-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
1/8
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
2/8
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
3/8
was performed prospectively in 819 ofthe 858 patients included
in the finalanalyses. In the remaining patients, allwith
pheochromocytoma, measure-ments of plasma free metanephrineswere
performed after removal of tu-
mors. Twenty-four hour urine collec-tions were obtainedfrom 790
of the858patients included in the final analyses.Urine samples were
usually subjectedto assays of 2 to 3 different analytes.
Plasma was analyzed, using high-performance liquid
chromatography(HPLC), for concentrations of catechol-amines,
norepinephrine and epineph-rine, and free metanephrines,
normeta-nephrine, and metanephrine.1 7 - 1 9
Metanephrines in urine were ana-lyzed as fractionated
normetaneph-rine and metanephrine by HPLC or as
total metanephrines by spectrophotom-etry.10,20 Urinary VMA was
measuredspectrophotometrically and urinary cat-echolamines by
HPLC.21,22 Upper ref-erence limits for biochemical tests
areprovided as established by the princi-pal laboratories
responsible for eachtest(TABLE 2).11
All 858 assays of plasma free meta-nephrines and 91% of the 855
assaysof plasma catecholamines were per-formed at the National
Institutes ofHealth. Seventy-five percent of the 557
assays of urinary fractionated meta-nephrineswere performed by
Quest Di-agnostics (Collegeville, Pa). Seventy-two percent of the
710 assays of urinarycatecholamines, 74% of the 297 as-saysof
urinary total metanephrines, and79% of the 616 assays of urinary
VMAwereperformed by MayoMedical Labo-ratories (Rochester, Minn).
The re-maining assays were performed at dif-ferent laboratories
depending on thecenter where patients were evaluated.
Data Analysis
For biochemical tests involving pairs ofmeasurements (eg,
normetanephrineand metanephrine or norepinephrineand epinephrine in
plasma or urine),a false-negative result in a patientwith
pheochromocytoma or a true-negative result in a patient
withoutpheochromocytoma was defined as a
value for each measurement lower thanthe upper reference limit.
A true-positive result for pairs of measure-ments in a patient with
pheochromo-cytoma or a false-positive result in apatient without
pheochromocytoma
was defined as a value for either or bothmeasurements equal to
or higher thanthe appropriate upper reference limit.
Sensitivity was calculated from thepercentageof
true-positiveover the totalof true-positive plus false-negative
testresults in patients with pheochromo-cytoma. Specificity was
calculatedfromthepercentage of true-negativeover thetotal of
true-negative plus false-positive test results in patients with-out
pheochromocytoma. Differencesinsensitivity and specificity were
exam-ined using the McNemar test and are
illustrated using 95% confidence inter-vals (CIs).
For each analyte, a receiver operat-ing characteristic (ROC)
curve wascon-structed from the relationship be-tween true-positive
and false-positiveresults (ie, sensitivity vs 1specific-ity) at
different upper reference limits
for each analyte.23 As summary mea-sures of the diagnostic
utility of eachtest, independent of upper referencelimits, areas
under ROC curves werecalculated and differences among testsexamined
according to the method by
Hanley and McNeil.
24
Negative predictive values were cal-culated from the percentage
of true-negative over the total of true-negativeplus false-negative
test results. Positivepredictive values were calculated fromthe
percentage of true-positive over thetotal of true-positive plus
false-positiveresults. Positive and negative predic-tive values of
each test were calculatedat different prevalences of
pheochromo-cytoma to establish posttest probabili-ties of
pheochromocytoma at differentpretest probabilities of the
tumor.
RESULTS
Biochemical Test Results
Relative to patients in whom pheochro-mocytoma wasexcluded,
medianplasmaconcentrations of free metanephrineswere increased by
7-foldin patients withhereditary pheochromocytoma and 21-
Table 2. Plasma Concentrations of Catecholamines and
Metanephrines and Urinary Outputsof Catecholamines, Metanephrines,
and Vanillylmandelic Acid
UpperReference
Limit
PheochromocytomaConfirmed*
PheochromocytomaExcluded*
Hereditary Sporadic Hereditary Sporadic
Plasma, nmol/LFree metanephrines
Normetanephrine 0.6 2.2 (0.3-69) 6.3 (0.4-173) 0.3 (0.1-1.6) 0.3
(0.1-2.2)
Metanephrine 0.3 0.2 (0-15) 0.6 (0-383) 0.1 (0-0.5) 0.2
(0-1.2)
CatecholaminesNorepinephrine 2.9 4.8 (1-80) 10.6 (0.7-1360) 1.4
(0.4-8.1) 2.1 (0.3-29)
Epinephrine 0.5 0.2 (0-4.8) 0.4 (0-1111) 0.1 (0-1.3) 0.1
(0-18)
Urine, mol/dFractionated
metanephrinesNormetanephrine
Women 1.75.2 (1.8-33) 17.7 (0.9-191) 1.2 (0.1-8.2) 2.1
(0.4-10)
Men 3.0
MetanephrineWomen 0.7
0.5 (0.1-28) 1.1 (0.1-466) 0.4 (0.1-2.8) 0.5 (0.1-22)Men 1.2
CatecholaminesNorepinephrine 0.5 1 (0.1- 5.4) 1.7 (0.1- 31) 0.2
(0-1) 0.3 (0.1-5.6)
Epinephrine 0.1 0 (0-2.1) 0.1 (0-7) 0 (0-0.1) 0 (0-0.4)
Total metanephrines 6 8 ( 2-260) 21 (3-234) 3 (1-12) 3
(1-16)
Vanillylmandelic acid 40 37 (11-330) 83 (13-777) 17 (3-56) 23
(2-81)
*Values are expressed as median (range).Measured by
high-performance liquid chromatography after acid
deconjugation.Measured together as a single analyte by
spectrophotometry after acid deconjugation.
DIAGNOSIS OF PHEOCHROMOCYTOMA
2002 American Medical Association. All rights reserved.
(Reprinted) JAMA, March 20, 2002Vol 287, No. 11 1429
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
4/8
fold in patients with sporadic pheochro-mocytoma (Table 2).
These increaseswere consistently larger than those ofplasma
norepinephrine (3-foldand5-foldincreases), urinary norepinephrine
(5-fold and 6-fold increases), urinary frac-tionated
normetanephrine (4-fold and8-fold increases), urinary total
meta-nephrines (3-fold and 7-fold in-creases), and urinary VMA
(2-fold and4-fold increases). Increases in all ana-lytes were
larger in patients with spo-radic rather than hereditary
pheochro-
mocytoma.
Test Sensitivity
The sensitivities of diagnostic tests fordetection of hereditary
or sporadicpheochromocytoma ranged from a lowof 46% (95% CI,
34%-59%) for use ofurinary VMA in the detection of he-reditary
pheochromocytoma to a highof 99% (95% CI, 96%-100%) for use
ofplasma free metanephrines in the de-tection of sporadic
pheochromocy-toma (TABLE 3).
Amongall patients withpheochromo-cytoma, sensitivities were
thehighest formeasurements of plasma free metaneph-rines at 99%
(95% CI, 96%-100%), fol-lowed closely by urinary
fractionatedmetanephrines at 97% (95% CI,92%-99%).Sensitivitiesof
both theabovetests considerably (P.001) exceededthose for urinary
catecholaminesat 86%
(95% CI, 80%-91%), plasma catechol-amines at 84% (95% CI,
78%-89%), uri-nary total metanephrines at 77% (95%CI, 68%-85%), and
urinary VMA at 64%(95% CI, 55%-71%).
Theabove variations in sensitivities ofdiagnostic tests showed
similar pat-terns inpatients with hereditary andspo-radic
pheochromocytoma (Table 3).Plasma free metanephrines and uri-nary
fractionated metanephrines of-fered the highest sensitivities.
Plasmaand urinary catecholamines had inter-
mediate sensitivities. Urinarytotal meta-nephrines
andVMAconsistentlyshowedthe lowest sensitivities in both groupsof
patients. The sensitivities of all testswere higher for detection
of sporadicpheochromocytoma than for detectionof hereditary
pheochromocytoma.
Test Specificity
Specificities of biochemical testsrangedwidely from 45% (95% CI,
36%-51%)for urinary fractionated metaneph-rines in patients tested
for sporadic
pheochromocytoma to 99% (95% CI,98%-100%) for urinary VMA in
pa-tients tested for hereditary pheochro-mocytoma (Table 3).
Among all patients tested for pheo-chromocytoma, the highest
specifici-ties were 95% (95% CI, 93%-97%) fortests of urinaryVMA
and 93% (95% CI,89%-97%)fortests of urinary total meta-
nephrines. Specificities were interme-diate for tests of plasma
free metaneph-rines at 89% (95% CI, 87%-92%),urinarycatecholamines
at 88%(95% CI,85%-91%), and plasma catechol-amines at 81% (95%
CI,78%-84%), and
lower than those of all other tests(P.001) for urinary
fractionatedmeta-nephrines at 69% (95% CI, 64%-72%).
In contrast to sensitivities, specifici-ties of all tests were
higher in patientstested for hereditary pheochromocy-toma than for
sporadic pheochromo-cytoma (Table 3). In both groups, uri-nary VMA
and total metanephrinesoffered the highest specificities and
uri-nary fractionated metanephrines thelowest specificities.
False-Negative Plasma
Free MetanephrinesOnly 2 of the 76 patients with
heredi-tarypheochromocytoma and1 ofthe138patients with sporadic
pheochromocy-toma had normal levels of plasma freemetanephrines.
Both hereditary caseswere in patients who were normoten-sive
andasymptomaticandhadno otherbiochemical evidence ofthetumor.
Bothwere patients with von Hippel-Lindausyndromeandhad
singleadrenal tumorsoflessthan1cmindiameter,whichwereidentified and
removed coincidentally
during surgery for renal carcinoma.The single false-negative
result for
plasma free metanephrines in patientswith sporadic
pheochromocytoma in-volved a patient tested for possible tu-mor
recurrence 13 years after theremoval of a large extra-adrenal
pheo-chromocytoma. Computed tomogra-phy and all biochemical tests
yieldednegative results. The patient was subse-quently
diagnosedwithmetastaticpheo-chromocytoma 312 years later.
Sincethere was no evidence for a hereditary
basis for thepatients disease, it was pre-sumed that the
malignancy developedsecondary to remaining
diseasethatwentundetected for more than 16 years afterthe original
tumor was removed. Thus,despite the considerable time
betweenbiochemical testing and final diagnosis,all tests performed
were designated asproviding false-negative results.
Table 3. Sensitivities and Specificities of Biochemical Tests
for Diagnosis of Hereditary andSporadic Pheochromocytoma*
Sensitivity, % Specificity, %
Heredi tary Sporadi c Hereditary Sporadic
PlasmaFree metanephrines 97 (74/76) 99 (137/138) 96 (326/339) 82
(249/305)
Catecholamines 69 (52/ 75) 92 ( 126/137) 89 (303/339) 72 (220/
304)Urine
Fractionated metanephrines 96 (26/27) 97 (76/78) 82 (237/288) 45
(73/164)
Catecholamines 79 (54/68) 91 (97/107) 96 (312/324) 75
(159/211)
Total metanephrines 60 (27/45) 88 (61/69) 97 (91/94) 89
(79/89)
Vanillylmandelic acid 46 (30/65) 77 (66/86) 99 (310/312) 86
(132/153)
*The reference limits used to calculate sensitivity and
specificity are presented in Table 2.For free plasma metanephrines
or urinary fractionated metanephrines, sensitivity was calculated
from patients with
pheochromocytoma and false-negative test results for both
normetanephrine and metanephrine. For plasma andurine
catecholamines, sensitivity was calculated from patients with both
false-negative test results for nonrepineph-rine and epinephrine.
Numbers in parentheses indicate true positive over true positive
plus false-negative.
For free plasma metanephrines or urinary fractionated
metanephrines, specificity was calculated from patients with-out
pheochromocytoma and with false-positive test results for either
normetanephrine or metanephrine. For plasmaand urine
catecholamines, specificity was calculated from patients without
pheochromocytoma and with false-positive test results for either
nonrepinephrine or epinephrine. Numbers in parentheses indicate
true negative overtrue negative plus false-positive.
DIAGNOSIS OF PHEOCHROMOCYTOMA
1430 JAMA, March 20, 2002Vol 287, No. 11 (Reprinted) 2002
American Medical Association. All rights reserved.
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
5/8
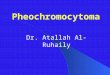
ROC Curves
Integrated comparisonof sensitivity andspecificity using
ROCcurvesshowedthatthediagnostic power
ofplasmafreemeta-nephrineswassuperior tothat ofallothertests
(FIGURE 1). The areas under the
ROC curves for plasma catecholamines(0.927),urinary
catecholamines (0.931),urinary total metanephrines(0.919),
andurinary VMA (0.896) were all signifi-cantly lower (P.001) than
the area forplasma free metanephrines (0.985). Al-though closer,
the area under the ROCcurvefor urinary fractionatedmetaneph-rines
(0.960) was also lower (P=.01)than that for plasma free
metaneph-rines (0.985).
Areas under the ROC curves wereonly marginally improved when
testsof urinary fractionated metanephrines
were combined with those for urinarycatecholamines (0.965) or
plasma cat-echolamines (0.969) or when tests ofurinary total
metanephrines and cat-echolamines were combined (0.949)(Figure 1).
Thus, combining tests fordifferent analytes did not improve
di-agnostic efficacy beyond that of a singletest of plasma free
metanephrines.
True-positive rates (ie, test sensitiv-ity) at higher upper
reference limitswhen false-positive rates were zero
(ie,whentestspecificityequaled100%) were
higher for plasma free metanephrinesthan for other tests (Figure
1). None ofthe 644 patients without pheochromo-cytoma had a plasma
concentration ofnormetanephrine above 2.19 nmol/L orof metanephrine
above 1.20 nmol/L,whereas79%of patientswith pheochro-mocytomahad
plasma concentrationsofnormetanephrine or metanephrineabove these
levels (TABLE 4).
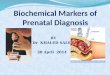
Positive and Negative
Predictive Values
Negative predictive values of tests ofplasma and urinary
metanephrines atdifferent prevalences of pheochromo-cytoma showed
that negative test re-sults for plasma free and urinary
frac-tionated metanephrines provided thehighest probabilities for
excludingpheochromocytoma at all pretest preva-lences of the tumor
(FIGURE 2). How-
ever, the posttest probability of a pheo-chromocytoma from a
positive testresult for plasma free metanephrines,although similar
to that for urinary totalmetanephrines, was consistently higherthan
that from a positive test result for
urinary fractionated metanephrines atall pretest prevalences of
the tumor.
COMMENT
The present examination of biochemi-cal tests used in the
diagnosis ofpheochromocytoma provides severaladvances
overpreviousstudies.First,thisstudycomprehensively compared
mea-surements of plasma free metaneph-rines with all other commonly
avail-able biochemical tests used to diagnoseexcess catecholamine
production. Sec-ond, these comparisons were made in
large populations of patients with andwithoutpheochromocytoma,
whoweretested for the tumor because of clini-cally appropriate
predisposing condi-tions or suspicioussymptoms andsigns.Finally,
standardcriteriathatwereinde-pendent of the biochemical tests
beingcompared were used to assign patientsintogroups with
andwithout thetumor.
Sensitivity, Specificity,
and ROC Curves
The present study confirms the find-
ings of several other reports thatmeasurements of plasma free
meta-nephrinesor urinary fractionated meta-nephrines offer higher
sensitivity for di-agnosis of pheochromocytoma thanmeasurements of
plasma or urinary cat-echolamines or of urinary total
meta-nephrines or VMA.8,9,11,14,16 Our com-parisons further
establish that amongall tests, including urinary fraction-ated
metanephrines, measurements ofplasma free metanephrines provide
thebest test for excluding or confirming
pheochromocytoma.Since measurements of urinary frac-tionated
metanephrines andplasmafreemetanephrines offer similarly high
sen-sitivity, a negative result for either testis equally effective
for excluding pheo-chromocytoma. However, because uri-nary
fractionated metanephrines havelow specificity, tests of plasma
free
Figure 1. Receiver Operating CharacteristicCurves
True-PositiveRate
(TestSensitivity)
1.0
0.6
0.8
0.4
0.2
0
0 0.2 0.6
Plasma Free Metanephrines
Plasma Catecholamines
Urinary Catecholamines
Urinary Vanillylmandelic Acid
1.00.80.4
1.0 0.8 0.4 00.20.6
True-Negative Rate (Specificity)
Plasma Free Metanephrines vs Urinary
Catecholamines and Vanillylmandelic Acid
A
Plasma Free Metanephrines vs Urinary
Fractionated Metanephrines and Total
Metanephrines
B
Plasma Free Metanephrines
vs Test Combination
C
True-Positive
Rate(TestSensitivity)
1.0
0.6
0.8
0.4
0.2
0
0 0.2 0.6
Plasma Free Metanephrines
Urinary Fractionated Metanephrines
Urinary Total Metanephrines
1.00.80.4
1.0 0.8 0.4 00.20.6
True-PositiveRate
(TestSensitivity)
1.0
0.6
0.8
0.4
0.2
0
0 0.2 0.6
Plasma Free Metanephrines
Urinary Fractionated Metanephrinesand Plasma Catecholamines
Urinary Total Metanephrinesand Urinary Catecholamines
1.00.80.4
1.0 0.8 0.4 00.20.6
False-Positive Rate (1 Specificity)
Urinary Fractionated Metanephrinesand Urinary Catecholamines
Relationships between rates of true-positive test re-sults (ie,
sensitivity) andratesof false-positive test re-sults (1
specificity) were calculated at different up-perreferencelimitsfor
each ofthe tests.At higherupperreference limits, rates of
true-positive test results de-crease(ie,
sensitivitydecreases),whereas rates of false-positive test results
increase (ie, specificity increases).
DIAGNOSIS OF PHEOCHROMOCYTOMA
2002 American Medical Association. All rights reserved.
(Reprinted) JAMA, March 20, 2002Vol 287, No. 11 1431
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
6/8
metanephrines exclude pheochromo-cytoma in many more patients
with-
out the tumor than do tests of urinaryfractionated
metanephrines.The above considerations illustrate the
importance of ROC curves for compar-ing different tests. At
equivalent levelsof sensitivity, the specificity of plasmafree
metanephrines is higher than thatof other tests. At equivalent
levels ofspecificity, the sensitivity of plasma free
metanephrines is also higher than thatof other tests, including
urinary frac-tionated metanephrines.
Multiple Biochemical Tests
To minimize the risk of missing a pa-tient with
pheochromocytoma, clini-cians often use multiple biochemical
tests during the initialdiagnostic workupof patients with
suspected tumors. Al-though this may increase sensitivity, itis at
the cost of decreased specificity.Thus, tests involving pairs of
measure-ments, such as fractionated catechol-amines or
metanephrines, have lowerspecificity and higher sensitivity
thantests involving single measurements,such as urinary VMA or
total metaneph-rines (Table 3).8 As shown by ROCcurves, the
diagnostic utility of tests ofplasma free metanephrines remains
su-
perior to that of other tests even whenthe latter are used in
combination.The above considerations lead us to
recommend against use of multiplebio-chemical tests to exclude
pheochro-mocytoma in favor of a single test ofplasma free
metanephrines. In pa-tients with negative test results forplasma
free metanephrines, indiscrimi-nate use of extra tests is unlikely
to im-prove diagnostic efficacy. If multiplebiochemical tests have
been run, thede-cision to exclude pheochromocytomashould be basedon
whether plasma freemetanephrines show a negative test re-sult,
regardless of whether other test re-sults are positive or
negative.
Differences in Test
Performance Explained
Whydo plasmafreemetanephrinespro-vide the best test to diagnose
pheochro-
mocytoma? First, plasma free meta-nephrines are produced
continuouslyby metabolismof catecholamineswithinpheochromocytoma
tumor cells.25-27
This contrasts with episodic secretionof catecholamines. Second,
sympa-
thoadrenal excitation causes largeincreases in catecholamine
release,whereas plasma free metanephrines re-mainrelatively
unaffected.14,25,27,28 Third,VMA and the total and
fractionatedmetanephrines measured in urine aredifferent
metabolites from the freemeta-nephrines measured in plasma, and
areproduced in different parts of the bodyby metabolic processes
not directly re-lated to the tumor itself.28-30 Urinarytotal and
fractionated metanephrinesaremeasured after a deconjugation stepand
largely reflect levels of conjugated
metanephrines that are produced out-side of tumor tissue.
Similarly, VMA isproduced mainly in the liver.
Sporadic vs Hereditary
Pheochromocytoma
The lower sensitivity and higher speci-ficity of biochemical
tests for hereditarycompared with sporadic pheochromo-cytoma
reflect differentreasons for test-ing in the 2 groups.31 Routine
screeningfor pheochromocytoma in patientswitha hereditary
predisposition to the tu-
mor often leadsto detection of small tu-mors that release
catecholamines inamounts that are insufficient to pro-duce signs or
symptomsof the tumor.
Incontrast,sporadicpheochromocytomaistypically suspected because of
signs andsymptomsof catecholamine excess, pro-duced by larger more
easilydetectedtu-mors thanfound by routinescreening inhereditary
pheochromocytoma. More-over, patients tested for sporadic
pheo-chromocytoma who do not have the tu-mor are often symptomatic
of some
condition associated with sympathoad-renal activation,leadingto
relatively highnumbers of false-positive results.
The consistently lower specificities ofbiochemical tests in
patients tested forsporadic rather than for
hereditarypheochromocytomamay alsoreflect re-ferral of patients in
the former groupwith previously determined positive
Table 4. Plasma Concentrations, Specificity, and Sensitivity of
Plasma Free Metanephrines atEstablished Upper Reference Limits
Compared With Reference Limits Adjusted to Provide aZero
False-Positive Rate
Upper Reference Limits Plasma Level, nmol/L Test Specificity, %
Test Sensitivity, %
EstablishedNormetanephrine 0.61
89 99Metanephrine 0.31
Adjusted*Normetanephrine 2.19
100 79Metanephrine 1.20
*Plasma concentrations and test sensitivity adjusted to provide
a zero false-positive rate were established from re-ceiver
operating characteristic curves in Figure 1.
Figure 2. Relationships Between Pretest andPosttest
Probability
PosttestProbability
1.0
0.6
0.8
0.4
0.2
0
0 0.2 0.6
Plasma Free Metanephrines
Urinary Fractionated Metanephrines
Urinary Total Metanephrines
1.00.80.4
Pretest Probability (Prevalence)
Plasma Free MetanephrinesPositive Predictive Values
Negative Predictive Values
Urinary Fractionated Metanephrines
Urinary Total Metanephrines
Positive
Predict
iveValue
s
1Ne
gativ
ePredict
iveValue
s
A positive or a negative result for tests of plasma orurinary
metanephrines changes the respective prob-abilities of having or
not having pheochromocytomain relationshipto
differentpretestprobabilities (preva-lences) of the tumor. The
dotted line represents therelationship expected between pretest and
posttestprobability if a test hadno diagnostic value.Relation-ships
illustrated by the filled symbols show the prob-abilities of
havinga pheochromocytomabased on posi-tive(abnormal)test
results,whereasthe open symbolsshow the probabilities of not having
a pheochromo-cytoma based on negative (normal) test results.
DIAGNOSIS OF PHEOCHROMOCYTOMA
1432 JAMA, March 20, 2002Vol 287, No. 11 (Reprinted) 2002
American Medical Association. All rights reserved.
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
7/8
biochemical tests. Thus, specificities ofbiochemical tests for
detection of spo-radic pheochromocytoma in the pres-ent study are
likelyto belower than inunselected populations tested by
com-mercial laboratories, but should re-
flect those expected in populationstested at referral
centers.Apart from patients at risk for heredi-
tary pheochromocytoma, patients withpreviously resected tumors
are anotherat-risk group who should be tested pe-riodically for the
tumor regardless ofsigns and symptoms. The importance ofthis group
is illustratedby thesingle pa-tient who tested negative for
pheochro-mocytoma by all tests 312 years beforemetastatic disease
was finally diag-nosed and 16 years after removal of theprimary
tumor.Thesensitivity of plasma
free metanephrines is not always suffi-cient for detection of
microscopic re-current or metastatic disease or smalltumors (1 cm)
in patientswith heredi-tary pheochromocytoma.
Pretest and Posttest Probabilities
Typically fewer than 1% of hyperten-sive patients tested for
pheochromo-cytoma have the tumor. In some pa-tient groups, such as
those withhypertension and an adrenal mass, thepretest probability
of a pheochromo-
cytoma may be higher. The probabil-ity that a negative test
result excludespheochromocytoma or that a positivetest result
confirms the tumor de-pends in part on the pretest probabil-ity of
the disease. These posttest prob-abilitiestherefore require
calculation ofpositive and negative predictive val-ues at different
pretest probabilities(prevalences) of the tumor.
As shown in Figure 2, a negative testresult for plasmafree
metanephrines orurinaryfractionatedmetanephrines pro-
vides a high probability of excludingpheochromocytoma at all
clinically rel-evant pretest probabilities of the tu-mor. In
contrast, at the typically lowprevalences of pheochromocytoma,
thelikelihood of the tumor after a singlepositive test remains low
even for testswith up to 95% specificity. A routinepractice to
further increase or de-
crease the likelihood of pheochromo-cytoma involves use of
additional bio-chemical tests.32
In patients with positive results foran initial test of plasma
free metaneph-rines,extratests canbe useful, butjudg-
ing the likelihood of a pheochromocy-toma should first take into
accountresults of ROC curves. In particular, athigher upper
reference limits, in whichtest specificity is 100%, plasma
con-centrations of free normetanephrinehigher than 2.19 nmol/L or
of free meta-nephrine higher than 1.20 nmol/L un-equivocally
confirm a pheochromocy-toma in 79% of patients with the tumor(Table
4), a higher proportion than forother tests (Figure 1). The
probabilityof pheochromocytoma in these pa-tients is so high that
further biochemi-
cal tests to confirm the tumor may beunnecessary. In the
remaining pa-tients, in whom increased levels are in-sufficient to
unequivocally confirm a tu-mor, additional judiciously
selectedfollow-up tests are appropriate, withad-ditional attention
focused on possiblecauses of false-positive test results.32-35
False-Positive Test Results
Because of the low prevalence of pheo-chromocytoma in the
patient groupsusually tested for the tumor, false-
positive results can be expected to out-number true-positive
results for all bio-chemical tests, including plasma
freemetanephrines. There are 3 potentialsourcesof false-positive
testresults: diet,drugs, and stressors.
Caffeic acid, a catechol found in cof-fee(including
decaffeinated coffee), andits derivative dihydrocaffeic acid are
di-etary substances known to interferewithassays of plasma
catecholamines.36
Moreover, both catechols are excellentsubstrates for catechol
O-methyltrans-
ferase, the enzyme that converts cat-echolaminesto
metanephrines, and thiseasily could affect plasmalevels of
meta-nephrines. There are many other uni-dentified dietary
constituentsthatcanin-fluence the results of HPLC assays.
Thesimplest way to avoid these sources offalse-positive results is
by drawingbloodsamples in patients who have fasted.
Acetaminophen is the only directsource of interference with
assays ofplasmafreemetanephrines thatwe haveidentified to date.19
However, caffeineand nicotine both increase plasma lev-els of
catecholamines and should also
be avoided. In our series, treatment withtricyclic
antidepressants or phenoxy-benzamine (dibenzyline) were majorcauses
of false-positive test results fornorepinephrineanditsmetabolites,
pre-sumably due to presynaptic actions onsympathetic nerves.
Phenoxybenza-mine, a nonselective -adrenoceptorblocker commonly
used to treat pa-tients with pheochromocytoma, can beparticularly
troublesome.
Although plasma levels of free meta-nephrines are less sensitive
to changesin sympathoadrenalactivity than arelev-
els of the parent amines, these metabo-lites are
neverthelessinfluenced by manyof the same stimuli and drugs that
in-fluence plasma catecholamines.25-28 Up-right posture and
emotional stress arewell-known to stimulate release of
cat-echolamines from sympathetic nervesand the adrenal medulla. To
minimizethe possibility of false-positive test re-sults, we
collected blood samples forplasma free metanephrines under thesame
conditions used for collection ofsamplesfor measurementsof plasma
cat-
echolamines. Blood samples weredrawnwith patients in the supine
position,through an in-dwelling intravenouscatheter, and after an
overnight fast.
Study Limitations
The major strength of this studyallpatientswere examined
becauseof clini-cal suspicion of pheochromocytomawas associated
with the limitation thatexclusion of pheochromocytomarequired use
of methods other than thebiochemicaltestsnormally used in
clini-
cal practice. Although computedtomog-raphy and magnetic
resonance imagingoffer high sensitivity for detecting adre-nal
tumors, sensitivity decreases
fordetectingextra-adrenaldisease.Wethere-fore followed up patients
for an averageof2.5yearsto furtherexclude pheochro-mocytoma in
patients with negativeimaging. Only 1 patient in whom pheo-
DIAGNOSIS OF PHEOCHROMOCYTOMA
2002 American Medical Association. All rights reserved.
(Reprinted) JAMA, March 20, 2002Vol 287, No. 11 1433
-
8/2/2019 Biochemical Diagnosis of Pheochromocytoma- Which Test
is Best.full
8/8
chromocytoma wasinitially excludedbyimaging
studieswassubsequentlyfoundto have the disease at follow-up.
Itremains possible, however, that otherpatients in whom
pheochromocytomawasexcluded according to thecriteriaof
ourstudymayhavehadundiagnoseddis-ease. Even so andunless these
numberswere large, it is unlikely that incorrectcategorization of
these patients wouldmake asignificantdifferenceto theresultsand
conclusions of the study.
A related potential limitation of thestudy was the need to omit
from theanalyses 145 patients who did not meettheresearch
criteriaforexclusion or con-firmation of pheochromocytoma.
Sepa-rate analyses of howinclusion of thedatafrom these patients
would affecttestper-formance revealed little influence on the
results and conclusions of the study.Another potential
limitation of the
study involved the multicenter nature
ofpatientrecruitmentandsubsequent mea-surements of urinary analytes
by differ-entlaboratories compared with thesinglelaboratory used
for plasma free meta-nephrines.However,separate analysisofdata
derived from single laboratoriesre-vealed no obvious influences.
Thus,rather than a limitation, the multi-center nature of the study
is a strengthestablishing thatmany ofthefindings(eg,
low specificity of urinary fractionatedmetanephrines, low
sensitivity of uri-nary VMA) were independent of thelaboratory
where tests were run.
Conclusions
Plasmafreemetanephrines constitute thebest test for excluding or
confirmingpheochromocytoma and should be thetest of first choice
for diagnosis of thetu-mor. A negative test result virtually
ex-cludes pheochromocytoma.In such pa-tients, representing more
than 80% of
those tested, no immediate further testsfor the tumor are
necessary. Further-more, in about 80% of patients
withpheochromocytoma, the magnitude ofincrease in
plasmafreemetanephrinesisso large that the tumor can be con-firmed
with close to 100% probability.In these patients, the immediate
task isto locate the tumor.
Author Contributions: Study concept and design:Lenders, Walther,
Friberg, Keiser, Eisenhofer.Acquisition of data: Lenders, Pacak,
Walther, Man-nelli, Friberg, Eisenhofer.Analysis and interpretation
of data: Lenders, Line-han, Goldstein, Eisenhofer.Drafting of the
manuscript: Lenders, Linehan, Gold-stein, Eisenhofer.Critical
revision of the manuscript for important in-
tellectual content: Lenders, Pacak, Walther, Man-nelli, Friberg,
Keiser, Goldstein, Eisenhofer.Statistical expertise:
Goldstein.Administrative, technical, or material support: Wal-ther,
Friberg, Keiser, Goldstein, Eisenhofer.Study supervision: Lenders,
Walther, Linehan, Gold-stein.Acknowledgment: We are grateful to
CourtneyHolmes, BS, Patricia Sullivan, BS, and Jacques J.
Wil-lemsen, BS, for expert technical assistance, to DonnaPeterson,
RN, BS, and Svisse Haegelind, BS, for datamanagement, to William M.
Manger, MD, PhD, forhelpful advice, toRaymondR. Townsend, MD,for
as-sistance with patients, and to the many other clini-cians
andtheirpatientswho participatedin thestudy.
REFERENCES
1. Bravo EL. Evolving concepts in the pathophysiol-
ogy, diagnosis, and treatment of pheochromocy-toma. Endocr Rev.
1994;15:356-368.2. Manger WM, Gifford RW Jr. Pheochromocy-toma:
current diagnosis and management. Cleve ClinJ Med.
1993;60:365-378.3. Mannelli M. Diagnosticproblems in
pheochromo-cytoma. J Endocrinol Invest. 1989;12:739-757.4. Bravo
EL,Tarazi RC, GiffordRW, Stewart BH.Cir-culating and urinary
catecholamines in pheochromo-cytoma. N Engl J Med.
1979;301:682-686.5. Duncan MW, Compton P, Lazarus L, Smythe GA.M e
a s u r e m e n t o f n o r e p i n e p h r i n e a n d 3 , 4
-dihydroxyphenylglycol in urineand plasma for the di-agnosis of
pheochromocytoma. N Engl J Med. 1988;319:136-142.6. Young
MJ,Dmuchowski C, Wallis JW, BarnasGP,Shapiro B. Biochemical tests
for pheochromocytoma:strategiesin hypertensive patients.J Gen
Intern Med.1989;4:273-276.
7. Peaston RT, Lai LC. Biochemical detectionof
phae-chromocytoma. J Clin Pathol. 1993;46:734-737.8. Gerlo EA,
Sevens C. Urinary and plasma catechol-amines and urinary
catecholamine metabolites in pheo-chromocytoma. Clin Chem.
1994;40:250-256.9. Lenders JW,KeiserHR, GoldsteinDS, et
al.Plasmametanephrines in the diagnosis of pheochromocy-toma. Ann
Intern Med. 1995;123:101-109.10. HeronE, Chatellier G, Billaud E,
Foos E, PlouinPF.The urinary metanephrine-to-creatinine ratio for
thediagnosis of pheochromocytoma. Ann Intern
Med.1996;125:300-303.11. Eisenhofer G, Lenders JW, Linehan WM,
Wal-ther MM, Goldstein DS, Keiser HR. Plasma normeta-nephrine and
metanephrine for detecting pheochro-mocytoma in von Hippel-Lindau
disease and multipleendocrine neoplasia type 2. N EnglJ Med.
1999;340:1872-1879.12. MannelliM, Ianni L, Cilotti A, Conti A.
Pheochro-
mocytoma in Italy:a multicentric retrospective study.Eur J
Endocrinol. 1999;141:619-624.13. Witteles RM, Kaplan EL, Roizen MF.
Sensitivityof diagnostic and localization tests for
pheochromo-cytoma in clinical practice. Arch Intern Med.
2000;160:2521-2524.14. Raber W, Raffesberg W, Bischof M, et al.
Diag-nostic efficacy of unconjugated plasma metaneph-rines for the
detection of pheochromocytoma. ArchIntern Med.
2000;160:2957-2963.15. Hernandez FC,Sanchez M, AlvarezA, et al.A
five-year report on experience in the detection of pheo-
chromocytoma. Clin Biochem. 2001;33:649-655.16. Gardet V, Gatta
B, Simonnet G, et al.Lessons froman unpleasant surprise. J
Hypertens. 2001;19:1029-1035.17. Eisenhofer G, Goldstein DS, Stull
R, et al. Simul-taneousliquid-chromatographic determination of
3,4-dihydroxyphenylglycol, catecholamines, and
3,4-dihydroxyphenylalanine in plasma,and their responsesto
inhibition of monoamine oxidase.Clin Chem.1986;
32:2030-2033.18. van der Hoorn FAJ, Boomsma F, Man int VeldAJ,
Schalekamp MADH. Determination of catechol-amines in human plasma
by high-performance liquidchromatography. J Chromatogr.
1989;487:17-28.19. Lenders JWM, Eisenhofer G, Armando I, KeiserHR,
Goldstein DS, Kopin IJ. Determination of plasmametanephrines by
liquid chromatography with elec-trochemical detection. Clin Chem.
1993;39:97-103.20. Pisano JJ. A simple analysis of
normetanephrineand metanephrine in urine. Clin Chim Acta.
1960;5:406-414.21. PisanoJJ, Crout R, Abraham D. Determination
of3-methoxy-4-hydroxymandelicacid in urine. ClinChimActa.
1962;7:285-289.22. Moyer TP,Jiang NS,Tyce GM,ShepsSG. Analy-sis for
urinary catecholamines by liquid chromatog-raphy with amperometric
detection. Clin Chem.1979;25:256-263.
23. Beck JR, Shultz EK. The use of relative
operatingcharacteristic (ROC)curvesin testperformanceevalu-ation.
Arch Pathol Lab Med. 1986;110:13-20.24. Hanley JA, McNeil BJ. A
method of comparing theareasunder receiver operating
characteristiccurves de-rivedfrom thesamecases. Radiology.
1983;148:839-843.25. Eisenhofer G, Friberg P, Pacak K, et al.
Plasmametadrenalines. Clin Sci (Colch). 1995;88:533-542.26.
Eisenhofer G, Rundqvist B, Aneman A, et al. Re-gional release and
removal of catecholaminesand ex-traneuronal metabolism to
metanephrines.J Clin En-docrinol Metab. 1995;80:3009-3017.27.
EisenhoferG, Keiser H, FribergP, et al.Plasmameta-nephrines are
markers of pheochromocytoma pro-duced by
catechol-O-methyltransferase within tu-mors. J Clin Endocrinol
Metab. 1998;83:2175-2185.28. Eisenhofer G, Huynh T-T, Hiroi M,
Pacak K. Un-derstanding catecholamine metabolism as a guide to
the biochemical diagnosisof pheochromocytoma. RevEndocrinol
Metab Dis. 2001;2:297-311.29. Eisenhofer G, Aneman A, Hooper D,
RundqvistB, FribergP. Mesentericorganproduction,
hepaticme-tabolism,and renal eliminationof norepinephrine andits
metabolites in humans. J Neurochem. 1996;66:1565-1573.30.
Eisenhofer G. Free or total metanephrines for di-agnosis of
pheochromocytoma: what is the differ-ence? Clin Chem.
2001;47:988-989.31. Walther MM,Reiter R, KeiserHR, et
al.Clinicalandgenetic characterization of pheochromocytoma in
vonHippel-Lindau families. J Urol. 1999;162:659-664.32. Pauker SG,
Kopelman RI. Interpreting hoof-beats. N Engl J Med.
1992;327:1009-1013.33. Bravo EL, Tarazi RC, Fouad FM, Vidt DG,
Gif-fordRW Jr. Clonidine-suppression test. N EnglJ
Med.1981;305:623-626.34. GrossmanE, Goldstein DS, HoffmanA, Keiser
HR.
Glucagon and clonidine testing in the diagnosis
ofpheochromocytoma. Hypertension. 1991;17:733-741.35. PacakK,
Linehan WM,EisenhoferG, Walther MM,Goldstein DS. Recent advances in
genetics, diagno-sis, localization, and treatment of
pheochromocy-toma. Ann Intern Med. 2001;134:315-329.36. Goldstein
DS, Stull R, Markey SP, Marks ES, Kei-ser HR. Dihydrocaffeic acid:
a common contaminantin the liquid chromatographic-electrochemical
mea-surement of plasma catecholamines in man. J Chro-matogr.
1984;311:148-153.
DIAGNOSIS OF PHEOCHROMOCYTOMA
1434 JAMA, March 20, 2002Vol 287, No. 11 (Reprinted) 2002
American Medical Association. All rights reserved.