Embed Size (px)
Citation preview

This article was downloaded by: [McMaster University]On: 31 October 2014, At: 09:59Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Dual DiagnosisPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wjdd20
Biological Basis for the Co-morbidityBetween Smoking and Mood DisordersYann S. Mineur PhD a & Marina R. Picciotto PhD aa Yale School of Medicine, Department of Psychiatry , New Haven,Connecticut, USAPublished online: 04 May 2009.
To cite this article: Yann S. Mineur PhD & Marina R. Picciotto PhD (2009) Biological Basis for theCo-morbidity Between Smoking and Mood Disorders, Journal of Dual Diagnosis, 5:2, 122-130, DOI:10.1080/15504260902869964
To link to this article: http://dx.doi.org/10.1080/15504260902869964
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Journal of Dual Diagnosis, 5:122–130, 2009Copyright © Taylor & Francis Group, LLCISSN: 1550-4263 print / 1550-4271 onlineDOI: 10.1080/15504260902869964
Biological Basis for the Co-morbidity BetweenSmoking and Mood Disorders
YANN S. MINEUR, PhD and MARINA R. PICCIOTTO, PhDYale School of Medicine, Department of Psychiatry, New Haven, Connecticut, USA
Nicotine dependence is still the major preventable cause of deathin the developed world, and it has strong co-morbidity with mooddisorders including major depression. Depressed patients are morelikely to smoke cigarettes, and quitting can precipitate an episode ofdepression in some individuals. Interestingly, antidepressants, par-ticularly the atypical antidepressant bupropion, are therapeuticsthat can help smokers quit. Despite these observations, the under-lying biological factors of the relationship between smoking anddepression remain unclear. Results from clinical and preclinicalstudies have seemed somewhat paradoxical because heightenedcholinergic activity can induce depression, while both nicotine andnicotinic antagonists can be antidepressant-like. These observa-tions can be reconciled by considering that high-affinity nicotinicreceptors in the brain can be desensitized by chronic nicotine use,leading to blunted cholinergic activity. Based on this hypothesis,nicotinic antagonists have recently been tested as treatments fordepression in humans, particularly as adjunct therapy along withclassical antidepressants. These data suggest that the relationshipbetween smoking and depression may be partially explained bythe fact that depressed patients smoke in an effort to self-medicatedepressive symptoms by desensitizing their nicotinic receptors. Thispossibility suggests new avenues for treatment of both nicotine de-pendence and depressive disorders.
This work was supported by the State of Connecticut, Department of Mental Health andAddiction Services and National Institutes of Health grants MH77681 and DA00436.
Address correspondence to Marina R. Picciotto, PhD, Department of Psychiatry, YaleUniversity School of Medicine, 34 Park St., 3rd Floor Research, New Haven, CT 06508. E-mail:[email protected]
122
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

Smoking and Mood Disorders: Biological Basis 123
KEYWORDS Translational science, mouse models, human stud-ies, review, depression, major depressive disorder, knockout mice,nicotine, nicotinic acetylcholine receptors
SMOKING AND DEPRESSION
Approximately 20% to 25% of the U.S. population smokes currently, butthe incidence increases to 35% to 65% in patients with mood disorders(Diwan, Castine, Pomerleau, Meador-Woodruff, & Dalack, 1998; Glassmanet al., 1990; Kessler, 1995). Depressed smokers are also less likely to quit andare more prone to withdrawal symptoms (reviewed in Kalman, Morissette,& George, 2005). Cigarette smoke contains more than 4,000 chemicals, butnicotine is thought to be the primary addictive compound in smoked to-bacco (U.S. Department of Health and Human Services, 1988). In the centraland autonomic nervous system, nicotine binds to, activates, and can desen-sitize nicotinic acetylcholine receptors (nAChRs; Picciotto, 1998). The acti-vation of nAChRs by the endogenous neurotransmitter acetylcholine (ACh)or other compounds, such as nicotine, leads to neuronal firing. nAChRs arepentameric cation channels composed of combinations of α (2 to 9) andβ (2 to 4) subunits. Three main families can be distinguished based ontheir pharmacological and physiological profiles: α4β2-containing nAChRs(α4β2∗, where ∗ denotes other subunits) combined with α5, α6, or β3 arethe most widespread family in the central nervous system and have the high-est affinity for nicotine (Zoli, Lena, Picciotto, & Changeux, 1998). The α7∗
nAChRs have a lower affinity for nicotine but do not desensitize in the pres-ence of low levels of nicotine (Mansvelder & McGehee, 2000). The α3β4∗
nAChRs are intermediate in affinity and are the primary receptors in theautonomic ganglia (Gotti, Zoli, & Clementi, 2006).
The relationship between smoking and mood disorders remains unclear:Does smoking lead to the onset of depression? Does depression increasethe likelihood that people will smoke? Do smoking and depression sharecommon environmental/genetic factors? (See Figure 1). Twin studies haveshown that there are shared susceptibility genes for smoking and depression(Kendler et al., 1993; Mccaffery, Niaura, Swan, & Carmelli, 2003). In addition,chronic nicotine intake through smoking leads to neuroadaptations that af-fect many brain circuits, including those related to affect (Paterson & Markou,2007). Thus, it may not be surprising that acutely abstinent smokers have re-ported symptoms similar to those of depression (Glassman et al., 1990), whiledepressed patients report heightened mood after smoking a cigarette com-pared to nondepressed volunteers (Kinnunen, Doherty, Militello, & Garvey,1996). Similarly, nicotine patches can reduce symptoms of depression, evenin nonsmokers (Salin-Pascual, de la Fuente, Galicia-Polo, & Drucker-Colin,1995). Finally, studies in preclinical rodent models corroborate these clinical
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

124 Y. S. Mineur and M. R. Picciotto
observations: chronic administration of nicotine can elicit antidepressant-likeeffects in rats in various well-established paradigms (Semba, Mataki, Yamada,Nankai, & Toru, 1998; Djuric, Dunn, Overstreet, Dragomir, & Steiner, 1999;Tizabi et al., 1999). These data strongly suggest that nicotine intake canregulate mood and that some smokers may use nicotine to self-medicatedepressive mood symptoms.
Whereas chronic nicotine exposure can be antidepressant, classical an-tidepressants can affect smoking behavior as well. One of the most effectivepharmacological treatments for smoking cessation, bupropion, was originallydeveloped as an antidepressant (Fava et al., 2005). Furthermore, several clas-sical antidepressants such as selective serotonin reuptake inhibitors (SSRIs),tricyclic antidepressants, and norepinephrine reuptake inhibitors (reviewedin Hughes, Stead, & Lancaster, 2004) can help smokers to quit (Hall et al.,1998; Hayford et al., 1999; Hurt et al., 1997). Thus, nicotine can be antide-pressant, and relieving mood symptoms can help with smoking cessation.
THE CHOLINERGIC HYPOTHESIS OF DEPRESSION
The fact that nAChRs can modulate depressive symptoms suggests that acetyl-choline, the endogenous ligand for nicotinic receptors, is also critical in reg-ulating mood. In the early 1970s, a clinical study suggested that depressionmay be triggered by cholinergic hyperactivity (Janowsky, el-Yousef, Davis,& Sekerke, 1972). In that study, physostigmine (an acetylcholinesterase in-hibitor that can increase ACh levels in the brain) increased depressive symp-toms in a subset of participants (Janowsky et al., 1972). Rat studies alsosupport the hypothesis that increased cholinergic tone can lead to depres-sive symptoms. The Flinders sensitive line (FSL) and resistant line weregenetically selected based on their differential sensitivity to a cholinesteraseinhibitor. FSL rats are more sensitive to cholinesterase inhibitors and show aconstellation of depression-like phenotypes (Overstreet, 1993).
The conclusion that increased cholinergic function results in depressivesymptoms may seem paradoxical since nicotine, a cholinergic agonist, hasantidepressant properties. These observations can be reconciled when oneconsiders that nicotine and nicotinic compounds administered chronically(as in animal models or with nicotine patches in humans) can transientlyactivate but subsequently desensitize nAChRs for relatively long periods (upto several hours in some cases [Gentry & Lukas, 2002; Paradiso & Steinbach,2003]). Thus, desensitization and not activation of nAChRs may result in an-tidepressant effects. In accord with this possibility, chronic (which would bemore likely to lead to desensitization) but not subchronic nicotine treatmenthad antidepressant effects in initial studies (Semba et al., 1998). Similarly,increased nAChR stimulation as a result of cholinesterase blockade has de-pressant effects in human patients and animal models (Fava et al., 2005).
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

Smoking and Mood Disorders: Biological Basis 125
Consistent with the cholinergic hypothesis of depression, mecamy-lamine, a nonselective nAChR antagonist, can decrease symptoms of de-pression and anxiety in patients (Dursun & Kutcher, 1999; Mihailescu& Drucker-Colin; 2000, Salin-Pascual, Alcocer-Castillejos, & Alejo-Galarza,2003). Mecamylamine can also result in decreased depressive symptomswhen added to an SSRI in patients who were resistant to the SSRIalone (George, Sacco, Vessicchio, Weinberger, & Shytle, 2008). Similarly,mouse studies also show that mecamylamine has antidepressant-like prop-erties in several behavioral paradigms (Mineur, Somenzi, & Picciotto, 2007;Rabenstein, Caldarone, & Picciotto, 2006) and can also potentiate the effectsof classical antidepressants such as amitriptyline (Caldarone et al., 2004) andimipramine (Popik, Kozela, & Krawczyk, 2003; two TCAs) or citalopram (anSSRI; Popik et al., 2003). These studies suggest that decreasing nAChR ac-tivity may affect the same monoamine systems that are affected by classicalantidepressants. Consistent with this possibility, both nicotine and mecamy-lamine can increase serotonin release in the rat hippocampus (Kenny, File,& Neal, 2000).
An increasing body of evidence also shows that classical antidepres-sants, in addition to their ability to block monoamine transporters, can in-hibit nAChR function (Fryer & Lukas, 1999; Garcia-Colunga, Awad, & Miledi,1997; Lopez-Valdes & Garcia-Colunga, 2001; Schofield, Witkop, Warnick, &Albuquerque, 1981). The majority of antidepressants tested can blocknAChRs at nanomolar concentrations at clinically relevant doses reachedin depressed patients after chronic treatment (for review, see Shytle et al.,2002). Thus, while increased monoaminergic tone is clearly important forantidepressant efficacy, these data suggest that nicotinic receptor blockadeby antidepressants might also contribute.
EVIDENCE FOR SPECIFIC NICOTINIC RECEPTOR MODULATIONOF MOOD FROM GENETIC MOUSE MODELS
Studies in transgenic mouse models have demonstrated that the deletion ofβ2∗ nAChRs leads to an antidepressant-like phenotype in the forced swimand tail suspension tests (Caldarone et al., 2004). Moreover, the effect of theclassical antidepressant amitriptyline is abolished in these knockout mice(Caldarone et al., 2004), strongly suggesting that blockade of β2∗ nAChRsmay result in antidepressant-like effects and could be necessary for efficacyof classical antidepressants. Similarly, the antidepressant-like effects of thenicotinic antagonist mecamylamine are also abolished in β2 subunit knock-out mice (Rabenstein et al., 2006). It should be noted that the absenceof β2∗ nAChRs throughout development in these knockout mice may re-sult in long-term changes in other neurotransmitter systems that might be
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

126 Y. S. Mineur and M. R. Picciotto
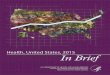
FIGURE 1 Simplified representation of the relationship among genetic factors, depressivesymptoms, and smoking behavior. Genetic factors contribute to susceptibility to smokingand depression, and twin studies show that some of these genetic factors are shared (Kendleret al., 1993; Mccaffery et al., 2003). Depression leads to an increased susceptibility to smoking.Inversely, smoking behavior improves mood and decreases depressive symptoms probablythrough nicotinic receptor desensitization. Concomitantly, nicotine withdrawal can precipitatedepression-like symptoms. Several classes of antidepressants, particularly the atypical antide-pressant bupropion, can decrease smoking and help smokers to quit in addition to their abilityto improve mood and decrease depressive symptoms.
responsible for the lack of antidepressant-like effects in these animals; how-ever, the hypothesis that high-affinity nAChRs are important for antidepres-sant response is consistent with these findings.
A number of pharmacological studies have also contributed to the hy-pothesis that nicotinic receptor blockade has antidepressant-like properties(Andreasen, Olsen, Wiborg, & Redrobe, 2008; Mineur et al., 2007; Rabensteinet al., 2006). In addition to studies of mecamylamine cited above, nicotinicpartial agonists (that can decrease endogenous acetylcholine transmission athigh-affinity nAChRs) also induce an antidepressant-like response. For ex-ample, cytisine, a plant alkaloid that is a nicotinic partial agonist used in
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

Smoking and Mood Disorders: Biological Basis 127
Eastern Europe as an aid for smoking cessation, is a low-efficacy partial ag-onist at α4β2∗ nAChRs (Papke & Heinemann, 1994). In mice, cytisine hasantidepressant-like properties in a number of behavioral paradigms includ-ing the tail suspension, forced swim, and novelty-suppressed feeding tests(Mineur et al., 2007). These studies suggest that use of the nicotinic partialagonist varenicline that is currently in use as an aid to smoking cessationmight also result in antidepressant effects in humans. Similarly, highly selec-tive partial agonists at α4β2∗ nAChRs may be useful for treating depressivesymptoms in people with mood disorders, either alone or in combinationwith more classical antidepressants such as SSRIs.
CONCLUSIONS
There is significant co-morbidity between smoking and mood disorders,suggesting that there is a common biological basis for tobacco dependenceand depression. It seems likely that the relationship between smoking anddepression is bidirectional, with nicotine and brain changes due to chronicnicotine intake leading to increases in depressed mood and depressed moodpromoting continued nicotine intake to maintain desensitization of nAChRs.These observations suggest that pharmacological treatments that modulatenicotinic receptor function could provide novel pharmacotherapeutic strate-gies for treating mood disorders. Furthermore, if smoking is used to self-medicate depression symptoms in a subset of smokers, then nicotinic an-tagonists and partial agonists could both limit depressive symptoms in thoseindividuals while decreasing nicotine craving and withdrawal.
REFERENCES
Andreasen, J. T., Olsen, G. M., Wiborg, O., & Redrobe, J. P. (2008). Antidepressant-like effects of nicotinic acetylcholine receptor antagonists, but not agonists, inthe mouse forced swim and mouse tail suspension tests. Journal of Psychophar-macology. Retrieved April 10, 2009 from PubMed; ID 18583432.
Caldarone, B. J., Harrist, A., Cleary, M. A., Beech, R. D., King, S. L., & Picciotto, M.R. (2004). High-affinity nicotinic acetylcholine receptors are required for antide-pressant effects of amitriptyline on behavior and hippocampal cell proliferation.Biological Psychiatry, 56, 657–664.
Diwan, A., Castine, M., Pomerleau, C. S., Meador-Woodruff, J. H., & Dalack,G. W. (1998). Differential prevalence of cigarette smoking in patients withschizophrenic vs mood disorders. Schizophrenia Research, 33, 113–118.
Djuric, V. J., Dunn, E., Overstreet, D. H., Dragomir, A., & Steiner, M. (1999). An-tidepressant effect of ingested nicotine in female rats of Flinders resistant andsensitive lines. Physiology & Behavior, 67, 533–537.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

128 Y. S. Mineur and M. R. Picciotto
Dursun, S. M., & Kutcher, S. (1999). Smoking, nicotine and psychiatric disorders:Evidence for therapeutic role, controversies and implications for future research.Medical Hypotheses, 52, 101–109.
Fava, M., Rush, A. J., Thase, M. E., Clayton, A., Stahl, S. M., Pradko, J. F., et al.(2005). 15 years of clinical experience with bupropion HCl: From bupropionto bupropion SR to bupropion XL. Primary Care Companion to the Journal ofClinical Psychiatry, 7, 106–113.
Fryer, J. D., & Lukas, R. J. (1999). Antidepressants noncompetitively inhibit nicotinicacetylcholine receptor function. Journal of Neurochemistry, 72, 1117–1124.
Garcia-Colunga, J., Awad, J. N., & Miledi, R. (1997). Blockage of muscle and neu-ronal nicotinic acetylcholine receptors by fluoxetine (Prozac). Proceedings ofthe National Academy of Sciences of the United States of America, 94, 2041–2044.
Gentry, C. L., & Lukas, R. J. (2002). Regulation of nicotinic acetylcholine receptornumbers and function by chronic nicotine exposure. Current Drug Targets–CNS& Neurological Disorders, 1, 359–385.
George, T. P., Sacco, K. A., Vessicchio, J. C., Weinberger, A. H., & Shytle,R. D. (2008). Nicotinic antagonist augmentation of selective serotonin reuptakeinhibitor–refractory major depressive disorder: A preliminary study. Journal ofClinical Psychopharmacology, 28, 340–344.
Glassman, A. H., Helzer, J. E., Covey, L. S., Cottler, L. B., Stetner, F., Tipp, J. E.,et al. (1990). Smoking, smoking cessation, and major depression. Journal of theAmerican Medical Association, 264, 1546–1549.
Gotti, C., Zoli, M., & Clementi, F. (2006). Brain nicotinic acetylcholine receptors:Native subtypes and their relevance. Trends in Pharmacology Science, 27,482–491.
Hall, S. M., Reus, V. I., Munoz, R. F., Sees, K. L., Humfleet, G., Hartz, D. T.,et al. (1998). Nortriptyline and cognitive-behavioral therapy in the treatmentof cigarette smoking. Archives of General Psychiatry, 55, 683–690.
Hayford, K. E., Patten, C. A., Rummans, T. A., Schroeder, D. R., Offord, K. P.,Croghan, I. T., et al. (1999). Efficacy of bupropion for smoking cessation insmokers with a former history of major depression or alcoholism. British Journalof Psychiatry, 174, 173–178.
Hughes, J., Stead, L., & Lancaster, T. (2004). Antidepressants for smoking cessation.Cochrane Database Systematic Reviews, CD000031.
Hurt, R. D., Sachs, D. P., Glover, E. D., Offord, K. P., Johnston, J. A., Dale, L. C., et al.(1997). A comparison of sustained-release bupropion and placebo for smokingcessation. New England Journal of Medicine, 337, 1195–1202.
Janowsky, D. S., el-Yousef, M. K., Davis, J. M., & Sekerke, H. J. (1972). A cholinergic-adrenergic hypothesis of mania and depression. Lancet, 2, 632–635.
Kalman, D., Morissette, S. B., & George, T. P. (2005). Co-morbidity of smoking inpatients with psychiatric and substance use disorders. The American Journal onAddictions/American Academy of Psychiatrists in Alcoholism and Addictions,14, 106–123.
Kenny, P. J., File, S. E., & Neal, M. J. (2000). Evidence for a complex influence ofnicotinic acetylcholine receptors on hippocampal serotonin release. Journal ofNeurochemistry, 75, 2409–2414.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

Smoking and Mood Disorders: Biological Basis 129
Kendler, K. S., Neale, M. C., MacLean, C. J., Heath, A. C., Eaves, L. J., & Kessler, R. C.(1993). Smoking and major depression. A causal analysis. Archives of GeneralPsychiatry, 50, 36–43.
Kessler, D. A. (1995). Nicotine addiction in young people. New England Journal ofMedicine, 333, 186–189.
Kinnunen, T., Doherty, K., Militello, F. S., & Garvey, A. J. (1996). Depression andsmoking cessation: Characteristics of depressed smokers and effects of nico-tine replacement. Journal of Consulting and Clinical Psychology, 64, 791–798.
Lopez-Valdes, H. E., & Garcia-Colunga, J. (2001). Antagonism of nicotinic acetyl-choline receptors by inhibitors of monoamine uptake. Molecular Psychiatry, 6,511–519.
Mansvelder, H. D., & McGehee, D. S. (2000). Long-term potentiation of excitatoryinputs to brain reward areas by nicotine. Neuron, 27, 349–357.
McCaffery, J. M., Niaura, R., Swan, G. E., & Carmelli, D. (2003). A study of depressivesymptoms and smoking behavior in adult male twins from the NHLBI twin study.Nicotine & Tobacco Research, 5, 77–83.
Mihailescu, S., & Drucker-Colin, R. (2000). Nicotine, brain nicotinic receptors, andneuropsychiatric disorders. Archives of Medical Research, 31, 131–144.
Mineur, Y. S., Somenzi, O., & Picciotto, M. R. (2007). Cytisine, a partial agonist ofhigh-affinity nicotinic acetylcholine receptors, has antidepressant-like propertiesin male C57BL/6J mice. Neuropharmacology, 52, 1256–1262.
Overstreet, D. H. (1993). The Flinders sensitive line rats: A genetic animal model ofdepression. Neuroscience & Biobehavioral Reviews, 17, 51–68.
Papke, R. L., & Heinemann, S. F. (1994). Partial agonist properties of cytisine onneuronal nicotinic receptors containing the beta 2 subunit. Molecular Pharma-cology, 45, 142–149.
Paradiso, K. G., & Steinbach, J. H. (2003). Nicotine is highly effective at producingdesensitization of rat alpha4beta2 neuronal nicotinic receptors. The Journal ofPhysiology, 553, 857–871.
Paterson, N. E., & Markou, A. (2007). Animal models and treatments for addictionand depression co-morbidity. Neurotoxicity Research, 11, 1–32.
Picciotto, M. R. (1998). Common aspects of the action of nicotine and other drugsof abuse. Drug and Alcohol Dependence, 51, 165–172.
Popik, P., Kozela, E., & Krawczyk, M. (2003). Nicotine and nicotinic receptor antag-onists potentiate the antidepressant-like effects of imipramine and citalopram.British Journal of Pharmacology, 139, 1196–1202.
Rabenstein, R. L., Caldarone, B. J., & Picciotto, M. R. (2006). The nicotinic antagonistmecamylamine has antidepressant-like effects in wild-type but not beta2- oralpha7-nicotinic acetylcholine receptor subunit knockout mice. Psychopharma-cology, 189, 395–401.
Salin-Pascual, R. J., Alcocer-Castillejos, N. V., & Alejo-Galarza, G. (2003). Nicotinedependence and psychiatric disorders. Revista de Investigacion Clinica, 55,677–693.
Salin-Pascual, R. J., de la Fuente, J. R., Galicia-Polo, L., & Drucker-Colin, R. (1995).Effects of transdermal nicotine on mood and sleep in nonsmoking major de-pressed patients. Psychopharmacology, 121, 476–479.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014

130 Y. S. Mineur and M. R. Picciotto
Schofield, G. G., Witkop, B., Warnick, J. E., & Albuquerque, E. X. (1981). Differentia-tion of the open and closed states of the ionic channels of nicotinic acetylcholinereceptors by tricyclic antidepressants. Proceedings of the National Academy ofSciences of the United States of America, 78, 5240–5244.
Semba, J., Mataki, C., Yamada, S., Nankai, M., & Toru, M. (1998). Antidepressantlikeeffects of chronic nicotine on learned helplessness paradigm in rats. BiologicalPsychiatry, 43, 389–391.
Shytle, R. D., Silver, A. A., Lukas, R. J., Newman, M. B., Sheehan, D. V., & Sanberg,P. R. (2002). Nicotinic acetylcholine receptors as targets for antidepressants.Molecular Psychiatry, 7, 525–535.
Tizabi, Y., Overstreet, D. H., Rezvani, A. H., Louis, V. A., Clark, E., Jr., Janowsky,D. S., et al. (1999). Antidepressant effects of nicotine in an animal model ofdepression. Psychopharmacology, 142, 193–199.
U.S. Department of Health and Human Services. (1988). The health consequencesof smoking: Nicotine addiction. In A report of the surgeon general (R. M. Davis,T. E. Novotny, & W. R. Lynn, Eds.). Washington, DC: U.S. Government PrintingOffice.
Zoli, M., Lena, C., Picciotto, M. R., & Changeux, J. P. (1998). Identification of fourclasses of brain nicotinic receptors using beta2 mutant mice. Journal of Neuro-science, 18, 4461–4472.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
09:
59 3
1 O
ctob
er 2
014