG studies[37]. There is
a
reduction in the plantarflexion and adduction external
moment
measurements in patients post ankle replacement relative to
normal subjects. These values were found to be reduced pre-
operatively and did not significantly improve following
joint
replacement. Dyrby found a significant improvement in ankle
dorsiflexion external moments following arthroplasty to
levels
comparable with unaffected controls. Ankle inversion moments
did not improve significantly in this study and remained
reduced
compared to normal subjects [27]. The global reductions in
joint
moments are again likely a result of both protective
mechanisms
and long-standing muscle weakness.Ingrosso et al. performed
kinetic studies pre- and post-ankle
arthroplasty using the B0X prosthesis and found no
significant
improvement in any of the measured kinetic parameters. The
authors do however report a normalisation of the internal
plantarflexion moment at mid-stance at the single support
phase.
This study also performed EMG analysis and found that the
co-
contacture of tibialis anterior and gastrocnemius in
mid-stance
which was absent in the arthritic ankle was fully restored
following
ankle arthroplasty[37]. A study published in 2009 by
Detrembleur
et al. stressed the importance of performing comparative
gait
analyses at similar speeds. This enables comparisons of gait to
be
made before and after ankle arthroplasty thataccuratelyrepresent
a
true consequence of the ankle replacement and not a result
of
variations in walking velocity. The authors found the vertical
centreof mass displacement to be significantly improved following
ankle
replacement, resulting in a less flat footed walking pattern
and
decreased energy expenditure during gait[35].
5. Summary
The diseased ankle joint results in significant
biomechanical
changes within the foot and ankle complex. Gait is
asymmetric,
and walking velocity is reduced as a consequence of reduced
cadence andstride length. Hindfoot motion is reduced in all
planes,
and this reduction is mirrored in the forefoot. The coupling
of
motion within the ankle and subtalar joints seen in normal
subjects is lost, and kinetic studies show a reduced magnitude
of
the vertical ground reaction force peaks. Ankle arthrodesis
[
Fig. 3. Graphs demonstrating ground reaction forces during
ambulation [58].
T. Barton et al. / Foot and Ankle Surgery 17 (2011) 5257 55
-
8/12/2019 Biomechanical Changes Associated With the
Osteoarthritic, Arthrodesed,
5/6
improves walking speed although the asymmetry of gait
remains.
Hindfoot motion is reduced in all planes, and forward
progression
of the tibia through stance is aided by knee hyper-extension
and
early heel lift. Kinetic studies confirmthe early heel lift
andreveal a
posterior displacement of the ground reaction force through
late
stance increasing the forces through the midfoot region.
Ankle
replacement produces a more symmetrical walking pattern, as
well as an improvement in overall velocity. Kinematics is
significantly improved but remain reduced when compared with
unaffected subjects. The pattern of hindfoot motion more
closely
resembles unaffected controls when compared with ankle
arthro-
sis or arthrodesis. A similar improvement is seen in kinetic
analysis
following ankle replacement, however external moments do not
reach normal levels as a consequence of long standing muscle
weakness.
6. Future directions
There is an increasing understanding of the biomechanics of
the
foot and ankle complex, in particular following ankle
arthrodesis
and ankle replacement. The ultimate aim of such research is
to
guide improvements in the non-surgical and surgical treatment
of
foot and ankle pathology and to this end our understanding is
stilllimited. Gait analysis remains an overall summary of foot
and
ankle biomechanics, without providing accurate information as
to
the kinematics and kinetics across individual joints during
gait. A
further issue is that of the changing direction and magnitude
of
forces across joints through the stages of gait, and this
remains of
particular relevance for the ankle replacement. Improving
the
longevity of such implants is essential if they are to remain a
valid
option in the treatment of the diseased ankle joint. When
performing an ankle replacement, consideration must be given
to the balance of the foot as a whole, and in particular
with
reference to the forefoot. Further studies are required with
respect
to the kinetics following ankle replacement in order to
ascertain
whether we are accurately able to balance the forces across
the
prosthesis which is essential to improve outcome and implant
survival. This is of increasing importance as such procedures
are
being performed on patients with increasing degrees of
hindfoot
and forefoot deformities.
Conflict of interest statement
There are no conflicts of interest.
References
[1] SaltzmanCL, ZimmermanMB, ORourkeM, Brown TD,Buckwalter
JA,JohnstonR. Impact of comorbidities on the measurement of health
in patients withankle osteoarthritis. J Bone joint Surg Am
2006;88(2):236672.
[2] Deland JT, Morris GD, Sung IH. Biomechanics of the ankle
joint. A perspective
on total ankle replacement. Foot Ankle Clin 2000;5(4):74759.[3]
KitaokaHB,CrevoisierXM,HansenD,et al.Footandanklekinematicsand
groundreaction forces during ambulation. Foot Ankle Int
2006;27(10):80813.
[4] Carson MC, Harrington ME, Thompson N, OConnor JJ, Theologis
TN. Kinematicanalysis of a multi-segment model for research and
clinical applications: arepeatability analysis. J Biomech
2001;34:1299307.
[5] Leardini A, OConnor JJ, Catani F, Giannini S. A geometric
model of the humanankle joint. J Biomech 1999;32(6):58591.
[6] WestbladP, Hashimoto T, Winson I, LundbergA, Arndt A.
Differences in ankle-joint complex motion during the stance phase
of walking as measured bysuperficial and bone-anchored markers.
Foot Ankle Int 2002;23(9):85663.
[7] Arndt A, Westbald P, Winson I, Hashimoto T, Lundberg A.
Ankle and subtalarkinematics measured with intracortical pins
during the stance phase ofwalking. Foot Ankle Int
2004;25(5):35764.
[8] Michelson JD, Schmidt GR, Mizel MS. Kinematics of a total
ankle arthroplasty:comparison to normal ankle motion. Foot Ankle
Int 2000;21:27884.
[9] Valderrabano V, Hinterman B, Nigg BM, Stefanyshyn D,
Stergiou P. Kinematicchanges after fusion and total replacement of
the ankle. Part 1. Range ofmotion. Foot Ankle Int 2003;24:8817.
[10] Valderrabano V, Hinterman B, Nigg BM, Stefanyshyn D,
Stergiou P. Kinematicchanges after fusion and total replacement of
the ankle. Part 2. Movementtransfer. Foot Ankle Int
2003;24:88896.
[11] Valderrabano V, Hinterman B, Nigg BM, Stefanyshyn D,
Stergiou P. Kinematicchanges after fusion and total replacement of
the ankle. Part 3. Talar move-ment. Foot Ankle Int
2003;24:897900.
[12] DeAsla R, Wan L, RubashHE, Li G. SixDOF in vivo kinematics
of theankle jointcomplex: application of a combined dual-orthogonal
fluoroscopic and mag-netic resonance imaging technique. J Orthop
Res 2006;101927.
[13] Leardini A, Stagni R, OConnor JJ. Mobility of the subtalar
joint in the intactankle complex. J Biomech 2001;34:8059.
[14] Kozanek M, Rubash HE, Li G, de Asla R. Effects of
post-traumatic tibiotalarosteoarthritis on kinematics of the ankle
joint complex. Foot Ankle Int2009;30(8):73441.
[15] Michael JM, Golshani A, Gargac S, Goswani T. Biomechanics
of the ankle jointand clinical outcomes of total ankle replacement.
J Mech Behav Biomed Mater2008;1:27694.
[16] Buechel Sr FF, Buechel Jr FF, Pappas MJ. Twenty year
evaluation ofcementless, mobile-bearing total ankle replacements.
Clin Orthop 2004;424:1926.
[17] Wood PL, Karski MT, Watmough P. Total ankle replacement:
the resultsof 100 mobility total ankle replacements. J Bone Joint
Surg Br 2010;92(7):95862.
[18] Henricson A, Knutson K, Lindahl J, Rydholm U. The AES total
ankle replace-ment: a mid-term analysis of 93 cases. Foot Ankle
Surg 2010;16(2):614.
[19] Saltzman CL, Mann RA, Ahrens JE, Amendola A. Prospective
controlled trial ofSTAR total anklereplacement versus ankle fusion:
initial results.Foot AnkleInt2009;30(7):57996.
[20] Espinosa N, Walti M, Favre P, Snedeker JG. Misalignment of
total anklecomponents can induce high joint pressure. J Bone Joint
Surg (Am)
2010;92:117987.[21] FukadaT, Haddad SL, Ren Y, Zhang LQ. Impact
of talar component rotation on
contact pressure after total ankle arthroplasty: a cadaveric
study. Foot AnkleInt 2010;31(5):40411.
[22] Hintermann B, Valderrabano V. Total ankle replacement. Foot
Ankle Clin2003;8(2):375405.
[23] Khazzam M, Long JT, Marks RM, Harris GF. Preoperative gait
characterizationof patients with ankle arthrosis. Gait Posture
2006;24:8593.
[24] Stauffer RN, Chao EYS, Brewter RC. Force and motion
analysis of thenormal, diseased, and prosthetic ankle joint. Clin
Orthop Rel Res 1977;127:18996.
[25] Valderrabano V, Nigg BM, von Tscharner V, Stefanyshyn DJ,
Goepfert B,HintermanB. Gaitanalysisin ankleosteoarthritis and total
anklereplacement.Clin Biomech 2007;22. 944-904.
[26] Mundermann A, Dyrby CO, Andriacchi TP. Secondary gait
changes in patientswith medial compartment knee osteoarthritis:
increased load at the ankleknee, and hip during walking. Arthritis
Rheum 2005;52(9):283544.
[27] Dyrby C, Chou LB, Andriacchi TP, Mann RA. Functional
evaluation of theScandinavian total ankle replacement. Foot Ankle
Int 2004;25:37781.
[28] Beyaert C, Sirveaux F, Paysant J, Mole D, Andre J-M. The
effect of tibio-talararthrodesis on foot kinematics and ground
reaction force progression duringwalking. Gait Posture
2004;20:8491.
[29] Mazur JM, Schwartz E, Simon SR. Ankle arthrodesis.
Long-term follow-up withgait analysis. J Bone Joint Surg Am
1979;61:96475.
[30] Piriou P, Culpan P, Mullins M, Cardon JN, Pozzi D, Judet T.
Ankle replacementversus arthrodesis: a comparative gait analysis
study. Foot Ankle Int2008;29(1):39.
[31] Thomas R, Daniels TR, Parker K. Gait analysis and
functional outcomesfollowing ankle arthrodesis for isolated ankle
arthritis. J Bone Joint SurgAm 2006;88(3):52635.
[32] WuWL, SuFC, ChengYM, HuangPJ, Chou YL,ChouCK.Gait
analysisafter anklearthrodesis. Gait Posture 2000;11:5461.
[33] Demottaz JD, Mazur JM, Thomas WH, Sledge CB, Simon SR.
Clinical study oftotal ankle replacement with gait analysis. A
preliminary report. J Bone JointSurg Am 1979;61:97688.
[34] Brodsky JE, Pollo FE, Baum BS. Gait analysis results after
STAR total anklearthroplasty. In: 5th European foot and ankle
society congress proceedings,
European Foot and Ankle Society; 2004.[35] Detrembleur C,
Leemrijse T. The effects of total ankle replacement on
gaitdisability: analysis of energetic and mechanical variables.
Gait Posture2009;29(2):2704.
[36] Doets HC, vanMiddelkopp M, Houdijk H, Nelissen RG, Veeger
HE. Gaitanalysisafter successful mobile bearing total ankle
replacement. Foot Ankle Int2007;28:31322.
[37] Ingrosso S, Benedetti MG, Leardini A, Casanelli S, Sforza
T, Giannini S. Gaitanalysis in patients operated with a novel total
ankle prosthesis. Gait Posture2009;30(2):1327.
[38] Conti S, Lalonde KA, Martin R. Kinematic analysis of the
agility total ankleduring gait. Foot Ankle Int
2006;27(11):9804.
[39] Lundberg A, Svensson OK, Bylund C, Selvk G. Kinematics of
the ankle/footcomplex. Part 2. Pronation and supination. Foot Ankle
1989;9(5):24853.
[40] Mann RA, RongstadKM. Arthrodesis of theankle: a
criticalanalysis. FootAnkleInt 1998;19(1):39.
[41] TakakuraY, TanakaY, Sugimoto K, AkiyamaK, Tamai S.
Long-term resultsforarthrodesis for osteoarthritis of the ankle.
Clin Orthop Rel Res 1999;361:17885.
T. Barton et al. / Foot and Ankle Surgery 17 (2011) 525756
-
8/12/2019 Biomechanical Changes Associated With the
Osteoarthritic, Arthrodesed,
6/6
[42] Buck P, Morrey BF, Chao EY. The optimum position of
arthrodesis of the ankle.A gait study of the knee and ankle. J Bone
Joint Surg Am 1987;69:105262.
[43] Sheridan BD, Robinson DE, Hubble MJ, Winson IG. Ankle
arthrodesis and itsrelationship to ipsilateral arthritis of the
hind- and mid-foot. J Bone Joint SurgBr 2006;88(2):2067.
[44] Perry J. Gait analysis: normal and pathological function.
Thorofare, NJ: SlackInc.; 1992.
[45] Blanc Y, Balmer C, Landis T, Vingerhoets F. Temporal
parameters and patternsof the foot role over during walking:
normative data for healthy adults. GaitPosture 1999;10:97108.
[46] Hunt AE, Smith RM, Torode M, Keenan A-M. Inter-segment foot
motion and
ground reaction forces over the stance phase of walking. Clin
Biomech (BristolAvon) 2001;16:592600.[47] Bobbyer GN. The long-term
results of ankle arthrodesis. Acta Orthop Scand
1981;52:10710. 1981.[48] Morgan CD, hence JA, Bailey RW, Kaufer
H. Long-term results of tibio-talar
arthrodesis. J Bone Joint Surg Am 1985;67:54650.[49] Coester LM,
Saltzman CL, Leupold J, Pontarelli W. Long-term results
following
ankle arthrodesis for post-traumatic arthritis. J Bone joint
Surg Am2001;83:21928.
[50] Lynch AF,BourneRB, Rorabeck CH. Thelong-term results of
ankle arthrodesis.JBone Joint Surg Br 1988;70:1136.
[51] Coetzee JC, Castro MD. Accurate measurement of ankle range
of motion aftertotal ankle replacement. Clin Orthop Rel Res
2004;424:2731.
[52] Knecht SI, Estin M, Callaghan JJ, Zimmerman MB. The agility
total ankle arthro-plasty, seven to sixteen year follow-up. J Bone
Joint Srug (Am) 2004;86(6):116171.
[53] Shih LY, Wu JJ, Lo WH. Changes in gait and maximal ankle
torque in patientswith ankle arthritis. Foot Ankle
1993;14:97103.
[54] Kerin AJ, Coleman A, Wisnom MR, Adams MA. Propagation of
surface fissuresin articular cartilage in responseto cyclic
loadingin vitro. ClinBiomech(Bristol
Avon) 2003;18(10):9608.[55] Zerahn B, Kofoed H. Bone mineral
density, gait analysis, and patient satisfac-tion, before and after
ankle arthroplasty. Foot Ankle Int 2004;25(4):20814.
[56] de Vries G, Roy K, Chester V. Using three-dimensional gait
data for foot/ankleorthopaedic surgery. Open Orthop J
2009;3(3):8995.
[57] Lin RS, Gage JR. J Prosthet Orthot 1990;2(1):111.[58]
Whittle M. Gait analysis: an introduction. Boston:
Butterworth-Heinemann/
Oxford; 2002.
T. Barton et al. / Foot and Ankle Surgery 17 (2011) 5257 57





![Provided by the author(s) and University College Dublin ... · 87 biomechanical analysis is a characteristic feature associated with the CAI [6]. Biomechanical ... 95 populations](https://img.pdfslide.us/doc/110x75/60390b96d017f17e7838551e/provided-by-the-authors-and-university-college-dublin-87-biomechanical-analysis.jpg)