Embed Size (px)
Citation preview

Biological therapy for the manipulation of complement system
Prohászka Zoltán, IIIrd Department of Medicine, Research LaboratorySemmelweis University

Biological therapy
• Biological therapy refers to the use of medication that is tailored to specifically target an immune mediator of disease or induce an immunological mechanism to cure a disease.
• Targeted therapy in clinical immunology (or oncology) refers to medications acting through specific molecular targets to achieve immunomodulation or oncolysis, in contrast to less specific treatments, like steroids or cytostatica.
• Specific form of targeted therapy is the substitutional therapy with purified „factors”, like coagulation factors in haemophilia, or insulin therapy
• Biological response modifiers (BRMs) are substances influencing biological functions, like interferons, interleukins, growth factors and colony stimulating factors
• Vaccination

Milestones in biological therapy
• Serum therapy for diphtheria (1890)

The first therapeutic approach, that was created with the understanding of the etiopathogensis of disease
Corynebacterium diphtheriae Klebs-Löffler bacillus (1883)
Edwin Klebs 1834-1913
Emil von Behring 1854-1917Nobel Prize in Physiology and Medicine, 1901: Orvosi Nobel díj, 1901: "for his work on serum therapy, especially its application against diphtheria, by which he has opened a new road in the domain of medical science and thereby placed in the hands of the physician a victorious weapon
against illness and deaths". Diphteria antitoxin, 1890
Johannes Bókay Jr 1858-1937„based on an international mandate, he checked the safity of the diphteria antitoxin”1894
Tom, the Horse (1894, London)

Milestones in biological therapy• Serum therapy for diphtheria (1890)• Treatment for agammaglobulinemia with purified immunogobulin G (1952)• The development of monoclonal antibody (mAb) technology by Köhler and
Milstein (1975) leading to the approval of the first therapeutic murine mAb, Muromonab-OKT3 (1986), for the prevention of transplantation rejection.

Niels K Jerne Georges JF Köhler César Milstein
In 1984, the Nobel Prize in Physiology and Medicine was awarded jointly to Niels K. Jerne, Georges J.F. Köhler and César Milstein
"for theories concerning the specificity in development and control of the immune system and the discovery of the principle for production of monoclonal antibodies".

Milestones in biological therapy• Serum therapy for diphtheria (1890)• Treatment for agammaglobulinemia with purified immunogobulin G (1952)• The development of monoclonal antibody (mAb) technology by Köhler and
Milstein (1975) leading to the approval of the first therapeutic murine mAb, Muromonab-OKT3 (1986), for the prevention of transplantation rejection.
• Moreover, the progress of molecular and transgenic technologies has enabled the development of
– chimeric mAb, Abciximab-ReoPro (Gp IIb-IIIa, 1994) and Rituximab-Rituxan (CD20, 1997),
– humanized (complementarity-determining region; CDR-grafted) mAb, Trastuzumab-Herceptin (Her2/Neu, 1998) and Infliximab-Remicade (TNFa, 1998)
– fully human mAb, phage display–derived Adalimumab-Humira (TNFa, 2002) and transgenic mouse-derived Panitumumab-Vectibix (EGFR, 2006)
• The progress of development of these substances has found a niche in the management of various severe diseases, including cancerous, autoimmune and inflammatory syndromes.

8
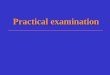
Monoclonal antibody product analysis, historical and forecast sales growth ($m)
0
10,000
20,000
30,000
40,000
50,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Avastin Rituxan Humira Herceptin Remicade bapineuzumab
denosumab Lucentis Erbitux Numax golimumab Tysabri
Xolair Actemra Cimzia Vectibix ocrelizumab Soliris
ustekinumab Synagis pertuzumab Raptiva ReoPro mepolizumab
lumiliximab ipilimumab Humax CD20 galiximab Humax CD20 (I&I) MAB Campath
Aurograb Mylotarg Simulect canakinumab MAB Campath (CNS) Rencarex
Removab Mycograb teplizumab epratuzumab Zevalin Humax CD4
ABT-874 Bexxar Zenapax Humax-EGFR belimumab inotuzumab ozogamicin
Theraloc reslizumab abagovomab Proxinium/Vicinium
0
10,000
20,000
30,000
40,000
50,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Avastin Rituxan Humira Herceptin Remicade bapineuzumab
denosumab Lucentis Erbitux Numax golimumab Tysabri
Xolair Actemra Cimzia Vectibix ocrelizumab Soliris
ustekinumab Synagis pertuzumab Raptiva ReoPro mepolizumab
lumiliximab ipilimumab Humax CD20 galiximab Humax CD20 (I&I) MAB Campath
Aurograb Mylotarg Simulect canakinumab MAB Campath (CNS) Rencarex
Removab Mycograb teplizumab epratuzumab Zevalin Humax CD4
ABT-874 Bexxar Zenapax Humax-EGFR belimumab inotuzumab ozogamicin
Theraloc reslizumab abagovomab Proxinium/Vicinium

9
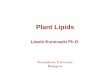
Monoclonal antibody product trends - companies
0
10,000
20,000
30,000
40,000
50,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Genentech Roche Abbott Laboratories Johnson & JohnsonAmgen Schering-Plough Elan AstraZenecaNovartis Wyeth Chugai Biogen IdecMerck KGaA Bristol-Myers Squibb UCB GlaxoSmithKlineAlexion Pharmaceuticals Eli Lilly Bayer Schering Pharma Bristol-Myers Squibb/MedarexMitsubishi Tanabe Eisai Wilex GenmabFresenius/TRION OncoScience/YM BioSciences Ception MenariniViventia
0
10,000
20,000
30,000
40,000
50,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Genentech Roche Abbott Laboratories Johnson & JohnsonAmgen Schering-Plough Elan AstraZenecaNovartis Wyeth Chugai Biogen IdecMerck KGaA Bristol-Myers Squibb UCB GlaxoSmithKlineAlexion Pharmaceuticals Eli Lilly Bayer Schering Pharma Bristol-Myers Squibb/MedarexMitsubishi Tanabe Eisai Wilex GenmabFresenius/TRION OncoScience/YM BioSciences Ception MenariniViventia

Outline of the lecture
• Overview on monoclonal antibodies as therapeutics• Molecular biological technologies to manipulate and
produce human antibody based therapeutics• Examples to highlight the application of biological
therapeutics to manipulate the complement system

The structure of human immunoglobulin G
Heavy chain (H)
Light chain (L)Light chain (L)
• Two light chains/molecule – (kappa or lambda)
• Two heavy chains/molecule – (mu, gamma, delta, alpha
or epsilon
Variable (V) domains(VL and VH domains)
Constant (C) domains (CL, CH1, CH2, CH3)
Antigen binding

Complementarity determining (CDR) and hypervariable regionsin the heavy and light chains

How to produce humanized or human antibodies in large scale?
• The sequence of the variable domains (VH, VL) with the 3+3 hypervariable regions are required – these sequences are unique, and only present in the mature B cells
(after immunization or infectious disease)
• The sequence of the constant domains are also required– Known and available
• Genetic modification of mouse monoclonal antibodies– Chimera production– Humanization
• Production of human antibodies– Hybridoma technology– Antibody (Phage) libraries– Transgenic animals

Induction of anti-mouse immune response in humans„HAMA”: human anti-mouse antibodies•loss of functional activity of the therapeutics•induction of side effects•interference in immunoassays

Single-chain Ab
Production of human antibodies

Engineering of constant domains
• Constant domains determine – The biological functions of the antibodies
• Receptor interactions (Fc receptors)• Complement activation (IgG1: ADCC reaction and CDC)• Neutralization (IgG4)
– In vivo half-life and access to storage pools depends on glycosilation, which is determined by expression/production systems
• Tissue culture: prokaryotes, yeast, insect cells, eukaryote cells• Living organisms: transgenic plants, transgenic animals (secretion
of antibodies to milk, to serum, etc…)
– The compartment of its production • Bloodstream• Milk (secretory component)

Targeting the human complement system by biological therapeutics, examples
• The complement system is a plasma serine protease system, composed by soluble (zymogen) proteases, proteins, humoral regulators, cell-surface regulators and cellular receptors
• It is part of the complex plasma serine protease system, including – Coagulation– Fibrinolysis– Contact (kinin-kallikrein) system– Complement system
• These systems have common activators (injury) and common regulators (protease inhibitors)

Complement system
Innate immunity Clearance Adaptive immunity
•Opsonisation•Lysis of pathogens•Chemotaxis•Inflammation•Activation of target cells
•Immunecomplexes•Apoptotic cells •Necrotic cells
•Augmentation of antibody production•T-cell response•Depletion of self-reacting B-cells•Induction of B-cell memory
Neutrophils
Monocytes
Mast cells
Tissue macrophages
Dendritic cells
B cells
T cells
Key biological functions of complement

Classical pathway (Immunecomplexes)
C3 activation
Alternative pathway (Spontaneous C3 activation)Factor B and Factor D
Lectin pathway (Carbohydrate structures)Alternative pathway
amplificationC3b
C5 activation
C5-C9Terminal Pathway
OpsonizationAntigen presentationAntibody production
Anaphylatoxins C3a, C5aInflammationChemotaxis
LysisCellular damages
Induction of apoptosis
Regulators: MCP, CD59, DAF, Factor H and Factor I
Regulators: C1-inhibitor, C4-binding protein, Factor I
Regulators: S protein and Clusterin
Schematic presentation of the complement system

Complement related human pathologies
• Deficiency (genetic or acquired)– C1-inhibitor (hereditary angioedema)– Alternative pathway regulators (Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic
Uremic Syndrome, )– Terminal pathway components (meningitis)
• Pathological activation– Autoimmune diseases (immunecomplex diseases)– Transplant rejection– Ischemia/reperfusion (stroke, myocardial infarction, etc…)– Hemodialysis, on-pump cardiac operation
• Dysregulated activation and consumption– Sepsis– Pathological pregnancies, preeclampsia, HELLP syndrome, DIC
• Complement related biological therapies– Substitution of deficient factor/protein– Non-specific inhibition of pathological activation– Targeted inhibition of complement activation

Regulators: MCP, CD59, DAF, Factor H and Factor I
Classical pathway (Immuncomplexes)
C3 activation
Alternative pathway (Spontaneous C3 activation)Factor B and Factor D
Lectin pathway (Carbohydrate strucutures)Alternative pathway
amplificationC3b
C5 activation
C5-C9Terminal Pathway
OpsonizationAntigen presentationAntibody production
Anaphylatoxins C3a, C5aInflammationChemotaxis
LysisCellular damages
Induction of apoptosis
Regulators: C1-inhibitor, C4-binding protein, Factor I
Regulators: S protein and Clusterin
Substitution therapy for HAE with C1-deficiency
•Life-threatening edematous attacks (Bradikinin overproduction)•Acute treatment with C1-inhibitor concentrate•Purified human C1-inhibitor
•Cetor/Sanquin or Berinert P/Behring•Nanofiltrated Cinryze/ViroPharma (4th most expensive drug, 350.000 $/year
•Recombinant human C1-inhibitor•Rhucin/Pharming

Classical pathway (Immunecomplexes)
C3 activation
Alternative pathway (Spontaneous C3 activation)Factor B and Factor D
Lectin pathway (Carbohydrate structures)Alternative pathway
amplificationC3b
C5 activation
C5-C9Terminal Pathway
OpsonizationAntigen presentationAntibody production
sCR1 (soluble complement receptor 1)
Anaphylatoxins C3a, C5aInflammationChemotaxis
LysisCellular damages
Induction of apoptosis
Regulators: C1-inhibitor, C4-binding protein, Factor I
Regulators: S protein and Clusterin
Inhibition of pathological complement activation
Regulators: MCP, CD59, DAF, Factor H and Factor I
•Inhibition of complement activation on multiple levels•Aimed to be used in I/R injury situation, i.e. by-pass operation•Lack of breakthrough results with this drug

Classical pathway (Immunecomplexes)
C3 activation
Alternative pathway (Spontaneous C3 activation)Factor B and Factor D
Lectin pathway (Carbohydrate structures)Alternative pathway
amplificationC3b
C5 activation
C5-C9Terminal Pathway
OpsonizationAntigen presentationAntibody production
Eculizumab (humanized murine anti-C5 Ab)1st most expensive drug, 409.500 $/year
Pexelizumab (scV anti-C5 Ab)Anaphylatoxins C3a, C5a
InflammationChemotaxis
LysisCellular damages
Induction of apoptosis
Regulators: C1-inhibitor, C4-binding protein, Factor I
Y
Regulators: S protein and Clusterin
Inhibition of pathological complement activation
Regulators: MCP, CD59, DAF, Factor H and Factor I
IgG4

Current on-label indication and off-label applications for Eculizumab
• On-label: Paroxysmal Nocturnal Hemoglobinuria (PNH)– Disease of hemopoetic stem cells (clonal deletion of GPI-anchor for receptors, including
complement regulators CD59 and DAF)
– Red blood cells are susceptible to episodic hemolysis mediated by complement
– Chronic, progressive disease with recurrent thrombosis and organ-ischemia
– Current management: regular transfusions, anticoagulation, bone-marrow transplantation, and since 2007 targeted therapy with Eculizumab
• Off-label applications: Current clinical trials with Eculizumab– Atypical hemolytic uremic syndrome
– Age-related macular degenration
– Complement-mediated injury after kidney transplantation
– Dense-deposit disease, C3-nephropathy
– Neuromyelitis optica
– Catastrophic Antiphospholipid syndrome
– Cold-agglutinin disease
– ANCA-vasculitis
– Sickle-cell disease

A simplified overview on the classification of thrombotic microangiopathies (based on Besbas et al., 2006, Kidney Int.)
• Advanced etiology, no underlying disease– Infections
• Shiga-like toxin producing pathogens• Neuraminidase producing pathogens
– Complement dysregulation• Alternative pathway dysregultaion• Thrombomodulin mutation
– Failure of von-Willebrand factor processing• Acquired ADAMTS13 inhibitory antibodies• Congenital defect of ADAMTS13 protease
– (Upshaw-Schülman sy)
• Secondary forms, underlying diseases
Typical clinical presentation
• Acute renal failure, HUS• Critically ill, HUS
• Acute renal failure, HUS
• Acute neurological symptoms, TTP
• TMA as severe complication

Laboratory tests currently used for the work-up of patients with clinical TMA in our laboratory
• Advanced etiology, no underlying disease
– Infections• Shiga-like toxin producing pathogens• Neuraminidase producing pathogens
– Complement dysregulation• Alternative pathway dysregultaion• Thrombomodulin mutation
– Failure of von-Willebrand factor processing
• Acquired ADAMTS13 inhibitory antibodies• Congenital defect of ADAMTS13 protease
– (Upshaw-Schülman sy)
• Secondary forms
• Functional complement measurements– CH50 and WIELISA-ALT
• Complement protein determination– C3, C4, FH, FB, FI
• Mutation screening– CFH exons 2, 4, 6, 9 14-15, 17, 18, 20-
23– CFI exons 3, 5-6, 9-10, 12-13– CD46 exons 5-6– C3 exons 14, 20, 26-27, 37– CFB exons 6-7– THBD in progress
• Haplotype analysis– CFH tag SNPs– MCP tag SNPs
• Copy number determination on 1q32 (MLPA)
• Screening for autoimmune form of aHUS (anti-Factor H IgG)

Episodic occurence of disease shub(hemolysis with fragmented erythrocytes, LDH increase , low platelet count)
Plasma exchange
ImmunosuppressionCytostatica
Therapy:
ESRD, dialysis, tx
Eculizumab900 mg/week for 4 weeks,thereafter 1200 mg/two weeks
Current and future therapeutic options for patients with aHUS

The autoimmune form of atypical HUS(Biologicals for the treatment of autoimmune disease)
• Presence of pathogenic autoantibodies against factor H – Linked to CFHR1-3 deletion
– Binding to the functionally active N-terminal part of the molcule
– Inhibition of the complement regulating activity of FH
• Specific therapeutic approach: inhibition of autoantibody production by the depletion of B-cells

Rituximab (Rituxan, MabThera)• Anti-CD20 monclonal antibody (human-mouse chimera) developed to deplete B-cells (treatment of lymphomas and
leukemias)• The ligand of CD20 is unknown, the molecule is involved in the regulation of calcium flux • The mechanisms of action are: induction of ADCC reaction, of complement dependent cytotoxicity, and of apoptosis;
and saturation of Fc receptors• Recently, the drug found its way to treat diseases characterized by hyperactive B-cells, producing autoantibodies• One treatment cycle (4 doses of 375 mg/m2, 1 each week) depletes CD20-pos B cells from the periphery for ~2 years

CD20-positive B-cell depletion in autoimmune diseases
• Rheumatological diseases– Rheumatoid arthritis– Systemic lupus erythematosus (SLE)– Sjögren’s syndrome– Dermatomyositis and polymyositis– Vasculitides
• Non-rheumatological autoimmune diseases– Idiopathic thrombocytopenic purpura (ITP)– Thrombotic thrombocytopenic purpura (TTP)– Autoimmune hemolytic anaemia (AIHA)– Pemphigus vulgaris and foliaceus
Perosa et al, J Intern Med, 2010

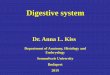
0,00
50,00
100,00
150,00
200,00
250,00
0,00
50,00
100,00
150,00
200,00
250,00
300,00
RR syst
RR diast
plt
Hgb
Hgmm
109 /l
g/l
Feresis
IVIG
Sectio
Curetta
ge
Hyste
rect
.
Haem
atom
a
eva
c.
Madách K és mtsai: Aneszteziológia és Intenzív Terápia, 2008; 38(1): 34-38
Diagnosis of TTP

Mechanisms of action of IVIG in autoimmune and inflammatory diseases
• Blockade of Fc receptors on macrophages of the reticuloendothelial system of liver and spleen
• Restoration of the idiotypic–anti-idiotypic network
• Suppression or neutralization of cytokines by specific antibodies in the IVIG
• Blockage of binding of adhesion molecules on leukocytes to vascular endothelium
• Inhibition of complement uptake on target tissues
• Neutralization of microbial toxins
• Saturation of the FcRn receptors to enhance the clearance of autoantibodies
• Induction of inhibitory FcgRIIb receptors on effector macrophages
• Neutralization of growth factors for B cells, such as B-cell activating factor
• Inhibition of T cell–proliferative responses
• Expansion, activation, or both of a population of Treg cells
• Inhibition of the differentiation and maturation of dendritic cells
Ballow M, JACI, 2011

Mechanisms of action of intravenous immune globulin (IgIV) on the immune modulation of various components of the innate and adaptive immune systems. (Adapted from Tha-In et al. Trend Immunol, 2008) DC, Dendritic cell; Mo, monocyte; NK, natural killer.

Take home messages• Biological therapy, 2011: 29 companies, 52 products, several
hundreds of indications, 40 milliard US dollars annual turnover• Several diseases, that were untreatable or treatable but only in non-
specific manner, are now efficiently cured or treated• Based on continuous product development, there is
– increased efficacy (engineering of biological effects)– decreased side-effects of novel products (100% human antibodies)
• Drugs, currently in clinical practice are increasingly used off-label, and this will soon result in broadening of the field of indications – rituximab for autoimmune diseases
• Alternative applications of different preparations for substitution therapies is also spreading– IVIG for modulation of autoimmunity and inflammation
• The appearance of generic drugs will also arrive soon (for rituximab: 1997+15=2012)– Biosimilarity, in contrast to bioequivalency