Embed Size (px)
Citation preview

BIOMATERIALS USED AS BONE GRAFT SUBSTITUTESs. Narang, V. Chava. Biomaterials used as bone graftsubstitutes. Annal Dent Univ Malaya 2000; 7: 36-42.
ABSTRACT
The ultimate goal of periodontal therapy should not belimited to the establishment and maintenance ofperiodontal health. The potential for regeneration of thehard and soft periodontal tissues lost to disease shouldbe considered. Of all the bone grafting materials beingdeveloped, the demineralized freeze dried bone allo-graft (DFDBA) has been used as a substitute for bonegraft for more than four decades. The basis for the useof any bone grafting material is to induce boneformation. In this article various biomaterials used arereviewed.
Key words: Bone, Graft, Biomaterial.
INTRODUCTION
The upcoming of various bone grafts and biomaterialshas given a big leap to the field of Periodontics. Theaim of periodontal therapy is to control periodontalinfection and inflammation in the periodontium. Thecontinued function of the periodontally involved toothrequires additional periodontal support and regenerationof the lost periodontium (1,2). This may be achievedby the use of guided tissue regeneration and variousbone grafts and biomaterials used as substitutes of bonegrafts. These are derived from vital or non vital bonesources or consist of organic or inorganic materials. Themain aim of utilizing bone grafts and performing bonegraft related osseous surgeries is to promote boneregeneration. However these materials should bebiologically acceptable to the patient without causing anysystemic or local hazards or side effects. Often,autogenous bone is not available in sufficient quantityand if available requires additional surgical sites as wellas an increased amount of chair time for the patient.Allogeneic bone is an alternative to autogenous bone,but poses the fear of disease transmission. Thisprompted the development of various bone substituteswhich have provided us biocompatible defect fillerswith differing biologic activity (l).
BASIC CONSIDERATIONS
Definitions:
1. Graft:A graft is a viable tissue that after removal from
the donor site is implanted within the lost tissue whichis then restored, repaired or regenerated (3).
Examples: Autografts and Allografts.
Aevievv Article
S. Narang1 and V. Chava2
}Post Graduate StudentDepartment of Periodontics
2Department of PeriodonticsS.D.M. College Of Dental SciencesAnd HospitalDharwad-580 009, Karnataka,INDIA
Corresponding author - V. Chava
2. Biomaterials:These are bone derived materials processed in such
a way that the cells are no longer vital and hence usedas bone graft substitutes (I).
Examples:- Freeze dried bone, decalcified or non-
decalcified.- Xenograft from a bovine derived material can
be more appropriately called Xenogenic bonederived biomaterial.
3. Osteogenesis:Occurs when cells of graft survive the
transplantation and contribute to the repair process. Theterm has been used by some authors to define bonegrafts with the capability of forming bone throughosteoblastic cells contained in the transplanted site (2,3).
4. Osteo conduction:Process also known as Trell's effect, occurs with
the ingrowth of capillaries in the new connective tissues.A material is osteo conductive when its structure andits chemical composition facilitate new bone formationfrom existing bone. This can be seen with various bonegrafts or non bone grafts such as synthetic materials(l,3).
5. Osteo induction:It is a process or a set of processes, which initiate
osteogenesis through cells orginally not involved in boneformation (I).
Examples: A graft, a biomaterial or a substance isosteo inductive when implanted in a non osseousenvironment called as an ectopic site, bone formationoccurs.
The Ideal Requirements for bone grafts or bone graftsubstitutes may be summarised as follows:
1. Biologic acceptabilityII. Predictabilityiii. Clinical feasibility

IV. Minimal operative hazardv. Minimal post operative sequelaeVI. Patient acceptance.
BONE GRAFTS AND BONE GRAFTSUBSTITUTES
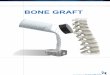
Figure I illustrate the categories of bone grafts and bonegraft substitutes.
I) Non-osseous materialA) Organic
i) DentinAlthough demineralised dentin has beenadvocated as a possible graft (5), it has notgained widespread acceptance (6) becauseclinical results have been somewhatdisappointing.
ii) DuraThe use of lyophilised allogeneic duramater inperiodontal osseous defects has resulted in gainof clinical attachment and reduction in probingdepth. Histologically bone has been seenalongside but never in the implant (7).
iii) ScleraSuccess has been reported with preserved sclera(4), but there were no signs of osteogenesiswithin the sclera and it remained encapsulatedat the site (6).
iv) CartilageCartilage allografts provide no statisticallysignificant advantage in bone or soft tissue repairover flap debridement alone (9).
B) Inorganici) Plaster of Paris
Plaster of Paris (Calcium sulphate) isbiocompatible and porous thereby allowing fluidexchange, which prevents nap necrosis. Plasterof Paris resorbs completely in 1-2 weeks(lO).Also, because plaster of paris is so rapidlyresorbed, it is questionable whether it is of anybenefit.
ii) Bio active glassesThere are 2 forms of bioactive glass currentlyavailable, perio glass (Bio glass synthetic bonegraft particulate) and biogran (resorbablesynthetic bone graft). Bio active glasses arecomposed of SI02, CaO, Na20, P2 05 and bondto bone is through the development of a surfacelayer of carbonate hydroxyapatite(HA). Whenexposed to tissue fluids invivo, the bioactiveglass is covered by a double layer composed ofsilica gel and a calcium phosphate-rich (apatite)layer. This calcium phosphate-rich layerpromotes adsorption and concentration of
Biomaterials used as bone graft substitutes 37
proteins used by osteoblasts to form amineralised extracellular matrix. It is theorizedthat these bioactive properties guide and promoteosteogenesis, allowing rapid and quick formationof new bone (II).
II. Bone derived materialA) Intraoral autografts.a) (i) Osseous coagulum and bone blend
Robinson, in 1969, having considered that thegrafted particles of bone should be of smallersize and that mineralised fragments can induceosteogenesis, developed a technique, which hetermed osseous coagulum, using the materialevacuated during osseous surgery. The donorbone is obtained from any intra-oral source,usually areas requiring osseous correction. Anumber 6 or 8 round carbide bur, rotating at25000 to 30000 rpm, without irrigation,produces bone dust which when coated withblood makes an osseous coagulum. Robinsonshowed the feasibility of the technique in severalcase reports with re-entries from 3 to 24 months.Diem et al in 1972, proposed the use of anamalgam trituration capsule and a pestle toreduce bone fragments to a workable, plastic likemass, called Bone Blend (I).
ii) Intra-oral cancellous bone marrow transplants.,Haitt and Schallhorn have described the use ofcancellous bone obtained from the maxillarytuberosity, edentulous areas and healing sockets.The maxillary tuberosity frequently contains agood amount of cancellous bone, particularly ifthe third molars are absent. Foci of red marroware also occasionally observed. Edentulousridges can be approached with a flap, andcancellous bone and marrow are removed withcurettes. Sockets are allowed to heal for 8-12weeks, and the apical portion is utilised as donormaterial. The particles are reduced to smallpieces (4).
b) Bone swaging.This technique requires the existence of anedentulous area adjacent to the defect, from whichthe bone is pushed into contact with the root surfacewithout fracturing the bone at its base (4)
B) Iliac bone and marrow autografts.Schallhorn, in 1968, described the first autogenous
iliac bone graft in one case report where a bone marrowbiopsy was immediately implanted into interproximalbony craters between both lower canines and lateralincisors. At 5 months re-entry, the defects appearedcompletely filled. Autografts of iliac bone and marrowpossess a high osteogenic potential, even in supra crestalbone fill and class II furcations. They are able to inducecementogenesis, bone regeneration and Sharpey's fibresreattachment with functionally oriented periodontalligament. Fresh iliac bone and marrow are responsible

38 Annals of Dentistry, University of Malaya, Vol. 72000
for a high rate of resorption and ankylosis. The needfor a~ extra oral surgical site and for a samplingtechmque performed by a trained specialist representserious limitations to this procedure (1)
AllograftsIliac autografts have proven to be a predictable
osseous grafting material, however, this necessitates anadditional extra oral surgical procedure in order toobtain the grafting material. Allogeneic bone eliminatesthe need for additional surgery (1). Attempts have beenmade to suppress the antigenic potential of allografts andxenografts by radiation, freezing and chemicaltreatment. Bone allografts are commercially availablefrom tissue banks. They are obtained from cortical bonewithin 12 hours of the death of the donor, defatted, cutin pieces, washed in absolute alcohol, and deep frozen.The material mayor may not then be demineralised and6ubsequently, it is ground and sieved to a particle sizeof 250 to 750 mm and freeze dried. Finally it is vaccumsealed in glass vials (4).
In conclusion, allografts do not elicit any adverseimmune response; have the same potential forregeneration as iliac autografts: crestal boneregeneration and regeneration of a normal periodontiumhave been demonstrated, and they do not give rise to:oot ~esorption or ankylosis. However, this approach,III spite of its many advantages, is not recommendedbecause of the high risk of disease transmission.
Bone grafts and Bone graft substitutes
I. Non-osseous material
" .._- J •
BIOMA TERIALSFigure II illustrates the categories of Biomaterials.
I. Bone derived biomaterials
A. Freeze dried human boneThese are bone graft substitutes which are available
through bone banks and are obtained from autopsy ofhuman donors within 24 hours after death and arefurther lyophilized after a series of physical andchemical processing. In this procedure the guide linesof the American Association of Tissue Banks is followed(1).
It includes:• Bone procured from the human donor within 24
hours after death.• It is frozen to -1790 C for 4 weeks.• Graft is freeze dried.• Graft is defatted in chloroform menthol for 6
hours at 25°C.• Autodigested in phosphate buffers containing
iodoacetate acid and sodium azide for 72 hoursat 37°C.
• Demineralized in 0.6 N HCL for 3 days at 4°C.• After each step bone is washed with triple
distilled water.• Refrozen and freeze dried.• Ground under cryogenic conditions to yield a
particle size of 125-1000 microns.
II. Bone derived material
A. Organic- Dentine- Cementum- Collagen- Coral
B. InorganicPlaster of ParisCalcium Phosphate HACeramicesBioglass
- Polymers
Non Bone(Freeze dried)Human Bone: FDBA-DFDBABovine Bone
~ _ .._ .._ .._--_._-_ _ _ ..__ ._------_ ..-
AUlOgrafls
. ., .PedIcle GrallsBone swaging
Oral
- Bone coagulum- Bone blend- From tuberosity- Extraction site- Edentulous ridge
Vital BoneBone grafts)
• •• •• •••• _ ••••• HH •• ~~H ••••••••••••• _ •• I..... --------.- .. -- _-----.Allografts
- Cryo preserved- Bone marrow
From iliac crest
+Free Grafts
1- Extra Oral
- Bone marrow- Iliac crest
Figure 1: Categories or"bone grafts and bone graft substitutes

Biomaterials used as bone graft substitutes 39
Biomaterials
I. Bone derived biomaterials
A. Freeze Dried Human BoneI
B. Freeze Dried Bovine Bone
I
FDBA DFDBA - Boplant- DBP
(Demineralised Bovine Bone Powder)_ Bovine derived hydroxyapatite_ Anorganic Bovine bone (ABB)
II. Alloolastic bone ~raft substitutes:r···· ·····.-·-.--..-··..-··-··.---r·--·····.L- ...·.··.····.r.-.- ..--..--.- ..+A. Calcium Phophate
Ceramics
a. DenseHydroxyapatites
b. PorousHydroxyapatite
B.Natural CoralSkeleton
~a. Calcium
Carbonate
C. Polymers
a. PMMAPolymers
b. ResorbablePolyesters
D. Tetracyclineaddition to bonegraft substitutes
Figure 2: Categories of Biomaterials.1. Bone derived. II. Alloplastic bone derived substitutes.
The osteo inductive capacity of these materials isgoverned by the processing procedure. The inductiveactivity gradually decreases atjd eventually is reducedto 0 within a period of 15 days when decalcification with0.6 N HCL is performed at 25°C. wheareas in coldtemperature (2°C), the inductive activity is fairlymaintained even at 30 days. Ethyl or isopropyl alcoholsin 0.6 N HCL produces total inactivation of inductivesubstitute. Delipidization with ether, alcohol, acetone,hexachlorophene, common detergents and Tween 80may even enhance bone induction. Heating above 60°Cinhibits bone formation.
B. Freeze Dried Bovine Bonei) Boplant:
The use of Boplant, a bovine bone processed bydetergent, chloroform and methanol extraction toreduce lipid content, washed, sterilized in antisepticsolution and lyophilized was first used way back in1966 (1). The extensive usage of this material ledto the conclusion that the material was incorporatedby new bone formation, and it was accepted as awell tolerated, non resorbable, osteoconductivematerial. It was observed that the osteogenicpotential of decalcified Boplant did not appeargreater than that of mineralized Boplant (1,12).
ii) Demineralized bovine bone powder (DBP)It is prepared from cortical portions of bovine boneafter 1 hour extraction in 100 % ethanol and ethylether. It is then pulverized in liquid nitrogen mill,demineralized for 3 hours in 0.5 N HCI and washed
with water, absolute ethanol and anhydrous etheruntil neutral pH is achieved (1).
iii) Bovine derived HydroxyapatiteThis is a xenogenic bone graft substitute, describedas 100 % crystalline, naturally porous, bovinederived hydroxyapatite. The use of this material wasreported in two cases by Callan and Rohrer, in1993(1).
iv) Anorganic bovine bone (ABB)This is also a xenogenic variety, said to containcarbonate apatite. It is defatted and collagen iseluted. Though various studies were conducted byThaller et al in 1993 and 1994 on animal models,there has been no study testing ABB in humanperiodontal defects to date (1).
Risks of disease transmissionTransmission of blood borne and tissue borne
disease has raised concern about allogenic bone graftsubstitutes (1,13). The xenogenic bone has also recentlybeen suspected of potentially transmitting prion diseases.AIDS and Creutzfeldt - Jakob diseases (CJD) are at riskof getting transmitted by allotransplantation and bovinespongiform encephalopathy (BSE) could get transmittedby bovine bone transplantation. Both BSE and CJDbelong to a group of diseases affecting CNS in animalsas well as in humans. Scrapie is the prototype of thesediseases. It affects mainly sheep, while BSE, a newform of prion disease, also known as mad-cow disease,affects bovines. In human CJD, Gerstmann - Straussler

40 Annals of Dentistry, University of Malaya, Vol. 72000
- Sheinker (GSS) disease and Kurv represents the mainform of this disease. These are characterized byexcitability, itching, ataxia, paralysis and death. Thediagnosis of this disease is by autopsy. At autopsy, thebrain show spongiform changes, formation of amyloidplaques and accumulation of abnormal form of hostencoded proteins.
Prevention of CJD transmission:There is not, till date, any marker of CJD
contamination to screen potential donors because onlybrain post mortem biopsy can identify degenerativeencephalopathies (1). Even the most stringent donorscreening cannot assure the exclusion of donors withprepatent CJD. The World Health Organisation(WHO)has recommended 3 methods of sterilization, thoughtotal inactivation is not warranted (1). They are asfollows:
a. Auto claving at 134°C to 138°C for 18 minutes orat 132"C for I hour.
b. Sodium hydroxide solution, IM for I hour at 200e.c. Sodium hypochlorite (at least 2 % of chlorine) for
I hour at 20°C.
Until now no case of CJD transmission via bonederived biomaterial has been reported. However, onehas to bear in mind that the mean latency of appearanceof initial symptoms after iatrogenic CJD transmissionis 59 months.
Prevention of HIV transmission:HIV can be transmitted to patients receiving kidney,
heart and liver transplants, as well as skin grafts andbone grafts. Rigorous screening of potential donors bymedical and social screening, HIV antibody test, HIVantigen test, autopsy and special lymph nodeexaminations is critical. Buck et al 1989, have calculatedthat the risk could be as low as 0.00006% (1). Melloniget al 1992, have demonstrated that HIV infected bonegraft is rendered free of virus contamination after theDFDBA processing (1).
II. Alloplastic Bone Graft Substitutes
A. Calcium phosphate ceramics.The currently used calcium phosphate compounds
are hydroxyapatite (HA) [CalO (P04)6(OH)2] and betatricalcium phosphate (~-TCP) [Ca3)P04)2]. These aresolid biomaterials obtained from powdery phosphates.First, compression with slowly increasing pressurereduces the inter particle spaces, followed by a sinteringprocess at a temperature of 11000 C to 15000 C (Osbornand Newesely , 1980) (1). A porous hydroxyapatite isalso obtained by a hydrothermal exchange process inwhich natural coral calcium carbonate of genus poritesis converted into hydroxyapatite (14).
a. Dense Hydroxyapatite: (HA)The usage of this material has been widespread andthe ultra structural mechanism of bone formationwith various bioceramics implanted in periodontal
tissues has been described. It has been observed thatthe smaller the size of the ceramic, the better thebone formation (15). These biomaterials are nonresorbable bone graft substitutes when used in theirdense polycrystalline form (16). Some biodegradation may Occur when preparation of HAmaterial gives rise to amorphous or porousstructure. Though the clinical use of this materialhas resulted in reduction in probing depth, clinicalattachment gain and partial bone defect resolution,human biopsies have shown no new periodontalattachment, osteogenesis or cementogenesis (1).
b. Porous hydroxyapatite (PHA)Porous hydroxyapatite has shown results similar toDFDBA and FDBA and it has been observedhistologically in humans and animals that PHA isunable to regenerate a connective tissue attachment.Whether PHA is able to enhance bone formation inan orthotopic site is controversial (1,17).
c. ~-Tricalcium phosphate:It is produced from calcium phosphate powdermixed with napthalene, pressed and heated attemperatures as high as 100000 C to 200000 Callowing it to fuse in a solid mass. The napthaleneevaporates, leaving spaces within the ceramic givingrise to a porous structure (1). It is difficult toascertain if ~-TCP is of any benefit in treatingperiodontal osseous defects. Histologically, noosteogenesis or reattachment has been trulydemonstrated (18).
B. Natural Coral Skeleton (NCS) - (Calcium Carbonate)It is a bone graft substitute of a genus porites,
obtained from the Great Barrier Coral Reef in NewCaledonia. After gathering, it is sundried for a fewdays, then organic parts are cleaned by ultrasonictreatment and sterilized in an autoclave at 131°C for60 min. This coral skeleton consists of calciumcarbonate (99%) in the form of arganite, the remainingI % being organic nutrient amino acids. It is porous innature with the average pore diameter of 150 p.m. NCShas no bone inductive potential and the type ofperiodontal regeneration obtained by NCS is unknownas no human histology is available till date (1).
C Polymers:a. PMMA Polymers
This is a bone graft substitute, well tolerated by therecipient site. It is a combination of poly-methylmethacrylate (PMMA) and poly-hydroxyl-ethylmethacrylate (PHEM). The PMMA 550-580 mmdiameter beads are embedded into PHEM andcoated by calcium hydroxide. It has been shown togive favourable results when implanted in intra bonydefects. But histologically, PMMA does notpromote new attachment. PMMA has also beenshown to have no osteoinductive property, but hasbeen shown to possess osteoconductive propertiesin favourable bony defects (1).

b. Resorbable PolyestersThe most commonly used polymers in medicalapplications are the poly hydroxy acids andparticularly polymers with lactic acid (PLA) orglycolic acid (PGA). Many polymers can besynthesized from PLA. PLA and PGA vary incharacteristics. PLA is highly resistant but brittlewhereas PLG/PGA 50:50 posesses high elasticity.It has been observed that these polymers do notseem to be adapted to bone grafting. However theirpotential for bioresorption and ease of handling hasencouraged some authors to use these biomaterialsas carriers for osseopromoting agents or as linkersfor other bone graft substitute. At present they arewidely used as resorbable membranes in guidedtissue regeneration (1).
D. Tetracycline Addition to Bone Graft Substitute:It has been seen that local application of tetracycline
(TTC) or doxycycline, combined with a bone graftsubstitute (FDBA or TCP)enhances bone periodontalregeneration in animal models. It has alsQ beenobserved in humans that the addition of TTC to FDBAalong with systemic administration of TTC enhancesbone formation in juvenile periodontitis. However. itis not· clear if the local application of TTC ordoxycycline along with biomaterials other than FDBAhas the same beneficial effects in adult or rapidlyprogressive periodontitis (1,19).
Fate of Graft Material:Once the material is placed in the bony defect it may
act in a number of ways which may decide the fate ofthe graft material (2,20). The various possibilitiesinclude:
Bone graft material may have no effect at all.The bone graft material may act as a scaffolding
material for the host site to lay new bone.The bone graft material may itself deposit new bone
because of its own viability.
SUMMARY AND CONCLUSION
From this review it is evident that bio materials used'in Periodontics have shown remarkable results ascompared to the simple procedures like open curettage,and flap debridement surgery alone for periodontalosseous defects. At present, barrier techniques toprevent epithelial downgrowth, with or withoutautogenous bone or decalcified freeze-dried boneallograft, are widely used. Coral - derived materials canbe used when non human derived grafts are preferred.Bone substitutes will definitely have an increased roleto play in the future of periodontal regeneration.
REFERENCES
1. Jean-Pirr Olika Youn. Proceedings of the 2nd
European workshop on Periodontics. In Niklous P.
Biomaterials used as bone graft substitutes 41
Lang, ed. Bone grafts and biomaterials used as bonegraft substitutes. Berlin, Quintic ssenz Verlag,1997-313.
2. Polson A.M. Periodontal regneration Current statusand directins. 151 edition; Quintessence publishingCo., Inc 1995, 9-10: 71-112.
3. Grant, Stern, List garten, Periodontics. (Sixthedition). The C.V. Mosby Company 1988; 838-82.
4. Carranza F.A. and Newman M.G. Clinicalperiodontology, eighth edition, W. B. SaundersCompany, 1996; 622-39.
5. Register, A.A. et al. Human bone induction byallogeneic dentin matrix. J Periodontol 1972; 43:459.
6. Dragoo M.R. Clinical and histologic evaluation ofalloplasts and allografts in regenerative periodontalsurgery in humans. Int J Periodont Rest Dent 1983;3(2): 8.
7. Busschop J, and De Boener, J. Clinical andhistologic characteristics of lyophilized allogeneicduramater in periodontal bony defects in humans.J Clin. Periodontol 1982; 9: 141.
8. Klingsberg J, Periodontal scleral grafts andcombined grafts of sclera and bone: two yearappraisal, J Periodontol 1974; 45: 262.
9. Chodroff, R.E. and Ammons, W.F. Periodontalrepair and surgical debridement with and withoutcartilage allografts. J Clin. Periodontol 1984; 11:295.
10. Alderman NE Sterile plaster of Paris as an implantin the infrabony environment. A preliminary study.J Periodontol 1969; 40: 11.
11. Aichelmann - Reidy ME and Yukna R.A. Bonereplacement grafts. The bone substitutes. Dent.Clin. North Am. Advances in Periodontics 1998;Part II 42(3): 491-501.
12. Mellonig, Bowers G.M. Comparison of bone graftmaterials. (Part I) J Periodontol 1981; 52: 291.
13. Sonis T, Williams L, Jeffcoat M. Healing ofspontaneous periodontal defects in dogs treated withxenograft demineralized bone. J Periodontol 1985;56: 470.
14. Strub J.R., Gabertlvelt W. Comparison of tricalcium phosphate and frozen allogenic bone JPeriodontol1979; 50: 627.
15. Zaner D.T. Yukna R.A. Partial size of periodontalgrafting material. J Periodontol 1987; 55: 406.

42 Annals af Dentistry, University af Malaya, Val. 72000
16. Stahl S.S. Frowm S.J Histologic and clinicalresponses to porous hydroxy -lapatite implants inhuman periodontal defects J Periodontol 1981; 54:589-695.
17. Oreameno S, Lekuvic V, Kenney E.B. Comparativeclinical study of porous hydroxyapatite and DFDB.J Periodontol 1990; 61: 399.
18. Shimazaki K. Comparative study of porousHydroxyapatite and Tri calcium phosphate. J ofOrthopedic Research 1985; 3: 301-10.
19. Evan S, Yukna R.A., Sepe W W. Effects of variousgrafts materials with tetracycline in localizedjuvenile periodontitis. J Periodontol 1989; 60: 491.
20. Genco, Goldman, Cohen. Contemporaryperiodontic. 1st Edition. The C.V. Mosby Company,1990; 585-604.