Embed Size (px)
Citation preview
Biomarkers in OsteoarthritisAli Mobasheri
1The screen versions of these slides have full details of copyright and acknowledgements
1
Biomarkers in Osteoarthritis
Ali Mobasheri, D.Phil. (Oxon)Musculoskeletal Research Group
School of Veterinary Medicine and ScienceFaculty of Medicine and Health Sciences
2
Aim and scope
• The aim of this presentation is to:Provide an overview of current research on osteoarthritis (OA) biomarkers
Highlight the lack of analytical tools and reagents in our toolbox
Discuss the limitations of currently available biomarkers
Explore future opportunities and identify key areas that are relevant to the pharmaceutical product pipeline
3
Overview of presentation
• Summary of the definitions of OA and biomarkers of OA
• Need for a better “gold standard”:Radiography is inadequate
• Recent developments in biomarker definition and classification“Wet” and “dry” biomarkers
• Post-genomic approaches for identification of new OA biomarkers aimed at early (pre-radiographic) identification of disease
• The advent of “combination biomarkers”
Biomarkers in OsteoarthritisAli Mobasheri
2The screen versions of these slides have full details of copyright and acknowledgements
4
Background and context
5
Osteoarthritis (OA)• Most common form of arthritis in humans
and companion animals Major cause of pain, inflammation and loss of mobility
6
Osteoarthritis (OA) (2)
• Characterised by progressive deterioration and loss of articular cartilage
• Affects load-bearing synovial joints
• Associated with ageing and excessive or abnormal joint loading
Biomarkers in OsteoarthritisAli Mobasheri
3The screen versions of these slides have full details of copyright and acknowledgements
7
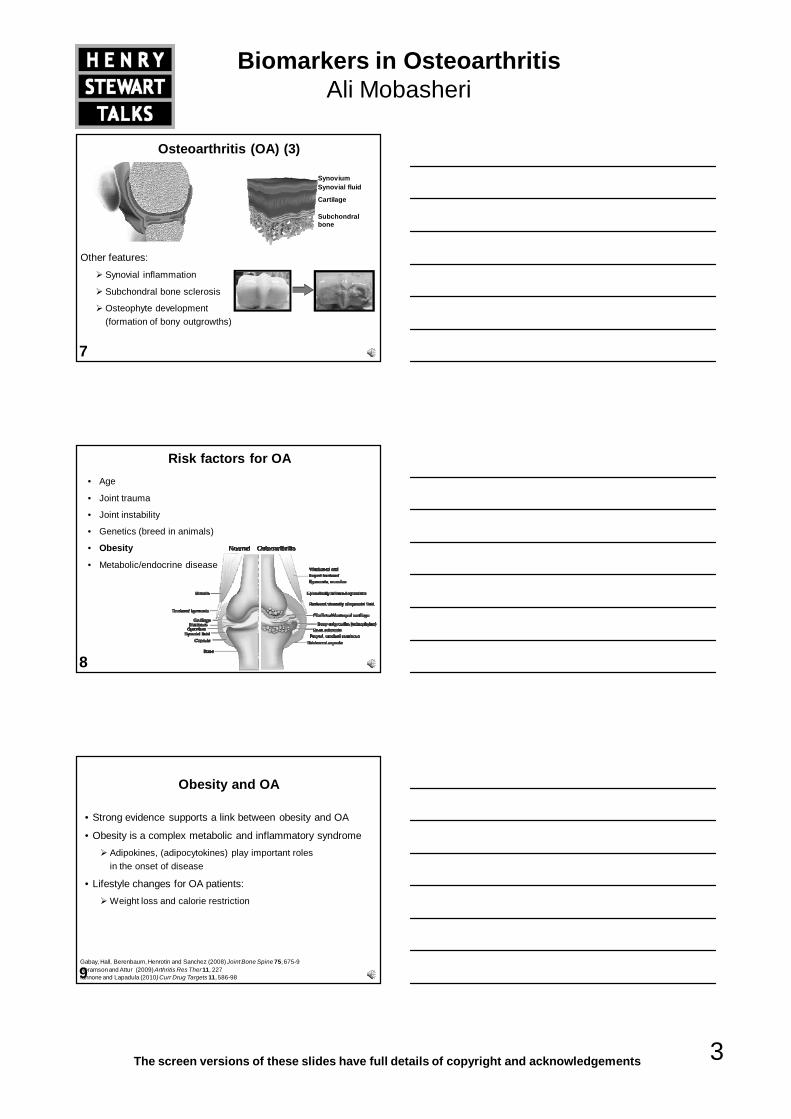
Osteoarthritis (OA) (3)
Other features:Synovial inflammation
Subchondral bone sclerosis
Osteophyte development (formation of bony outgrowths)
SynoviumSynovial fluid
Cartilage
Subchondral bone
8
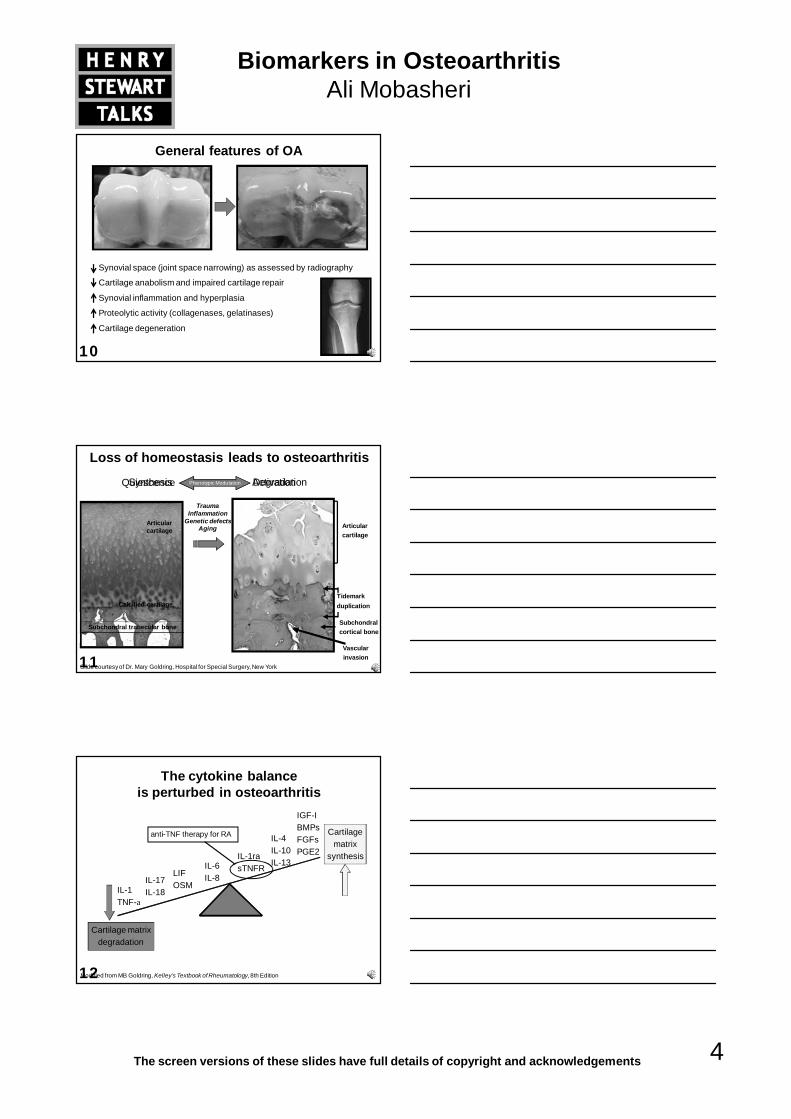
Risk factors for OA• Age
• Joint trauma
• Joint instability
• Genetics (breed in animals)
• Obesity
• Metabolic/endocrine disease
9
Obesity and OA
• Strong evidence supports a link between obesity and OA
• Obesity is a complex metabolic and inflammatory syndrome Adipokines, (adipocytokines) play important rolesin the onset of disease
• Lifestyle changes for OA patients:Weight loss and calorie restriction
Gabay, Hall, Berenbaum, Henrotin and Sanchez (2008) Joint Bone Spine 75, 675-9Abramson and Attur (2009) Arthritis Res Ther 11, 227Iannone and Lapadula (2010) Curr Drug Targets 11, 586-98
Biomarkers in OsteoarthritisAli Mobasheri
4The screen versions of these slides have full details of copyright and acknowledgements
10
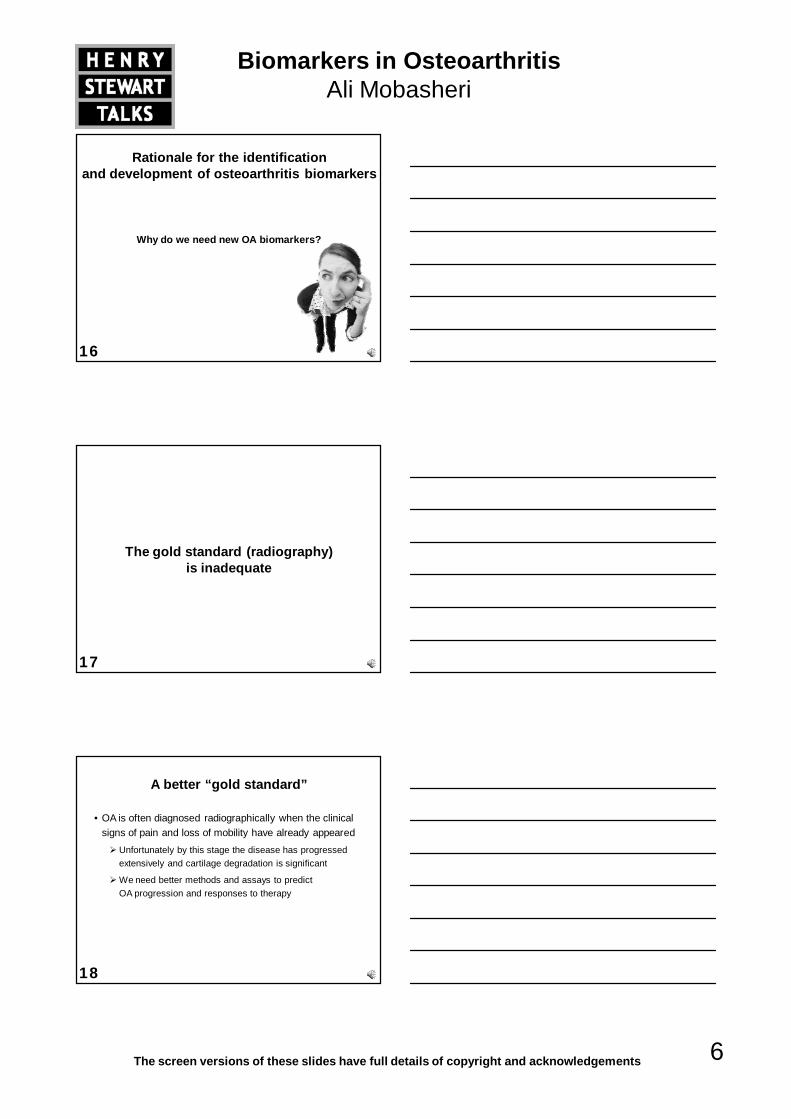
General features of OA
Synovial space (joint space narrowing) as assessed by radiography
Cartilage anabolism and impaired cartilage repair
Synovial inflammation and hyperplasia
Proteolytic activity (collagenases, gelatinases)
Cartilage degeneration
11
Synthesis DegradationPhenotypic ModulationQuiescence Activation
Loss of homeostasis leads to osteoarthritis
TraumaInflammation
Genetic defectsAging
Articular cartilage
Calcified cartilage
Subchondral trabecular bone
Slide courtesy of Dr. Mary Goldring, Hospital for Special Surgery, New York
Articular cartilage
Subchondral cortical bone
Tidemark duplication
Vascular invasion
12
The cytokine balance is perturbed in osteoarthritis
IL-1TNF-a
IL-17IL-18
LIFOSM
IL-6IL-8
IL-1rasTNFR
IL-4IL-10IL-13
IGF-IBMPsFGFsPGE2
Modified from MB Goldring, Kelley’s Textbook of Rheumatology, 8th Edition
Cartilage matrixdegradation
Cartilagematrix
synthesis
anti-TNF therapy for RA
Biomarkers in OsteoarthritisAli Mobasheri
5The screen versions of these slides have full details of copyright and acknowledgements
13Goldring MB, Goldring SR. J Cell Physiol 2007; 213: 626-634
14
Synovial, chondral and subchondral changes in OA
15
Biomarker: definition
• A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention
Biomarkers in OsteoarthritisAli Mobasheri
6The screen versions of these slides have full details of copyright and acknowledgements
16
Rationale for the identification and development of osteoarthritis biomarkers
Why do we need new OA biomarkers?
17
The gold standard (radiography) is inadequate
18
A better “gold standard”
• OA is often diagnosed radiographically when the clinical signs of pain and loss of mobility have already appeared
Unfortunately by this stage the disease has progressed extensively and cartilage degradation is significant
We need better methods and assays to predict OA progression and responses to therapy
Biomarkers in OsteoarthritisAli Mobasheri
7The screen versions of these slides have full details of copyright and acknowledgements
19
Limitations of radiography
• Indirect measure of alterations in articular cartilage
• Fails to measure a dynamic process
• Changes overtime are small, and occur in only a subset (progressors) of patients
• Poor reproducibility
• Poor correlation with joint function and pain
• Numerous other confounders
20
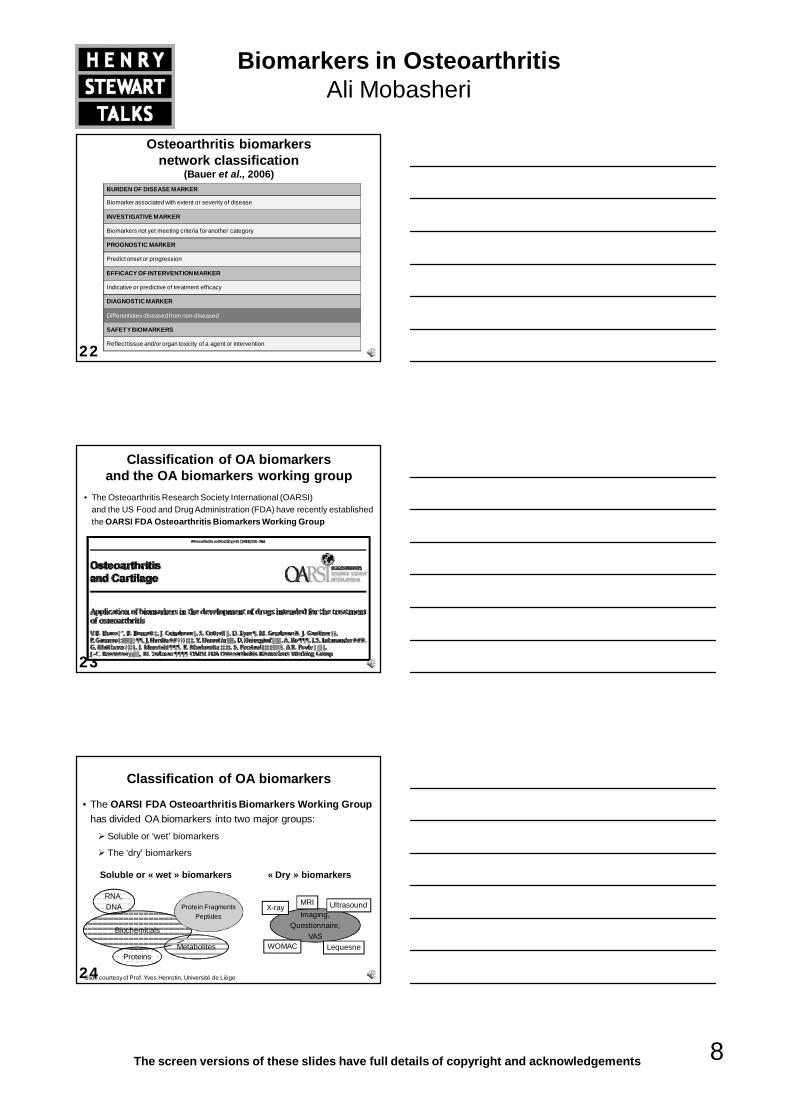
Rationale for identifying early osteoarthritis biomarkers
• Early detection will facilitate earlier diagnosis and treatment because OA which is characterised by a prolonged pre-clinical ‘molecular’ phase, a ‘pre-radiographic’ phase, and a ‘recalcitrant radiographic’ phase by which time there are extensive structural changes to joints along with pain and loss of function
• Biomarkers could provide an early warning of joint degenerationwhich could prompt earlier, more targeted treatment
Osteoarthritis and Cartilage 19 (2011) 515-542
21
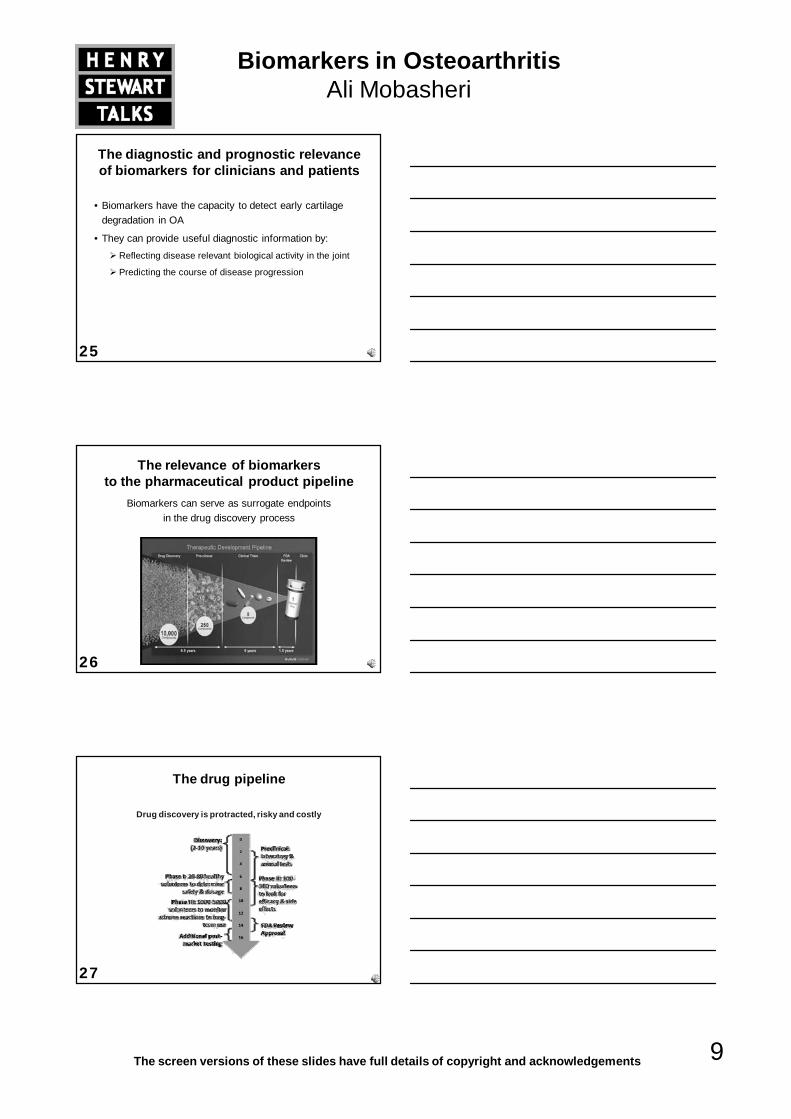
Classification of OA biomarkers: BIPEDs
Safety
Burden of Disease, Investigative, Prognostic,Efficacy of Intervention, Diagnostic, and Safety
Biomarkers in OsteoarthritisAli Mobasheri
8The screen versions of these slides have full details of copyright and acknowledgements
22
Osteoarthritis biomarkers network classification
(Bauer et al., 2006)BURDEN OF DISEASE MARKER
Biomarker associated with extent or severity of disease
INVESTIGATIVE MARKER
Biomarkers not yet meeting criteria for another category
PROGNOSTIC MARKER
Predict onset or progression
EFFICACY OF INTERVENTION MARKER
Indicative or predictive of treatment efficacy
DIAGNOSTIC MARKER
Differentiates diseased from non-diseased
SAFETY BIOMARKERS
Reflect tissue and/or organ toxicity of a agent or intervention
23
Classification of OA biomarkers and the OA biomarkers working group
• The Osteoarthritis Research Society International (OARSI) and the US Food and Drug Administration (FDA) have recently established the OARSI FDA Osteoarthritis Biomarkers Working Group
24
Classification of OA biomarkers
• The OARSI FDA Osteoarthritis Biomarkers Working Group has divided OA biomarkers into two major groups:
Soluble or ‘wet’ biomarkers
The ‘dry’ biomarkers
Biochemicals
RNA, DNA
MetabolitesProteins
Protein FragmentsPeptides
Soluble or « wet » biomarkers
Imaging, Questionnaire,
VAS
X-rayMRI Ultrasound
« Dry » biomarkers
WOMAC Lequesne
Slide courtesy of Prof. Yves Henrotin, Université de Liège
Biomarkers in OsteoarthritisAli Mobasheri
9The screen versions of these slides have full details of copyright and acknowledgements
25
The diagnostic and prognostic relevance of biomarkers for clinicians and patients
• Biomarkers have the capacity to detect early cartilage degradation in OA
• They can provide useful diagnostic information by:Reflecting disease relevant biological activity in the joint
Predicting the course of disease progression
26
The relevance of biomarkers to the pharmaceutical product pipeline
Biomarkers can serve as surrogate endpoints in the drug discovery process
27
The drug pipeline
Drug discovery is protracted, risky and costly
Biomarkers in OsteoarthritisAli Mobasheri
10The screen versions of these slides have full details of copyright and acknowledgements
28
Challenges facing the drug pipeline
• Convoluted – not linear
• “Leaky” – high levels of attrition
• Highly susceptible to the recession
29
The OA drug pipeline
• Currently empty
• Nothing new to offer patients and the OA research community
30
Surrogate OA biomarkers facilitate the drug discovery process
• Linking a biomarker to a clinical endpoint facilitates the drug discovery process
• Qualification is a process applied to a particular biomarker to support its use as a surrogate endpoint in:
Drug discovery and development
Post approval
Regulatory decision making
Biomarkers in OsteoarthritisAli Mobasheri
11The screen versions of these slides have full details of copyright and acknowledgements
31
• Quantifiable decision points – go/no-go decisions
• Use in translational medicine – bridging information
• Early identification of responders & non-responders
• Early quantification of first clinical efficacy
• Identification of those in need of treatment
• Selection of patients most likely to respond
• Dose determination – Phase II
• Safety and efficacy – cost/benefit ratio
• Differentiating compounds from competitors
• Drug repositioning
• Monitoring of patients – compliance
• Personalised health care (PHC)
• Pharmacovigilance
Applying the biochemical marker toolbox in drug discovery and development
Slide courtesy of Dr. Anne-Christine Bay-Jensen, Nordic Bioscience Company
32
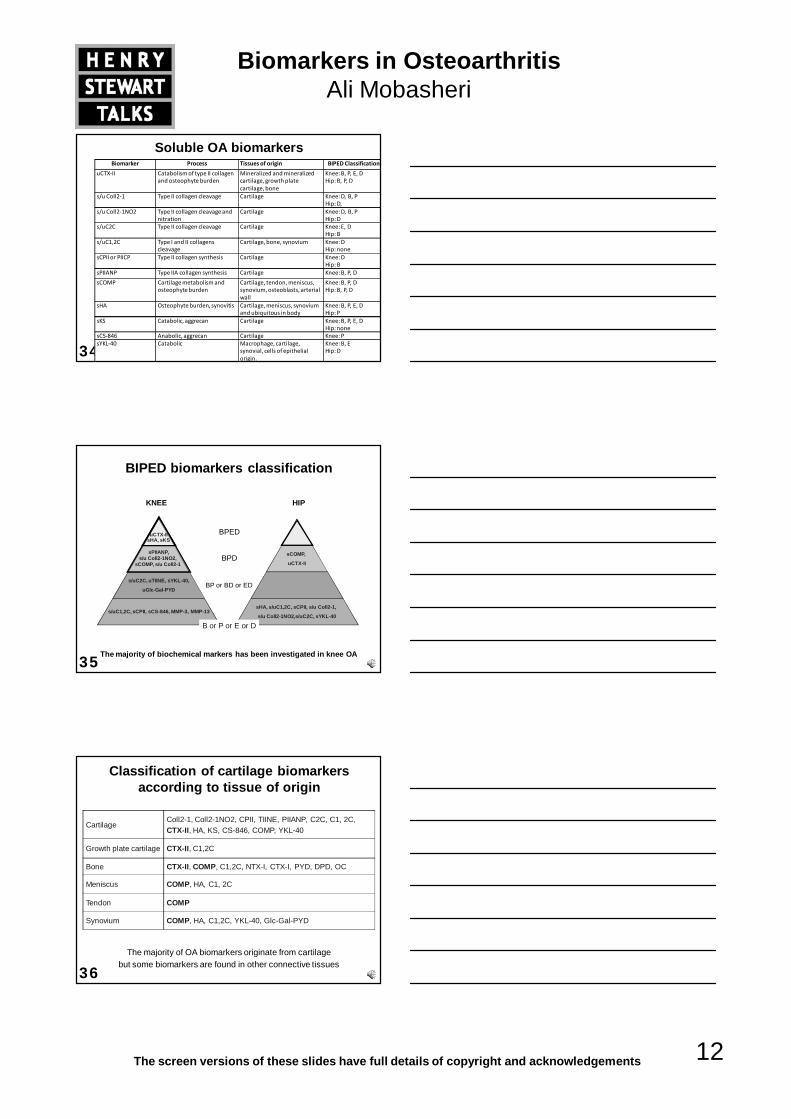
Biomarker Discovery
Verification §
Assay Development and Optimization
Validation ¶
Commercialization
Qualification *
§ Independent scientific and analytical verification of the biomarker – this process involves verification of the analytical performance characteristics and clinical correlation of a biomarker with a biological process or clinical outcome
* Linking a biomarker to a clinical endpoint –Qualification is a process applied to a particular biomarker to support its use as a surrogate endpoint in drug discovery, development or post approval and, where appropriate, in regulatory decision making
¶ Assessing all technical aspects of the biomarker assay
The biomarker pipeline
33
Major classes of OA biomarkers
• Collagenous biomarkersFragments of collagens (particularly type II collagen)
• Non-collagenous biomarkers
Cartilage Oligomeric Matrix Protein (COMP)
• Hyaluronic acid (HA)
• Others:YKL-40 - chitinase 3-like 1 glycoprotein
Biomarkers in OsteoarthritisAli Mobasheri
12The screen versions of these slides have full details of copyright and acknowledgements
34
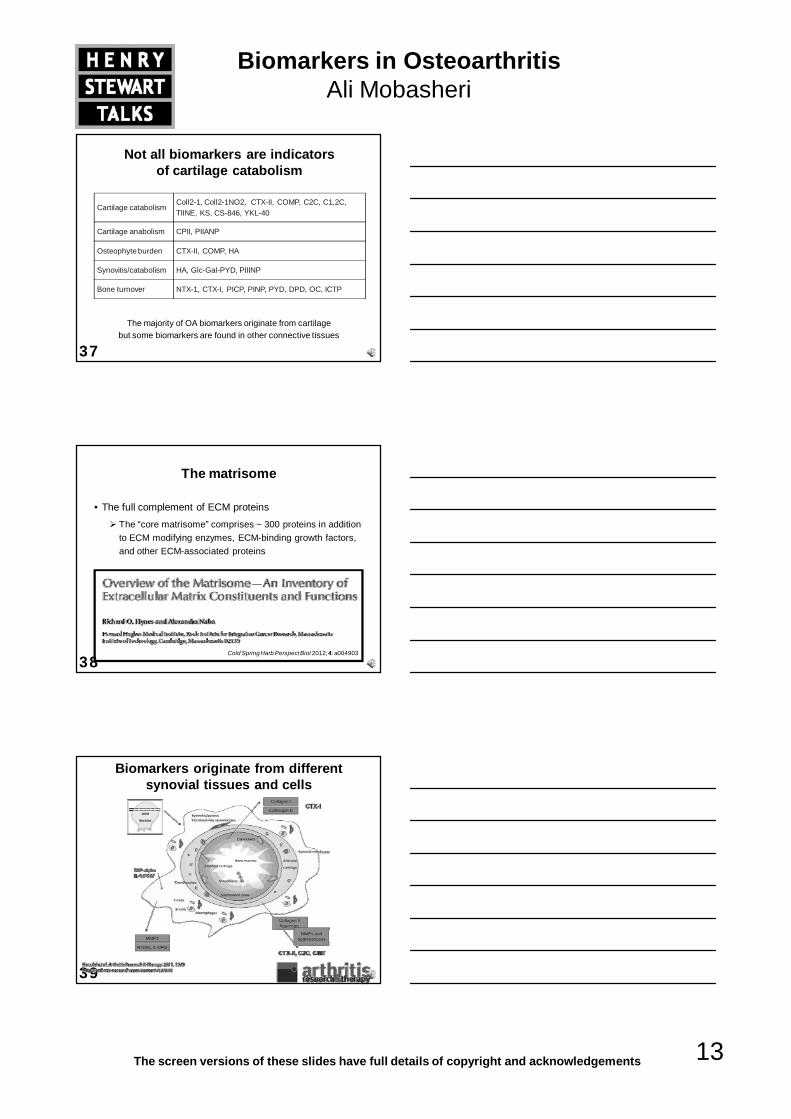
Soluble OA biomarkersBiomarker Process Tissues of origin BIPED Classification
uCTX‐II Catabolism of type II collagen and osteophyte burden
Mineralized and mineralized cartilage, growth plate cartilage, bone
Knee: B, P, E, DHip: B, P, D
s/u Coll2‐1 Type II collagen cleavage Cartilage Knee: D, B, PHip: D,
s/u Coll2‐1NO2 Type II collagen cleavage and nitration
Cartilage Knee: D, B, PHip: D
s/uC2C Type II collagen cleavage Cartilage Knee: E, DHip: B
s/uC1,2C Type I and II collagens cleavage
Cartilage, bone, synovium Knee: DHip: none
sCPII or PIICP Type II collagen synthesis Cartilage Knee: DHip: B
sPIIANP Type IIA collagen synthesis Cartilage Knee: B, P, D
sCOMP Cartilage metabolism and osteophyte burden
Cartilage, tendon, meniscus, synovium, osteoblasts, arterial wall
Knee: B, P, DHip: B, P, D
sHA Osteophyte burden, synovitis Cartilage, meniscus, synovium and ubiquitous in body
Knee: B, P, E, DHip: P
sKS Catabolic, aggrecan Cartilage Knee: B, P, E, DHip: none
sCS‐846 Anabolic, aggrecan Cartilage Knee: PsYKL‐40 Catabolic Macrophage, cartilage,
synovial, cells of epithelial origin.
Knee: B, EHip: D
35
BIPED biomarkers classification
uCTX-IIsHA, sKS
sPIIANP,s/u Coll2-1NO2,
sCOMP, s/u Coll2-1
s/uC2C, uTIINE, sYKL-40,
uGlc-Gal-PYD
s/uC1,2C, sCPII, sCS-846, MMP-3, MMP-13
BPED
BPD
BP or BD or ED
sCOMP,
uCTX-II
sHA, s/uC1,2C, sCPII, s/u Coll2-1,
s/u Coll2-1NO2,s/uC2C, sYKL-40
KNEE HIP
B or P or E or D
The majority of biochemical markers has been investigated in knee OA
36
Classification of cartilage biomarkers according to tissue of origin
The majority of OA biomarkers originate from cartilage but some biomarkers are found in other connective tissues
CartilageColl2-1, Coll2-1NO2, CPII, TIINE, PIIANP, C2C, C1, 2C, CTX-II, HA, KS, CS-846, COMP, YKL-40
Growth plate cartilage CTX-II, C1,2C
Bone CTX-II, COMP, C1,2C, NTX-I, CTX-I, PYD, DPD, OC
Meniscus COMP, HA, C1, 2C
Tendon COMP
Synovium COMP, HA, C1,2C, YKL-40, Glc-Gal-PYD
Biomarkers in OsteoarthritisAli Mobasheri
13The screen versions of these slides have full details of copyright and acknowledgements
37
Not all biomarkers are indicators of cartilage catabolism
The majority of OA biomarkers originate from cartilage but some biomarkers are found in other connective tissues
Cartilage catabolismColl2-1, Coll2-1NO2, CTX-II, COMP, C2C, C1,2C, TIINE, KS, CS-846, YKL-40
Cartilage anabolism CPII, PIIANP
Osteophyte burden CTX-II, COMP, HA
Synovitis/catabolism HA, Glc-Gal-PYD, PIIINP
Bone turnover NTX-1, CTX-I, PICP, PINP, PYD, DPD, OC, ICTP
38
The matrisome
• The full complement of ECM proteinsThe “core matrisome” comprises ~ 300 proteins in addition to ECM modifying enzymes, ECM-binding growth factors, and other ECM-associated proteins
Cold SpringHarb Perspect Biol 2012; 4: a004903
39
Biomarkers originate from different synovial tissues and cells
Biomarkers in OsteoarthritisAli Mobasheri
14The screen versions of these slides have full details of copyright and acknowledgements
40
Proteomic strategies to identify OA biomarkers
41J Proteomics 2012
ECM proteins
Proteins involved in inflammation and the immune response
42
J Proteome Res 2011 Nov 4; 10(11): 5095-101
Complement proteins (alternative pathway)
COMP, Lumican, Tetranectin
Biomarkers in OsteoarthritisAli Mobasheri
15The screen versions of these slides have full details of copyright and acknowledgements
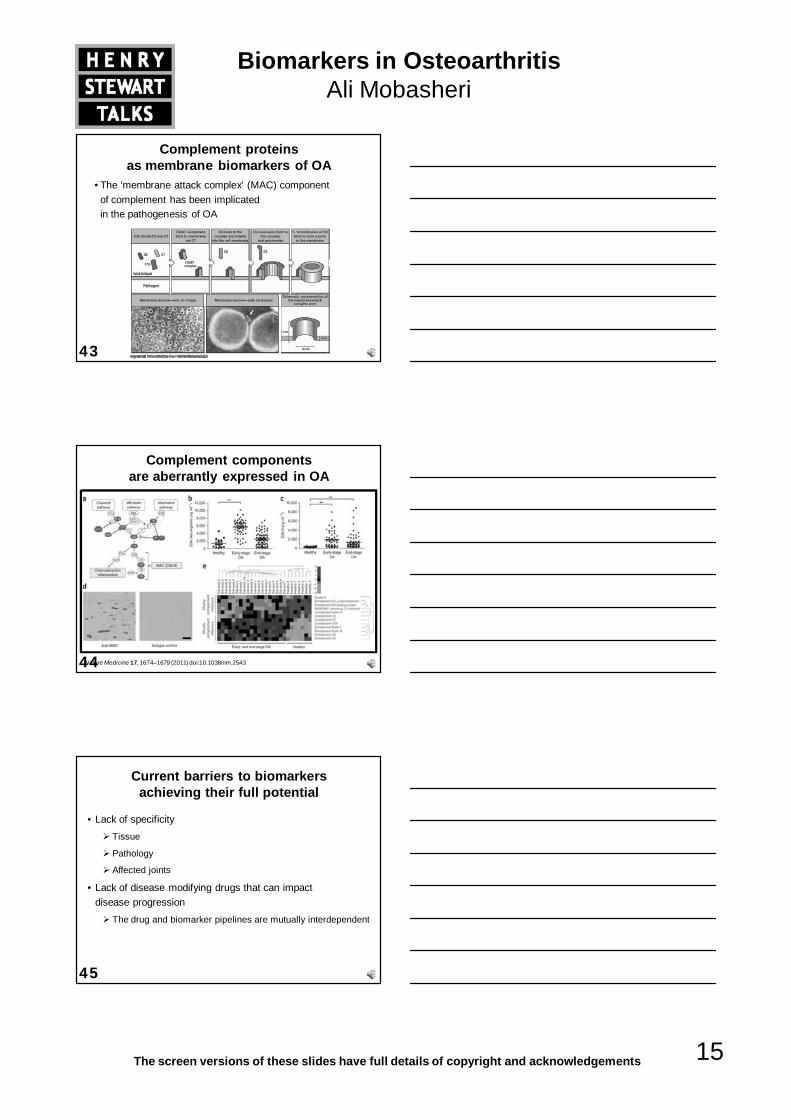
43
Complement proteinsas membrane biomarkers of OA
• The ‘membrane attack complex’ (MAC) component of complement has been implicated in the pathogenesis of OA
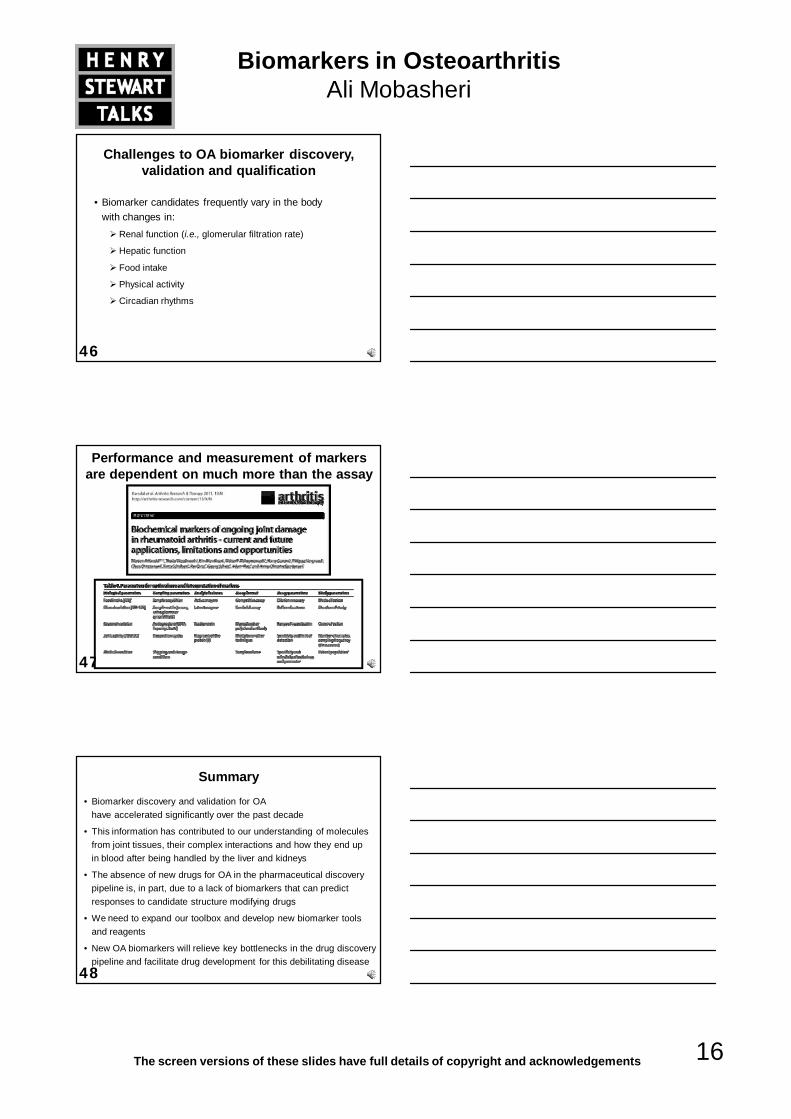
44
Complement components are aberrantly expressed in OA
Nature Medicine 17, 1674–1679 (2011) doi:10.1038/nm.2543
45
Current barriers to biomarkers achieving their full potential
• Lack of specificityTissue
Pathology
Affected joints
• Lack of disease modifying drugs that can impact disease progression
The drug and biomarker pipelines are mutually interdependent
Biomarkers in OsteoarthritisAli Mobasheri
16The screen versions of these slides have full details of copyright and acknowledgements
46
Challenges to OA biomarker discovery, validation and qualification
• Biomarker candidates frequently vary in the body with changes in:
Renal function (i.e., glomerular filtration rate)
Hepatic function
Food intake
Physical activity
Circadian rhythms
47
Performance and measurement of markers are dependent on much more than the assay
48
Summary
• Biomarker discovery and validation for OA have accelerated significantly over the past decade
• This information has contributed to our understanding of molecules from joint tissues, their complex interactions and how they end up in blood after being handled by the liver and kidneys
• The absence of new drugs for OA in the pharmaceutical discovery pipeline is, in part, due to a lack of biomarkers that can predict responses to candidate structure modifying drugs
• We need to expand our toolbox and develop new biomarker tools and reagents
• New OA biomarkers will relieve key bottlenecks in the drug discovery pipeline and facilitate drug development for this debilitating disease
Biomarkers in OsteoarthritisAli Mobasheri
17The screen versions of these slides have full details of copyright and acknowledgements
49
Conclusions
• There are currently no reliable biomarkers for early diagnosis of OA
• The existing biomarkers can only confirm what we know already (i.e., from radiography, the so-called “gold standard”)
• The challenge is to identify sensitive and reliable pre-radiographic markers that can be accurately and reproducibly measured in body fluids
• The assays should be robust and easy to establish in any laboratory
50
Conclusions (2)
• Future research in OA biomarker discovery will need to focus on the identification and validation of panels of protein and/or metabolite biomarkers that correlate with a range of diagnostic imaging techniques such as:
Radiography
Ultrasound
Computed tomography (CT)
Magnetic resonance imaging (MRI)
• Ideally, such biomarkers will serve in non or minimally-invasive, reliable diagnostic and prognostic assays of disease severity and act as reliable monitors of the patient response to a range of different therapies
51
Current progress and existing bottlenecks
• Proteomics is increasingly applied in cartilage biology and pathophysiology and the discovery of novel OA biomarkers
• Many existing biomarkers reflect catabolic and cartilage degradation in the later stages of OA
• Some biomarkers indicate normal cartilage turnover, tissue repair, or ECM remodelling
• We need to be able to discriminate between catabolic and maintenance events
• The definition of ‘biomarker’ will need to reflect these diverse processes and the validation and qualification processes will ultimately depend on the context and specific purpose of their intended applications
Biomarkers in OsteoarthritisAli Mobasheri
18The screen versions of these slides have full details of copyright and acknowledgements
52
Future priorities
• Development of new sophisticated analytical techniques for studying post-translational modifications in ECM molecules in OA
• Expanding the databases to allow detailed bioinformatic studies
Current databases are too small – size matters and small is not beautiful
• Refinement of bioinformatic tools and techniques to “mine” for information in databases
Machine learning
Clustering
Data visualisation
53
Biomarker combinations
• Development of new “combination biomarkers” that include biochemical markers, and imaging markers(i.e., radiographs, MRI)
• OA may be diagnosed better and much more sensitively when two or more biomarkers are assayed and the data combined with one or more imaging modalities (i.e., plain radiograph and MRI)Williams, MK (2009) Biomarkers: in combination they may do better; Arthritis Research & Therapy, 11: 130 doi:10.1186/ar2839
54
Biomarkers of joint overuse and injury
• Joint injuries sustained by athletes are a major risk factor for the development of OA
• Developing biomarkers for monitoring joint overuse and injury in athletes can help monitor responses to different therapies (i.e., corticosteroid, NSAIDs, surgery) and avoid further joint damage associated with overuse injuries
Biomarkers in OsteoarthritisAli Mobasheri
19The screen versions of these slides have full details of copyright and acknowledgements
55
The is in the
Take-home message
We need:• New biomarker targets
• Monoclonal antibodies
• Sensitive biomarker assays
• Affordable diagnostic kits
56
Acknowledgements: funding and collaborators
Dr. Julia Smith
Dr. Susan Liddell
Dr. Jaume Bacardit
Professor Charlie Hodgman
Professor Yves Henrotin
University of Liège, Belgium
The D-BOARD Consortium
57