Embed Size (px)
Citation preview

Biomechanical Aspects of Spinal Cord Injury
Thomas R. Oxland PhD PEngProfessor & Director
Division of Orthopaedic Engineering ResearchDepartments of Orthopaedics & Mechanical Engineering
The University of British Columbia Vancouver Coastal Health Research Institute

UBC – The University of British Columbia
• 40,000 students
• 4,000 faculty

UBC Department of Orthopaedics
• 65 faculty members• 5 teaching hospitals• basic & clinical
research
• seven Divisions– Athletic Injuries– Lower Limb Reconstruction– Upper Limb Reconstruction– Pediatrics– Spine– Trauma– Orthopaedic Engineering
Research

Orthopaedic Engineering Research (DOER)
• the application of engineering principles to clinically relevant problems in the field of Orthopaedics

DOER at UBC
• Thomas Oxland• David Wilson• Heather McKay• Karim Khan• Peter Cripton• Steve Robinovitch• Rizhi Wang• Goran Fernlund• Gail Thornton
• Clive Duncan• Bassam Masri• Don Garbuz• Marcel Dvorak• Brian Kwon • Charles Fisher• Pierre Guy• Peter O’Brien• Robert McCormack• Bill Regan

Research Themes
• Mechanisms of Spine and Spinal Cord Injury [Oxland, Cripton, Kwon, Dvorak,Tetzlaff]
• Etiology of Osteoarthritis [Wilson, MacKay, Cibere]
• Hip Fracture Prevention [McKay, Khan, Robinovitch, Guy]
• Surgical Solutions in presence of Bone Loss– osteoporotic spine [Oxland, Cripton, Dvorak, Fisher]– revision hip [Oxland, Duncan, Masri, Fernlund]

SCI Epidemiology
• ~11,000 new injuries/year in North America (40/million)
• 200,000 chronic injuries• Average age 32 • $9.73 billion/year
– hospitalization, rehabilitation, medication, equipment, loss productivity
-Spinal Cord Injury Information Network - www.spinalcord.uab.edu

ICORD – new home for Spinal Research Centre in Vancouver
•Vancouver General Hospital
•51 principal investigators
•120,000 square feet
•Spinal clinics
•Rehabilitation research
•Molecular Biology
•Bioengineering
•Neuropysiology
February 2008
October 2008

Theme 3-
Develop novel animal models of SCI where damage can be induced within an enclosed vertebral column, thereby more accurately mimicking human SCI.
Can only be achieved through the combined efforts of spine surgeons, biomechanical engineers and neuroscientists working side-by-side.

Theme 3 - Overview
Spinal cord injury represents a
mechanical insult that triggers a
biological response which results in a
wide range of clinical sequelae.


Type of Vertebral Injury
40% Fracture Dislocation
5% Dislocation
Burst Fracture 30%
SCIWORET 10%
SCIWORA 5%
10% Minor Fracture
Sekhon & Fehlings Spine 2001

Spinal Injury
FRACTURE DISLOCATION
BURST FRACTURE
FLEXION-DISTRACTION

Clinical Observation
• the mechanism of column damage correlates with the neurological deficit – Marar 1974, Tator 1983
…. but current treatments do not incorporate injury mechanism!


Methods – Cord/Column
• Surrogate Cord – Silicone gel
– In vivo-like in tension
• Barium Sulfate added
• Oval shaped
Saari MASc 2006

Methods – Specimen Preparation
• Human cervical spines occiput to T2 (n = 6)
• Surrogate head attached to occiput
Saari MASc 2006

Methods – Imaging
• High Speed X-ray
– Industrial X-ray source
• 75kV, 5mA
– 9” image intensifier
– Internal high speed camera
• 1000 frames per second
• 256 x 240 pixels
Image Intensifier
X-ray Source
Saari MASc 2006

Saari MASc 2006

Flexion-compression injury model
Effect of Constraint
Zhu 2008

Compression to the Specimen
Displacement
-25
-20
-15
-10
-5
0
0.5 0.7 0.9 1.1 1.3 1.5
Time (sec)
Dis
pla
cem
ent
(mm
)
35 msec
Zhu 2008

Flexion-Compression (constrained)

Flexion-Compression (unconstrained)
Zhu 2008

Canal Occlusion
130
140
150
160
170
180
190
200
0 10 20 30 40 50 60
compression (mm)
Sp
ina
l c
an
al
are
a (
mm
^2
)
unconstrained
constrained
Zhu 2008

Column-Canal Relationships
constrained unconstrained
Zhu 2008

Pro-Neck-TorTM Standard Helmet
http://injury.mech.ubc.ca http://www.pronecktor.com
Dr. Peter Cripton

15º, Med Stiffness, Extension Escape, Vimpact ~3.2 m/s
Proof of Concept Study – Results:
• Axial Force Escape-Angle Interaction
56% reduction

C4
C5
C6
Greaves 2008

Von Mises StrainCompression
0.320.280.240.200.160.120.080.040.00 0.370.320.280.240.200.160.120.080.040.00 0.370.290.260.220.180.150.110.070.040.00 0.330.290.260.220.180.150.110.070.040.00 0.33
dorsalventralventral
dorsal
Greaves 2008

Von Mises StrainDistraction
0.320.280.240.200.160.120.080.040.00 0.370.320.280.240.200.160.120.080.040.00 0.37
0.110.100.080.070.050.040.030.010.00 0.120.110.100.080.070.050.040.030.010.00 0.12
0.090.080.070.060.050.040.030.030.02 0.100.090.080.070.060.050.040.030.030.02 0.10
dorsalventral ventral
dorsal
Greaves 2008

Von Mises StrainDislocation
0.280.250.210.180.140.110.080.040.00 0.320.280.250.210.180.140.110.080.040.00 0.320.270.230.200.170.130.100.070.030.00 0.300.270.230.200.170.130.100.070.030.00 0.30
dorsalventralventral
dorsal
Greaves 2008

Different Cord Strain Patterns
Greaves Annals BME 2008

Contusion

Theme 3 - Overview
Spinal cord injury represents a
mechanical insult that triggers a
biological response which results in a
wide range of clinical sequelae.

Spinal Injury
FRACTURE DISLOCATION
BURST FRACTURE
FLEXION-DISTRACTION
Do these well-known spinal column injury patterns create different spinal cord injuries?

Injury Models
1970 199019801911 2004
NYU -Gruner
g-cm-Albin
F, IH -Scheff
d, OSU -Noyes
d
Weight drop-Allen
m
h
clip -Tator
Transection
LateralDislocation
-Fiford
Distraction-Maiman

Contusion Paradigm
Figure from McDonald & Belegu. J Neurotrauma 2006
… central cavitation with peripheral rim of spare white matter …

Type of Vertebral Injury
40% Fracture Dislocation
5% Dislocation
Burst Fracture 30%
SCIWORET 10%
SCIWORA 5%
10% Minor Fracture
Sekhon & Fehlings Spine 2001

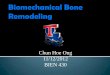
Experimental Animal Model
Compression/Contusion Shear/Dislocation Distraction
Choo PhD 2006

UBC SCI Test System
Load Cell(22 & 225N)
accelerometer(50 & 500G)
LVDT(0.001mm)
Actuator12mm
Choo PhD 2006

Contusion
5.005 5.01 5.015 5.02-2
-1
0
1
2
3
4
time (s)
dis
pla
cem
ent
(mm
)velo
city
(m
/s)
-2
-1
1
0
4
2
3
forc
e (
N)
Cord surface
Choo PhD 2006

Dislocation
2.995 3 3.005 3.01 3.015-1
-0.5
0
0.5
1
1.5
2
2.5
3
time (s)
dis
pla
cem
ent
(mm
)velo
city
(m
/s)
forc
e (
N)
-10
-5
10
5
30
15
25
20
Choo PhD 2006

Distractiondis
pla
cem
ent
(mm
)velo
city
(m
/s)
0
10
40
20
30
forc
e (
N)
Choo PhD 2006

Hemorrhage
Choo PhD 2006

Anatomy
&

Study 1: Primary Injury

Membrane Integrity

Membrane Integrity

Membrane Damage
Neuronal Cell Bodies Axons
NeuN

Primary Injury• 275-325g Sprague-Dawley rats• Infused 0.375mg 10kD fluorescein dextran into cisterna magna• Incubated for 1 hour + 30 min surgery• Injury ~100cm/s @ C4/5• 5 min sacrifice – primary damage
Mechanism N Severity
Contusion 9 1.1mm
Dislocation 9 2.5mm
Distraction 9 4.1mm
Shams 8 -

Membrane DamageNeuronal Cell Bodies
Lesion RostralInjury
Choo J. Neurosurg. 2007

Membrane DamageAxons
Lesion RostralInjury
Choo J. Neurosurg. 2007

Rostro-Caudal Distribution

Study 2: Early Secondary Injury

Early Secondary Injury• 275-325g Sprague-Dawley rats• Infused 0.375mg 10kD fluorescein dextran into cisterna magna• Incubated for 1 hour + 30 min surgery• Injury @ ~100cm/s• 0.75mg 10kD cascade-blue dextran @ 2hrs
– detect persistent membrane permeability
• 3hrs sacrifice – early secondary
Mechanism N Severity
Contusion 10 1.1mm
Dislocation 10 2.5mm
Distraction 10 4.1mm
Shams 7 -
Dextran Controls 3 -

Membrane Integrity at 3hrs
Pre-injury Dextran Post-injury Dextran Merged Image
Choo Exp. Neurol. 2008

Secondary Axonal Injury
((ββAPP)APP)

Secondary Axonal Injury

Secondary Axonal Injury

Microglial Activation
Activation

Microglial Activation
Act
ivati
on
Choo Exp. Neurol. 2008

Overall Patterns of Tissue Damage

Tissue Damage ≈ Mechanics?

Limitations
• Early time-points for analysis
• Comparable severities?
• Behaviorial differences?
• No therapies tested

Summary
• SCI is a high-speed event that we are characterizing from a biomechanical perspective– Cadaver models– Mathematical models– Small animal models
• Ultimate goal is a clinically relevant sub-classification of SCI

Next Steps…..
• Further characterize primary injury & secondary changes;
• Assess behavioural differences between mechanisms;
• Determine the effectiveness of imaging (MRI) in differentiating between injury mechanisms;
• Evaluate the efficacy of novel therapeutic strategies for spinal cord injury (e.g. neuroprotective, remyelination)

Collaborators
• Anthony Choo• Carolyn Sparrey• Carolyn Greaves• Simon Sjovold• Liz Clarke (AUS)• Amy Saari (PC)• Shannon Reed
(PC)• Tim Bhatnagar• Colin Russell
• Wolfram TetzlaffWolfram Tetzlaff• Peter CriptonPeter Cripton• Marcel DvorakMarcel Dvorak• Brian KwonBrian Kwon• Charles FisherCharles Fisher• Mohamed GadalaMohamed Gadala• Piotr KozlowskiPiotr Kozlowski• Lynne Bilston Lynne Bilston
(AUS)(AUS)
• Qingan ZhuQingan Zhu• Jie LiuJie Liu• Clarrie LamClarrie Lam• Chad LarsonChad Larson• Darrell Darrell
GoertzenGoertzen• Andrew YungAndrew Yung

Acknowledgements
Canada Research Chairs Program
George W. Bagby Research Fund
BC Leading Edge Endowment Fund
Canadian Institutes of Health Research
Rick Hansen Man in Motion Fund

Professor Manohar Panjabi
Yale University
1970-2006

Professor Clive Duncan
Chairman of Orthopaedics at UBC from 1996-2006

Thank you!