Embed Size (px)
Citation preview

Bioequivalence accomplishments, ongoing initiatives, and remaining
challenges1
M. N. MARTINEZ
US Food and Drug Administration, Center
for Veterinary Medicine, Rockville, MD,
USA
Martinez, M. N. Bioequivalence accomplishments, ongoing initiatives, and
remaining challenges. J. vet. Pharmacol. Therap. 37, 2–12.
Although bioequivalence (BE) concepts date back to the late 1960s, there has
been a steady evolution in the tools applied to the assessment of product
comparability. Despite these advancements, we continue to face a multitude
of unresolved challenges. Several of these challenges are unique to veterinary
medicine due to issues such as multiple species approvals, unique dosage
forms (e.g., intramammary infusion and medicated premixes), physiological
challenges (e.g., limitations in blood volume and stress reactions), and the
need to evaluate product equivalence for products intended to release drug
over a duration of months. Thus, while in some instances, we can adopt
advancements implemented by our human health counterparts but in other
situations, we need to pioneer our own method for resolving these challenges.
The purpose of this manuscript is to provide an update on recent advances,
achievements, and ongoing initiatives associated with the assessment of prod-
uct BE in veterinary medicine. This review reflects the highlights of a presen-
tation given at the 2012 meeting of the European Association for Veterinary
Pharmacology and Toxicology.
(Paper received 13 April 2013; accepted for publication 01 June 2013)
Marilyn N. Martinez, US Food and Drug Administration, Center for Veterinary
Medicine, HFV-100, Rockville, MD 20855, USA. E-mail: marilyn.martinez@
fda.hhs.gov1This article reflects the views of the author and should not be construed to
represent FDA’s views or policies.
INTRODUCTION
An examination of the changes in the bioequivalence (BE) par-
adigm provides a fascinating study of the evolution of a scien-
tific discipline (Martinez & Hunter, 2010). While today, most
scientists agree that (with all else equal) equivalent rate and
extent of drug exposure will result in equivalent therapeutic
outcomes, this perspective was born from extensive debate
within the scientific and medical communities. In reviewing
published manuscripts from the late 1960s, we find many
examples of expressed concern about the validity of BE con-
cepts. During these early years, fundamental problems were
the paucity of insights into factors impacting in vivo product
performance and a lack of efficient tools for evaluating drug
product comparability. However, even after significant
advances were achieved, there remained concerns and skepti-
cism. I myself recall working on the evaluation of human gen-
eric drug products shortly after the enactment of Drug Price
Competition and Patent Term Restoration Act of 1984 (Public
Law 98-417; Hatch Waxman) at which time state formularies
and critics of generic drug product interchangeability exhibited
misconceptions about the implications of the confidence inter-
val approach for assessing product comparability. Skeptics
argued that an allowance of 90% confidence bounds of �20%
for rate (as estimated by peak drug concentration, Cmax) and
extent (as estimated by the area under the concentration vs.
time profile, AUC) implied that two generic products could
actually differ by �40%. Such statements reflected a lack of
understanding of the statistical underpinnings upon which BE
assessments were based.
While those days are behind us, we still face a multitude of
issues that remain to be resolved. Within the area of animal
health, we encounter not only challenges impacting human BE
assessments but also those associated with dosage forms and
physiologies unique to veterinary species. Therefore, while it is
helpful to follow many of the solutions developed by our
human health colleagues, there needs to be a willingness to
forge unique paths that address the numerous issues encoun-
tered within animal health.
With this in mind, this manuscript provides a summary of
our accomplishments, ongoing initiatives, and remaining BE
challenges.
2 Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
J. vet. Pharmacol. Therap. 37, 2--12. doi: 10.1111/jvp.12063. REVIEW ARTICLE

BASIC CONCEPTS
The evaluation of product BE is a compilation of several scien-
tific disciplines:
• Pharmacokinetics (PK): the way that the body handles the
active pharmaceutical ingredient (API). This includes absorp-
tion, metabolism, distribution, and elimination (ADME).
○ PK can influence the extent to which formulation differ-
ences will impact the product comparability of in vivo
blood level profiles. For example, the more rapid the elim-
ination, the more sensitive will be the profiles to product
differences in absorption rates. The presence of saturable
elimination processes can lead to exaggerated interprod-
uct differences in AUC, especially in the presence of drug
accumulation. The PK of the drug will influence the
study design (e.g., the duration of the washout interval,
the magnitude of variability in PK characteristics, and
the ability to employ a crossover vs. a parallel study
design).
○ Absorption constraints:
• The internal environment to which the dosage form
will be exposed. In turn, this dictates the rate and
extent of product dissolution, partitioning into biologi-
cal fluids and drug solubilization, regardless of whether
the product is orally, parenterally, or topically adminis-
tered.
• The characteristics of the absorption site, which
includes membrane permeability, blood flow, absorptive
surface area, and active transport processes.
• The presence of presystemic drug metabolism, whether
it be in the liver or gut. This metabolism is often a
cause for interspecies differences in apparent bioavail-
ability and for large within- and between-subject fluc-
tuations in apparent oral bioavailability.
• Biopharmaceutics: the relationship between the physico-
chemical characteristics of the drug and the formulation
through which that drug is being delivered. Integrated into
biopharmaceutics principles are the concepts of quality by
design (QbD), critical quality attributes (CQAs), and quality
target product profile (QTPP; Annon1, 2009).
• Statistics: the analysis and interpretation of the PK parame-
ters based upon a set of assumptions and criteria. The statis-
tical approaches used for determining product BE also
dictates many attributes of the study design, such as subject
number and the overall dosing scheme (e.g., extended period
crossover designs) that may be appropriate addressing spe-
cific sets of concerns (e.g., reference products presenting with
highly variable blood level profiles, methods for identifying
unequal carryover of PK or PD effects from one period to the
next).
• Clinical pharmacology: the allowable difference between test
and reference means (as they pertain to the rate and extent
of drug exposure) that insures that the products will be
therapeutically indistinguishable within the target patient
population. Inherent in this approach is an assumed absence
of any patient-by-formulation interaction (Hauck & Ander-
son, 1994). When dealing with a generic drug product, leg-
ally prescribed constraints on the allowable differences are
usually imposed (e.g., confidence bounds of 0.80–1.25).
However, if a drug has a narrow therapeutic window or
when a drug sponsor has right of reference to the underly-
ing safety and effectiveness data, the allowable differences
can be modified as appropriate. This distinction between
generic and pioneer products is contained within the con-
cepts of prescribability vs. switchability (Hauck and Ander-
son, 1994).
ACCOMPLISHMENTS
International harmonization
The presence of a global marketplace necessitates international
harmonization of the study requirements for demonstrating in
vivo blood level BE. Through the efforts of the Veterinary Inter-
national Conference on Harmonization (VICH), an Expert
Working Group (EWG) was convened and a draft in vivo blood
level BE guideline was developed. The VICH is a trilateral (EU-
Japan-USA) program aimed at harmonizing technical require-
ments for veterinary product registration. The EWG is
appointed to draft recommendations by the VICH Steering
Committee. Each EWG will normally consist of six topic experts
– one representing each VICH full member. Once finalized,
VICH guidelines represent a harmonization in guidance by the
European Union, the United States, and Japan, and may find
even wider acceptance across the various other jurisdictions.
For additional information on the VICH, please refer to http://
www.vichsec.org.
The VICH BE guideline is slated to progress to Step 4 of
the eight-step VICH process in the near future (for informa-
tion on the VICH step process, please refer to http://www.
vichsec.org/en/process.htm). Despite this success, there remain
numerous challenges not addressed within this guideline.
These include:
• biowaivers;
• biosimilars;
• pharmacological or clinical endpoint studies;
• human food safety;
• in vitro dissolution studies;
• study designs for those products where blood drug concen-
trations may not be indicative of drug concentrations at the
site of action. This can include products such as topically
active formulations, intramammary products, intravenous
administration of complex drug delivery systems where the
drug is release directly at the site of action.
Identifying potential solutions to existing BE challenges
In 2009, the plan for a BE initiative was presented at the Tri-
ennial meeting of the European Association of Veterinary Phar-
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
BE accomplishments and ongoing initiatives 3

macology and Toxicology (EAVPT). This initiative, sponsored
by the American Academy of Veterinary Pharmacology and
Therapeutics (AAVPT), the European College of Veterinary
Pharmacology and Toxicology (ECVPT), and the EAVPT, pro-
vided the support necessary to accomplish the following goals:
• Publication of a stimuli article describing some of the BE
challenges encountered by veterinary medicine (Martinez &
Hunter, 2010).
• The convening of an AAVPT/EAVPT/ECVPT cosponsored
webinar to review basic BE concepts. This was accomplished
in May, 2010.
• The convening of a BE Workshop as a platform for dialog on
the challenges encountered when evaluating product BE for
veterinary pharmaceuticals. This event occurred on June,
2010 (http://aavpt.affiniscape.com/associations/12658/files/
BEWorkshopfinalagenda6-4-10.pdf.
• Publication of a workshop summary report (Martinez et al.,
2011).
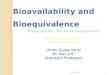
• Development of white papers by working groups represent-
ing experts from across the globe. These white papers were
published in a 2012 Supplemental Issue of the Journal of
Veterinary Pharmacology and Therapeutics (JVPT; Fig. 1).
As a result of this initiative, innovative solutions were pro-
posed and the groundwork established for identifying creative
paths forward on these complex issues.
UNRESOLVED CHALLENGES AND ONGOING
INITIATIVES
Some of the remaining unresolved challenges, many of which
were topics of manuscripts included in the JVPT 212 BE Sup-
plement, were reviewed at the 2012 EAVPT Triennial meeting.
These included the following topics are discussed below.
Biowaivers
The term biowaiver is applied to a regulatory drug approval
process where the efficacy and safety part of the dossier (appli-
cation) are approved based on evidence of equivalence other
than through in vivo equivalence testing. The issue of biowai-
vers has garnished a tremendous amount of attention within
both human and veterinary medicine. For products associated
with negligible systemic absorption, BE assessments have been
largely limited to clinical endpoint trials. However, given the
limited discriminative capability of such trials, the question is
whether or not alternative methods for assessing product com-
parability may not be more sensitive to potential differences in
in vivo product performance.
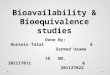
To expand upon this point, consider the hypothetical situation
described in Fig. 2 where we compare the clinical response to
two different formulations of an orally administered, locally act-
ing, antiparasitic agent. In this example, due to formulation dif-
ferences in their respective in vivo drug release characteristics
different amounts of a locally acting antiparasitic agent are deliv-
ered to the site of action by formulations A and B. In this exam-
ple, the local exposure associated with formulation A = 4 units
while that of formulation B = 8 units. If a clinical endpoint study
were conducted on animals infected with a wild-type strain of
the pathogen, then the percent therapeutic success (Y-axis)
achieved with each of two formulations could be indistinguish-
able and the two products would be declared bioequivalent.
However, if an animal were now infected with a less susceptible
pathogen strain, the clinical response to the formulations would
be markedly different. This outcome is consistent with the work
of Holford and Sheiner (1981) where they showed that when
the response is in excess of 80% its maximum, the pharmacody-
namic endpoint will be insensitive to further changes in drug
concentrations. A similar scenario may be encountered when
attempting to derive a correlation between surrogate vs. targeted
clinical responses, between two events originating through dif-
INTRODUCTION
• Introduc on to the bioequivalence theme issue: MN Mar nez & RP Hunter
DATA ANALYSIS• Assessing product bioequivalence for extended-release formula ons and drugs with long half-lives. R. Gehring & MN Mar nez•
Su onEs ma ng product bioequivalence for highly variable veterinary drugs. R Claxton, J Cook, L Endrenyi, A Lucas, MN Mar nez, & SC
• Pharmacokine cs and pharmacodynamics of stereoisomeric drugs with par cular reference to bioequivalence determina ons. P Lees,RP Hunter, PT Reeves & PL Toutain
STUDY DESIGN
• Demonstra ng bioequivalence using clinical endpoint studies. E Bermingham, JRE Del Cas llo, C Lainesse, K Pasloske, & S Radecki
• Should licking behavior be considered in the bioavailability evalua on of transdermal products? PL Toutain, S. Modric, A Bousquet-Mélou, JM Sallovitz, & C Lanusse
• Considera ons for extrapola ng in vivo bioequivalence data across species and routes. S Modric, E Bermingham, M Heit, C Lainesse &C Thompson
• Establishing bioequivalence of veterinary premixes (Type A medicated ar cles). RP Hunter, P Lees, D Concordet, & PL Toutain
• Challenges associated with the demonstra on of bioequivalence of intramammary products in ruminants. C. Lainesse, R Gehring, KPasloske, G Smith, S Soback, S Wagner, & T Whi em
BIOWAIVERS
• The scien fic basis for establishing solubility criteria for veterinary species. MN Mar nez & R Fahmy
• Drug solubility classifica on in the dog. MN Mar nez & MG Papich
• Drug solubility classifica on in the bovine. MN Mar nez & MD Apley
• How do you define equivalence of the API of biomass products? RP Hunter, E. Deridder, A. Lucas,KO Smedley & DW Yordy
• Challenges obtaining a biowaiver for topical veterinary dosage forms. R Baynes, J Riviere,T Franz, N Monteiro-Rivere, P Lehman, M Peyrou, & PL Toutain Special Issue:
Bioequivalence, April, 2012, Volume 35, Supplement S1
Fig. 1. Contents of the JVPT supplemental
issue on product BE. BE, bioequivalence.
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
4 M. N. Martinez

fering mechanisms of action, or when assessing the relationship
between drug exposure and a toxic effect.
Thus, the question is whether or not a paradigm can be estab-
lished to provide greater scientific rigor to our BE assessments in
those situations when blood level BE studies are not feasible.
One possible solution could include a ‘totality-of-the-evidence’
approach, such that described by Yu (2008) and by the 2009
ICH Q8R2 document (Annon1, 2009). This approach incorpo-
rates the concept of quality by design (QbD), which has been
defined as ‘a systematic approach to development that begins
with predefined objectives and emphasizes product and process
understanding and process control, based on sound science and
quality risk management’ (ICH Q8). The foundation of the QbD
approach is a scientific understanding that supports the estab-
lishment of a design space, product specifications, and manufac-
turing controls. To accomplish this goal, the relationships
between formulation and manufacturing process variables
(including drug substance, excipient attributes, and process
parameters) need to be understood and the sources of variability
identified. It is through this understanding that the product
design space is determined. The design space is the multidimen-
sional combination of factors that have been demonstrated to
provide the desirable product quality. It represents an optimized
set of conditions whereby the formulation and process variables
give rise to a product that will have the desired in vivo perfor-
mance in the targeted patient population.
Accordingly, the QbD approach also necessitates a character-
ization of the physicochemical properties of the API. Physical
properties of the API include (Yu, 2008):
• Physical description
○ particle size, shape, and distribution;
○ polymorphism;
○ aqueous solubility as function of pH;
○ hygroscopicity;
○ melting points.
• Chemical properties include
○ pKa;
○ chemical stability in solid state and in solution;
○ photolytic and oxidative stability.
• Biological properties
○ partition coefficient;
○ membrane permeability and/or oral bioavailability.
Once the API has been characterized and the in vivo and in
vitro product performance characteristics have been identified,
a design space can be described in terms of ranges of material
attributes and process parameters within which product qual-
ity and performance attributes can be assured. Operation
within the design space will result in a product meeting the
defined quality and performance (Annon1, 2009).
The QbD paradigm provides a springboard for the develop-
ment of an approach to support the in vitro assessment of drug
products that are not systemically absorbed. This approach
involves a characterization of similarity based upon (Yu et al.,
2003):
Q1: Qualitative similarity – that is, the same components.
Q2: Quantitative similarity – that is, the same amounts of
the same components.
Q3: Structural similarity – that is, the same amounts of the
same components arranged in the same way.
While the assessment of Q1 and Q2 may appear to be rela-
tively straightforward, the characterization of Q3 is more com-
plicated. For example, Q3 includes arrangement of matter and
the state of aggregation. Q3 considerations may include parti-
cle size distribution of a suspension, API polymorphic form and
crystalline habit. Although Q2 implies Q3 for a solution, for
suspensions, creams, ointments, and gels, the physical state
can be impacted by a variety of factors, including the physical
state of the starting materials. In this regard, Noonan (2009)
discussed vancomycin capsules, which act locally in the gut to
treat Clostridium difficile infection and Staphylococcus aureus
enterocolitis in people. He showed an example of how products
meeting the criteria for Q1 and Q2 may not meet the criteria
for Q3, citing differences in molecular weights distribution
across several batches of polyethyleneglycol (PEG) 600. Such
differences could lead to inequivalent product performance,
underscoring the importance of Q3 sameness when evaluating
product performance.
The combination of Q1, Q2, Q3, when evaluated in conjunc-
tion with a battery of in vitro release tests, will likely provide a
more sensitive metric to small changes in product performance
than might otherwise be possible in a typical clinical endpoint
BE trial. Thus, this is a paradigm worthy of further consider-
ation within the scientific community.
Highly soluble drugs
A description of drug solubility is an important starting point
for identifying the variables that can influence in vivo product
performance. Within the human drug arena, the Biopharma-
ceutics Classification System (BCS) has gained tremendous sup-
port as a prognostic tool for identifying the relationship
between product formulation and in vivo product performance
Effect of change in pathogen susceptibility on clinical endpoint decision
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14Exposure
Res
pons
e (p
erce
nt s
ucce
ss)
Less susceptiblewild-type responders
FORM A
FORM B
Fig. 2. Changes in response outcome, and therefore conclusions of clin-
ical BE, if there is a shift in the targeted drug exposure (e.g., pathogen
susceptibility) shifts. BE, bioequivalence.
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
BE accomplishments and ongoing initiatives 5

(Amidon et al., 1995). The BCS classifies compounds on the
basis of their solubility and permeability. Given the availability
of high throughput tools for defining human drug solubility
and intestinal permeability, classification can be readily accom-
plished. This in turn has opened the opportunity in human
drugs for the US FDA Center for Drug Evaluation and Research
(CDER), the European Medicines Agency (EMA), and Health
Canada (HC) to employ the BCS as an instrument for identify-
ing compounds eligible for biowaivers (Annon2, 2000; An-
non3, 2008; Annon4, 2012).
Complications emerge when trying to define drug solubility
and permeability in animals. In this regard, a frequently asked
question is: If solubility is an inherent physicochemical prop-
erty of a molecule, why should there be differences in drug sol-
ubility in humans vs. veterinary species? The answer to this
question involves several factors:
• Dose:
○ As veterinary drugs are usually administered on a milli-
gram per kilogram basis, the dose needs to be evaluated
from the perspective of the size of the animal. However,
it is not known if gastrointestinal (GI) fluid volumes scale
in proportion to body weight. This complicates efforts to
establish a relationship between maximum dose and drug
solubility.
○ For some veterinary drugs, the product is administered ad
libitum in feed. Therefore, solubility criteria need to be
evaluated from the perspective of the grazing behavior of
the animal species.
• Volume: pronounced interspecies diversity exists in the phys-
iology of the GI tract. This complicates the paradigm of
assessing solubility at a well-defined dose and some pre-
scribed fluid volume.
• The pH and composition of the GI fluids is highly species-
specific (Martinez et al., 2002) and the range of pH values to
be considered should be tailored accordingly. Additionally,
for certain species (e.g., ruminants), the gastric fluids con-
tain natural surfactants and there is no normal physiological
state comparable to that of a fasted human (Martinez &
Apley, 2012). Furthermore, it may be of value to consider
the potential influence of GI ionic composition when consid-
ering the possibility of ‘common ion effect’ on the solubility
of certain salts (Martinez & Fahmy, 2012). Based upon a
review written by Dressman et al., 1998, the factors that
need to be considered when defining interspecies differences
in drug solubility include:
○ surfactants in gastric juice;
○ viscosity of the luminal fluids;
○ flow rate and fluid turnover rate;
○ GI pH and buffering capability;
○ bile acid composition.
• From a solubility perspective, body temperature itself can dif-
fer across animal species. Whether or not these slight differ-
ences in normal healthy body temperature will influence
drug solubility is a point to consider.
The US Pharmacoepia (USP) has assumed an active role in
assisting the veterinary community in its efforts to address this
challenging issue. This early effort culminated in the publica-
tion of the 2004 Stimuli article (Martinez et al., 2004), which
focused on the application of human BCS principles to the dog.
Within that stimuli article, it was noted that although it might
be feasible to estimate a maximum soluble dose (if the relation-
ship between body size and gastric fluid volume could be deter-
mined), an assessment of drug permeability would be very
difficult to obtain due to the absence of a validated canine
in vitro system. Thus, with respect to permeability, diverse GI
physiologies render it difficult to establish a single, species-inde-
pendent prediction of how a dissolved drug will penetrate the
GI mucosal membranes.
Upon eliminating the permeability parameter from our delib-
erations, this initiative was transformed into one whose goal
was to define ‘fully soluble’ based upon existing human drug
criteria for ‘highly soluble’: that is, the ability to dissolve the
highest dose strength within a set volume of fluid and across a
pH range of 1–7.5 [US FDA (Annon2, 2000)] or 1–6.8 [EMA
(Annon3, 2008) and HC (Annon4, 2012)]. Accordingly, the
2012 USP Stimuli article (Apley et al., 2012) focused on defin-
ing ‘fully soluble’ in a ruminant (cattle) and in a monogastric
species (dog). However, as veterinary drugs are generally
administered on a milligram per kilogram basis, there needed to
be a well-defined fluid volume criterion based upon the
relationship between body size and GI fluid volume. To date,
particularly in the case of dogs whose body weights can range
from 2 kg to over 70 kg, there are no published data that corre-
late GI fluid volume to body weight across the various canine
breeds. Some discrepancies also exist on the fluid volume of the
bovine rumen. The stimuli article not only was an effort to
define the appropriate media composition but also fluid volumes
appropriate for rendering an estimate of drug solubility.
This Stimuli article provided the background for discussions
at the 2012 USP Veterinary Workshop (Annon5, 2012). At
that workshop, the decision was to further limit the focus of
the initiative to species-specific test conditions for estimating
the maximum drug solubility (expressed in mg/mL). In other
words, the issues of dose and GI fluid volumes were now
outside the scope of this USP initiative. In so doing, the focus
evolved into one that is limited to a description of species-spe-
cific biorelevant conditions for estimating the solubility of an
API. Currently, a manuscript summarizing the workshop
outcomes and a corresponding third stimuli article methods on
testing drug solubility in veterinary species are in preparation.
The ultimate goal of this initiative is to develop a USP Gen-
eral Chapter on solubility assessments in veterinary species.
While the first publication will focus on drugs intended for use
in dogs or bovine, subsequently expansion of this chapter is
anticipated to include additional animal species.
Multiple species approvals
Approval of a generic formulation is contingent on the submis-
sion of data necessary to support the acquisition of all indica-
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
6 M. N. Martinez

tions included in the innovator’s product label. This translates
to the need for the generic drug sponsor to confirm product BE
in every major target animal species included on the approved
(pioneer) product label (Lainesse, 2012). Because of the burden
imposed by such requirements, questions have been raised as
to whether or not a finding of in vivo BE in one target animal
species can be extrapolated to other target animal species.
Unfortunately, within our current toolset, such extrapolations
are not feasible or appropriate for reasons described below.
Orally administered medications. As described in the discussion
on drug solubility, interspecies differences in GI physiology can
impact in vivo product performance. In addition to those
conditions that will influence drug solubility, other species-
specific physiological characteristics that can influence product
relative bioavailability include:
• GI transit time;
• absorptive surface area;
• diet and food effects;
• gastric crushing force;
• potential differences in site of drug absorption.
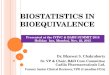
An example of how these differences can influence in vivo
product performance is exemplified by a comparison of the per-
cent ciprofloxacin absorbed following administration of an
identical formulation of a solid oral dosage form in dogs vs.
human (modeling generated with GastroPlus version 8, soft-
ware Simulations Plus, Inc., Lancaster, CA, USA). The data
used in these modeling examples were collected from an ongo-
ing collaborative study between the University of Maryland
School of Pharmacy and the US FDA Center for Veterinary
Medicine. Figure 3a,b reflect the location of ciprofloxacin
absorption across the human (a) and canine (b) GI tracts.
Upon comparing these two figures, we see several important
interspecies differences in drug absorption kinetics. Firstly, the
majority of the absorption occurred in the duodenum of
the dog as compared to the jejunum and ileum of the human.
The absorption phase was effectively completed as the drug
passed through the jejunum of the dog but continued through
the ascending colon of the human. The drug was nearly 100%
bioavailable in the dog while only 77.3% the administered dose
was absorbed in the human.
When considering these observed differences, one can predict
that a formulation that retards ciprofloxacin release will have
a greater impact on canine systemic exposure as compared to
that likely to occur in humans. In this regard, studies compar-
ing human and canine ciprofloxacin drug absorption for an
oral solution and two formulations (fast and slow release) are
near completion and will be submitted for publication. From a
regulatory perspective, species-by-formulation interactions for
oral dosage forms (i.e., species differences in the expression of
formulation effects) have been observed (M.N. Martinez,
personal unpublished observation), thus supporting the posi-
tion that it will be difficult to scientifically justify the use of
interspecies extrapolations to support decisions of product BE.
Parenteral administered medications. Interspecies differences in
the relative bioavailability of parenterally administered
products have been shown to occur (Lifschitz et al., 1999;
Martinez et al., 2001). Potential reasons for such differences
include (Martinez, 2011):
• Hot melt viscosity
○ differences in injection site physiology;
○ fluid composition;
○ fluid volumes;
○ lymphatic and vascular composition of the injection site;
○ muscle movements;
○ inflammatory responses;
○ differences in injected volumes.
(a)
(b)
Compartmental Absorption
Compartmental Absorption
85
80
75
70
65
60
55
50
45
Am
ount
(mg)
Am
ount
(mg)
40
35
30
25
20
15
10
05
00
000010020030040050060070080090100110120130140150160170180190200210220230240
0.0%S
tomach
Duodenum
Jejunum 1
Jejunum 2
lleum 1
lleum 2
lleum 3
Caecum
Asc C
olon
Total
Stom
ach
Duodenum
Jejunum 1
Jejunum 2
lleum 1
lleum 2
lleum 3
Caecum
Asc C
olon
Total
8.6%
0.0%
37.4%
4.2%0.1% 0.1% 0.1% 0.1%
99.9%
0.2%
57.8%
23.8%
16.2%
11.4%7.7%
5.3%
1.1%3.2%
77.3%
Fig. 3. Modeled location of ciprofloxacin absorption in a normal (a)
human and (b) canine subject.
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
BE accomplishments and ongoing initiatives 7

Moreover, differences in drug elimination rate can influence
the degree to which inequivalence in drug absoption rate will
impact peak drug concentrations (Cmax). This point is illus-
trated in the simulated example provided in Fig. 4 where the
interproduct ratios of Cmax values are shown to depend upon
the prevailing elimination rate constant (Ke). In brief, when
the absorption rate constant (Ka) approaches (or is less than)
Ke, differences in drug absorption will have a far greater effect
on comparative Cmax values as compared to situations when
the Ke is much smaller than Ka (that is, the drug products are
very rapidly absorbed relative to the drug elimination rate
constant).
In Fig. 4a, when Ke (the elimination rate constant) equaled
0.1/h, a Cmax ratio of 1.22 was determined when comparing
profiles generated with a Ka value of 0.15/h vs. Ka = 0.25/h.
Conversely, Fig. 4b shows that with a reduction in the Ke
(i.e., a slower elimination rate constant), the same difference
in Ka values (as was used in generating Fig. 4a) now resulted
in only a 6% difference in Cmax (Cmax ratio = 1.06). If we
translate outcome to what might occur if this were linked
with an assessment of in vivo BE across two target animal
species with differing rates of drug elimination, the products
could fail to meet the criteria for one animal species but not
for the other.
Biosimilars
A biosimilar is a biological product that is highly similar to an
already approved biological product, notwithstanding minor
differences in clinically inactive components, and for which
there are no clinically meaningful differences between the bio-
similar and the approved biological product in terms of the
safety, purity, and potency. Biological products are therapies
used to treat diseases and health conditions. Unlike most pre-
scription drugs prepared through chemical processes, biological
products generally are prepared from human and/or animal
materials (Annon6, 2012).
In February, 2012, the FDA, the Center for (human) Drug
Evaluation and Research (CDER) and the Center for (human)
Biologics Evaluation and Research (CBER), issued three draft
guidances on the assessment of ‘biosimilar’ products (Annon7,
2012; Annon8, 2012; Annon9, 2012):
• Quality Considerations in Demonstrating Biosimilarity to a
Reference Protein Product.
• Scientific Considerations in Demonstrating Biosimilarity to a
Reference Product.
• Biosimilars: Questions and Answers Regarding Implementa-
tion of the Biologics Price Competition and Innovation Act
of 2009.
These draft guidances describe a risk-based ‘totality-of-the-
evidence’ approach for evaluating the data and information
submitted in support of a determination of biosimilarity
between proposed vs. marketed reference product.
Within the framework of human medicine, biosimilar prod-
ucts intended for marketing within the U.S. are the subject of a
new drug application (NDA) submitted under section 505(b)(2)
of the U.S. Food, Drug, and Cosmetic Act (the FD&C Act).
Under Section 505(b)(2), comparability of the biosimilar prod-
uct to the listed reference product can include a comparison to
structure, function, animal toxicity, human PK, and pharma-
codynamics (PD), clinical immunogenicity, as well as original
clinical safety and effectiveness data. Thus, the legal framework
of Section 505(b)(2) allows for the submission of an NDA that
contains full reports of investigations of safety and effective-
ness, as needed, but also contains components of the applica-
tion where at least some of the information required for
approval comes from studies not conducted by or for the appli-
cant and for which the applicant has not determined a right of
reference (i.e., a ‘generic-like’ application).
Within the U.S. regulatory control over human drug, regula-
tions are provided under both the Federal Food Drug and Cos-
metic Act (FD&C) and the Public Health Service Act (PHSA). To
be considered a ‘biosimilar’ drug under section 351(k) of the US
PHSA, the application must contain, among other things, infor-
mation demonstrating that ‘the biological product is biosimilar
to a reference product’ based upon data derived from:
• analytical studies that demonstrate that the biological prod-
uct is highly similar to the reference product notwithstand-
ing minor differences in clinically inactive components;
0
10
20
30
40
50
60
Con
cent
ratio
n
Ke = 0.1 Cmax .25/.15 = 1.22
ka = 0.25
ka = 0.2
ka = 0.15
0102030405060708090
100
0 10 20 30 40 50 60
Con
cent
ratio
n
Time
0 10 20 30 40 50 60Time
Ke = 0.01 Cmax .25/.15 = 1.06
ka = 0.25
ka = 0.2
ka = 0.15
(a)
(b)
Fig. 4. Influence of changing the absorption rate constant, Ka from
0.15/h to 0.25/h when the Ke (elimination rate constant) is (a) 0.1/h
and (b) 0.01/h. In both sets of simulations, dose and percent of dose
absorbed did not vary and a one compartment open body model was
employed to generate the simulated profiles.
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
8 M. N. Martinez

• animal studies (including the assessment of toxicity); and
• a clinical study or studies (including the assessment of
immunogenicity, and PK or PD) that are sufficient to dem-
onstrate safety, purity, and potency in one or more appropri-
ate conditions of use for which the reference product is
licensed and intended to be used and for which licensure is
sought.
The Agency has the discretion to determine that an element
described above is unnecessary. Any aspect of the proposed
product that differ from the listed drug must be supported by
adequate data and information to show that the differences do
not affect the safety and effectiveness of the proposed product.
Of potential interest are some additional thoughts and concerns
regarding biosimilar products from a European perspective that
were recently published Declerck and Simoens (2012).
While the legal tools needed to support the U.S. regulatory
approval of human biosimilar products are contained within
the FD&C Act, no comparable regulations are available for vet-
erinary drug products. Accordingly, absent from within the
regulatory framework of U.S. FDA is the legal pathway for
approving biosimilar veterinary formulations.
Evaluating product BE for highly variable drugs
Efforts to identify statistical methods to evaluate the in vivo BE
of highly variable drugs have continued for more than two
decades (Shah et al., 1996). In general, a drug is considered to
be highly variable when the within-subject percent coefficient
of variation (%CV) is >30 (McGilveray et al., 1990; Blume
et al., 1995; Shah et al., 1996; Haidar et al., 2008). To date,
with the exception of its mention in the draft VICH Blood Level
BE Guideline, there are no stated policies regarding the adop-
tion of scaled statistical approach procedures for use in veteri-
nary medicine.
In an effort to address this gap, Claxton et al. (2012) devel-
oped a white paper addressing the potential application of a
scaled BE approach for use in veterinary species. It was noted
that the current algorithm used in human medicine necessi-
tates the use of an extended crossover study design (i.e., three
or four periods). Such designs can only be conducted in adult
animals whose blood volume and behavior will allow for the
capture of multiple samples without inducing undue stress or
compromising animal health.
Unfortunately, there are many situations encountered in vet-
erinary medicine where the use of an extended crossover
design is not feasible. Furthermore, there are many formula-
tions that are intended to release drug over a very long dura-
tion of time, thereby necessitating the use of a parallel (rather
than crossover) study design. Because between-subject varia-
tion is typically larger than within-subject variability, observ-
ing a %CV ≥30 for AUC or Cmax will not be an unusual event
when using a parallel study design. Therefore, the number of
animals needed to achieve the necessary power to demonstrate
product BE can be prohibitive.
As I have observed (personal observation), the current algo-
rithm for a scaled BE approach (which is based upon within-
subject variance estimates) cannot be readily translated to the
scaling of BE studies that employ a parallel design. This impor-
tant void in our BE tool chest needs to be resolved and clearly,
it will be up to the animal health community to address this
statistical challenge.
Evaluating product BE for long half-life (T½) drugs and/or dosageforms
As the objective of product BE studies is to compare the effects
of formulation on the rate and extent of drug absorption, it is
important to distinguish between rapidly absorbed compounds
that remain in the body for prolonged periods due to their
inherent PK characteristics vs. those compounds where the
extended duration of exposure is a function of product formula-
tion. Potential study design considerations associated with
these two distinctly different situations were considered by
Gehring and Martinez (2012).
For slowly depleting drugs in immediate release formula-
tions, there is a duration of sampling time that will maximize
the precision of the bioavailability comparison. In this regard,
the longer the sampling period in the postabsorptive phase, the
greater the likely variation in AUC values will be. This is due
both to the noise associated with quantification of low drug
concentrations and to the inherent variability of the elimina-
tion phase. For that reason, extending the duration of mea-
surement beyond 3–5 multiples of the T½ may increase the
risk of study failure, particularly when we consider that the
study usually employs a parallel study design.
In contrast, when the long duration of exposure is attribut-
able to formulation effects, sampling should continue for as
long as possible to characterize the formulation effects on prod-
uct performance. Unlike the previous example, in this situa-
tion, the terminal phase is dictated by the rate of drug
absorption, which is the precise formulation property being
investigated. Importantly, in contrast to BE studies on immedi-
ate release products where traditional AUC and Cmax metrics
are appropriate, this may not be the situation for some modi-
fied release formulations. Depending upon the intended charac-
teristics of the product release, it may be preferable to consider
the use of partial AUCs as an estimate of the rate of absorp-
tion.
Partial AUCs may be appropriate in situations when:
• The time to peak concentrations is critical to product perfor-
mance.
• There are multiple maxima.
• The duration of exposure (particularly as it pertains to some
targeted drug concentration) may be an important consider-
ation from a therapeutic perspective.
As a case in point, Endrenyi and Tothfalusi (2010) examined
blood concentration-time profile of the reference modified release
formulation of methylphenidate vs. a marketed generic product
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
BE accomplishments and ongoing initiatives 9

for which there were several accounts of therapeutic failure in
children. That generic formulation was determined to be bio-
equivalent to the reference product based upon an assessment of
AUC and Cmax values. However, upon examination of the profile
shapes, Endrenyi and Tothfalusi observed that the test formula-
tion exhibited a delay in its release. Therefore, even though its
peak and total exposure were equivalent to the reference prod-
uct, the initial portion of the concentration-time profile differed,
and it was that early portion of the profile that was critical for
insuring comparability in terms of the onset of effect. This profile
difference would have been captured if partial AUCs rather than
Cmax were used in the BE evaluation.
While considering the scientific validity for considering the
use of partial AUCs in a BE assessment, we need to also consider
the challenge of determining the appropriate method for curve
segmentation. For example, it may be important to consider the
portion of the curve that is most closely aligned to some clinical
outcome, such as onset of effect or duration of action. However,
the precise timepoints included in the partial areas can substan-
tially alter the resulting test/reference ratios. Even more compli-
cated are those products that exhibit multiple maxima, where
justification for curve segmentation becomes even more arbi-
trary. Furthermore, due to the risk of inflating the Type I error
(failure to identify products as bioequivalent when they in fact
are equivalent), the number of parameters included in the BE
assessment need to be very carefully considered.
Food-by-formulation interactions
The impact of food on drug bioavailability is directly correlated
with the drug’s dose-to-solubility ratio. For low solubility com-
pounds, food intake will enhance its ability to dissolve in the GI
fluids, thereby increasing its oral absorption (Singh, 2005). In
the case of some lipophilic bases (such as propranolol), food
intake can further enhance oral drug bioavailability by reducing
its presystemic metabolic clearance if that compound exhibits
saturable first-pass drug loss (Melander & McLean, 1983). How-
ever, when dealing with the question of product BE, it is impor-
tant to distinguish between food-by-drug interactions (not
formulation-specific) vs. food-by-formulation interactions. From
a BE perspective, our concern is whether or not two products
demonstrated to be bioequivalent in one prandial state continue
to be BE in under the opposite prandial condition.
Examples of food-by-formulation interactions are provided
below:
• Particle size: Changing the particle size of cilostazol, a low
solubility compound was shown to have a marked impact
on oral bioavailability in healthy dogs, with the smaller
particles having substantially higher oral bioavailability as
compared to that of the larger particles (Jinno et al., 2006).
The particle sizes tested included submicron (wet-milled
median particle size = 0.26 lm), jet-milled (2.4 lm), and
hammer-milled (median particle size = 13 lm). When
evaluating the impact of food on the bioavailability of each
formulation, it was observed that while food increased the
oral bioavailability of the larger particles sizes associated
with the jet-milled and hammer-milled products, food
actually resulted in the opposite effect for wet-milled parti-
cles, leading to a slight decrease in oral bioavailability
(Table 1).
• Tablet formulation and strength: In this study, the reference
formulation of the drug nelfinavir (250 mg) was adminis-
tered as four tablets while the test formulation (625 mg)
was administered as two tablets (Kaeser et al., 2005). The
tablets were administered in four-period crossover involving
to 52 healthy male subjects under fed or fasted conditions.
The results of this study showed that food had a markedly
different impact on the oral absorption of the test and refer-
ence formulations (Table 2).
Another question frequently asked is why, in some situations,
food may have a negative effect on oral bioavailability. The
answer reflects the interaction between the physicochemical
properties of the drug molecule, its PK properties, the animal
species being considered, and the site of absorption. Negative
food effects may occur under the following conditions:
Table 1. Evaluating the impact of prandial state on the oral bioavail-
ability of three cilostazol formulations. Numbers provided are the fed/
fasted ratios when the oral bioavailability each of the three particle
sizes were examined in dogs (from Jinno et al., 2006)
Jet-milled Hammer-milled Wet-milled
AUC 3.7 � 0.7 1.8 � 0.6 0.76 � 0.04
Cmax 2.9 � 0.5 2.0 � 0.3 0.91 � 0.13
Table 2. Relative bioavailability of two nelfinavir formulations under fed or fasted conditions. The bottom portion of this table provides the test/ref-
erence ratios for AUC and Cmax when compared under fed vs. under fasted conditions (from Kaeser et al., 2005)
Ref fasted Ref fed Ref fasted/Fed Test fasted Test fed Test fasted/Fed
AUC0–inf (h�ng/mL) 5589 33 390 0.17 4077 31 580 0.13
Cmax (ng/mL) 812 3954 0.21 786 3999 0.20
Test/Ref fasted Test/Ref fed
AUC0–inf 0.73 0.95
Cmax 0.97 1.01
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
10 M. N. Martinez

• Food will reduce drug absorption of a soluble drug if that
compound is absorbed primarily in the upper small intestine.
This may be due to:
○ Increased volume in GI tract decreases concentration of
drug exposed to absorptive membrane.
○ Increased viscosity decreases interaction of drug and
absorptive membrane. In this regard, Radwan et al.
(2012) determined that a negative food effect is largely
attributed to increased GI fluid viscosity, leading to a
decrease of the API diffusion (D) and a decreased move-
ment of dissolved drug through the aqueous layer (possi-
bly increasing the thickness of the diffusion boundary
layer, d).○ A bile salt-induced decrease i Changing the particle size n
intermicellar ‘free’ drug fraction in the upper intestine
which, in turn, can result in a decrease in drug absorption.
• Food can decrease oral bioavailability due to its effects on
drug degradation, chelation, or first-pass drug loss.
CONCLUDING THOUGHTS
There are a multitude of differences between human and veter-
inary medicine that can influence the application of BE princi-
ples. Unique factors such as methods of drug delivery, multiple
species approvals, prandial state issues, animal physiological
characteristics, husbandry practices, dosages (mg/kg vs. mg
per person or per animal), and study design constraints all ren-
der it necessary for the veterinary community to be willing to
champion its own unique paths for addressing our scientific
challenges. The issues are highly complex, necessitating that
the animal health community secure the involvement highly
trained scientists across a variety of disciplines. This means
that we need to attract young talent who are interested in
exploring these veterinary issues. Given the greater job market
and financial incentives associated with human health, this is
not a simple task.
It also means that we need to establish productive collabora-
tions with our human health counterparts. The technological
advances are tremendous, and we need to insure that we make
full use of the available in silico and in vitro tools to address
our complex issues. The two communities can both learn from
each other, as we each explore the multifactorial set of vari-
ables influencing in vivo product performance. This understand-
ing will facilitate our ability to extrapolate across animal
species and for the human community, to both make better
use of animal models during formulation development and to
identify some of the potential complications that may occur as
a result of human pathologies.
Ultimately, the complexity of issues will only increase with
time as we move forward with the novel drugs and delivery
platforms necessary to address an evolving therapeutic land-
scape. Hopefully, we will succeed in our ability to address some
of the more basic questions raised in this manuscript so that
we can be prepared to meet the challenges of the future.
REFERENCES
Amidon, G.L., Lennern€as, H., Shah, V.P. & Crison, J.R. (1995) A theo-
retical basis for a biopharmaceutic drug classification: the correlation
of in vitro drug product dissolution and in vivo bioavailability. Phar-
maceutical Research, 12, 413–420.Annon1 (2009) ICH harmonised tripartite guideline pharmaceutical
development Q8(R2). Available from: http://www.ich.org/fileadmin/
Public_Web_Site/ICH_Products/Guidelines/Quality/Q8_R1/Step4/
Q8_R2_Guideline.pdf (accessed 23 March 2013).
Annon2 (2000) US FDA, Center for Drug Evaluation and Research.
Waiver of in vivo bioavailability and bioequivalence studies for imme-
diate-release solid oral dosage forms based on a biopharmaceutics
classification system. Available from: http://www.fda.gov/downloads/
Drugs/GuidanceComplianceRegulatoryInformation/Guidances/
UCM070246.pdf (accessed 23 March 2013).
Annon3 (2008) European medicines agency guideline on the investiga-
tion of bioequivalence. Available from: http://www.emea.europa.eu/
docs/en_GB/document_library/Scientific_guideline/2009/09/
WC500003011.pdf (accessed 23 March 2013).
Annon4 (2012) Health Canada draft guidance document: biopharma-
ceutics classification based biowaiver. Available from: http://www.
hc-sc.gc.ca/dhp-mps/alt_formats/pdf/consultation/drug-medic/
bcs_draft_guide_ebauche_ld_scb-eng.pdf (accessed 23 March 2013).
Annon5 (2012) Introduction to a general chapter for veterinary prod-
ucts posted for comment, workshop scheduled. Available from:
http://www.usp.org/usp-nf/notices/introduction-general-chapter-vet-
erinary-products-posted-comment-workshop-scheduled (accessed 23
March 2013).
Annon6 (2012) FDA news release: FDA issues draft guidance on bio-
similar product development. Available from: http://www.fda.gov/
NewsEvents/Newsroom/PressAnnouncements/ucm291232.htm
(accessed 23 March 2013).
Annon7 (2012) U.S. FDA center for drug evaluation and research and
center for biologics evaluation and research, guidance for industry:
quality considerations in demonstrating biosimilarity to a reference
protein product: draft guidance. Available from: http://www.fda.gov/
downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guid-
ances/UCM291134.pdf (accessed 23 March 2013).
Annon8 (2012) U.S. FDA center for drug evaluation and research and
center for biologics evaluation and research, guidance for industry:
scientific considerations in demonstrating biosimilarity to a reference
product: draft guidance. Available from: http://www.fda.gov/down-
loads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/
UCM291128.pdf (accessed 23 March 2013).
Annon9 (2012) U.S. FDA center for drug evaluation and research and
center for biologics evaluation and research, guidance for industry:
biosimilars: questions and answers regarding implementation of the
biologics price competition and innovation act of 2009. Draft Guid-
ance. Available from: http://www.fda.gov/downloads/Drugs/Guid-
anceComplianceRegulatoryInformation/Guidances/UCM273001.pdf
(accessed 23 March 2013).
Apley, M., Crist, B., Gonzalez, M.A., Hunter, R.P., Martinez, M.N., Mo-
dric, S., Papich, M.G., Parr, A.R., Riviere, J.E. & Marques, M.R.C.
(2012) Stimuli to the revision process. Available from: http://www.
usp.org/sites/default/files/usp_pdf/EN/USPNF/s200600.pdf (accessed
23 March 2013).
Blume, H.H., McGilveray, I.J. & Midha, K.K. (1995) Bio-international 94,
conference on bioavailability, bioequivalence and pharmacokinetic
studies. European Journal of Pharmaceutical Sciences, 3, 113–124.Claxton, R., Cook, J., Endrenyi, L., Lucas, A., Martinez, M.N. & Sutton,
S.C. (2012) Estimating product bioequivalence for highly variable
veterinary drugs. Journal of Veterinary Pharmacology and Therapeutics,
35 (Suppl. 1), 11–16.
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
BE accomplishments and ongoing initiatives 11

Declerck, P.J. & Simoens, S. (2012) A European perspective on the
market accessibility of biosimilars. Biosimilars, 2, 33–40.Dressman, J.B., Amidon, G.L., Reppas, C. & Shah, V.P. (1998) Dissolu-
tion testing as a prognostic tool for oral drug absorption: immediate
release dosage forms. Pharmaceutical Research, 15, 11–22.
Endrenyi, L. & Tothfalusi, L. (2010) Do regulatory bioequivalence
requirements adequately reflect the therapeutic equivalence of modi-
fied-release drug products? Journal of Pharmacy & Pharmaceutical Sci-
ences, 13, 107–113.
Gehring, R. & Martinez, M. (2012) Assessing product bioequivalence for
extended-release formulations and drugs with long half-lives. Journal
of Veterinary Pharmacology and Therapeutics, 35 (Suppl. 1), 3–9.Haidar, S.H., Davit, B., Chen, M.L., Conner, D., Lee, L., Li, Q.H., Lion-
berger, R., Makhlouf, F., Patel, D., Schuirmann, D.J. & Yu, L.X.
(2008) Bioequivalence approaches for highly variable drugs and
drug products. Pharmaceutical Research, 25, 237–241.Hauck, W.W. & Anderson, S. (1994) Measuring switchability and pre-
scribability: when is average bioequivalence sufficient? Journal of
Pharmacokinetics and Biopharmaceutics, 22, 551–564.
Holford, N.H. & Sheiner, L.B. (1981) Understanding the dose–effectrelationship: clinical application of pharmacokinetic-pharmacody-
namic models. Clinical Pharmacokinetics, 6, 429–453.Jinno, J., Kamada, N., Miyake, M., Yamada, K., Mukai, T., Odomi, M.,
Toguchi, H., Liversidge, G.G., Higaki, K. & Kimura, T. (2006) Effect
of particle size reduction on dissolution and oral absorption of a
poorly water-soluble drug, cilostazol, in beagle dogs. Journal of Con-
trolled Release, 111, 56–64.Kaeser, B., Charoin, J.E., Gerber, M., Oxley, P., Birnboeck, H., Saiedaba-
di, N. & Banken, L. (2005) Assessment of the bioequivalence of two
nelfinavir tablet formulations under fed and fasted conditions in
healthy subjects. International Journal of Clinical Pharmacology and
Therapeutics, 43, 154–162.
Lainesse, C. (2012) International veterinary bioequivalence guideline
similarities and differences between Australia, Canada, Europe,
Japan, New Zealand and the United States. The AAPS Journal, 14,
792–798.
Lifschitz, A., Pis, A., Alvarez, L., Virkel, G., Sanchez, S., Sallovitz, J.,
Kujanek, R., & Lanusse, C. (1999) Bioequivalence of ivermectin for-
mulations in pigs and cattle. Journal of Veterinary Pharmacology and
Therapeutics, 22, 27–33.
Martinez, M.N. (2011) Factors influencing the use and interpretation
of animal models in the development of parenteral drug delivery sys-
tems. The AAPS Journal, 13, 632–649.Martinez, M.N. & Apley, M.D. (2012) Drug solubility classification in
the bovine. Journal of Veterinary Pharmacology and Therapeutics, 35
(Suppl. 1), 93–97.
Martinez, M.N. & Fahmy, R. (2012) The scientific basis for establishing
solubility criteria for veterinary species. Journal of Veterinary Pharma-
cology and Therapeutics, 35 (Suppl. 1), 81–86.Martinez, M.N. & Hunter, R.P. (2010) Current challenges facing
the determination of product bioequivalence in veterinary
medicine. Journal of Veterinary Pharmacology and Therapeutics, 33,
418–433.Martinez, M.N., Pedersoli, W.M., Ravis, W.R., Jackson, J.D. & Cullison, R.
(2001) Feasibility of interspecies extrapolation in determining the bio-
equivalence of animal products intended for intramuscular administra-
tion. Journal of Veterinary Pharmacology and Therapeutics, 24, 125–135.Martinez, M., Amidon, G., Clarke, L., Jones, W.W., Mitra, A. & Riviere,
J. (2002) Applying the biopharmaceutics classification system to vet-
erinary pharmaceutical products. Part II. Physiological consider-
ations. Advanced Drug Delivery Reviews, 54, 825–850.Martinez, M.N., Papich, M.G. & Riviere, J.E. (2004) Veterinary applica-
tion of in vitro dissolution data and the biopharmaceutics classifica-
tion system. Pharmacopeial Forum, 30, 2295–2303.
Martinez, M., Hunter, R.P., Baynes, R., Bermingham, E., Claxton, R.,
Cole, C., Del Castillo, J., Gehring, R., Harshman, K., Lainesse, C.,
Lucas, A., Modric, S. & Robinson, J. (2011) The 2010 AAVPT/EA-
VPT/ECVPT bioequivalence workshop. Journal of Veterinary Pharma-
cology and Therapeutics, 34, 105–107.McGilveray, I., Midha, K., Skelly, J., Dighe, S., Doluisio, J., French, I.,
Karim, A. & Burford, R. (1990) Consensus report from “Bio Interna-
tional ‘89”: issues in the evaluation of bioavailability data. Journal of
Pharmaceutical Sciences, 79, 945–946.Melander, A. & McLean, A. (1983) Influence of food intake on presys-
temic clearance of drugs. Clinical Pharmacokinetics, 8, 286–296.Noonan, P. (2009) Biopharmaceutical limitations of the proposed guid-
ance. Available from: http://www.fda.gov/downloads/AdvisoryCom-
mittees/CommitteesMeetingMaterials/Drugs/AdvisoryCommitteefor-
PharmaceuticalScienceandClinicalPharmacology/UCM179424.pdf.
Radwan, A., Amidon, G.L. & Langguth, P. (2012) Mechanistic investi-
gation of food effect on disintegration and dissolution of BCS class III
compound solid formulations: the importance of viscosity. Biopharma-
ceutics & Drug Disposition, 33, 403–416.
Shah, V.P., Yacobi, A., Barr, W.H., Benet, L.Z., Breimer, D., Dobrinska,
M.R., Endrenyi, L., Fairweather, W., Gillespie, W., Gonzalez, M.A.,
Hooper, J., Jackson, A., Lesko, L.J., Midha, K.K., Noonan, P.K., Pat-
naik, R. & Williams, R.L. (1996) Evaluation of orally administered
highly variable drugs and drug formulations. Pharmaceutical
Research, 13, 1590–1594.
Singh, B. (2005) A quantitative approach to probe the dependence and
correlation of food-effect with aqueous solubility, dose/solubility
ratio, and partition coefficient (Log P) for orally active drugs admin-
istered as immediate-release formulations. Drug Development Research,
65, 55–75.Yu, L.X. (2008) Pharmaceutical quality by design: product and process
development, understanding, and control. Pharmaceutical Research,
25, 781–791.
Yu, L., Bunge, A. & Wilkin, J. (2003) Bioequivalence of topical prod-
ucts – discussion points, food and drug administration advisory com-
mittee for pharmaceutical science. Available from: http://www.fda.
gov/ohrms/dockets/ac/03/slides/3996s2.htm (accessed 23 March
2013).
Published (2013). This article is a U.S. Government work and is in the public domain in the USA.
12 M. N. Martinez