Embed Size (px)
Citation preview

Biomarkers in the Age of Sacubitril/Valsarten
AlanS.MaiselMDFACC
ProfessorofMedicine,Emeritus
UniversityofCalifornia,San
Diego,

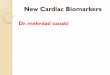
Myocardial injury to the heart (CAD, HTN, CMP, valvular disease)Initial fall in LV performance, ↑ wall stress
Morbidity and mortalityArrhythmiasPump failure
Peripheral vasoconstrictionHemodynamic alterations
Remodeling and progressiveworsening of LV function
Fibrosis, apoptosis,hypertrophy, cellular/molecular alterations,
myotoxicity
Heart failure symptomsFatigue
Activity altered Chest congestion
EdemaShortness of breath
Activation of RAAS and SNS
Neurohormonal Activation inHeart Failure
RAAS = renin-angiotensin-aldosterone system; SNS = sympathetic nervous system;CMP = cardiomyopathy. Fonarow GC. Rev Cardiovasc Med. 2001;2:7-12.

ACC/AHA HF Guidelines 2013:Management of HFrEF (Stage C)
Life-ProlongingMedicalTherapy• ACEinhibitorsorARB(ClassI,evidenceA)inallpatientswithoutcontraindicationsorintolerance.
• Evidence-basedbeta-blockers(ClassI,evidenceA)inallpatientswithoutcontraindicationsorintolerance. Thiswouldincludecarvedilol(immediateorextendedrelease),metoprololsuccinate,orbisoprolol.
• Aldosteroneantagonists(ClassI,evidenceA)inallpatientswithClassII–IVHFwithoutcontraindicationsorintolerancewhenclosemonitoringcanbeensured.
Yancy CW, et al. J Am Coll Cardiol. 2013;62:1495-1539.

Residual Risk for HFrEF Despite Conventional GDMT
In PARADIGM-HF, study patients were followed over a median of 27 months.2,*
*Adult patients with NYHA class II–IV symptoms and an ejection fraction of 40% or less were required to take a stable dose of a beta blocker and an ACE inhibitor (or ARB) equivalent to at least 10 mg of enalapril daily, with most also receiving MRA.
McMurray J, et al. N Engl J Med. 2014;371:993-1004.
Of all patients randomized to enalapril, the absolute risk of CV death as a first event was 10.9% (n=459/4212)1

Sacubitril /ValsartanMechanismofAction

AlanS.MaiselMD,FACC(1) SherylL.Chow,PharmD,FCCP,FAHA,(2)NicholasWettersten,MD (1)NicholasVoldovarPhD(3),Danielle
GualandroMDFACC(4)OlgaBarnettMDPhD(5),MarinNishimuraMD(1),DamienLogeart MD,(6)MicheleSenni,MD,FESC(7)
AlexandreMebazza MD(8)
Biomarkers in the era Era of Sacubiatril/Valsartaen: Diagnosis, Patient Patient Phenotyping and the
prospect of Personalized Therapy

PRE NT-PRO BNP PreproBNP1-134
PRE
NT-PRO BNP proBNP1-108
Cleavage in sarcoplasmic reticulum
Threonine71 Glycosylation
Predominant binding of BNP assay to proBNP
NT-PRO NT-PRO
Current NT-proBNP assays can only bind non-glycosylated fragments, leaving glycosylated fragment, which are higher in chronic heart failure, unmeasured
Cleavage by corinand furin
BNP BNP1-32
NT-proBNP1-76

PARADIGM-HF:NT-proBNP andBNP
0 2 4 6 80
100
200
300
400
500
600
700
800
900
1000
1100
1200
1300
1400
0
50
100
150
200
250
300
350
400
450
500
NT-proB
NPpg
/ml
Months
BNPpg
/ml
LCZ696Enalapril
NT-proBNP
BNP


WhichpeptidewithSacubitril/Valsartan? NT-proBNP?BNP?

BNP
ADD-00056845

Prospective comparison of ARNI with ACEI toDetermine Impact on Global Mortality and
morbidity in Heart Failure trial (PARADIGM-HF)
Sacubitril/Valsartan 97/103 mg twice daily
Enalapril10 mg twice daily
Aim of the PARADIGM-HF Trial
SPECIFICALLY DESIGNED TO REPLACE CURRENT USEOF ACE INHIBITORS AND ANGIOTENSIN RECEPTOR
BLOCKERS AS THE CORNERSTONE OF THETREATMENT OF HEART FAILURE

PARADIGM-HF Trial: DesignEntryCriteria:• NYHAClassII-IVHF,LVEF≤40%→amendedto≤35%• BNP≥150pg/mL(orNT-proBNP≥600pg/mL)or1/3lowerifhospitalizedforHFwithin12mos• OnastabledoseofACEIorARBequivalentto≥10mgofenalaprildailyfor≥4weeks• Unlesscontraindicated,onstabledoseofbeta-blockerfor≥4weeks• SBP≥95mmHg,eGFR≥30mL/min/1.73m2andserumK≤5.4mmol/Latrandomization
Sac/Val = Sacubitril/Valsartan.McMurray JJV, et al. N Engl J Med. 2014;371:993-1004.
34-month follow-up
Single-blind run-in period
HFPatients
(n=8,442)R
Enalapril 10 mg BID(n=4,212)
Sac/Val 97/103 mg BID(n=4,187)
Enalapril 10 mg BID(n=10,513)
Sac/Val49/51 mg to
97/103 mg BID(n=9,419)
2 Weeks 4–6 Weeks
Study stopped early after median follow-up of 27 mos
Primary endpoint: Death from CV causes or hospitalization for HF

Sac/Val(n=4187)
Enalapril(n=4212)
Hazard Ratio(95% CI)
p-Value
Primary endpoint
914(21.8%)
1117(26.5%)
0.80(0.73–0.87) <0.001
Cardiovascular death
558(13.3%)
693(16.5%)
0.80(0.71–0.89) <0.001
Hospitalization for heart failure
537(12.8%)
658(15.6%)
0.79(0.71–0.89) <0.001
Sac/Val = Sacubitril/Valsartan. McMurray JJV, et al. N Engl J Med. 2014;371:993-1004.
PARADIGM-HF: Effect of Sac/Val vs. Enalapril on the Primary Endpoint and Its Components


BNP NTproBNP
TimeAcuteHF AcuteHFSacubitril/
valsartan
100 300
?

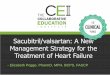
IL-33
ST2L
sST2
Decoy Receptor
Cardiomyocyte
• Increased Fibrosis• Inflammation• Adverse Remodeling• Hypertrophy• Pro-apoptosis • Anti-fibrotic
• Anti-hypetrophy• Reduced apoptosis


19
Figure2.RelationshipsbetweenbaselinesST2concentrationsandclinicaloutcomes

WhyST-2levelsmightbebetterthanNPlevelstofollowpatients
• MuchdaytodayvariabilityofBNP-diureticuse,saltloadfrommeals,timeofblooddraw.
• “wetbnp”changesrapidly- whichmayjustrepresentvolumeandnotremodeling
• DifficulttousewithCKD-• GUIDEITnegative
• Littlevariability• Doesnotseemtobeaffectedbyvolumeasmuch
• NoteffectedbyCKD• ST-2especiallyresponsivetoantifibroticdrugslikeMRAandSacubitril/Valsarten– Dowereallyneeda“GUIDEitlikestudy?
NP sST2

ENTREST2UsingST2levelstostartEntrestoinhighriskpatientscurrentlynoton
thedrug

PatientswithHReEF qualifiedforSacubitril/Valsartenbutnottaking:Feelwellonace/arb,etc
1000Patients
ST-2levelsmeasured
ST2<35ng/mlREGISTRYARM
N=400
Standardcare
Day90&180Patientscontacted
forevents
ST2≥35ng/mlRANDOMIZATIONARM
N=600
UsualCare(N=300)
Day30SafetyLabMonitoring
Day90&180Patientscontacted
forevents
UsualCare+Entresto(N=300)
Day7SafetyLabMonitoring
Day30SafetyLabMonitoring
Day90&180Patientscontacted
forevents
Astartingdoseof24/26mgtwicedailyisrecommendedforpatientsnotcurrentlytakinganACEinhibitororanangiotensinIIreceptorblocker(ARB)andforpatientspreviously takinglowdosesoftheseagents.DoublethedoseofSacubitril/Valsartenevery2to4weekstothetargetmaintenancedoseof97/103mgtwicedaily,astoleratedby thepatient.
SafetyLabMonitoringwithin3-7daysofanydosetitration
orwhenclinicallyindicated
ENTREST2

NatriureticPeptides RecommendationPredischargeBNP/NTproBNP canhelppredictprognosisprognosticate inpatientshospitalizedwithHF.
Inpatientswithhighriskforreadmissions ormortality,uptitration ofGDMTmaybereasonableusingcurrentHF guideline recommendations aswellasincorporatingotherrecommendations fortransitions ofcare.Otherconsiderations includeimplantablehemodynamicmonitoring orreferralforadvancedtherapies.
BNP/NT-proBNPcanbecollectedathospitaladmissionandbeforedischargetodeterminefutureprognosisandstratifyrisk.
Relativechangesinnatriureticpeptidesduringhospitalization canhelptodetermineresponse totherapy(wettoeuvolemic) andprovideimportantprognosticinformation.Furtheradjustmentsinmedications should bebasedoncurrentHFguidelinerecommendations.Inabilitytoreducenatriureticpeptidesmayidentify ahigh-risk populationapproachingend-stageheartfailure.
DifferentialeffectsonfnatriureticpeptideslevelsshouldberecognizedwhenstartinganARNI.
1.BothBNPandNT-ProBNPcanprovide usefulinformationwheninitiatingARNItherapy.A.NT-proBNPisnotdirectlyaffectedbyBNPorNT-NT-proBNP assaysandcanbeusedasamarkertodetectimprovementoffillingpressures andLVstretchovertimewithARNIs.B.BNPcanbemonitoredupto1monthaslevelsriseasaresultofneprilysieninhibition. Levelsareexpectedtodeclineafter1monthasfillingpressure andLVstretchimprovewiththerapyovertime .
ST-2SerialsST-2concentrationsinCHFpatientsmayidentifypatientswhoarehigh-riskfordeathandreadmissionandmaybenefitfromrequireadditionalanti-fibroticintervention.
BasedonGDMT,itisreasonabletoaddorintensify antifibroticmedicationssuchasMRAsorARNIstoreducesST-2< 35ng/mLaccordingtocurrent US HFguidelines .Especially highrisk populations arethosewithrisingsST2levels onrepeatassessment andmaybenefitmostfromintensificationoftherapy.*Atpresent,therearenoprospective datasupporting biomarker-guidedtherapywithsST2.