Embed Size (px)
Citation preview
J Occup Health 2005; 47: 22–48Journal of
Occupational Health
Biological Monitoring of Exposure: Trends and Key Developments
Marek JAKUBOWSKI and Malgorzata TRZCINKA-OCHOCKA
Nofer Institute of Occupational Medicine, Poland
Abstract: Biological Monitoring of Exposure:Trends and Key Developments: Marek JAKUBOWSKI,et al. Nofer Institute of Occupational Medicine,Poland—The concept of biological monitoring (BM) hasgained the special interest of individual scientists andinternational organizations. Today, when analyticalproblems have almost ceased due to new laboratorytechniques and quality assurance systems, themethods for interpretation of results have become themost important issue. There are importantdiscrepancies regarding the role of biological monitoringof occupational exposure between Europe and theUnited States. BM has been an important tool ofmedical health surveillance in the European countries.In the United States it belongs rather to the field ofoccupational hygiene. It seems that both theapproaches can be accepted. More attention shouldbe paid to the development of the truly health-basedbiomarkers of exposure based on the dose-effect anddose-response relationships. New areas of applicationof BM of occupational exposure include determinationof DNA and protein adducts, unchanged volatile organiccompounds in urine, monitoring of exposure topesticides, antineoplastic drugs, hard metals, andpolycyclic aromatic hydrocarbons. In the generalenvironment BM is the most valuable tool for acquiringknowledge of current levels of internal exposure toxenobiotics, identifying the hot spots and developmentsin trends of exposure. BM can provide policy makerswith more accurate information on the control measuresundertaken. At present, the main areas include heavymetals, persistent organic pollutants and pesticides.BM of chemical exposure has become increasinglyimportant in the assessment of the health risk inoccupational and environmental medicine. Thereforeit would be worthwhile to include BM in the curriculafor the training of occupational hygienists.(J Occup Health 2005; 47: 22–48)
Key words: Biological monitoring, Occupationalexposure, Environmental exposure
Received July 14, 2004; Accepted Oct 29, 2004Correspondence to: M. Jakubowski, Nofer Institute ofOccupational Medicine, 8 Teresy St., 90-950 Lodz, Poland(e-mail: [email protected])
The view has been commonly shared among scientiststhat the likelihood of adverse health effect(s) of exposureto chemicals depends on its magnitude. Measures ofexposure have been developed independently in variousareas of environmental toxicology. Therefore,environmental toxicologists have worked out proceduresfor the risk assessment of adverse health effects that werebased on the daily intake of a given chemical. Thereference values, such as the reference dose (RfD)published by the Environmental Protection Agency (USA)(US EPA), or the Provisionally Tolerated Weekly Intake(PTWI) published by the World Health Organization—Food and Agricultural Organization (WHO-FAO), reflectthe levels of exposure that should prevent humans fromsuffering adverse effects of environmental exposure.Moreover, guidelines for the concentrations of chemicalsubstances in the air or drinking water are also publishedby international organizations1, 2) or local authorities indifferent countries. Industrial toxicologists havedeveloped guidelines for interpreting the concentrationsof chemicals in the air of industrial enterprises. Thesevalues have been published either as recommendations3, 4)
or as official lists of admissible concentrations.The setting of acceptable exposure limits is based on
the assumption that there is no appreciable risk at levelsbelow these limits for all or almost all the personsexposed. Although the recommended daily intake oradmissible concentration in environmental media or inthe workplace atmosphere have been commonly used andaccepted at the governmental level in different countries,it has become clear that various factors can affectexposure. These include additional absorption throughthe skin; differences in individual uptake which can, forinstance, be age-dependent; differences in individualbehavior in the general environment and poor workingpractice; different uptake at the same air concentrations,due to different workload during the shift; and the useand effectiveness of personal protection devices.
In view of the possible influence of these individualfactors, the concept of biological monitoring of exposurewas developed in the mid fifties5, 6) of the 20th cent. Thisconcept originates from industrial toxicology as a method
Review

23Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
for estimating individual exposure to single compounds,but the researchers noted that large individual variationin results could be found for the same exposure levels.This variation was on the one hand due to the impact ofsome physiological factors, and on the other, to the lowprecision of measurements carried out in the past. Totake account of both these factors, the idea of collectiveexposure tests was put forward. Then the concept ofbiological monitoring started gaining interest amongindividual scientists and international organizations.Apart from a large number of reports on the results ofstudies employing biological monitoring, there weremany articles7–13) as well as textbooks14–19) on the generalaspects of the method. The complete scientificdocumentation of Biological Exposure Indices (BEI) inthe USA20) and Biologische Arbeitstofftoleranzwerte(BAT) values21–23) in Germany is available.
Biological monitoring of exposure is presently appliedto environmental and occupational toxicology as well asepidemiological studies on the dose-response relationshipbetween internal exposure and adverse health effects ofexposure to chemicals.
The aim of the present paper is to evaluate:1. The usefulness of available biomarkers for occupational
exposure assessment, taking account of the decreasingtrend in occupational exposure levels.
2.The usefulness of biological monitoring forenvironmental exposure assessment
3. Identification of the new biomarkers of exposure.4. Interlaboratory quality assurance systems and reference
materials for daily quality control within the laboratory.
Definitions
Exposure assessment can be performed with ambientair monitoring and biological monitoring. The term‘biomarker’ is a general term for specific measurementsof an interaction between a biological system and anenvironmental agent. According to the InternationalProgram of Chemical Safety (IPCS)24), three classes ofbiomarkers can be identified:
biomarker of exposure—an exogenous substance orits metabolite or the product of an interaction between axenobiotic agent and some target molecule or cell that ismeasured in a compartment within an organism;
biomarker of effect—a measurable biochemical,physiological, behavioral or other alteration within anorganism that, depending on the magnitude, can berecognized as associated with an established or possiblehealth impairment or disease;
biomarker of susceptibility—an indicator of an inherentor acquired ability of an organism to respond to thechallenge of exposure to a specific xenobiotic substance.
It has been commonly accepted that determining thefirst two kinds of biomarkers can be recognized as a partof more complex prophylactic activities in the
occupational setting. However, the practical applicationof biomarkers of susceptibility at present gives rise toserious doubts. Genetic screening can be applied both asan indicator of susceptibility to occupational hazards ora predictor of future health. Inborn genetic characteristicsthat determine the relatively increased susceptibility toparticular diseases include the host characteristics thatmodify the effect of exposure to environmental agents(genes affecting the metabolic capacity and repaircapacity e.g. cytochrome P450, glutathione S-transferase,N-acetyltransferase), host susceptibility to occupationaldiseases e.g. chronic beryllium disease, occupationalasthma, or susceptibility to diseases that are not relatedto work but affect the rate of absence. Consequently, anemployer might wish to use such information to deployworkers in the areas appropriate to their particular geneticmake-up or to exclude them from employment.
Testing genetic susceptibility for the prevention ofoccupational diseases is, at present, likely to be irrelevantdue to its low predictive value. According to the opinionexpressed by the European Group on Ethics in Scienceand New Technologies to the European Commission on28 July 200325): “The legitimate duties and rights ofemployers concerning the protection of health and theassessment of ability can be fulfilled through medicalexamination but without performing genetic screening.Thus, employers should not in general perform geneticscreening or ask employees to undergo tests”.
In view of the above, the biomarkers of susceptibilitywill not be discussed in the present paper.
According to the review undertaken by the ScientificCommittee on Occupational Exposure Limits (SCOEL),the biological monitoring (BM) methods that are currentlyused to assess workplace exposure fall into three maincategories26):· determination of a substance or its metabolite in a
biological medium (biological exposure monitoring)· measurement of reversible, non-adverse biological
effects (biological effects monitoring)· measurement of the amount of substance interacting
with a target (biological monitoring of effective dose)
The present application of biomarkers ofoccupational exposure
The concept of BM has been given specialconsideration on the part of individual scientists andinternational organizations. The biological monitoringof exposure thus far has been applied to environmentaland occupational toxicology as well as epidemiologicalstudies to evaluate the dose-response relationship betweeninternal exposure and adverse health effects of exposureto chemicals.
Presently, biological monitoring plays but acomplementary role in industrial hygiene practice. Thereare several reasons for that. Firstly, this attitude used to

24 J Occup Health, Vol. 47, 2005
be commonly accepted as something obvious. Then BMwas thought to be more expensive than environmentalmonitoring (EM), the worker could not, for ethicalreasons, serve as an individual sampler, and the collectionof blood samples has not been generally approved.
Moreover, it is not clear whether BM actually belongsto occupational hygiene or occupational medicine.Consequently, BM recommendations are not consideredto represent legal standards, as is the case of EM in mostcountries.
Today, when the analytical problems have almostceased due to new laboratory techniques and qualityassurance systems, the methods for interpretation ofresults have become the most important issue. And theseare much more difficult to understand for the legislativebodies than the methods used in environmentalmonitoring where the rules are relatively simple.
The problem of the selection of a sampling strategy ismuch more difficult than in EM because of the differenttoxicokinetics of unchanged compounds and theirmetabolites in different media (blood, urine, exhaled air).There are also problems in expressing the results ofdeterminations of chemical substances or theirmetabolites excreted in urine (these can be calculated forcreatinine, specific gravity or rate of excretion).
There are two basic ways that the data for interpretationcan be obtained. They can be either health-based orconstitute an equivalent to the air concentration of a givenchemical. The latter can be gained as the outcomes of ahuman volunteer study under controlled experimentalconditions or of a field study where the workload and thepossible additional absorption through the skin aredifficult to control.
The true health-based values have been obtained mostlyvia epidemiologic studies, on the basis of the dose-effector dose-response relationships. These values make itpossible to directly evaluate the health risk based on thedetermination of chemical agents or their metabolites inbiological material. These are the most valuableindicators. Unfortunately, in occupational exposure theirnumber is limited to lead in blood, cadmium in bloodand urine, mercury in urine, fluorides in urine,carboxyhemoglobine, methemoglobine, and the decreasein cholinesterase activity in erythrocytes, and to someextent also the arsenic concentration in urine.
The American Conference of Governmental IndustrialH y g i e n i s t s ( A C G I H ) a n d t h e D e u t s c h eForschungsgemeinschaft (DFG), the two mainorganizations involved in the setting of BM referencevalues differ in their approach to and definitions of thesevalues.
ACGIH BEI values represent the levels of analytesthat are most likely to be observed in specimens collectedfrom a healthy worker who has been exposed to chemicalsto the same extent as a worker with inhalation exposure
at the TLV (Threshold Limit Value) level. BEIs areunderstood as advisory levels that may be exceeded byindividuals in the observed group. Industrial hygienistsare expected to reduce the exposure if BEI values areexceeded for a longer period of time or if a BEI isexceeded for a substantial group within the exposedpopulation. ACGIH3) has already published BEI valuesfor 37 substances or groups of substances.
The DFG BAT values are defined as “the maximumpermissible quantity of a chemical substance or itsmetabolites, or the maximum possible deviation from thenorm for biological parameters induced by thesesubstances in exposed humans. The BAT values areconsidered the ceiling values for healthy individuals”.They are intended to protect the workers from work-related health impairments. DFG has so far determinedBAT values for 50 substances or groups of substances.For 14 carcinogenic substances, exposure equivalents forcarcinogenic materials (EKA) have been established4).
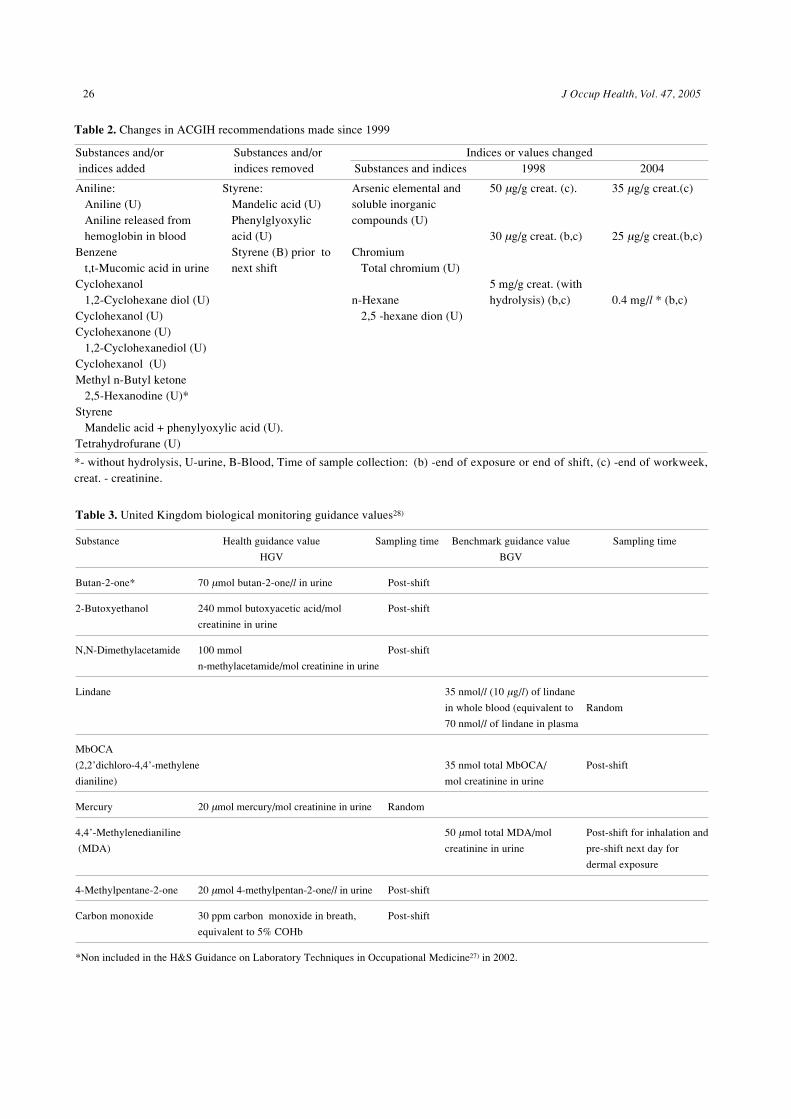
Previously, an analysis of the criteria for biologicallimit values developed in Germany and the US and acomparison of the BEI and BAT values was undertakenby Morgan and Schaller13). The changes in the BAT andBEI values that have been made since the latterpublication are shown in Tables 1 and 2. According tothese data, both DFG and ACGIH were very active in thefield of BM and these activities were aimed at extendingthe respective lists as well as updating the existing values.As regards the ACGIH listing, the most important changesrefer to n-hexane and methyl n-butyl ketone, where thespecific determination of 2,5-hexanodione withouthydrolysis made it possible to eliminate the influence ofbackground levels, as well as styrene, for which thenumber of parameters has been considerably reduced. Inthe DFG classification, 24 new substances have beenadded (e.g. manganese) and what is important the BATfor lead in blood (Pb-B) has been reduced from 700 µg/lto 400 µg/l for men and from 300 µg/l to 100 µg/l forwomen <45 yr old.
There are 33 compounds with BAT values that are notincluded in the BEI list. Only three compounds haveBEI values without a counterpart in the BAT list. In manycases, there are discrepancies between the exposureindices recommended by these two organizations.Moreover, different concentrations in biological materialhave been recommended for the same indices.
In the United Kingdom (UK), biological exposureindices have been established for 64 compounds. Theyare based mostly on the ACGIH values but six of themwere proposed by the UK Health and Safety Executive27)
(Table 3). These belong to the health guidance values(HGV) and the benchmark guidance values (BGV). Thehealth guidance values are set at a level at which there isno indication from the scientific evidence available thatthe substance being monitored is likely to be injurious to

25Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
Gro
ups:
1. -
BA
T v
alue
s; 2
. -E
xpos
ure
equi
vale
nts
for
carc
inog
enic
mat
eria
ls (
EK
A);
3. -
Car
cino
geni
c su
bsta
nces
for
whi
ch E
KA
can
not
be e
valu
ated
; 4.
-B
LW
; th
e am
ount
of
ach
emic
al s
ubst
ance
or
its
met
abol
ites
or
the
devi
atio
n fr
om th
e no
rm o
f bi
olog
ical
par
amet
ers
indu
ced
by th
e su
bsta
nce
in e
xpos
ed h
uman
s w
hich
ser
ves
as a
n in
dica
tor
for
nece
ssar
ypr
otec
tive
mea
sure
s. (
U)-
urin
e, (B
)-B
lood
, Tim
e of
sam
ple
coll
ecti
on: (
a) -
not f
ixed
, (b)
- en
d of
exp
osur
e or
end
of s
hift
, (c)
- en
d of
wor
kwee
k, (d
) - a
t the
beg
inni
ng o
f the
nex
t shi
ft.
crea
t. -
crea
tini
ne
n-B
utyl
alc
ohol
, C
umen
e,C
yclo
hexa
ne,
1,2-
Dic
hlor
oben
zene
N,N
- D
imet
hyl a
ceta
mid
eE
thyl
ene
glyc
ol m
onob
utyl
eth
er,
Eth
ylen
e gl
ycol
mon
obut
yl e
ther
acet
ate,
Eth
ylen
e gl
ycol
mon
ethy
l eth
er,
Isop
ropy
l alc
ohol
, Man
gane
se,
4,4
-Me
thy
len
e
dip
he
ny
lis
ocya
nate
(M
DI)
2-B
utox
yeth
anol
2-B
utox
yeth
ylac
etat
eδ-
Am
inol
evul
inic
aci
d1,
4-D
ichl
orob
enze
neD
ichl
orom
etha
neD
iph
eny
lmet
han
e-4
,4’-
diis
ocya
nate
2-E
thox
yeth
anol
Pro
pano
lP
heno
l
Lea
d (B
)(a)
Chl
orob
enze
ne T
otal
4-c
hlor
ocat
echo
l (U
)
Dim
ethy
l for
mam
ide
N-M
ethy
l for
mam
ide
(U)
Car
bon
tetr
achl
orid
e (B
)
Tet
rahy
drof
uran
e (U
)
700
µg/
l30
0 µ
g/l (
wom
en)
70 m
g/g
crea
t.(d)
300
mg/
g cr
eat.
(b)
15 m
g/l
(b)
70 µ
g/l (
c,b)
8 m
g/l (
b)
400
µg/
l10
0 µ
g/l
(wom
en 4
5yrs
)
35 m
g/g
crea
t. (d
)17
5 m
g/g
crea
t. (b
)
35 m
g/l (
b)
3,5
µ g/l
(c,
b)
2 m
g/l
(b)
Tab
le 1
. C
hang
es in
DF
G r
ecom
men
dati
ons
mad
e si
nce
1999
Cat
egor
ies
of D
FG
Sub
stan
ces
adde
dS
ubst
ance
s re
mov
edC
hang
es in
BA
T v
alue
sre
com
men
dati
ons
Sub
stan
ces
and
indi
ces
1999
2003
1. B
AT
2. E
KA
Dic
hlor
omet
hane
Tet
rach
loro
ethy
lene
Tri
chlo
roet
hyle
ne
3.C
arci
noge
nic
subs
tanc
esw
ithou
t EK
A
An
tim
on
y a
nd
its
in
org
anic
com
poun
ds,
Ber
yliu
m,
Dic
hlor
oben
zene
Eth
ylbe
nzen
e,M
ercu
ry, o
rgan
ic c
ompo
unds
,M
ethy
l bro
mid
e
Tet
rach
loro
ethy
lene
Tri
chlo
roet
hyle
ne
4. B
LW
Ars
enic
and
inor
gani
c co
mpo
unds
Cre
sol,
Met
hyl b
rom
ide,
Phe
nol
26 J Occup Health, Vol. 47, 2005
Table 3. United Kingdom biological monitoring guidance values28)
Substance Health guidance value Sampling time Benchmark guidance value Sampling time
HGV BGV
Butan-2-one* 70 µmol butan-2-one/l in urine Post-shift
2-Butoxyethanol 240 mmol butoxyacetic acid/mol Post-shift
creatinine in urine
N,N-Dimethylacetamide 100 mmol Post-shift
n-methylacetamide/mol creatinine in urine
Lindane 35 nmol/l (10 µg/l) of lindane
in whole blood (equivalent to Random
70 nmol/l of lindane in plasma
MbOCA
(2,2’dichloro-4,4’-methylene 35 nmol total MbOCA/ Post-shift
dianiline) mol creatinine in urine
Mercury 20 µmol mercury/mol creatinine in urine Random
4,4’-Methylenedianiline 50 µmol total MDA/mol Post-shift for inhalation and
(MDA) creatinine in urine pre-shift next day for
dermal exposure
4-Methylpentane-2-one 20 µmol 4-methylpentan-2-one/l in urine Post-shift
Carbon monoxide 30 ppm carbon monoxide in breath, Post-shift
equivalent to 5% COHb
*Non included in the H&S Guidance on Laboratory Techniques in Occupational Medicine27) in 2002.
*- without hydrolysis, U-urine, B-Blood, Time of sample collection: (b) -end of exposure or end of shift, (c) -end of workweek,creat. - creatinine.
Aniline: Aniline (U) Aniline released from hemoglobin in bloodBenzene t,t-Mucomic acid in urineCyclohexanol 1,2-Cyclohexane diol (U)Cyclohexanol (U)Cyclohexanone (U) 1,2-Cyclohexanediol (U)Cyclohexanol (U)Methyl n-Butyl ketone 2,5-Hexanodine (U)*Styrene Mandelic acid + phenylyoxylic acid (U).Tetrahydrofurane (U)
Table 2. Changes in ACGIH recommendations made since 1999
Substances and/or Substances and/or Indices or values changed indices added indices removed Substances and indices 1998 2004
Styrene: Mandelic acid (U) Phenylglyoxylic acid (U) Styrene (B) prior to next shift
Arsenic elemental andsoluble inorganiccompounds (U)
Chromium Total chromium (U)
n-Hexane 2,5 -hexane dion (U)
50 µg/g creat. (c).
30 µg/g creat. (b,c)
5 mg/g creat. (withhydrolysis) (b,c)
35 µg/g creat.(c)
25 µg/g creat.(b,c)
0.4 mg/l * (b,c)

27Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
health. The values not greatly in excess of an HGV areunlikely to produce serious short- or long-term effectson health. The health guidance values are thereforehealth-based and are equivalent in terms of healthprotection to the occupational exposure standards. Thebenchmark guidance values are not health based; theyare the practicable, achievable levels set at the 90th
percentile of available biological monitoring resultscollected from a representative sample of workplaces withgood occupational hygiene practice. A result greater thana BGV does not necessarily mean that ill health will occur,but it does indicate that the control of exposure may beinadequate28).
In Finland, the BM practice is well established. Thebooklet published every year by the Finnish Institute ofOccupational Health contains 74 recommended values29).In Italy, there are 44 compounds with biological exposureindices. They are based mostly on the ACGIH BEI values.Considering some of the regression curves published inliterature, the so-called Biological Equivalent ExposureLimits (Limite Biologico Equivalente) for unchangedvolatile organic compounds (VOCs) in urine have beenproposed in Italy for seven substances (benzene, n-hexane, methylchloroform, methylethylketone, styrene,toluene and xylene)30). In Poland, BM recommendationshave been published for 20 substances31).
Where no biological monitoring guidance values havebeen set, it may be appropriate for employers to considersetting “in-house” values32).
In general, in spite of the decrease in occupationalexposure limits, the currently published BATs and BEIscan be used as the reference values for evaluatingexposure or health risk. Nevertheless, specific andsensitive analytical methods of instrumental analysis arerequired, such as gas chromatography (GC), and highpressure liquid chromatography (HPLC) and in somecases possibly with mass detectors (MS or MS-MS ) fororganic compounds and flame (FL-ASA) or flamelessatomic absorption spectrometry for metals. High qualityof determinations is necessary and this can be ensuredthrough the laboratory’s participation in external qualityassurance systems. Obviously, the quality assuranceissues apply also to the measurements of toxic substancesin the air.
The usefulness of biological monitoring forenvironmental exposure assessment
In the biological monitoring of population exposure,two different kinds of criteria can be applied: (a) health-based, and (b) used for the evaluation of the magnitudeof exposure against the reference values or to comparethe levels and trends of exposure in different regions orcountries.
The health-based recommendations can be obtainedfor substances that are deposited in the organism.
Unfortunately, for a majority of environmental toxinsthere a re no appropr ia te and wel l -des ignedepidemiological studies. Furthermore, it is at presentdifficult to find groups within the general population thathave been substantially exposed to environmental toxinsto study the dose-effect and dose-response relationshipsbetween the levels of biomarkers and early health effectsand to determine the Lowest Observed Adverse EffectLevel (LOAEL) or the No Observed Adverse Effect Level(NOAEL) values.
1. Health-based recommendationsTo d a t e , w e l l - d o c u m e n t e d h e a l t h - b a s e d
recommendations after the results of epidemiologicstudies have been formulated for three substances:inorganic lead, inorganic cadmium and methylmercury.Cadmium
Kidneys are the critical organs in a long-termoccupational or environmental exposure to cadmium. Awide range of tests of different sensitivity and significancehave been used among cadmium-exposed populations toassess cadmium nephrotoxicity.
The results of several studies performed on populationsenvironmentally exposed to cadmium indicate thatchanges in sensitive renal biomarkers may occur at lowerurinary cadmium levels than those found in adult maleworkers.
The number of well-performed environmental studieson the influence of cadmium on kidney functions islimited. Several markers of renal tubular dysfunction,including β
2-microglobulin (β
2M), retinol binding protein
(RBP) and N-acetyl-β-D-glucosamidase (NAG), werepositively associated with urinary excretion of cadmium.There was a 10% probability of the values being higherthan the cut-off level when cadmium excretion exceeded2 ÷ 4 µg/24 h33). Schütz and Elinder34) noted urinaryexcretion of α
1-microglobulin (HC) above the cut-off
level in 10% of the investigated population with cadmiumin urine (Cd-U) concentrations about 1 µg/g creatinine.The results obtained recently by Noonan et al.35) andTrzcinka-Ochocka et al.36) revealed that the urinaryexcretion of early biomarkers of kidney dysfunction canbe increased at cadmium levels in urine of about 2.0 µg/g creatinine.
It has been postulated that for the general populationthe Cd-U levels should be below 2.5 µg/g creatinine37).Lead
Biological monitoring is used for the assessment oftotal exposure from different sources. In the case ofenvironmental exposure to lead, health effects can bereferred to blood lead levels.
Children constitute the highest risk group and thecentral nervous system (CNS) is the critical organ inenvironmental exposure to lead. A wide range ofbehavioral tests have been performed on lead-exposed

28 J Occup Health, Vol. 47, 2005
populations to assess the influence of lead on CNSfunctions. A meta-analysis of the results ofepidemiological studies carried out mainly in the US,Australia and Europe was published by IPCS in 199538).
The WHO Air Quality Guidelines for Europerecommended that at least 98% of the population exposedin the general environment should have Pb-B below 100µg/l, and the median blood lead level should not exceed54 µg/l. The Centers for Disease Control39) (CDC)recommended that the Pb-B values in children should bebelow 100 µg/l. Nevertheless, according to the recentlypublished results of studies by Canfield et al.40), bloodlead concentrations, even those below 100 µg/l, areinversely associated with children’s IQ scores at threeand five years of age, and associated declines in IQ aregreater at these concentrations than at higher levels.
The geometric mean values published recently indifferent countries imply that in women and children thePb-B levels are approaching the range of 10–30 µg/lconsidered as “baseline” of minimal anthropogenicorigin41–45).Methyl mercury
The effects of methylmercury on the adult differ bothin quantitative and qualitative terms from the effectsobserved after prenatal or, possibly, postnatal exposure.The critical organ is the nervous system and the criticaleffects include developmental neurologic abnormalitiesin human infants, and paraesthesia in adults. The foetusis at particular risk. Prenatal exposure leads topsychomotor retardation in infants. Developmentalneurologic abnormalities are considered the critical effectsin the infant population.
Hair is a biomarker of long-term exposure tomethylmercury. Once mercury is incorporated into hair,it remains unchanged. The level of mercury in hair (Hg-
H) is dependent on fish consumption.The dose-response relationship between maternal hair
concentration and the frequency of health effects inchildren was used by the IPCS for the purpose of riskassessment46). At peak mercury levels in maternal hair atabove 70 µg/g, there is a high risk (more than 30%) ofneurological disorder in the offspring, and a 5% riskmay be associated with a peak mercury level of 10–20µg/g in maternal hair.
Recently, benchmark dose calculations have beenperformed for methylmercury-associated delays onevoked potential latencies in two cohorts of children fromthe Faroe Islands and Madeira47). The obtained bench-mark dose (BMDL 5%) of approximately 10 µg/gmaternal hair was similar to that calculated for otherneurological variables48) in the Faroese children and inthe New Zealand population49).
The present background level of Hg-H, associated withno or low fish consumption or a low fish methylmercuryconcentration, amounts to from 0.25 µg/g to 0.8 µg/g50–52).Much higher Hg-H levels result from the consumptionof large amounts of fish or sea mammals. The mean Hg-H levels in the Faroe Island population amounted from1.6 µg/g (one fish meal per week) to 5.2 µg/g (four fishmeals per week)51). In the Madeira fishermen and theirfamilies, it amounted to 38.9 µg/g in men and 10.4 µg/gin women53).
2. The German approach to human biological monitoringvalues for environmental toxins
Two kinds of values are recommended by theCommission on Human Biological Monitoring of theGerman Federal Environmental Agency established in1993: (a) reference values and (b) human biologicalmonitoring values (HBM values)54, 55). The HBM values
Table 4. Human Biological Monitoring Values (HBM) - values recommended by the German Commission on Human BiologicalMonitoring (Status: March 1999)
Analyte Group HBM I HBM II
Lead in blood Children ≤12 yr and females in the reproductive age 100 µg/l 150 µg/lMales and females <45 yr 150 µg/l 250 µg/l
Cadmium in urine Children, males and females <25 yr 1 µg/g creat. 3 µg/g creat.Adults >25 yr 2 µg/g creat. 5 µg/g creat.
Mercury in urine Children and adults 5 µg/g creat. 20 µg/g creat.Mercury in blood Children and adults 5 µg/l 15 µg/lPentachlorophenol (PCP) in serum Children and adults 40 µg/l 70 µg/lPentachlorophenol (PCP) in urine Children and adults 25 µg/l 40 µg/l
20 µg/g creat. 30 g/g creat.
HBM—The concentration of an environmental toxin in human biological material, below which there is no risk of advance healtheffects. HBM II—The concentration above which there is increased risk of adverse health effects in susceptible individuals in thegeneral population. creat. - creatinine

29Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
have been derived from human toxicology andepidemiology studies and are intended as a basis for ahealth-related evaluation of human biological monitoringdata. Usually, the Commission recommends two differentHBM values: HBM I, the concentration of anenvironmental toxin in human biological material belowwhich there is no risk of adverse health effects, and HBMII, the concentration above which there is an increasedrisk of adverse health effects in susceptible individualsin the general population. The HBM values are shownin Table 4.
3 Centers for Disease Control and Prevention (CDC,USA)
On March 21, 2001, the U.S. Centers for DiseaseControl and Prevention released the National Report onHuman Exposure to Environmental Chemicals withpreliminary data on biological monitoring of a large U.S.population. The Report provided summary analyses forblood and urine samples obtained in 1999 from theNational Health and Nutrition Examination Survey(NHANES 99+) and enhanced information from previousNHANES. This report described the results for 27environmental chemicals, including several metals,several phthalate metabolites, a nicotine metabolite, andsix organophosphate metabolites.
In January 2003, CDC released the Second NationalReport on Human Exposure to EnvironmentalChemicals56, 57). Chemicals and their metabolites weremeasured in blood and urine samples from selectedparticipants in the National Health and NutritionExamination Survey. This report presents exposureinformation on 116 chemicals in people who had bloodand urine samples taken during 1999 and 2000. Theprovided 95th-percentile levels mean that 95 percent ofthe serum or urine concentrations in the population arebelow that level.
4. Evaluation of the magnitude of exposure against thereference values and comparison of the levels and trendsof exposure in different regions or countries
The so-called reference values, mainly for metals andpersistent organic pollutants, have been published bydifferent organizations57–62), but such data are of limitedvalue on the international scale. They may be influencedby environmental exposure levels in a given country, theconfounding factors (smoking, kind of food consumed),changes due to reduced emission (e.g. lead), improvedcontrol of the contamination that may occur duringsampling63), better analytical procedures and internal orexternal quality control of the determinations.Nonetheless, these data may be useful at a local level.For example, in Germany, the reference values areintended to indicate the upper margin of the currentbackground exposure of the general population and to
identify subjects with an increased level of exposure55).The results of biological monitoring can be used for
evaluating the background contamination or the trendsregarding contamination in different countries. On theinternational level, they were used to compare internalexposure to organochlorine compounds63) or the trendsin the concentration of dioxins in breast milk in theEuropean countries64). The application of biologicalmonitoring can also confirm the effectiveness of thetechnical solutions aimed at reducing environmentalexposure on the local scale in a country as was the casefor lead blood levels in children. For example, in theU.S., the geometric mean of the Pb-B concentration inchildren, during the consecutive phases of NHANES II,III and IV in 1976–80 ; 1988–91 and 1991–94, amountedto 150 µg/l; 36 µg/l and 27 µg/l, respectively45). InSweden, the geometric mean of the Pb-B concentrationin schoolchildren has decreased from about 60 µg/l in1978 to about 25 µg/l over a period of 15 yr65).
The main prospective areas for application ofbiological monitoring of occupational exposure
1. Unchanged VOCs in urineFor volatile organic compounds (VOCs), the biological
monitoring of exposure is based mainly on thedetermination of specific metabolites in urine. Thisapproach has been developing since biological monitoringstarted to be applied and most of the recommendations3,
4, 27) on exposure assessment concern the level ofmetabolites in urine.
Nevertheless, in the occupational settings, VOCs arealmost as a rule present in mixtures66) and for a largenumber of them, the critical effect consists of a depressiveaction on the central nervous system3). The necessity toperform numerous determinations of different metabolitesin urine may be the main reason why biologicalmonitoring is rarely used in practice, unlike for e.g.metals, for the evaluation of VOCs exposure. It can bereliable in some cases involving exposure to a singlecompound, e.g. styrene, during the production oflaminated constructions, or compounds with specifictoxicity, such as the carcinogenic benzene or stronglyneurotoxic n-hexane.
Relevant literature reports mainly on two methods fora simultaneous screening and quantitative determinationof VOCs in biological material, but the determinationsof unchanged compounds in blood and exhaled air havenot gained wide acceptance mainly because the first oneis invasive, and in the second one the sampling is difficult.What is more, the half-life of the first phase of VOCselimination from blood and expired air is very short andthe concentration can decrease by half within severalminutes after exposure termination. There arerecommendations that blood samples should be collectedbefore the shift next day3) but then the concentrations are

30 J Occup Health, Vol. 47, 2005
low.VOCs are eliminated from the organism through the
kidneys as metabolites; a certain percentage of absorbedsolvents is eliminated unchanged through the lungs. Afteroccupational exposure the proportion of the solventexcreted in urine to the amount absorbed is not high. Itmay vary, depending on the hydrophobicity, from 1.5%for methanol to 0.001% both for 1,1,1-trichloroethane andtoluene, and to even less for hexane67). This small amountof solvent dissolved in urine collected in the bladder tendsto reach a pressure equilibrium with alveolar air and arterialblood68). Therefore, following Ghittori et al.69), the end-of-exposure urinary concentration of the unmetabolizedamount can be seen as the outcome of the naturalintegration over time of a rather fast partition between airand arterial blood and between arterial blood and urine,with the bladder serving as a collection and mixing vessel.
The determination of unchanged VOCs in urine wasrecommended mostly for short-chain alcohols andketones3, 4). They possess a high to medium watersolubility and are easily excreted in urine withoutmetabolism, by a simple diffusion process (into acetone,methyl isobutyl ketone and methanol).
This method has been recommended by severalresearch teams also for the biomonitoring of otherchemical classes of VOCs. Ghittori et al.69) proposedwhat they called the biological equivalent exposure limitfor nine solvents (acetone, 2-cyclohexane, 1,2-dichloropropane, n-hexane, methyl-ethyl ketone,perchloroethylene, styrene, toluene and 1,1,1-trichloroethane). This study was performed in anoccupational setting. High correlation (r=0.87–0.96) wasfound between the concentration of these solvents in theair and the concentration of unchanged compounds inurine samples collected during the first four hours of thework shift. There were also attempts to use thedetermination of unchanged VOCs in urine for theevaluation of exposure to low concentrations of thecomponents of gasoline vapours during the unloading oftankers and railway wagons70), during tank lorry loading71)
and in road tanker drivers72). During the unloading70),the concentrations of VOC vapours were very low. Forbenzene, toluene, xylenes, trimethylbenzenes, methyl tert-butyl ether (MTBE) and methyl tert -amyl ether (MTAE),the geometric mean concentrations amounted to 0.10;0.61; 0.68; 0.50 0.69 and 0.27 mg/m3, respectively. Inspite of the very low exposure, the correlation coefficientsfor the concentrations in the breathing zone and in urinesamples collected at the end of shift amounted to from0.411 to 0.981. Vainiotalo et al.71) and Saarinen et al.72)
found a correlation between MTBE and methyl tert - amylether (TAME) concentrations in the breathing zone andthe excretion of unchanged compounds in urine collectedafter the shift. Determinations of unchanged toluene73),toluene and xylenes74) or tetrachloroethylene75) were also
performed, showing a correlation between theconcentration of these compounds in the air and in urinesamples collected at the end of exposure.
The conditions concerning urine sampling and samplestorage were investigated and general conclusions havebeen reached67, 76). The determination can be performedby means of gas chromatography after VOCs’ separationfrom urine by means of traditional ‘head space’ (HS) orhead space solid phase microextraction (HS-SPME)76, 77).
Based on some of the regression curves published inliterature, the so-called Biological Equivalent ExposureLimits (Limite Biologico Equivalente) for unchangedVOCs in urine have been proposed in Italy for benzene,n-hexane, methylchloroform, methylethylketone, styrene,toluene and xylene30).
Generally, the results reported in literature show thatthe measurement of urinary excretion of unchangedsolvents provides a highly sensitive and specific exposureindex. This method can be applied to the biologicalmonitoring of occupational exposure to low levels ofsolvents or, what is more important, to solvent mixtures.
But, according to the opinion of the ACGiH20), there isinsufficient information at present on the kinetics of e.g.toluene excretion in urine. If the kinetics is similar tothat for toluene in expired air and blood, the end-of-shiftspecimens would be reflective of exposure only for thelast two hours of the shift. The lack of experimental dataconcerning the toxicokinetics of unchanged VOCs excretedin urine refers to all the other compounds as well. Alsothe linearity of the regression curve between theconcentration in the air and in urine was studied for alimited range of exposure levels. For example, the resultsobtained by Kawai et al.73) indicate that this relation canbe curvilinear since for the air toluene concentrations of10, 25, 50 and 100 ppm, the respective urine concentrationsof toluene amounted to 16, 26, 40 and 67 µg/l.
All the problems concerning the kinetics of urinaryexcretion of unchanged compounds with differentoctanol: water partition coefficients and the resultingsampling strategy, or the linearity within the relativelylarge range of concentrations, can be resolved only withthe aid of a well-designed experimental study. Thearguments for the use of this method are the noninvasivespecimen collection, the possibly minor kinetic influencein comparison with VOC levels in blood, and thesimultaneous quantification of mixture compounds in asingle urine sample. The arguments against include thesmall percentage of lypophilic VOCs excreted in urine,increased analytical requirements, probability of VOCsloss during the pre-analytical phase, and more complexsample handling. It has been estimated that theconcentrations of toluene, xylene and tetrachloroethylenein blood can be about ten times as high as in urine samplescollected at the same time11).

31Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
2. Polycyclic aromatic hydrocarbons (PAH)PAHs are a large group of compounds which consist
of two or more fused aromatic rings made entirely fromcarbon and hydrogen. In an occupational setting, PAHsuptake is through the respiratory tract and the skin as aresult of contact with PAHs-containing materials.Metabolites in urine
Several methods have been developed to assess internalexposure to PAHs after exposure in workplaces. In moststudies, PAHs metabolites were measured in urine. Themetabolites measured in urine and feces include urinarythioethers, 1-naphtol, β-naphtylamine, hydroxyphenanthrenes and 1-hydroxypyrene (1-HP)78).
No difference in thioether excretion in urine wasobserved between the controls and coke oven workers orworkers at coke and graphite-electrode-producing plants.It was concluded that the determination of thioethers inurine was of little value, since smoking is a strongconfounding factor79–81). Becher and Bjorseth82) developedan analytical procedure to measure PAHs in human urineafter reducing metabolites to parent compounds. TotalPAHs were higher than the levels for nonsmokers, butwhen individual PAHs were examined, there was nosignificant difference. Further application of this methodto the analysis of urine samples from workers at analuminum plant83) and from coke oven workers84) did notshow differences between the exposed workers andcontrols in PAH levels in urine.
1-HP, a pyrene metabolite, was introduced as abiomarker of exposure to PAHs by Jongenellen et al.85)
and has been widely used as such since that time. Itsadvantage lies in that pyrene is present in all PAHsmixtures in relatively high concentrations. Pyrene ismetabolized predominantly to 1-HP. In contrast to otherPAHs metabolites, which are excreted mainly in feces,1-HP is excreted mostly in urine.
When 1-HP was used as a biomarker for PAHsexposure, the oral, dermal and inhalation routes were allshown to be important. Furthermore, low levels ofexposure could also be determined. A great advantage isthat the determination of urinary 1-HP is quick and easyand thus well suited for use in large-scale epidemiologicalstudies.
The determination of 1-HP in urine can be used todayto trace the trends of exposure in a given enterprise andto evaluate the effectiveness of prophylactic measuresundertaken. For example, the use of dermal protectionin the form of impermeable polyvinyl chloride suits ledto a substantial decrease in the urinary concentrations of1-HP86). Frequent changes of work clothes andunderclothes reduced 1-HP excretion by 37–55%87, 88).
The comparison of different work environments may,however, be difficult because the proportion of pyrene ascompared to that of benzeno [a] pyrene (BaP) and otherpotentially carcinogenic PAHs, may vary. For example,
the creosote oil used in a wood impregnation plantcontained about 3.4% pyrene and less than 0.0004% BaP.The levels of 2–10% pyrene and 0.4–0.6% BaP are foundin coal-tar that is the main PAH contaminant in the cokeindustry, in primary aluminum industry, and during roadpaving with tar. Polluted ambient air contains about 6.5%BaP and 1.8–2.7% pyrene78).
Several authors tried to establish admissible levels of1-HP in urine for specific exposures. According toJongenellen89), in coke-oven workers, the urinaryconcentration of 1-HP of 4.4 µg/g creat. reflects theconcentrations of coal tar pitch and BaP in the air of 0.2mg/m3 and 2 µg/m3, respectively. A similar value, of 4µg/g creat., was proposed by Levin et al.90) A highervalue of 6.1 µg/g creat. was suggested by Van Roij etal.91) In the study on workers at an aluminum reductionplant, Tjoe Ny et al.92) assumed that exposure to 0.2 mg/m3 of coal tar pitch or 5 µg/m3 of BaP will result in aurinary concentration of 1-HP of 8.6 µg/g creat.
Based on the logistic regression between the prevalenceof abnormal high frequency cells (HFC) in peripherallymphocytes and PAHs in the air or 1-HP in postshifturine of nonsmoking workers exposed to PAHs, Buchetet al.93) concluded that the concentrations of PAHs in theair and 1-HP in urine should be kept below 6.4 µg/m3
and 2.7 µg/g creat., respectively.Recently Jongenellen94) proposed a three-level
benchmark guideline for urinary 1-hydroxypyrene as abiomarker of occupational exposure to PAHs. Thereference value, as a 95th percentile in non-occupationallyexposed controls, is 0.24 µmol/mol creat (0.46 µg/gcreat.) and 0.76 µmol/mol creat. (1.44 µg/g creat.) fornonsmokers and smokers, respectively. This is the firstlevel of the benchmark guideline. A no biological effectlevel of 1-hydroxypyrene in exposed workers was foundat 1.4 µmol/g creatinine (2.66 µg/g creatinine). It is thelowest reported level at which no genotoxic effects werefound (the second level of the benchmark guideline). Thecorrelation between airborne concentrations and urinary1-HP in coke oven workers and workers in the primaryaluminum industry was used to estimate the level ofurinary 1-HP corresponding to the current occupationalexposure limit (OEL) of PAH. The concentration of 1-HP in urine, equal to the OEL, is 2.3 µmol/mol creat.(4.37 µg/g creat.) and 4.9 µmol/mol creat. (9.31 µg/gcreat.), respectively, in these two industries, but thescattering of results in this case is substantial and thesevalues represent the lowest reported estimate for theconcentration equal to the OEL.Mutagenicity in urine
The mutagenicity in urine from persons exposed toPAHs has been assayed by the Ames’ test in a number ofstudies. Tobacco smoking was found to be mutagenic.No increase in mutagenic activity was found in moststudies of workers exposed in occupational settings such

32 J Occup Health, Vol. 47, 2005
as coking, coal tar distillation, aluminum plants, anodeplants or graphite electrode plants78). Only a heavyexposure to coal-tar formulations in patients withpsoriasis95, 96) and in coke oven workers97) resulted inmutagenic urine.
The Ames’ test, therefore, appears not to be sensitiveenough to detect the presence of urinary mutagens dueto occupational exposure to low levels of PAHs.Current recommendations
At present, only ACGIH3) in their notice of intendedchanges mentioned the measurement of 1-hydroxypyreneas a possible BEI but with Nq notation which means thatbiological monitoring should be considered, but a specificBEI could not be determined due to insufficient data.
3. PesticidesPesticides comprise a large group of chemical
compounds designed specifically for the control of pests,weeds and plant diseases. In the United States, therewere about 620 pesticidal active ingredients which wereformulated into approximately 20,000 different productsregistered with the Environmental Protection Agency(EPA)98).
Unlike other man-made chemicals, exposure topesticides may affect a large part of the human population,including workers involved in their industrialmanufacture, formulation and application either inagriculture or public health, and a part of the generalpopulation who may experience exposure throughdomestic use and consumption of contaminated food andwater.
In the case of pesticides for which occupationalexposure, mainly in agriculture, fluctuates in time andthe skin is a significant route of absorption99), biologicalmonitoring constitutes an important tool for obtaininginformation on exposure and possible early health effects.
Unfortunately, biological monitoring of occupationalexposure to pesticides is not always carried out for routinefield activities. At present, the number of biologicalexposure indices recommended by ACGIH3) is limited toorganophosphorous pesticides (OP) (measurements ofacetylcholinesterase (AchE) activity in red blood cellsand p-nitrophenol, a metabolite of parathion in urine) andpentachlorophenol (PCP) in urine and plasma. TheGerman BAT values are available for lindane (blood,serum), for AchE activity and parathion4). Biological limitvalues for dieldrin, endrin, coumarins, 4-chloro-2-methylphenoxyacet ic acid (MCPA), and 2,4-dichlorophenoxyacetic acid (2,4-D) were also proposedby the Study Group of the Scientific Committee onPesticides of the International Commission onOccupational Health100).
This situation seems to be changing and the biologicalmonitoring of pesticide exposure is gaining more andmore attention both in occupational (agricultural) and
environmental settings56, 100).Considerable progress has been made in the field of
analytical methods. Most of the studies are aimed atmeasuring metabolites or unchanged compounds in urineand/ or blood. The principal groups of pesticides include:organophosphorous compounds , carbamates ,organochlorine compounds, pyrethroids, herbicides,fungicides and other compounds. The choice of themethod should be based on the objective. For monitoringthe general population, the limit of detection (LOD) ofthe analytical methods must be about 1 µg/l, higher valuesapply to the monitoring of occupationally exposedpersons. Aprea et al.101) reviewed the analytical methodscurrently used in this field. In the case of OP compoundsit is possible to measure unchanged compounds or theirmetabolites, mainly alkylphosphates (AP). The mostcommonly used ana ly t ica l methods a re gaschromatography (GC) with photometric detection (GC-FPD, or mass detection (GC-MS). The LODs are for anAP amount to about 1 µg/l of urine. Recently, CDC hasdeveloped a scientifically sound GC-MS-MS method toquantify non-specific AP102). GC with an electron capturedetector (GC-ECD) is used for the measurement oforganochlorine pesticides. The LODs for these methodsare between 1 ng/l and 1 µg/l.
There is a rapidly growing body of evidence frombiomonitoring studies aimed at the evaluation ofexposure, mainly to OP compounds, in pesticideapplicators103–108) and their families as well as in membersof the general population (pesticide residues in food andpesticides in indoor environments). A subject of specialconcern is the necessity for the biological monitoring ofenvironmental exposure of children who, depending onage, may come into contact with dust and soil, and ofpregnant women’s exposure109–114).
In the case of biological monitoring of pesticideexposure, the development of analytical methods is muchfaster than the capacity for interpreting the results of thedeterminations. Angerer115) presented the results ofstudies conducted among 1000 representatives of thegeneral population in Germany. The metabolites oforganophosphorous pesticides, dimethylphosphate anddimethylthiophosphate were found in about 80% of thestudy while diethylphosphate was detected in about 70%of the subjects.
Health-based interpretation of results is lacking as arule and the biological monitoring is used mainly to assessthe absorbed dose, which can be done by a comparisonwith the pre-exposure levels or reference values. As theLODs of the methods for biological monitoring continueto decrease, the reference doses also become lower. CDCestablished the reference ranges for several pesticidesbased on the measurements of their metabolites in urinesamples from randomly selected adults in the USpopulation. These data have been successfully used to

33Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
evaluate internal pesticide doses of the spouses andchildren of farmer applicators. For example the 2,4-Dlevels in the urine of applicators’ children clearlyexceeded the reference range (<1.0 to 1.8 µg/l)98).Biological monitoring was also used for the calculationof daily intake, which can then be compared withrespective recommendations. For example Koch et al.116)
determined the concentrations of 3,5,6 -trichloro-2-piridinol (TCPyr), a specific metabolite of OP pesticides,chlorpyrifos (CHP) and chlorpyrifos-methyl (CHPM).The median excretion of 3,5,6-trichloro-2-piridinol(TCPyr) in non-occupationally exposed persons was 1.4µg/l, which corresponds to a daily intake of 2.5 µg CHP+ CHPM. The acceptable daily intake (ADI) amounts to10 µg/kg b.w. Similar results were obtained in othercountries. A study carried out in the USA117) yielded a 50percentile of 3 µg/l, and an Italian study101) a geometricmean of 2.8 µg/g creatinine.
4. Cytostatic drugsThere has been a major concern about the potential
exposure and subsequent effects in health care workerswho handle cytotoxic and antineoplastic drugs. Many ofthese drugs have mutagenic, teratogenic, or carcinogenicproperties, where no threshold dose can be identified.Therefore, exposure to these compounds should beavoided. Any drug absorption in hospital staff is generallyassumed to proceed via the skin or mucous membranes,and to a lesser extent by inhalation, but the ward staffmay be exposed not only from the spillage of drugs, butalso via contact with the patients’ body fluids, such asvomit, sweat and urine118). Biological monitoringconstitutes the best method for determining whether theexposure hazard at the hospital wards where cytotoxicdrugs were handled was controlled appropriately.
The apparent half lives for urinary excretion areroughly 5 h fo r metho t rexa te , 12–24 h fo rcyclophosphamide and isofosfamide, and 72 h forcisplatin. The urine measurement for these chemicalsmay be largely influenced by exposure in the preceding24 h, but for those drugs whose half lives are 24–72 h,the urine measurement may more exactly reflect the levelof exposure over the previous week118).
In order to monitor the possible uptake of these drugs,it is necessary to use sensitive and compound specificdetection methods. In recent studies, GC-MS, HPLC-MS-MS, GC -ECD, ELISA, voltametry and inductivelycoupled plasma with mass spectrometry (IPC-MS)methods were used. The detection limit of these methods(except for GC-ECD) was lower than 1 µg/l of urine.The results of the investigations carried out in theNetherlands, Germany, Italy and U.K.118–122) show that theinternal exposure of the personnel involved in thepreparation and administration of drugs may depend onthe practice applied.
According to the opinion of Ziegler et al.118) the “non-detected” urine measurement result does not signify anyexposure or risk. These authors calculated that acontinuous uptake of cyclophosphamide commensuratewith a detection limit of about 0.25 µg/l urine, mayrepresent an annual cancer risk of 3–20 per million.
5. Hard metalsHard metals are commonly used, mainly because of
their resistance to corrosion, temperature, and wear. Themost important use is as alloy components. For example,the main components of cemented carbides are tungstencarbide and cobalt metal. Beryllium is used in alloyswith other metals (particularly Cu and Ni, and to a lesserextent Co, Cr, Fe and Mg) for improving hardness andresistance to corrosion, wear, vibration, and collision123).As a result of the increasing industrial use of beryllium,occupational exposure to the metal may be an importantissue.
Occupational exposure to hard metal dust was reportedto induce adverse effects on the upper and lowerrespiratory tract and the skin. Several studies suggestedthat cobalt is the main aethiological agent for thedevelopment of interstitial fibrosis. Soluble tungstencompounds affect the functions of the central nervoussystem. Chronic pulmonary beryllium disease (CBD) isan immunologically-mediated syndrome, defined as theoccurrence of lymphocyte proliferation coupled with thepresence of alveolar granulomas124). The other well-known effect of occupational exposure to beryllium iscancer (group A1 by IARC).
The recommended levels for biological material areavailable for cobalt and nickel, but not for tungsten andberyllium. In Germany, the exposure equivalent forcarcinogenic materials (EKA) is 30 µg/l urinary cobaltfor 0.05 mg/m3 cobalt in air4). ACGIH3) set up two BEIsfor cobalt: 15 µg/l for urine and 1 µg/l for blood samplescollected at the end of the shift at the end of the workweek.The reference value for urinary cobalt is 1.5 µg/l125). TheEKA value for nickel is 15 µg/l urine for 0.10 mg/m3
nickel in air34). The reference value for urinary nickel is2.2 µg/l125).
Kraus et al.125) attempted to evaluate the excretion oftungsten in the urine of workers exposed to differenttungsten compounds in a plant producing hard metals.The tungsten analysis was carried out with ICP-MS. Thedetection limit for urine was 0.05 µg/l. The mean tungstenconcentrations in the urine of non-exposed people (n=33)were 0.31 µg/l and 0.30 µg/g creatinine. The referencevalues (95 percentile) were 0.86 µg/l and 1.00 µg/gcreatinine. The mean concentrations of tungsten in urineamounted to 94.4 µg/g creatinine in the grinders, 42.2µg/g creatinine in workers at departments producingtungsten carbide, and 24.9 µg/g creatinine in heavy alloysworkers. Due to the low limit of detection, the results

34 J Occup Health, Vol. 47, 2005
obtained made it possible to differentiate between therenal excretion in the exposed and non-exposed groups.But, due to the different bioavailability of tungsten,increasing in the order: tungsten metal, tungsten carbide,tungstenate, there was no correlation, on a group basis,between tungsten concentrations in the air and urine. Thismeans that a simple solution for biological monitoringof exposure to tungsten compounds is not possible. Theauthors postulate that only when the data fromenvironmental and biological monitoring are consideredin combination, can a valid and effective definition ofhigh risk be derived.
Also the data for biological monitoring of exposure toberyllium are not available because of the small numberof working activities involving exposure to this metal,and formerly the lack of appropriate analytical methods.The mean values for urinary beryllium in non-exposedpersons as reported in the past amounted to 0.4 µg/l126),0.28 µg/l127). In the studies by Apostoli and Schaller123)
or Wegner et al.128) where beryllium analysis was carriedout by the ICP-MS method, the detection limit was 0.03µg/l, or 0.06 µg/l, and beryllium concentrations in theurine samples of persons not occupationally exposed werebelow these detection limits.
Wegner et al.l28) investigated 57 gemstone cutters. For27 cutters working in contact with beryls for 21 h/wk onaverage, beryllium could be detected in 17 pre-shift and12 post-shift urine specimens. The median for the pre-shift urine samples was 0.09 µg/l (<0.06 to 0.56 µg/l)and for the post-shift urine samples <0.06 µg/l (<0.06–0.29 µg/l). No analysis of the correlation betweenexternal and internal exposure was carried out.
Apostoli and Schaller123) examined 65 metallurgicworkers in two electric steel plants and two copper alloyfoundries. Beryllium concentrations in urine varied from<0.03 to 0.54 µg/l. A significant correlation was foundfor the relationship between external and internalexposure. The urinary Be levels were in the range 0.12to 0.15 µg/l whereas the concentrations of Be in inhalabledust were below the recommended threshold limit value–time weighted average (TLV-TWA) of 0.2 µg/m3.
6. DNA and protein adductsExposure to genotoxic carcinogens results in the
formation of covalently bound adducts between thegenotoxin and DNA, which if not repaired may lead to amutation and alteration of gene function. Genotoxiccarcinogens also react with many other nucleophilic sitesintra- and extra-cellularly (eg. protein, glutathione).Protein adducts are not repaired and are regarded simplyas exposure monitors, but DNA adducts may also givefurther information with regard to the mutagenicsignificance of exposure.
According to Farmer129), the sensitivity of the currentlyavailable methods (32P postlabelling, HPLC-MS-MS) for
adduct measurement has been shown to be sufficient fordetecting the background level of DNA and proteindamage, i.e. the one observed in non-smoking peoplewithout known exogenous exposures to electrophiliccarcinogens. It appears that the total extent of adductformation in normal human DNA (excluding oxidativedamage) is at least 1 modification per 107 nucleotides,which stands for at least 600 modified nucleotidemolecules per adult cell and over 1016 modified nucleotidemolecules per adult human body. This would indicatethat the effectiveness of repair of the steady state damageis high, so that mutations do not accumulate excessively.DNA-adducts
The measurement of DNA adducts in human tissueswould provide an excellent means to assess the genotoxicdamage. A major limitation is the requirement of DNAfrom biopsy samples; an invasive procedure. Analternative, non-invasive source of tissue would bedesirable. Buccal mucosa tissue has been successfullyused to measure DNA adducts in smokers130) andexfoliated urothelial cells for compounds that areassociated with urinary bladder cancer131). White bloodcells are another alternative tissue source, but there aredoubts as to what extent the DNA adducts in leukocytesreflect DNA adduct formation in target tissues. Forexample, DNA adducts in white blood cells of rats andh u m a n s e x p o s e d t o 2 - a m i n o - 1 - m e t h y l -phenylimidazolo[4, 5-b]pyridine (PhIP), a heterocyclicaromatic amine, decline rapidly and do not appear toreflect PhIP-DNA adduct formation in the colon orbreast130). Also the relationship between smoking historyand DNA adducts in the leukocytes has not beenadequately demonstrated132, 133). According to Bhatnagaret al.131), it is not clear whether blood leukocytes are avalid surrogate for the target tissue level in everyexposure.
Individual differences can influence the DNA-adductlevels. As regards the polycyclic aromatic hydrocarbons,exposures that result in the excretion of highconcentrations of 1-HP in urine also lead to high DNAadduct levels, but in all the populations studied, therewas a substantial individual variation in PAH-DNA adductlevels, after oral or inhalation exposure, that was greaterthan that described for 1-HP excretion in urine. In onestudy, about 50-fold individual variations were reportedamong controls and about 100-fold ones among coke-oven workers134). The variations were probably due todifferences in the induction of arylhydrocarbonhydroxylase (AHH) activity in lymphocytes and in thesubsequent detoxification of carcinogenic PAHs, theability to repair DNA lesions, and the turnover of damagedcells. These individual variations resulted in a wideoverlap in the ranges of values for exposed and unexposedsubjects in all studies.
The levels of DNA adducts in controls ranged from

35Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
0.2 to about 10 adducts per 108 nucleotides in leukocytes.Workers exposed to PAHs had high mean levels ofadducts and a higher percentage of positive samples thanthe controls. In the cases of high exposure, for examplein coke-oven workers, 5–70 adducts per 108 nucleotideshave been detected. DNA adducts are much less sensitivein human exposure assessment than the excretion of 1-HP in urine. This method, however, makes it possible toidentify subjects who are highly susceptible to the DNA-damaging properties of PAHs and who are thereforepredisposed to lung cancer135).Protein adducts
Electrophilic carcinogens can be bound to amino acidresidues on such molecules as albumin or hemoglobin.Monitoring carcinogen-protein adducts is possible dueto the relative abundance of certain proteins likehemoglobin and albumin in the central compartment.Blood samples are relatively easy to obtain. Because ofthe long life span of the proteins used for protein adductdetermination, as well as the stability of these adductsthat allows for their accumulation over the protein life-span, there are some practical advantages of determiningprotein adducts as a marker of exposure.
Several laboratories have studied the binding ofaromatic amines and alkylating agents to hemoglobin oralbumin. Recently, this has referred to such compoundsas ethylene oxide, propylene oxide, acrylonitrile,acrylamide135, 136), 1,3-butadiene137), styrene, styrene-7,8-oxide and benzene138), heterocyclic amines140),dimethylformamide, t r ini trotoluene and 4,4’-methylenedianiline141). Boogaard et al.137) demonstratedthat in the case of low-level (0.015–1.1 mg/m3)occupational exposure to 1,3-butadiene, the correlationbetween airborne concentrations of 1,3-butadiene and itshemoglobine adducts, 1- and 2-hydroxy-3-butenyl valine,was much closer than for its urinary metabolites. Alsoin workers exposed to 4,4’-methylenedianiline atconcentrations below the detection limit, the adductswere detected in a high percentage of samples141).Hagmar et al.136) established a dose-response relationshipbetween hemoglobin adducts of acrylamide and theperipheral nervous system symptoms in tunnel workers,but protein adducts can be seen in supposedly unexposedcontrols129, 135, 138).
According to Bhatnagar and Talaska131), thedetermination of unchanged carcinogenic compounds ortheir metabolites with relatively short half-lives makes itpossible to evaluate only the most recent exposure (1–2days’). Protein adducts integrate exposure over the half-life of the cells/protein sampled. The estimated lifespanof hemoglobin is 120 d. With such a long lifespan, theday-to-day variation is minimal once exposure hasreached a steady state. Sampling for these markers shouldbe performed semi-annually or annually to complementthe medical screenings.
The practical application of adduct measurement inorder to improve the prevention of diseases caused byhazardous substances in industry is a subject of particularinterest in Germany. During the recent DFG round-tablediscussion on biological monitoring, two sessions weredevoted to this problem141).
Also the use of adduct measurements for evaluatingoccupational exposure has been proposed only in theGerman DFG recommendations4). The authors postulatethe measurement of aniline released from the aniline-haemoglobin conjugation in whole blood after exposureto aniline and nitrobenzene. The recommendedconcentration is 100 µg aniline released from theconjugate. This conjugate can be measured after a periodof at least three working days has elapsed. The proposedvalue is based on the studies of 1,000 workers exposedregularly to aniline and more than 50 employees withacute aniline intoxication. It was found that atmethemoglobin levels of less than 5% also, less than 100µg aniline was released from the hemoglobin conjugateper litre of whole blood. This approach has not beenapplied in any other recommendation. The authors ofthe ACGIH documentation20) stressed that the kinetics ofthis indicator was studied only in one volunteer and thatthe concentration of aniline hemoglobin conjugates varieddepending on the population (fast acetylators have aconcentration 10 times lower than slow acetylators). Alsothe measurement of hydroxyethylvaniline after exposureto ethylene oxide and ethylene was recommended byDFG4).
Although the area of DNA and protein adductsmeasurement is developing very fast, it appears that asyet little is known about the diagnostic meaningfulnessof the results of these measurements. Considerably morestudies are required in order to clarify the possible routineapplication of these methods in occupational practice.
Interlaboratory quality assurance systems andreference materials for a daily quality controlprogram within the laboratory
To meet the demands for reliable biomonitoringdeterminations is not an easy task. The low analyte levelsrequire complex sample treatment procedures that haveto be carried out with a high degree of precision to allowreliable assessment of exposure. An approach widelyapplied today to achieve, maintain and document thequality of work of a biological monitoring laboratory isthe adoption of a quality management program142–144).Internal quality control and external quality assuranceare important parts of the quality management. Thefollowing measures should be undertaken to ensure thehighest quality of the determinations11, 145):—to give an exact protocol about the person’s working
time and exposure conditions (e.g. workload, skincontact, time of specimen collection),

36 J Occup Health, Vol. 47, 2005
—during the pre-analytical phase, standardize all theprocedures that cannot be controlled by a classicalquality control, including conditions of specimencollection, handling and storage,
—work out and strictly follow a validated method forthe complete analytical procedure. (The appropriateanalytical procedures for chemical substances in bodyfluids can be found in the materials published byACGIH20), WHO15) or DFG146)),
—establish a well performed system of internal andexternal quality control.Quality assessment refers to the quality of the analytical
results. It has two components: internal quality control,which is a set of procedures used by the staff of alaboratory to continuously assess the results as they areproduced, and external quality assessment, which is asystem for objectively checking the laboratoryperformance by an external agency or institution.
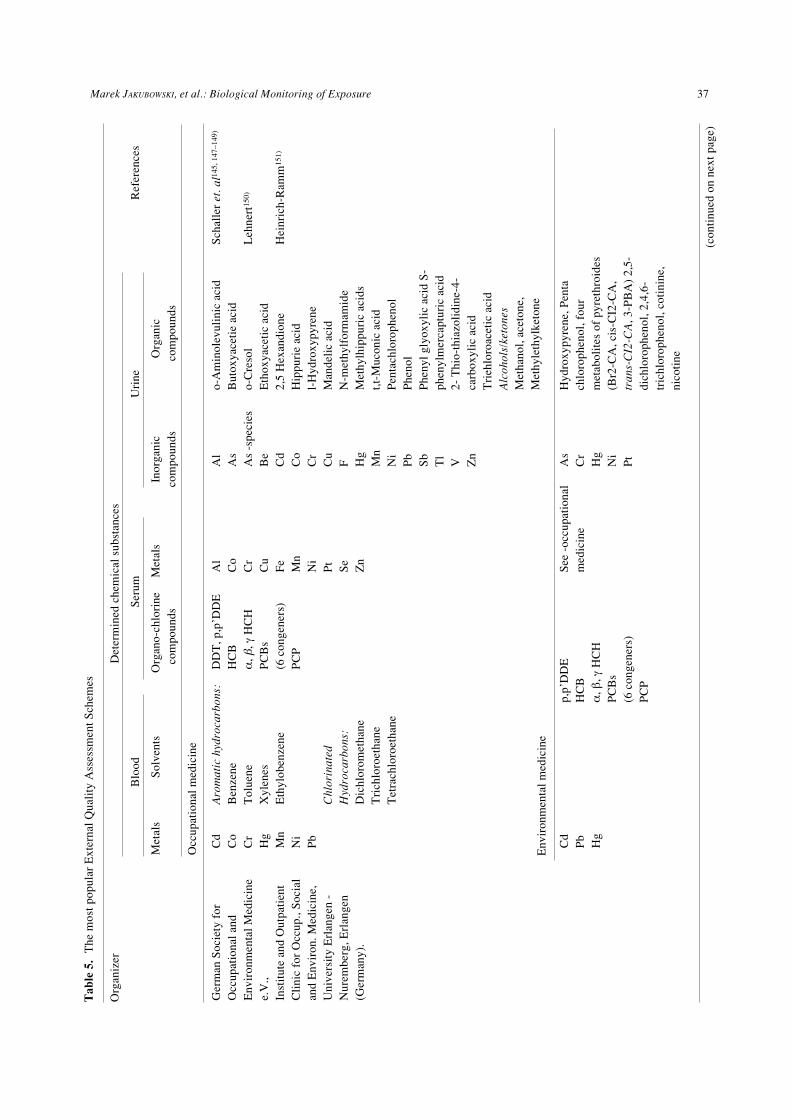
The most popular external quality assurance systemsfor chemical substances and their metabolites, atconcentrations in biological media relevant tooccupational exposure, are shown in Table 5. A qualityassurance scheme which encompasses the range ofconcentrations of toxic substances relevant toenvironmental exposures is available from the Instituteof Occupational, Social and Environmental Medicine,University Erlangen—Nürnberg, Germany (Table. 5).
Standard reference materials are the samples whosequantitative composition of certain components has beendetermined by various methods and by qualifiedlaboratories. They are accompanied by a certificatestating the concentration of these components. Since thismaterial is very expensive, it is usually used during thevalidation of an analytical procedure rather than forroutine accuracy control. In view of the above, thecommercially available control samples with an assignedconcentration are used for routine internal quality control.The most commonly used certified and routine referencematerials are specified in Table 6.
Potential users of BM and an attitude towards thepractical application of BM in different countries.
It is not clear whether BM actually belongs tooccupational hygiene or occupational medicine.Traditionally, biological monitoring has been conductedby occupational physicians and health professionals, andthis is still the case in many European countries. But,the focus on noninvasive sampling (urine, and exhaledair sampling) and the growing awareness of the usefulnessof biological monitoring has shifted BM closer to theactivity area of occupational hygienists and work safetyprofessionals. In fact, a vast majority of BEIs are directlyrelated to the corresponding TLV values. Thecomparative ease of biological sample collection makesit a simple procedure that small firms may find useful,
for example, urine samples collected at the end of theworkday. But the use of biological monitoring as a toolfor occupational hygienists needs more simplified datafor the interpretation of results and implementation ofthe methods reflecting exposure to several compoundsin a mixture that have similar endpoints (e.g.determination of unchanged VOCs in urine).
Despite the numerous long-term studies andconsiderable efforts of the researchers, the so-called‘health-based’ reference values have been proposed andvalidated only for several chemical substances or groupsof substances. These recommendations are of great valueto health professionals because the health effect ofexposure can be predicted directly from the determinationof a biomarker of exposure. It is possible to predict earlydirect health effects of lead based substances on bloodlead levels1). The results shown in Fig.1 indicate theadvantage of using an integrated index of cadmiumexposure CdB × t (cadmium in blood (µg/l) × years ofexposure) as a predictor of kidney dysfunction in workerschronically exposed to cadmium (Jakubowski et al.157)).This is also possible in the case of other biomarkers ofexposure (mercury, fluorides and to some extent arsenic)or biomarkers of early reversible effects (thecarboxyhemoglobin or methemoglobin concentration inblood, decreased cholinesterase activity in red bloodcells). Such measurements can constitute an integral partof periodical medical examination and can be interpretedwithout knowing the results of environmental monitoring.
Recent policy developments in the United Kingdomhave been aimed at clarifying the role of biologicalmonitoring which can be used both for exposureassessment and health surveillance28). With regard tohealth surveillance, biological monitoring is applied whenit is possible to link the results of biological tests to (an)adverse health effect(s). What is implicit in thisrequirement is that a no-adverse-effect level can beestablished. Where biological monitoring is being carriedout as a part of health surveillance, it should be performedunder the supervision of an occupational healthprofessional; in some cases this must be a registeredmedical practitioner.
In Germany, biomonitoring is required by law andexplicitly addressed in the German Ordinance onDangerous Substances32). Section 18 deals with the “dutyof surveillance”. If the existence of dangerous substancesin the workplace cannot be excluded, it must be assuredthat maximum concentration at the work place (MAK)values, technical exposure limits (TRK) values orBiological Exposure Values ( BAT) are not exceeded.
The application of biological monitoring is regulatedin completely different ways in the European countries.While BM is required by law in Germany, some countriescarry out BM only where there are correspondinginstructions from the European Union. This applies e.g.
37Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
Ger
man
Soc
iety
for
Occ
upat
iona
l and
Env
iron
men
tal M
edic
ine
e.V
.,In
stit
ute
and
Out
pati
ent
Cli
nic
for
Occ
up.,
Soc
ial
and
Env
iron
. Med
icin
e,U
nive
rsit
y E
rlan
gen
-N
urem
berg
, Erl
ange
n(G
erm
any)
.
Cd
Co
Cr
Hg
Mn
Ni
Pb
Aro
mat
ic h
ydro
carb
ons:
Ben
zene
Tol
uene
Xyl
enes
Eth
ylob
enze
ne
Chl
orin
ated
Hyd
roca
rbon
s:D
ichl
orom
etha
neT
rich
loro
etha
neT
etra
chlo
roet
hane
DD
T, p
,p’D
DE
HC
Bα
, β, γ
HC
HP
CB
s(6
con
gene
rs)
PC
P
Al
Co
Cr
Cu
Fe
Mn
Ni
Pt
Se
Zn
Al
As
As
-spe
cies
Be
Cd
Co
Cr
Cu
F Hg
Mn
Ni
Pb
Sb
Tl
V Zn
o-A
min
olev
ulin
ic a
cid
But
oxya
ceti
e ac
ido-
Cre
sol
Eth
oxya
ceti
c ac
id2,
5 H
exan
dion
eH
ippu
rie
acid
l-H
ydro
xypy
rene
Man
deli
c ac
idN
-met
hylf
orm
amid
eM
ethy
lhip
puri
c ac
ids
t,t-M
ucon
ic a
cid
Pen
tach
loro
phen
olP
heno
lP
heny
l gly
oxyl
ic a
cid
S-
phen
ylm
erca
ptur
ic a
cid
2- T
hio-
thia
zoli
dine
-4-
carb
oxyl
ic a
cid
Tri
ehlo
roac
etic
aci
dA
lcoh
ols/
keto
nes
Met
hano
l, ac
eton
e,M
ethy
leth
ylke
tone
Sch
alle
r et
. al1
45, 1
47–1
49)
Leh
nert
150)
Hei
nric
h-R
amm
151)
Tab
le 5
.T
he m
ost p
opul
ar E
xter
nal Q
uali
ty A
sses
smen
t Sch
emes
Org
aniz
erD
eter
min
ed c
hem
ical
sub
stan
ces
Blo
odS
erum
Uri
neR
efer
ence
s
Met
als
Sol
vent
sO
rgan
o-ch
lori
neM
etal
sIn
orga
nic
Org
anic
com
poun
dsco
mpo
unds
com
poun
ds
Occ
upat
iona
l med
icin
e
Env
iron
men
tal m
edic
ine
Cd
Pb
Hg
p,p’
DD
EH
CB
α, β
, γ H
CH
PC
Bs
(6 c
onge
ners
)P
CP
See
-oc
cupa
tion
alm
edic
ine
As
Cr
Hg
Ni
Pt
Hyd
roxy
pyre
ne, P
enta
chlo
roph
enol
, fou
rm
etab
olit
es o
f py
reth
roid
es(B
r2-C
A, c
is-C
I2-C
A,
tran
s-C
I2-C
A, 3
-PB
A)
2,5-
dich
loro
phen
ol, 2
,4,6
-tr
ichl
orop
heno
l, co
tini
ne,
nico
tine
(co
ntin
ued
on n
ext p
age)

38 J Occup Health, Vol. 47, 2005
http
://w
ww
.cdc
.gov
/nc
eh/d
ls/l
ead.
htm
(con
tinu
ed)
Org
aniz
erD
eter
min
ed c
hem
ical
sub
stan
ces
Blo
odS
erum
Uri
neR
efer
ence
s
Fin
nish
Ins
titu
te o
fO
ccup
atio
nal H
ealt
h,B
iom
onit
orin
gL
abor
ator
y,H
elsi
nki (
Fin
land
) F
IOH
.
man
deli
c ac
id, m
ethy
lene
dian
ilin
e,tr
ans,
tran
s-m
ucon
ic a
cid,
met
hylh
ippu
ric
acid
; phe
nol,
tric
hlor
oace
tic
acid
2,5
-hek
sane
dion
e,cr
eati
nine
and
rel
ativ
e de
nsit
y
Val
kone
n et
-al
.152
, 153
)
Wol
fson
EQ
A L
abor
ator
y,P
O B
ox 3
909,
Bir
min
gham
,B
15 2
UE
(Gre
at B
rita
in)
UK
NE
QA
S.
Cd,
Pb
Bul
lock
154)
Tay
lor
et a
l.155
)
Sch
ool o
f B
iom
edic
al a
ndL
ife
Sci
ence
s U
nive
rsit
y of
Sur
rey,
Gui
ldfo
rd, S
urre
y,G
U2
7XH
(Gre
at B
rita
in).
UK
NE
QA
S.
As,
Cd,
Pb,
Hg,
Mn
Al,
Cu,
Se,
Zn
Rep
ort a
ndD
irec
tory
, 4th
Edi
tion
, 200
0, U
KN
EQ
AS
Dan
ish
Nat
iona
l Ins
titu
teof
Occ
upat
iona
l Hea
lth
-A
MI,
Den
mar
k(D
EQ
AS
).
Pb
Chr
isit
anse
n et
al .1
56)
Cen
tre
de T
oxic
olog
ie d
uQ
uébe
c, T
oxic
olog
yL
abor
ator
y, Q
uébe
c,C
anad
a (C
TQ
).
Cd,
Pb,
Hg
Al,
Cu,
Mn,
Se,
Zn
As,
Cd,
Cr,
Cu,
F, H
g, P
b, S
e, Z
nht
tp:/
/ww
w.c
tq.q
c.ca
/
Cen
ter
for
Dis
ease
Con
trol
and
Pre
vent
ion,
Blo
od L
ead
Lab
orat
ory
Ref
eren
ce S
yste
m,
US
A (
BL
LR
C).
Pb

39Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
NIS
T26
71a,
267
2b,
1589
, 956
A,
955,
966
Tab
le 6
. S
elec
ted
com
mer
cial
ly a
vail
able
ref
eren
ce m
ater
ials
for
bio
logi
cal m
onit
orin
g
Sou
rce/
labe
l Ord
erM
atri
xA
naly
te(s
) w
ith
cert
ifie
dA
naly
te(s
) w
ith
non-
cert
ifie
dN
umbe
r of
conc
entr
atio
nsco
ncen
trat
ions
conc
entr
atio
n le
vels
Hum
an u
rine
Hum
an s
erum
Bov
ine
bloo
d
F, H
g
Ca,
K, L
i, M
g, N
aP
CB
’s, P
esti
cide
s an
d D
ioxi
n/F
uran
s
Cd,
Pb,
2 1 1 2 or
4
BC
R19
4, 1
95, 1
96,
397,
304,
573,
574
, 575
Bov
ine
bloo
d
Hum
an h
air
Hum
an s
erum
Hum
an s
erum
Cd,
Pb
Cd,
Hg,
Pb,
Se,
Zn
Ca,
Mg,
Li
crea
tini
ne
3 1 1
Ani
mal
blo
odH
uman
hai
rB
r, C
a, C
u, F
e, K
, Na,
RB
, S, S
e, Z
nH
g, m
ethy
lmer
cury
Mg,
Ni,
P, P
bC
a, C
u, M
g,
1 2
Rec
ipe
(Cli
nChe
ck®
)R
P88
83, R
P88
81,
RP
8882
RP
8883
, RP
8884
,R
P88
85
RP
8847
, RP
8848
,R
P88
49
RP
8867
, RP
8868
,R
P88
69
RP
8860
RP
8861
Hum
an s
erum
Hum
an p
lasm
a
Hum
an u
rine
Hum
an u
rine
Tox
ic o
rgan
ic c
ompo
unds
Hum
an s
erum
Org
anoc
hlor
ic c
ompo
unds
Al,
As,
Cd,
Co,
Cr,
Cu,
F, F
e, M
n, N
i, S
e, Z
n
Al,
As,
Cd,
Co,
Cr,
Cu,
Fe,
Li,
Mg,
Ni,
Pt,
Se,
Zn
Al,
As,
Cd,
Co,
Cr,
Cu,
F, H
g, M
n, N
i, P
t, P
b, S
b, T
h, Z
n
Cot
inin
e, n
icot
ine,
2,5
-dic
hlor
ophe
nol,
HA
, l-H
P, o
-cre
sol,
MA
, MH
A, t
,t-M
CA
, PC
P, p
heno
l, P
GA
, TC
A, p
yret
hroi
dm
etab
olite
s, (
Br 2
-CA
, cis
-CI 2
-CA
, tra
ns-C
I 2-C
A, 3
-PB
A)
PC
B 2
8, 5
2, 1
01, 1
38, 1
53, 1
80
3 2 2 2 3
(con
tinu
ed o
n ne
xt p
age)
IAE
AA
1308
5
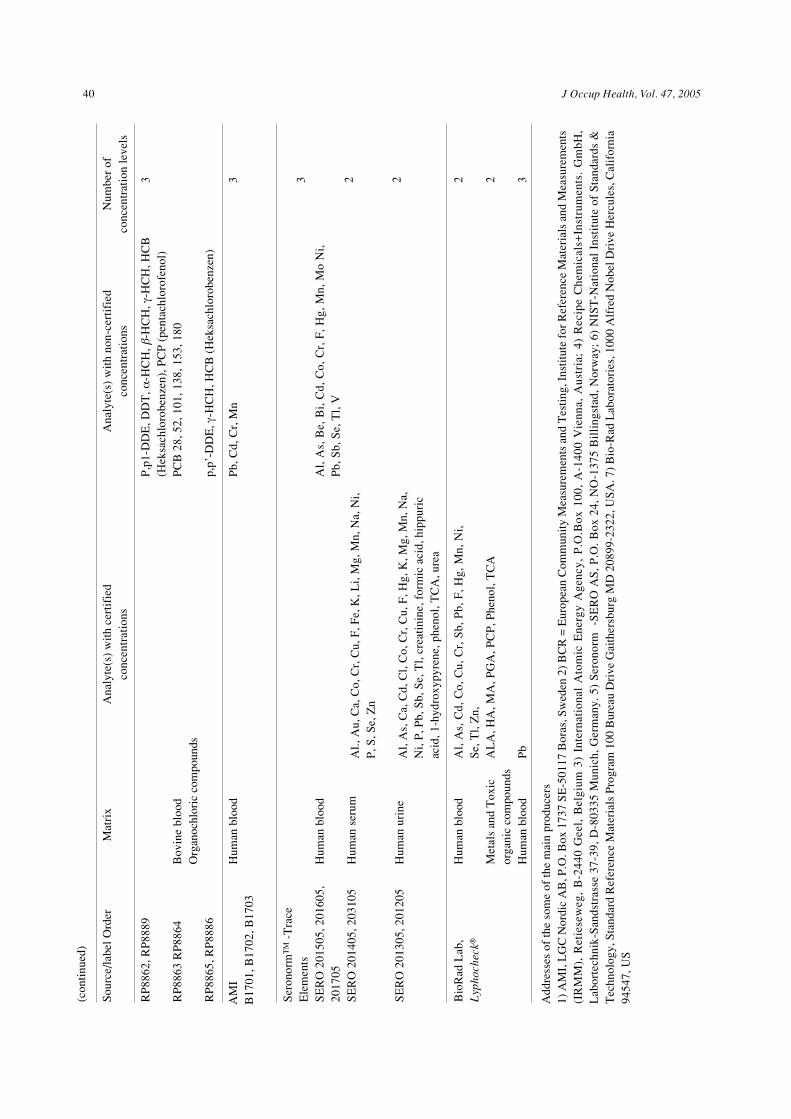
40 J Occup Health, Vol. 47, 2005
P,p
1-D
DE
, DD
T, α
-HC
H, β
-HC
H, γ
-HC
H, H
CB
(Hek
sach
loro
benz
en),
PC
P (
pent
achl
orof
enol
)P
CB
28,
52,
101
, 138
, 153
, 180
p,p’
-DD
E, γ
-HC
H, H
CB
(H
eksa
chlo
robe
nzen
)
3R
P88
62, R
P88
89
RP
8863
RP
8864
RP
8865
, RP
8886
Bov
ine
bloo
dO
rgan
ochl
oric
com
poun
ds
(con
tinu
ed)
Sou
rce/
labe
l Ord
erM
atri
xA
naly
te(s
) w
ith
cert
ifie
dA
naly
te(s
) w
ith
non-
cert
ifie
dN
umbe
r of
conc
entr
atio
nsco
ncen
trat
ions
conc
entr
atio
n le
vels
AM
IB
1701
, B17
02, B
1703
Hum
an b
lood
Pb,
Cd,
Cr,
Mn
Ser
onor
mT
M -
Tra
ceE
lem
ents
SE
RO
201
505,
201
605,
2017
05S
ER
O 2
0140
5, 2
0310
5
SE
RO
201
305,
201
205
Hum
an b
lood
Hum
an s
erum
Hum
an u
rine
Al.,
Au,
Ca,
Co,
Cr,
Cu,
F, F
e, K
, Li,
Mg,
Mn,
Na,
Ni,
P, S
, Se,
Zn
Al,
As,
Ca,
Cd,
Cl,
Co,
Cr,
Cu,
F, H
g, K
, Mg,
Mn,
Na,
Ni,
P, P
b, S
b, S
e, T
l, cr
eati
nine
, for
mic
aci
d, h
ippu
ric
acid
, 1-h
ydro
xypy
rene
, phe
nol,
TC
A, u
rea
Al,
As,
Be,
Bi,
Cd,
Co,
Cr,
F, H
g, M
n, M
o N
i,P
b, S
b, S
e, T
l, V
3 2 2
Bio
Rad
Lab
,L
ypho
chec
k®H
uman
blo
od
Met
als
and
Tox
icor
gani
c co
mpo
unds
Hum
an b
lood
Al,
As,
Cd,
Co,
Cu,
Cr,
Sb,
Pb,
F, H
g, M
n, N
i,S
e, T
l, Z
n,A
LA
, HA
, MA
, PG
A, P
CP
, Phe
nol,
TC
A
Pb
2 2 3
Add
ress
es o
f th
e so
me
of th
e m
ain
prod
ucer
s1)
AM
I, L
GC
Nor
dic
AB
, P.O
. Box
173
7 S
E-5
0117
Bor
as, S
wed
en 2
) B
CR
= E
urop
ean
Com
mun
ity
Mea
sure
men
ts a
nd T
esti
ng, I
nsti
tute
for
Ref
eren
ce M
ater
ials
and
Mea
sure
men
ts(I
RM
M),
Re t
iese
we g
, B
-244
0 G
e el,
Be l
gium
3)
Inte
rna t
iona
l A
tom
ic E
nerg
y A
genc
y, P
.O.B
ox 1
00,
A-1
400
Vie
nna ,
Aus
tria
; 4)
Re c
ipe
Che
mic
a ls+
Inst
rum
ents
. G
mbH
,L
abor
tech
nik-
San
dstr
asse
37-
39, D
-803
35 M
unic
h, G
erm
any.
5)
Ser
onor
m
-SE
RO
AS
, P.O
. Box
24,
NO
-137
5 B
illi
ngst
ad, N
orw
ay;
6) N
IST
-Nat
iona
l In
stit
ute
of S
tand
ards
&T
echn
olog
y, S
tand
ard
Ref
eren
ce M
ater
ials
Pro
gram
100
Bur
eau
Dri
ve G
aith
ersb
urg
MD
208
99-2
322,
US
A. 7
) B
io-R
ad L
abor
ator
ies,
100
0 A
lfre
d N
obel
Dri
ve H
ercu
les,
Cal
ifor
nia
9454
7, U
S
3
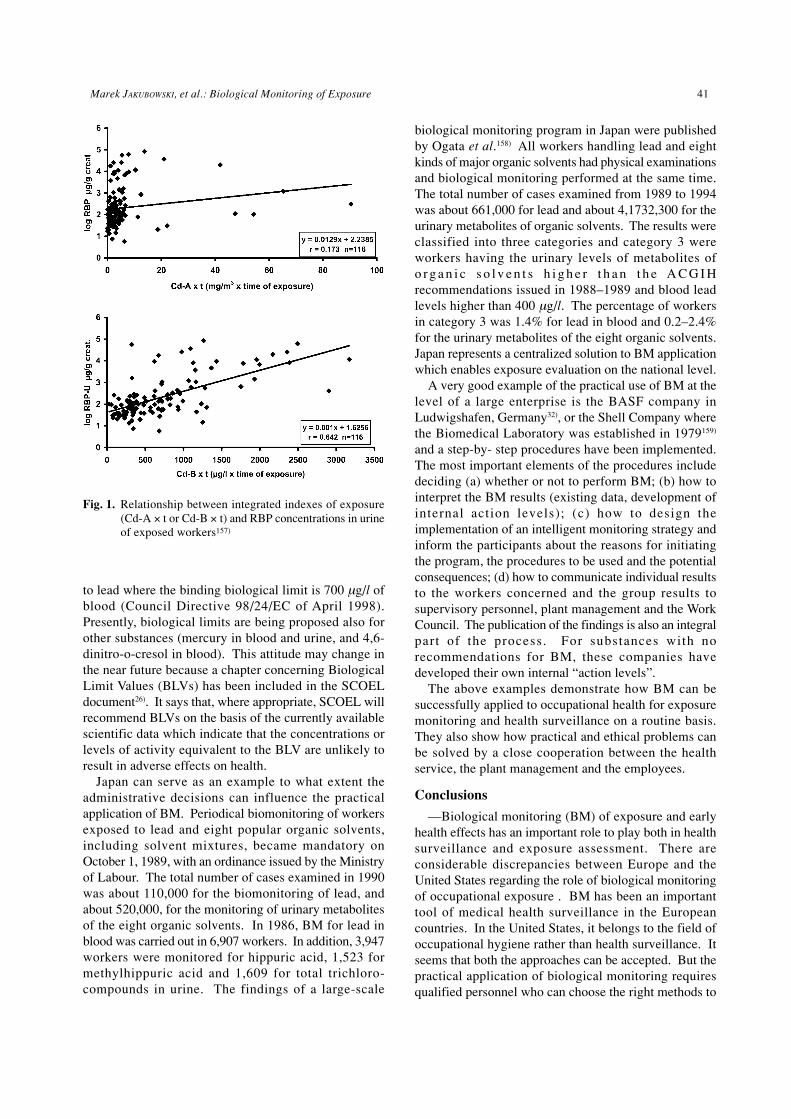
41Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
to lead where the binding biological limit is 700 µg/l ofblood (Council Directive 98/24/EC of April 1998).Presently, biological limits are being proposed also forother substances (mercury in blood and urine, and 4,6-dinitro-o-cresol in blood). This attitude may change inthe near future because a chapter concerning BiologicalLimit Values (BLVs) has been included in the SCOELdocument26). It says that, where appropriate, SCOEL willrecommend BLVs on the basis of the currently availablescientific data which indicate that the concentrations orlevels of activity equivalent to the BLV are unlikely toresult in adverse effects on health.
Japan can serve as an example to what extent theadministrative decisions can influence the practicalapplication of BM. Periodical biomonitoring of workersexposed to lead and eight popular organic solvents,including solvent mixtures, became mandatory onOctober 1, 1989, with an ordinance issued by the Ministryof Labour. The total number of cases examined in 1990was about 110,000 for the biomonitoring of lead, andabout 520,000, for the monitoring of urinary metabolitesof the eight organic solvents. In 1986, BM for lead inblood was carried out in 6,907 workers. In addition, 3,947workers were monitored for hippuric acid, 1,523 formethylhippuric acid and 1,609 for total trichloro-compounds in urine. The findings of a large-scale
biological monitoring program in Japan were publishedby Ogata et al.158) All workers handling lead and eightkinds of major organic solvents had physical examinationsand biological monitoring performed at the same time.The total number of cases examined from 1989 to 1994was about 661,000 for lead and about 4,1732,300 for theurinary metabolites of organic solvents. The results wereclassified into three categories and category 3 wereworkers having the urinary levels of metabolites ofo r g a n i c s o l v e n t s h i g h e r t h a n t h e A C G I Hrecommendations issued in 1988–1989 and blood leadlevels higher than 400 µg/l. The percentage of workersin category 3 was 1.4% for lead in blood and 0.2–2.4%for the urinary metabolites of the eight organic solvents.Japan represents a centralized solution to BM applicationwhich enables exposure evaluation on the national level.
A very good example of the practical use of BM at thelevel of a large enterprise is the BASF company inLudwigshafen, Germany32), or the Shell Company wherethe Biomedical Laboratory was established in 1979159)
and a step-by- step procedures have been implemented.The most important elements of the procedures includedeciding (a) whether or not to perform BM; (b) how tointerpret the BM results (existing data, development ofinternal action levels); (c) how to design theimplementation of an intelligent monitoring strategy andinform the participants about the reasons for initiatingthe program, the procedures to be used and the potentialconsequences; (d) how to communicate individual resultsto the workers concerned and the group results tosupervisory personnel, plant management and the WorkCouncil. The publication of the findings is also an integralpart of the process. For substances with norecommendations for BM, these companies havedeveloped their own internal “action levels”.
The above examples demonstrate how BM can besuccessfully applied to occupational health for exposuremonitoring and health surveillance on a routine basis.They also show how practical and ethical problems canbe solved by a close cooperation between the healthservice, the plant management and the employees.
Conclusions
—Biological monitoring (BM) of exposure and earlyhealth effects has an important role to play both in healthsurveillance and exposure assessment. There areconsiderable discrepancies between Europe and theUnited States regarding the role of biological monitoringof occupational exposure . BM has been an importanttool of medical health surveillance in the Europeancountries. In the United States, it belongs to the field ofoccupational hygiene rather than health surveillance. Itseems that both the approaches can be accepted. But thepractical application of biological monitoring requiresqualified personnel who can choose the right methods to
Fig. 1. Relationship between integrated indexes of exposure(Cd-A × t or Cd-B × t) and RBP concentrations in urineof exposed workers157)
42 J Occup Health, Vol. 47, 2005
evaluate health risk (medical health surveillance) orquantify dermal exposure, or the quality of individualprotective measures (mask, clothes). Small and mediumenterprises can rent services in regional laboratories.
—In spite of the tendency to reduce the occupationalexposure limits, the recommended BAT or BEI valuescan be applied for routine measurements. New areas ofBM application to occupational exposure include thedetermination of DNA and protein adducts, unchangedvolatile organic compounds in urine, the monitoring ofexposure to pesticides, antineoplastic drugs, hard metals,and polycyclic aromatic hydrocarbons. These areasrequire sophisticated analytical methods such as GC-MS-MS, HPLC-MS-MS and ICP-MS.
—More attention should be paid to the developmentof truly health-based biomarkers of exposure based onthe dose-effect and dose-response relationships.
—In the general environment, BM is the most valuabletool for acquiring knowledge of current levels of internalexposure to xenobiotics, identifying the hot spots anddevelopments in the trends of exposure. BM can providepolicy makers with more accurate information on thecontrol measures undertaken. At present, the main areasinclude heavy metals, persistent organic pollutants andpesticides.
—The use of BM for the assessment of exposure tochemical substances has recently found its place in theofficial recommendations of the European Union and isassumed to be helpful for the prevention of adverse healtheffects. This may position biological monitoring next toenvironmental monitoring where the data for theinterpretation of results are available. Therefore, it wouldbe worthwhile to include BM in the training curriculafor occupational hygienists and occupational physicians.
Acknowledgments: This review was supported byGrant NMALRI-D1.1NOFE-0207from the EuropeanChemical Industry Council- CEFIC.
Glossary of abbreviations:
β2M β
2 microgobulin
ACGIH The American Conference of GovernmentalIndustrial Hygienists
AchE acethylcholinesteraseADI acceptable daily intakeAHH arhydrocarbon hydroxylaseBaP benzeno [a] pyreneBAT Biologische ArbeitstofftoleranzwerteBEI Biological Exposure IndicesBGV benchmark guidance valuesBLV biological limit valuesBM biological monitoringBMDL bench-mark doseCBD chronic beryllium diseaseCDC Center for Disease Control and Prevention
Cd-U cadmium in urineCHP chlorpyrifosCHPM chlorpyrifos-methylCNS central nervous systemDFG Deutsche ForschungsgemeinschaftEKA exposure equivalents for carcinogenic
materialsEM environmental monitoringEPA Environmental Protection AgencyFL-AAS —flame atomic absorption spectrometryGC gas chromatographyGC-ECD gas chromatography with electron capture
detectorGC-FPD gas chromatography with photometric
detectionGC-MS gas chromatography with mass detectionGF-ASA flameless atomic absorption spectrometryHBM human biological monitoring valuesHC α
1-microglobulin
HFC high frequency cellsHg-H mercury in hairHGV health guidance valuesHP hydroxy-pyreneHPLC high-pressure liquid chromatographyHS head spaceHS-SPME head space solid phase microextractionIPC-MS inductively coupled plasma with mass
spectrometryIPCS International Program of Chemical SafetyLOAEL lowest observed adverse effect levelLOD limit of detectionMAK maximum concentration in the workplaceMCPA 4-chloro-2-methylphenoxyacetic acidMS mass detectorMTAE methyl tert-amyl etherMTBE methyl tert-butyl etherNAG N-acetyl β-D glucosaminidaseNHANES National Health and Nutrition Examination
SurveyNOAEL no observed adverse effect levelOEL occupational exposure limitOP organophosphorous pesticidesPAH policyclic aromatic hydrocarbonsPb-B lead in bloodPTWI Provisionally Tolerated Weekly IntakeRBP retinol binding proteinRfD reference doseSCOEL Scientific Committee on Occupational
Exposure LimitsTAME tert-amyl methyl etherTCPyr 3,5,6-trichloro-2-piridinolTLV threshold limit valueTLV-TWA threshold limit value—time weighted averageTRK technical exposure limitsUS EPA Environmental Protection Agency (USA)
43Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
VOC volatile organic compoundsWHO-FAO World Health Organization—Food and
Agricultural Organization
References
1) WHO. Air Quality Guidelines for Europe. SecondEdition. WHO Regional Publications, European Series,No 91. Copenhagen, 2000.
2) WHO. Guidelines for Drinking-water Quality. SecondEdition. Vol.1. Geneva, 1993.
3) ACGIH. TLVs and BEIs Based on the Documentationof the Threshold Limit values for Chemical Substancesand Physical Agents & Biological Exposure Indices.Cincinnati: OH, 2003.
4) DFG Deutsche Forschungsgemeinschaft. List of MAKand BAT Values. Wiley-VCH Verlag, Weinheim, 2003.
5) Teisinger J, Skramovsky S, Srbova J. Investigationsof Biological Media in Industrial Toxicology. Prague:Statni Zdrovotni Nakladitelstvi, 1956: 127 (in Czech)
6) HB Elkins: The Chemistry of Industrial Toxicology.2nd edn. New York: John Wiley and Sons, Inc., 1959:452
7) WM Draper: Biological Monitoring: Exquisite researchprobes, risk assessment, and routine exposuremeasurement. Anal Chem 73, 2745–2760 (2001)
8) P Hoet and V Haufroid: Biological monitoring: stateof art. Occup Environ Med 54, 361–366 (1997)
9) MS Morgan: The biological exposure indices: A keycomponent of protecting workers from toxic chemicals.Environ Health Perspect 105, Suppl.1, 105–114 (1977)
10) A Aitio: Biomarkers and their use in occupationalmedicine. Scand J Work Environ Health 25, 521–528(1999)
11) R Heinrich-Ramm, M Jakubowski, B Heinzow, J MolinChristensen, E Olsen and O Hertel: Biologicalmonitoring for exposure to volatile organic compounds(IUPAC Recommendations 2000). Pure Appl Chem 72,385–436 (2000)
12) A Sato: Confounding factors in biological monitoringof exposure to organic solvents. Int Arch OccupEnviron Health 65, S61–S67 (1993)
13) MS Morgan and KH Schaller: An analysis of criteriafor biological limit values developed in Germany andin the United States. Int Arch Occup Environ Health72, 195–102 (1999)
14) Piotrowski JK. Exposure Tests for Organic Compoundsin Industrial Toxicology. Cincinnati: U.S. Departmentof Health, Education and Welfare, 1977: 137.
15) WHO. Biological Monitoring of Chemical Exposurein the Workplace. Volume 1. Geneva, 1996: 300.
16) WHO. Biological Monitoring of Chemical Exposurein the Workplace. Volume 2. Geneva, 1996: 203.
17) Que Hee SS. Biological Monitoring. An Introduction.Van Nostrand Reinhold, N.Y.
18) Lauwerys RR, Hoet P. Industrial Chemical Exposure.Guidelines for Biological Monitoring. London, N.Y.,Washington D.C.: Lewis Publishers, Boca Raton, 1993:318.
19) Lauwerys RR, Hoet P: Industrial Chemical Exposure.
Guidelines for Biological Monitoring. Third edition.London, N.Y., Washington D.C.: Lewis Publishers,Boca Raton, 2001: 638.
20) ACGIH. Documentation of the TLVs and BEIs withother Worldwide Occupational Exposure Values.Cincinnati: OH, 2003.
21) DFG. Deutsche Forschungsgemeinschaft: BiologicalExposure Values for Occupational Toxicants andCarcinogens. Critical data Evaluation for BAT and EKAValues. Volume 1. (Henschler D., Lehnert G., eds).VCH Verlag,Weinheim, 1994: 235.
22) DFG. Deutsche Forschungsgemeinschaft: BiologicalExposure Values for Occupational Toxicants andCarcinogens. Critical data Evaluation for BAT and EKAValues. Volume 2. (Greim H, Lehnert G, eds). VCHVerlag, Weinheim, 1995: 221
23) DFG. Deutsche Forschungsgemeinschaft: BiologicalExposure Values for Occupational Toxicants andCarcinogens. Critical data Evaluation for BAT and EKAValues. Volume 3. (Greim H., Lehnert G., eds). VCHVerlag,Weinheim, 1994: 264.
24) IPCS. Biomarkers and Risk Assessment: Concepts andPrinciples. Environmental Health Criteria. Vol. 155.World Health Organization, Geneva, 1993.
25) Opinion of the European Group on Ethics in Scienceand New technologies to the European Commission:Ethical Aspects of genetic testing in the Workplace.No18. Final July 2003.
26) SCOEL. Methodology for the derivation ofoccupational exposure limits: Key documentation.European Commission. Directorate-General forEmployment, Industrial Relations and Social Affairs,1999.
27) Health & Safety Laboratory. Guidance on LaboratoryTechniques in Occupational Medicine. Ninth Edition,2002.
28) HK Wilson: Biological monitoring values foroccupational exposure: a United Kingdom perspective.Int Arch Occup Environ Health, 72, 274–278, (1999).
29) Ty ö t e r v e y s l a i t o s . K e m i k a a l i a l t i s t u m i s e nBiomonitorrointi. Näyytteenotto-ohjeet, 2003.
30) S Ghittori, A Alessio, L Maestri, S Negri, M Sgroi andP Zadra: Schede informative per il monitoraggiobiologico. Giornale Italiano di medicina del Lavoroed Ergonomia 24, 3 Suppl (2002)
31) ˛ .
CIOP. Miedzyresortowa Komisja ds. Najwyzszych˛ .
´ ˛ .
´Dopuszczalnych Stezen i Natezen Czynników´Szkodliwych dla Zdrowia w Srodowisku Pracy.
´ ´Czynniki Szkodliwe w Srodowisku Pracy, wartoscidopuszczalne. CIOP, Warszawa 2003.
32) A Zober and W Will: Biological monitoring and riskassessment in occupational settings. Int Arch OccupEnviron health 68, 389–393 (1996)
33) R Lauwerys, A Bernard, JP Buchet and H Roels:Assessment of the health impact of environmentalexposure to cadmium: cont r ibut ion of theepidemiological studies carried out in Belgium.Environmental Research 62, 200–206 (1993)
34) A Schütz and CG Elinder: Low-level exposure tocadmium and early kidney damage; the OSCAR study.
44 J Occup Health, Vol. 47, 2005
Occup Environ Med 57, 668–672 (2000)35) CW Noonan, SM Sarasua, D Campagna, SJ Kathman,
JA Lybarger and PW Mueller: Effects of exposure tolow levels of environmental cadmium on renalbiomarkers. Environ Health Perspect 110, 151–155,(2002)
36) ´M Trzcinka-Ochocka, M Jakubowski, G Razniewska,⁄T Halatek and A Gazewski: The effects of
environmental cadmium exposure on kidney function:the possible influence of age. Environ Res 95, 143–150 (2004)
37) L Järup, M Berglund, CG Elinder, G Nordberg and MVahter: Health effects of cadmium exposure-a reviewof the literature and a risk estimate. Scand J workEnviron Health 24, (suppl 1) 1–51 (1998)
38) IPCS. Inorganic Lead. Environmental Health Criteria.Geneva: WHO, 1995.
39) Centers for Disease Control. Preventing LeadPoisoning in Young Children. 1991.
40) RL Canfield, CR Henderson, DA Cory-Slechta, C Cox,TA Jusko and B Lanphear: Intellectual impairment inchildren with blood lead concentrations below 10 µgper decilitre. N Engl J Med 348, 1517–1526 (2003)
41) MJ Trepka, J Heinrich, Ch Krause: The internal burdenof lead among children in smelter town-a small areaanalysis. Environ Res 72, 118–130 (1997).
42) M Cikrt, Z Smerhovsky and K Blaha: Biologicalmonitoring of child lead exposure in the CzechRepublic. Environ Health Perspect 105, 406–411(1997)
43) M Berglund, B Lind, E Lannero and M Vahter: A pilotstudy of lead and cadmium exposure in young childrenin Stockholm, Sweden: Methodological considerationsusing capillary blood microsampling. Arch EnvironContam Toxicol 27, 281–287 (1994)
44) ´M Jakubowski, M Trzcinka-Ochocka, G Razniewska,JM Christensen and A Starek: Blood lead in the generalpopulation in Poland. Int Arch Occup Environ Health68, 193–198 (1996)
45) Toxicological Profile. U.S.Department of Health andHuman Services. Toxicological Profile for Lead(Update ). July, 1999.
46) IPCS. Methylmercury. Environmental Health Criteria,Vol. 101. WHO, Geneva, 1990.
47) K Murata, E Budtz-Jorgernsen and P Grandjean:Benchmark dose calculation for methylmercury-associated delays on evoked potential latencies in twocohorts of children. Risk Analysis 22, 465–474 (2002).
48) E Budtz-Jorgensen, P Grandjean, N Keiding, RF Whiteand P Weiche: Benchmark dose calculations ofmethylmercury-associated neurobehavioral deficits.Toxicology Letters, 112–113, 193–199 (2000).
49) KS Crump, T Kjellstrom, AM Shipp, A Silvers and AStewart: Influence of prenatal mercury exposure uponscholastic and psychological test performance:benchmark analysis of a New Zealand cohort. RiskAnalysis 18, 701–713 (1998)
50) G Drasch, E Wanghofer and G Roider: Are blood, urine,hair, and muscle valid biomonitors for the internalburden of men with the heavy metals: mercury, lead
and cadmium? Trace Elements and Electrolytes 14,116–123 (1997)
51) P Grandjean, P Weihe and PJ Jorgensen: Impact ofmaternal seafood diet on foetal exposure to mercury,selenium and lead. Arch Environ Health 47, 185–195(1992)
52) A Oskarsson, A Schultz and S Skerfving: Total andinorganic mercury in breast milk in relation to fishconsumption and amalgam in lactating women. ArchEnviron Health 51, 234–241 (1996)
53) A Renzoni, F Zino and E Franchi: Mercury levels alongthe food chain and risk for exposed populations.Environ Res 77, 68–72 (1998)
54) U Ewers, C Krause, C Schulz and M Wilhelm:Reference values and human biological monitoringvalues for environmental toxins. Report on the workand recommendations of the Commission on HumanBiological Monitoring of the German FederalEnvironmental Agency. Int Arch Occup Environ Health72, 255–260 (1999)
55) M Wilhelm, U Ewers and Ch Schultz: Revised andnew reference values for some trace elements in bloodand urine for human biomonitoring in environmentalmedicine. Int J Hyg Environ Health 207, 69–73 (2004)
56) A Duggan, G Charnley, W Chen, A Chukwudebe, RHawk and RI Krieger : Di-a lkyl phosphatebiomonitoring data: assessing cumulative exposure toorganophosphate pesticides. Reg Toxicol Pharmacol37, 382–393 (2003)
57) CDC. Second National Report on Human Exposure toEnvironmental Chemicals. National Center forEnvironmental Health. Publication No 03-0572,October 2003. Web site:www.cdc.gov/exposure report.
58) KH Schaller and J Angerer: Biomonitoring in derUmweltmedizin. Umweltmed Forsch Prax 3, 168–175(1998) (in German)
59) Christensen JM. Human exposure to metals. Factorsinfluencing Interpretation of biomonitoring results.Copenhagen: National Institute of Occupational Health,1995.
60) L Alessio: Reference values for the study of low dosesof metals. Int Arch Occup Environ Health 65, S23–S27 (1993)
61) O Vesterberg, L Alessio and D Brune: Internationalproject for producing reference values forconcentrations of trace elements in human blood andurine -TRACY. Scand J Work Environ Health suppl.1, 19–26 (1993)
62) R Cornelis, B Heinzow and RFM Herber: Samplecollection guidelines for trace elements in blood andurine. Pure Appl Chem, 67, 1575–1568 (1995)
63) K Schmidt, P Lederer, T Goen, K H Schaller, H Strebl,A Weber, J Angerer and G Lehnert: Internal exposureto hazardous substances of persons from variouscontinents: investigations on exposure to differentorganochlorine compounds. Int Arch Occup EnvironHealth 69, 399–406 (1997)
64) FRX Van Leeuwen and R Malisch: Results of the thirdround of the WHO-coordinated study on the levels ofPCBs, PCDDs and PCFFs in human mi lk .
45Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
Organohalogen Compounds 56, 311–316 (2002)65) MD Gerhardsson, G Kazantzis and A Schutz:
Evaluation of selected publications on reference valuesfor lead in blood. Scand J Work Environ Health 31,325–331 (1996)
66) ⁄W Wesolowski and JP Gromiec: Occupational exposurein Polish paint and lacquer industry. Int J Occup MedEnviron Health 10, 79–88 (1997)
67) M Ikeda: Solvents in urine as exposure markers.Toxicology Letters 108, 99–106 (1999)
68) FJ Klocke and H Rahan: The arterial-alveolar inert gasdifference in normal and emphysematous subjects asindicated by the analysis of urine. J Clin Invest 40,286–294 (1961)
69) S Ghittori, M Imbriani, G Pezzagno and E Capodaglio:The urinary concentration of solvents as a biologicalindicator of exposure: Proposal for the biologicalequivalent exposure limit for nine solvents. Am IndHyg Assoc J 48, 786–790 (1987)
70) M Hakkola, L Saarinen and K Pekari: Exposure togasoline vapor during offloading of tankers and railwaywagons and biological multicompartment monitoring.J Occup Health 43, 287–290 (2001)
71) S Vainiotalo, K Pekari and A Aitio: Exposure to methyltert-butyl ether and tert-amyl methyl ether fromgasoline during tank lorry loading and its measurementusing biological monitoring. Int Arch Occup EnvironHealth 71, 391–396 (1988)
72) L Saarinen, M Hakkola, K Pekari, K Lappalainen andA Aitio: Exposure of gasoline road-tanker drivers tomethyl tert-butyl ether and methyl tert-amyl ether. IntArch Occup Environ Health 71, 143–147 (1998)
73) T Kawai, K Mizunuma, T Yasugi, S Horiguchi and MIkeda: Toluene in blood as a marker of choice for low-level exposure to toluene. Int Arch Occup EnvironHealth, 66: 309–315 (1994)
74) A Tageuchi, T Kawai and ZW Zhang: Toluene, xylenesand xylene isomers in urine as biological indicators oflow-level exposure to each solvent; a comparativestudy. Int Arch Occup Environ Health 75, 387–393(2002)
75) S Ghittori, G Saretto and M Imbriani: Biologicalmonitoring of workers exposed to carbon tetrachloridevapor. Appl Occup Environ Hyg 9, 353–357 (1994)
76) S Fustinioni, R Giampiccolo, S Pulvirenti, M Burattiand A Colombi: Headspace solid-phase microextractionfor the determination of benzene, toluene, ethylbenzeneand xylenes in urine. J Chromatogr 723, 105–115(1999)
77) S Fustistoni, M Buratti, R Giampiccolo, G Brambilla,V Foa and A Colombi: Comparison between blood andurinary toluene as biomarkers of exposure to toluene.Int Arch Occup Environ Health 73, 389–396 (2000)
78) IPCS. Environmental Health Criteria 202. SelectedNon-heterocyclic Polycyclic Aromatic Hydrocarbons.Geneva: WHO, 1998.
79) MJ Ferreira, JP Buchet, JB Burrion, J Moro, L Cupers,JP Jacques and R Lauwerys: Determination of urinarythioethers, D-glucaric acid and mutagenicity afterexposure to polycyclic aromatic hydrocarbons assessed
by air monitor ing and measurements of 1-hydroxypyrene in urine: A cross-sectional study inworkers of coke and graphite-electrode-producingplants. Int Arch Occup Environ Health 65, 329–338(1994)
80) M J Ferreira, S Tas, M Dell’Omo, G Goormans, JBuchet and R Lauwerys : Determinants ofbenzo[a]pyrene diol epoxide adducts to hemoglobinin workers exposed to polycycl ic aromatichydrocarbons. Occup Environ Med 51, 451–455 (1994)
81) C Reuterwall, L Aringer, CG Elinder, A Rannug, JOLevin and L Juringe: Assessment of genotoxic exposurein Swedish coke-oven work by different methods ofbiological monitoring. Scand J Work Environ Health17, 123–132 (1991)
82) G Becher and A Bjorseth: Determination of exposureto polycyclic aromatic hydrocarbons by analysis ofhuman urine. Cancer Lett 17, 301–311 (1983)
83) P Venier, E Clonfero and D Cottica: Mutagenic activityand polycyclic aromatic hydrocarbon level in urine ofworkers exposed to coal tar pitch volatiles in anodeplant. Carcinogenesis 6, 749–752 (1985)
84) A Haugen, G Becher and C Bemestad: Determinationof polycyclic aromatic hydrocarbons in the urine,benzo[a]pyrene diol epoxide-DNA adducts inlymphocytes, and antibodies to the adducts in sera fromcoke-oven workers exposed to measured amounts ofpolycyclic aromatic hydrocarbons in the workatmosphere. Cancer Res 46, 4178–4183 (1986)
85) FJ Jongenellen, RP Bos and RBM Anzion: Biologicalmonitoring of polycyclic aromatic hydrocarbons. ScandJ Work Environ Health 12, 137–143 (1986).
86) PJ Boogaard and NJ van Sittert: Exposure to Polycyclicaromatic hydrocarbons in petrochemical industries bymeasurement of urinary 1-hydroxypyrene. OccupEnviron Med 51, 250–258 (1994)
87) JGM van Rooij, MM Bodelier-Bade, PM, J Hopmansand FJ Jongeneelen: Reduction of urinary 1-hydroxypyrene excretion in coke-oven workersexposed to Polycyclic aromatic hydrocarbons due toimproved hygienic skin protective measures. AnnOccup Hyg 38, 247–256 (1994)
88) R Quinlan, G Kowalczyk, K Gardiner and I Calvert:Exposure to polycyclic aromatic hydrocarbons in coalliquefaction workers: Impact of a workwear policy onexcretion of urinary 1-hydroxypyrene. Occup EnvironMed 52, 600–605 (1995)
89) FJ Jongeneelen: Biological exposure limit foroccupational exposure to coal tar pitch volatiles incoke-ovens. Int Arch Occup Environ Health 63, 511–515 (1992)
90) JO Levin, M Rhen and E Sikström: Occupational PAHexposure: urinary 1-hydroxypyrene levels in coke-ovenworkers, aluminium smelter pot-room workers,roadpavers, and occupationally non-exposed personsin Sweden. Sci Total Environ 193, 169–177 (1995)
91) GM van Rooij , MM Bodelier- Bade and FJJongeneelen: Estimation of individual dermal andrespiratory uptake of polycyclic aromatic hydrocarbonsin12 coke-oven workers. Brit J Ind Med 50, 623–632
46 J Occup Health, Vol. 47, 2005
(1993)92) EY Tjoe Ny, D Heedrik, H Kromhout and FJ
Jongenellen: The relationship between polycyclicaromatic hydrocarbons in air and urine of workers in aSöderberg potroom. Adv Ind Environ Hyg 54, 277–284 (1993)
93) JP Buchet, M Ferreira and JB Burrion: Tumor markersin serum, polyamines and modified nucleosides inurine, and cytogenetic aberrations in lymphocytes ofworkers exposed to Polycyclic aromatic hydrocarbons.Am J Ind Med 27, 523–543 (1995)
94) FJ Jongenellen: Benchmark guideline for urinary 1-hydroxypyrene as biomarker of occupational exposureto polycyclic aromatic hydrocarbons. Ann Occup Hyg45, 3–13 (2001)
95) E Clonfero, M Zordan and P Venier: Biologicalmonitoring of human exposure to coal tar. Urinaryexcretion of total Polycyclic aromatic hydrocarbons,1-hydroxypyrene, and mutagens in psoriatic patients.Int Arch Occup Environ Health 61, 363–368 (1989)
96) RM Santella, MG Nunes and R Blaskovicet:Quantification of polycyclic aromatic hydrocarbons,1-hydroxypyrene, and mutagenicity in urine of coaltar-treated psoriasis patients and untreated volunteers.Cancer Epidemiol Biomarkers Prev 3, 137–140 (1994)
97) .
´D Mielzynska and M Snit: Urine mutagenicity inworkers directly employed in coke production. Pol JOccup Med 5, 363–371 (1992)
98) DB Barr, JR Barr, WJ Driskell, RH Hill, DL Ashley,LL Needham, SL Head and EJ Sampson: Strategiesfor biological monitoring of exposure to contemporary-use pesticides. Toxicol Ind Health 15, 168–179 (1999)
99) Z Zhang, J Sun, S Chen, Y Wu and F He: Levels ofexposure and biological monitoring of perythroids insprayman. Brit J Ind Med 48, 82–86 (1991)
100) M Maroni, C Colosio, A Ferioli and A Fait: Biologicalmonitoring of pesticide exposure: a review. Toxicology143, 1–118 (2000)
101) C Aprea, C Colosio, T Mammone, C Minoia and MMaroni: Biological monitoring of pesticide exposure:a review of analytical methods. J Chromatogr B 769,191–219 (2002)
102) R Bravo, WJ Driskell, RJ Whitehead, LL Needhamand DB Barr: Quantification of dialkyl phosphatemetabolites of organophosphate pesticides in humanurine using GC-MS-MS with isotope internal standards.J Anal Tox 26, 245–252 (2002)
103) NJ Simcox, J Camp, D Kalman, A Stebbins, G Bellamy,I-Ch Lee and R Fenske: Farmworker exposure toorganophosphorus pesticide residues during applethinning in Central Washington State. Am Ind HygAssoc J 60, 752–761 (1999)
104) M Maroni and A Fait: Risk assessment and healthsurveillance of pesticide workers. Med Lav 89 (suppl2 ), S81–S90 (1998)
105) A Tuomainen, J Kangas, J Liesivuori and A Manninen:Biological monitoring of deltamethrin exposure ingreenhouses. Int Arch Occup Environ Health 69, 62–64 (1966)
106) G Leng, K-H Kühn and H Idel: Biological monitoring
of perythroids in blood and perythroid metabolites inurine: applications and limitations. Sci Total Environ199, 173–181 (1997)
107) SA Harris, PN Corey, AM Sass-Kortsak and JTPurdham: The development of a new method toestimate total daily dose of pesticides in professionalturf applicators following multiple and variedexposures in occupational settings. Int Arch OccupEnviron Health 74, 345–358 (2001)
108) WA Anwar: Biomarkers of exposure to pesticides.Environ Health Persp 105, Suppl 4, 801–806 (1997)
109) C L C u r l , R A F e n s k e a n d K E l e g e t h u n :Organophosphorous pesticide exposure of urban andsuburban preschool children with organic andconventional diets. Environ Health Persp 111, 377–382 (2003)
110) JL Adgate, DB Barr, CA Clayton, LA Eberly, NCGFreeman, PJ Lioy, LL Needham, ED Pellizarri, JJQuackenboss, AM Roy and K Sexton: Measurementof children’s exposure to pesticides: Analysis of urinarymetabolite levels in a probability-based sample.Environ Health Persp 109, 583–589 (2001)
111) RA Fenske, LChensheng, D Barr and L Needham:Children’s exposure to chloropyrifos and parathion inan agricultural community in central Washington State.Environ Health Persp 110, 549–553 (2002)
112) C Aprea, M Strambli, MT Novelli, L Lunghini and NBozzi: Biologic monitoring of exposure toorganophosphorous pesticides in195 Italian children.Env Health Persp 108, 521–525 (2000)
113) RM Whyatt, DB Barr, E Camann, PL Kinney, JR Barr,HF Andrews, LA, Hoepner, R Garfinkel, Y Hazi, AReyes, J Ramirez, Y Cosme and FP Parera:Contemporary-use pesticides in personal air samplesduring pregnancy and blood samples at delivery amongurban monitory mothers and newborns. Environ HealthPersp 111, 749–756 (2003)
114) C Loewenherz, RA Fenske, NJ Simcox, G Bellamyand D Ka lman: B io log ica l moni to r ing o forganophosphorous pesticide exposure among childrenof agricultural workers in central Washington state.Environ Health Persp 105, 1344–1353 (1997)
115) Angerer J. Biological monitoring in Occupational andenvironmental medicine—The present state of the artand future prospects. In: DFG Biological Monitoring.Prospects in Occupational and Environmental Medicine.Wiley- VCH Verlag, Weinheim, 2002: 5–15.
116) HM Koch, J Hardt and J Angerer: Biologicalmonitoring of exposure of the general population tothe organophosphorous pesticides chlorpyrifos andchlorpyrifos-methyl by determination of their specificmetabolite 3,5,6-trichloro-2-pyridinol. Int J HygEnviron Health 204, 175–180 (2001)
117) RH Hill Jr., SE Baker, C Rubin, E Esteban, SL Bailey,DB Shealy and LL Needham: Pesticide residues inurine of adults living in the United States: referencerange concentrations. Environ Res 71, 99–108 (1995)
118) E Zieglel, HJ Mason and J Baxter: Occupationalexposure to cytotoxic drugs in two UK oncology wards.Occup Environ Med 59, 608–612 (2002)
47Marek JAKUBOWSKI, et al.: Biological Monitoring of Exposure
119) AS Ensslin, R Huber, A Pethran, H Rommelt, R Schierland U Kulka: Biological monitoring of hospitalpharmacy personnel occupationally exposed tocytostatic drugs: urinary excretion and cytogeneticstudies. Int Arch Occup Environ Health 70, 205–208(1997)
120) C Minoia, E Sabbioni, P Apostoli, L Alessio and ECapaodaglio: Trace elements reference values in tissuefrom inhabitants of European cummunity. A study of46 elements in urine, blood and serum of Italiansubjects. Sci Total Environ 95, 89–105 (1990)
121) PJM Sessink, KA Boer, APH Schefhals, RBM Anzionand RP Bos: Occupational exposure to antineoplasticagents at several departments in a hospital. OccupEnviron Med 64, 105–112 (1992)
122) R Turci, C Sottani, A Ronchi and C Minoia: Biologicalmonitoring of hospital personnel occupationallyexposed to antineoplastic agents. Toxicol Lett 134, 57–64 (2002)
123) P Apostoli and KH Schaller: Urinary beryllium—asuitable tool for assessing occupational andenvironmental beryllium exposure? Int Arch OccupEnviron Health 74, 162–166 (2001)
124) KJ Nikula, DS Swafford and MD Hoover: Chronicgaranulomatous pneumonia and lymphocytic responsesinduced by inhaled beryllium metal. Toxicol Path 25,2–12 (1997)
125) T Kraus, TP Schramel, PKH Schaller, P Zöbelein, AWeber and J Angerer: Exposure assessment in the hardmetal manufacturing industry with spezial regard totungsten and its compounds. Occup Environ Med 58,631–634 (2001)
126) C Minoia, R Turci, C Sottani, A Achiavi, L Perbellini,S Angeleri, F Draicchio and P Apostoli: Applicationof high performance liquid chromatography/tandemmass spectrometry in the environmental monitoring ofhealth care personnel occupationally exposed tocyclophosphamide and ifosfamide. Rapid CommunMass Spectr 12, 1485–1493 (1998)
127) DC Paschal, BG Ting, JL Pirkle, DT Miller and KLCaldwell: Trace metals in urine of United Statesresidents: reference range concentrations. Environ Res76, 53–59 (1998)
128) R Wegner, R Heinrich-Ramm and D Nowak: Lungfunction, biological monitoring, and biological effectmonitoring of gemstone cutters exposed to beryls.Occup Environ Med 57, 133–139 (2000)
129) PB Farmer: DNA and protein adducts as markers ofgenotoxicity. Toxicol Lett 149, 3–9 (2004)
130) RJ Turesky and P Vouros: Formation and analysis ofheterocyclic aromatic amine-DNA adducts in vitro andin vivo. J Chromatogr B 802, 155–166 (2004)
131) VK Bhatnagar and G Talaska: Carcinogen exposureand effect biomarkers. Toxicol Lett 108, 107–116(1999)
132) GD Jahnke, CL Thompson, MP Walker, JE Gallagher,GW Lucier and RP DiAugustine: Multiple DNAadducts in lymphocytes of smokers and non-smokersde te rmined by 32P -pos t l abe l l i ng ana lys i s .Carcinogenesis 11, 205–211 (1990)
133) DH Phillip, A Hewer, CN Martin, RC Garner and MMKing: Correlation of DNA adduct levels in human lungwith cigarette smoking. Nature (London) 336, 790–792 (1988)
134) M Rojas, K Alexandrov, G Auburtin, A Wastiaux-Denamur, L Mayer, B Mahieu, P Sebastien and HBartsch: Anti-benzo[a]pyrene diolepoxide-DNAadducts levels in pheripheral mononuclear cells fromcoke-oven workers and the enhancing effect ofsmoking. Carcinogenesis 16, 1373–1376 (1995)
135) T Schettgen, HC Broding, J Angerer and H Drexler:Hemoglobin adducts of ethylene oxide, propyleneoxide, acrylonitrile and acrylamide-biomarkers inoccupational and environmental medcicine. ToxicolLett 134, 65–70 (2002)
136) L Hagmar, M Törnnqvist, C Nordander, I Rosen, MBruze, A Kautiainen, A-L Magnusson, B Malmberg, PAprea, F Granath and A Axmon: Health effects ofoccupational exposure to acrylamide using hemoglobinadducts as biomarkers of internal dose. Scand J WorkEnviron Health 27, 291–226 (2001)
137) PJ Boogaard, NJ van Sittert and HJJJ Megens: Urinarymetabolites and haemoglobin adducts as biomarkersof exposure to 1,3-butadiene: a basis for 1,3-butadienecancer risk assessment. Chem-Biol Interactions 135–136, 695–701 (2001)
138) SM Rappaport and K Yeowell-O’Connel: Proteinadducts as dosimeters of human exposure to styrene,styrene-7,8-oxide, and benzene. Toxicol Lett 108, 117–126 (1999)
139) C Magagnotti, F Orsi, R Bagnati, N Celli, D Rotilio, RFanelli and L Airoldi: Effect of diet on serum albuminand hemoglobin adducts of 2-amino-1-methyl-6-phenylimidazo[4,5-b] pyridine ( PhIP) in humans. IntJ Cancer 88, 1–6 (2000)
140) G Sabbioni: Biological monitoring of arylamines andnitroarenas. In: DFG Biological Monitoring. Prospectsin Occupational and Environmental Medicine.Weinheim: Wiley-VCH Verlag, 2002: 24–34.
141) DFG. Biological Moni tor ing. Prospects inOccupational and Environmental Medicine. Weinheim:Wiley-VCH Verlag, 2002.
142) ISO. International Organization for standardization(ISO), ISO/IEC Guide 58. Calibration and testinglaboratory accreditation systems: General requirementsfor operation and recognition. 1st ed. Geneva, 1993.
143) ISO. International Organization for standardization(ISO), ISO/IEC Guide 25. General requirements forthe competence of calibration and testing laboratories,3rd ed. Geneva, 2000.
144) CEN/CENELEC. European standard EN45001,General criteria for the operation of testing laboratories.Brusssels, Belgium: CEN/CENELEC The JointEuropean Standards Institution. (1989)
145) K-H Schaller, J Angerer and H Drexler: Qualityassurance of biological monitoring in occupational andenvironmental medicine. J Chromatogr 778, 403–417(2002)
146) J Angerer, K-H Schaller, eds. Analyses of HazardousSubstances in Biological Materials, Vols. 1 to

48 J Occup Health, Vol. 47, 2005
6,Weinheim, Germany, 1985–1999.147) K-H Schaller, J Angerer, G Lehnert, H Valentin and D
Welte: External quality control programmes in thetoxicological analysis of biological material in the fieldof occupational medicine—experiences from threeround-robins in the Federal Republic of Germany.Fresenius Z Anal Chem 326, 643–646 (1987)
148) K-H Schaller, J Angerer and G Lehnert: Internal andexternal quality control in the toxicological analysisof blood and urine samples in the federal Republic ofGermany. Int Arch Occup Environ Health 62, 537(1991)
149) K-H Schaller, J Angerer, D Weltle and H Drexler:External Quality Assurance program for biologicalmonitoring in occupational and environmentalmedicine, Rev Environ Health 16, 223–232 (2001)
150) G Lehnert, K-H Schaller and J Angerer: Report on thestatus of the external quality control programs foroccupational medical and environmental medicaltoxicological analyses in biological materials inGermany. Int Arch Occup Environ Health 72, 60–64(1999)
151) R Heinrich-Ramm, G Lehnert and J Angerer: TheGerman external quality assessment scheme inoccupational and environmental medicine. Ann IstSuper Sanità 32 (2), 247–251 (1996)
152) S Valkonen, K Engström, I Ahonen., P Mutanen and A
Aitio: FIOH external quality assessment scheme fororganic solvent metabolites. Ann Ist Super Sanità 32(2), 225–231 (1996)
153) S Valkonen and A Kallio: Finnish quality assuranceprogram for biological monitoring of organic solvents.Journal of Chromatogr B Analyt Technol Biomed LifeSci 778, 419–427 (2002)
154) D Bullock, N Smith and T Whitehead: External qualityassessment assays of lead in blood. Clin Chem 32 (10),1884–1889 (1986)
155) A Taylor and RJ Briggs: The Guilford trace elementsexternal quality assessment scheme. Ann Ist SuperSanità 32 (2) 253–259 (1996)
156) JM Christiansen and J Kristiansen: The Danish externalquality assessment scheme. Ann Ist Super Sanità 32(2) 221–224 (1996)
157) M Jakubowski, M Trzcinka-Ochocka, T Halatek, G´Razniewska and W Szymczak: Integrated indexes of
occupational exposure as predictors of kidneydysfunction. Int J Occup Environ Health, 15, 393–399(2002)
158) M Ogata, T Numano, M Hosokawa and H Michitsui:Large-scale biological monitoring in Japan. Sci TotalEnviron, 199, 197–204 (1997)
159) Boogaard PJ. Personal information on establishmentof the Shell Biomedical Laboratory. 2004.





![FDTD Simulation of Exposure of Biological Material to ... · arXiv:physics/0407054v1 [physics.bio-ph] 12 Jul 2004 FDTD Simulation of Exposure of Biological Material to Electromagnetic](https://img.pdfslide.us/doc/110x75/5ee1096fad6a402d666c1090/fdtd-simulation-of-exposure-of-biological-material-to-arxivphysics0407054v1.jpg)























