Embed Size (px)
Citation preview

BIOCHEMISTRYBONE METABOLISM
MSK BLOCK SYSTEM
Nabil Bashir
October 1st, 2009

Bone• Inorganic (67%)
– Hydroxyapatite 3 Ca10(PO4)6(OH)2
– There is some amorphous calcium phosphate
• Organic (33%) component is called osteoid– Type I collagen (28%)– Non-collagen structural proteins (5%)
• Proteoglycans• Sialoproteins• Gla-containing proteins (gamma carboxyglutamate)• Phosphoproteins• Bone specific proteins: osteocalcin, osteonectin
– Growth factors and cytokines (Trace)
• Bone undergoes continuous turnover or remodeling throughout life– About 20% of bone is undergoing remodeling at any one
time

Osteoblast and Osteoclast Function
Osteoblasts• Bone formation• Synthesis of matrix
proteins– Type I collagen– Osteocalcin– Others
• Mineralization• Activation of
osteoclasts via RANKL production
Osteoclasts• Bone resorption
– Degradation of proteins by enzymes
– Acidification
• RANK is activated by RANKL, and this leads to cells differentiation to osteoclasts


PTH and Osteoblastogenesis

Osteoclast Mediated Bone Resorption

Osteoclastogenesis: RANK/RANKL/OPG axis
RANK:Receptor activator of nuclear factor (NF)-kB
RANKL:RANK ligand
OPG:Osteoprotegerin (cytokine)
Activating factors:M-CSF, IL-6etc.
ASBMR Bone Curriculum

Osteoclastogenesis
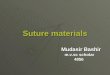
Activating factors cause the lining cells to produce RANKL, and then the RANK of the preosteoclasts binds with the RANKL and the forms multinucleated activated osteoclasts (10-20 fused cells, called polykaryons)
OPG also binds with RANKL, preventing the preosteoclast RANK from binding
ASBMR Bone Curriculum


Hormonal Control of Resorption: Pro-resorptive
Most of the proresorptive factors upregulate mRNA expression of RANKL in osteoblasts
Boyle et al, Nature 2003

Hormonal Control of Resorption: Anti-resorptive
Boyle et al, Nature 2003

Genetic Mutations
What would an OPG knock-out mouse look like?
Boyle et al, Nature 2003

CALCIUM& PHOSPHORUS HOMEOSTASIS
• PTH,
• VIT D,
• CALCITONIN,
• ESTROGENS

CaPO4
1,25 D
INTESTINE
Absorption
Ca2+
BLOOD
KIDNEYPTH
Bioactivation25D 1,25D
PTH
1,25 D
PO4
BONE
Mineralization
PTH
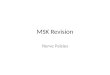
Figure 1. Control of blood Ca2+ and PO4
3- matrix
1,25 D
PO4
Reabsorption
Ca2+
PTH1,25 D
Ca2+Resorption
PO4
PTH, in response to low serum Ca, increases plasma Ca by increasing bone resorption, and renal reabsorption of CaPTH prevents hyperphosphatemia, which could be caused by the PTH effect on bone resorption, by inhibiting renal reabsorption of phosphate
PTH activates the hydroxylation of 25(OH)D3 to the active 1,25(OH)2D3 form1,25(OH)2D3, in response to low serum Ca, increases plasma Ca by increasing intestinal absorption, bone resorption, and renal reabsorption of Ca
1,25(OH)2D3 increases intestinal and renal absorption of phosphate to help promote bone mineralization
calcitonin (CT) can counteract the effect of PTH on bone resorptionestrogen (E2) counteracts effects of PTH and 1,25(OH)2D3 on bone resorption
CTE2

Bone Remodeling• Osteoclasts dissolve
bone– Large multinucleated
giant cells
• Osteoblasts produce bone– Have receptors for
PTH, CT, Vitamin D, cytokines, and growth factors
– Main product is collagen
• When osteoblasts become encased in bone, they become osteocytes

MOP
ODF receptor
Differentiationand fusion
c-FMS receptor
Gs cAMP PKA
OsteoblastBone constructor
ODF
Osteoprotegerinreceptor decoy
osteoblast
osteoclast
OsteoclastBone destructor
Figure 3. Control of bone remodeling by PTH
IL-6IL-6; othercytokines
activation
M-CSF
PTH
PTH
MOP – monocytic osteoclast progenitor cells
M-CSF – macrophage colony stimulating factor
ODF – osteoclast differentiating factor

IL-6Gs cAMP PKA
IL-6; othercytokines
ODF
OsteoblastBone constructor
OsteoclastBone destructor
Figure 3. Control of bone remodeling by PTH and calcitonin
activationCTPKA cAMP
inactivation PTH
Gs
CT gene can yield calcitonin gene-related peptide (CGRP) if processed differently (alternative mRNA splicing)
CGRP = a potent vasodilator
Calcitonin secreted by thyroid C-cells in response to hypercalcemia

HO
Vitamin D3
Diet
HO
OH
25(OH) D3
Liver
25-OHase
OHHO
OH
1,25(OH)2 D3
(active hormone form)
Kidney
1-OHase
HO 7
Provitamin D3
(7-dehydrocholesterol: Intermediate in cholesterol synthesis)
UV fromsunlight
Skin
24,25(OH)2 D3
(inactive form)
OH
HO
OH
24-OHase(kidney; manyother tissues)
High Ca2+
or PO43-
Figure 4. Photobiosynthesis of vitamin D3 and its metabolism
Specific receptors in intestine, bone, kidney
Ca:Intestinal absorptionRenal reabsorptionBone resorption
PO4:Intestinal absorption Renal reabsorption

MOPDifferentiationand fusion
OsteoblastBone constructor
ODF receptor
1,25D3
osteoblast
osteoclast
OsteoclastBone destructor
Figure 7. Control of bone remodeling by 1,25(OH)2D3
inactivation
c-FMS receptor
M-CSF
CTPKA cAMP Gs
1,25D3
RXR receptor
VDR receptor Nucleus
mRNA
Osteocalcin
Ca2+
Gla
IL-6IL-6; othercytokines
activationODF
Chemotaxis

MOP
ODF receptor
Differentiationand fusion
c-FMS receptor
IL-6IL-6; othercytokines
ODF
OsteoblastBone constructor
PTH, 1,25D3
osteoblast
osteoclast
OsteoclastBone destructor
Figure 8. Control of bone remodeling by PTH and 1,25(OH)2D3 and antagonism of their effects by estrogen and androgen
activationCTPKA cAMP
inactivation
M-CSF
Gs
1,25D3
3 mRNA
Ca2+
Osteocalcin
Gla
Collagen matrix Ca2+/PO4
3-
Bone mineralization
Gs cAMP PKA PTH
Estrogen (E2)and Androgen
Estrogen (E2)and Androgen
proliferation collagen syn.
Osteoblast
E2