Embed Size (px)
Citation preview

Review Article
From the Virginia Commonwealth
University School of Nursing,
Richmond, Virginia.
Address correspondence to
Mamoona Arif-Rahu, RN, PhD,
CCRN, VCU Medical Center, 1250 E.
Marshall Street, Box 985825,
Richmond, VA 23298. E-mail:
Received November 30, 2009;
Revised October 26, 2010;
Accepted October 26, 2010.
1524-9042/$36.00
� 2012 by the American Society for
Pain Management Nursing
doi:10.1016/j.pmn.2010.10.036
Biobehavioral Measuresfor Pain in the PediatricPatient
--- Mamoona Arif-Rahu, RN, PhD, CCRN,
Deborah Fisher, RN, MS, CS, CPON,
and Yui Matsuda, RN, BSN
- ABSTRACT:Pain is a complex biobehavioral phenomenon. The quantification of
pain involves the incorporation of many factors, including physio-
logic, behavioral, and psychologic factors. Recognition of pain relies
heavily on the expression of the patient as well as the interpretation of
the caregiver. There aremany studies published on biobehavioral pain
assessment tools, such as neuroimaging, neuromuscular, biomarker,
and behavioral pain assessment scales. These tools present a clinical
challenge to appropriately assess and manage pain in the noncom-
municative pediatric patients, such as infants, preverbal toddlers, and
intubated and/or unconscious or cognitively impaired patients. Pain is
a combination of physiologic, behavioral, and psychologic interac-
tions. Any tool that incorporates themeasurement of only one of those
domains is inherently incomplete in the assessment of pain. There-
fore, the purpose of this literature review was to provide a compre-
hensive overview of these biobehavioral pain assessment tools used in
pain assessment in the noncommunicative pediatric population.
� 2012 by the American Society for Pain Management Nursing
Pain is a complex biobehavioral phenomenon still not fully understood by re-
searchers and clinicians alike. The goal of objectifying a highly subjective phe-nomenon in a noncommunicative pediatric population continues to perplex
many researchers. For the nonverbal population, the American Society for Pain
Management Nursing (ASPMN) recommends using multidimensional instru-
ments that are characterized by both behavioral and physiologic indicators of
pain (Herr, Coyne, Key, Manworren, McCaffery, Merkel, Pelosi-Kelly, & Wild,
2006). There are several studies that have addressed the need for a pain assess-
ment tool that uses multimodal variables (Buttner & Finke, 2000; Gregg, 1998;
Labus, Keefe, & Jensen, 2003; Ramelet, Abu-Saad, Rees, & McDonald, 2004).The three approaches to pain assessment include cognitive (self-report),
behavioral (cry, posture, and facial expression), and physiologic (heart rate
variability, blood pressure fluctuations, decreases in oxygen saturation, and
metabolic and endocrine increases). Of all of these options, self-report is still
the gold standard in pain assessment. Unfortunately, when children cannot ex-
press themselves, self-report is not possible; further investigations and observa-
tions are needed for accurate pain assessment. Over the past 2 decades, there
have been an increasing number of studies published on biobehavioral
Pain Management Nursing, Vol 13, No 3 (September), 2012: pp 157-168

158 Arif-Rahu, Fisher, and Matsuda
assessment tools such as neuroimaging, neuromuscu-
lar, biomarker, and behavioral pain assessment scales.
ASSESSING PAIN IN PEDIATRICPATIENTS
Neuromuscular Activity of PainThe quantification of pain involves the incorporation
of many imprecise factors, so measurements tend tobe very subjective, relying heavily on the expression
of the patient as well as the interpretation of the care-
giver. An objective pain measurement tool would pro-
vide those in the clinical arena with a standardized
form of measurement that would not vary with patient
or caregiver. With this as a goal, various researchers
have evaluated the use of electroencephalography
(EEG), electromyography (EMG), and brain imagingtechniques as the basis for such objective measure-
ments of pain (Davis, Taylor, Crawley, Wood, &
Mikulis, 1997; Dowman, Rissacher, & Schuckers, 2008;
Henderson, Gandevia, & Macefield, 2008; Jancke,
Vogt, Musial, Lutz, & Theodor, 1996; Raux, Ray, Prella,
Duguet, Demoule, & Similowski, 2007).
EEG is readily available in thehospital setting for use
on a wide range of patients, which makes it a tool of in-terest in research applications. It provides a noninvasive
measurement of cortical brain activity. This activity can
be measured by application of electrodes to the scalp
and measurements taken at various band frequencies.
It has been shown that the somatosensory cortex, the an-
terior cingulate cortex, and the somatosensory associa-
tion areas located in the parietal operculum and insula
are activated by painful stimuli (Apkarian, Bushnell,Treede,&Zubieta, 2005). Dowman et al., (2008) studied
the pain-related cortical activity of the brain by using
EEG during tonic experimental pain stimulus and con-
trol conditions. They observed pain-related changes in
the EEG at specific electrode locations, such as the con-
tralateral central, frontocentral, and temporal scalp re-
gions. Their results indicated that pain-related changes
in the EEG showed a decrease in alpha over the contra-lateral temporal scalp (Newman–Keuls test: p < .05).
Raux et al., (2007) used EEG to demonstrate a pre-
motor cortical activation during a situation mimicking
one form of patient-ventilator asynchrony in noninva-
sive ventilated patients. The basis of the Raux et al.,
(2007) study was the underlying association between
specific brain regions and the control of breathing by
use of EEG. The results indicated that mean inspiratoryflow increased during ‘‘discomfort’’ compared with
the two ‘‘comfort’’ periods (p ¼ .0003). Furthermore,
the EEG results indicated that motor potentials were
significantly more frequent during ‘‘discomfort’’ than
during any of the ‘‘comfort’’ conditions (Fisher exact
test: p < .001) and thus are associated with an activa-
tion of the premotor cerebral cortex. Although EEG
may be a valid tool to measure brain activities associ-
ated with pain response, it requires trained technician
time to apply electrodes and translate results, therefore
making it impractical for clinical settings.
EMG has been widely used in the assessment ofpain in various regions of the body. EMG registers mus-
cle activity with surface electrodes. Several studies
have used EMG to study facial expressions by using in-
tensity of muscular response in patients suffering from
back pain, headache, and neck and shoulder pain
(Cram & Steger, 1983; Ong, Nicholoson, & Gramling,
2003; Sonnby-Borgstrom, 2002; Weyers, Muhlberger,
Hefele, & Pauli, 2006; Wolf, Raedler, Henke, Kiefer,Mass, Quante, & Wiedemann, 2005). Wolf et al.,
(2005) validated a facial EMG method for the measure-
ment of facial pain expression in ten healthy subjects
induced with a laser system pain stimulus. They stud-
ied nine muscle groups of the face. The results indi-
cated two groups of muscles corresponding to pain
expression. The first muscle group identified is assem-
bled around the orbicularis oculi muscle, which initi-ates staring. The second group consists of the
mentalis and depressor anguli oris muscles, both of
which trigger mouth movements. The investigators
recommended further studies with psychometric mea-
surements, a larger sample size, and a female test
group. Another study, by Jancke et al. (1996), exam-
ined the changes in facial EMG to auditory stimuli.
They found that when high-intensity stimuli were ad-ministered to subjects, a strong upper-face EMG re-
cording was observed. Similarly, in response to the
crying of a baby, muscle activity in the mouth region
increased.
So although EMG can be used to measure facial
muscular activity, which can be used as an indicator
of pain, EMG on its own should not be used as a direct
absolute measurement of pain, in either a research set-ting or a clinical setting. One of the main drawbacks in
the use of objective measurements such as EEG, EMG,
and other brain imaging techniques is that there is
a lack of research on the associated interpretation of
the emotional response of patients (Jancke et al.,
1996). In addition, intersubject reliability can be influ-
enced by lead placement, possibly leading to inconsis-
tent results.Although a myriad of brain imaging techniques ex-
ist, the main one used in the assessment of pain is mag-
netic resonance imaging (MRI). This is largely due to
the fact that MRI is noninvasive and has a combination
of high temporal and spatial resolution. A study done
by Henderson et al., (2008) demonstrated gender differ-
ences in functional MRI measurements made during

TABLE 1.
Chemical Biomarkers for Pain
Biomarker (receptor) Pathophysiologic Role Pharmacologic Modulation
b-Endorphin Produced by fetal pituitary gland.c
An opioid peptide produced by leukocytes and released inresponse to pain and/or stress; antinociceptive effect.cde
Opioidse
Interleukin (IL) 1b Proinflammatory cytokine.f
Stimulates secretion of opioid peptides from leukocytes.b
IL-4 Antiinflammatory cytokine produced by lymphocytes and mastcells.fg
Analgesic effect by inhibition of TNF-a, IL-8, and IL-1b.f
IL-8 (CXCR1) Proinflammatory cytokine involved in inflammatory,hypernociception and neuropathic pain; induces mechanicalhypernociception.f
Produced by macrophages.g
b-Adrenergic receptorantagonistsf
Metenkephalin Opioid peptide with antinociceptive effect as analgesicmediator.bd
Opioidsd
Serotonin (5HT) Acts as a stimulant for nociceptive nerve endings; found inplatelets and basophils.a
5-HT3 antagonistsa
Tumor necrosis factor(TNF) a (TNFR1)
Proinflammatory cytokine produced by macrophages; directsensitization of nociceptors.f
Present in neurons and glia; involved in inflammatory andneuropathic hyperalgesia.g
Indomethacin, infliximab,etanercept, adalimumab,thalidomide, and atenololf
References: aDegenhart et al., 2007; bMachelska, 2007; cMahieu-Caputo et al., 2002; dMousa et al., 2007; eRittner et al., 2008; fVerri et al., 2006; gZhang & An,
2007.
159Pediatric Biobehavioral Pain Measures
muscle and cutaneous pain, 2008. They examined
22 healthy adult subjects (11 men, 11 women; aged 19-
49 years). An increase change in signal intensity was
used as their form of measurement, and they observed
that there were gender-based differences in the hippo-
campus, cerebella cortex, midcingulate cortex, and dor-
solateral prefrontal cortex. Women showed increasedsignal intensity which occurred in the cingulate, insular,
primary somatosensory, secondary somatosensory, and
cerebellar cortices during both muscle and cutaneous
pain compared with men. Another study performed on
14 adult subjects (aged 14-40 years), by Owen, Bureau,
Thomas, Prato, and Lawrence (2008), used perfusion
MRI to examine pain-induced changes in cerebral blood
flow. The induced pain consisted of a thermal stimuluson the left hand. They found that this method was effec-
tive for the measurement of chronic pain and observed
changes in the insula, secondary somatosensory, and cin-
gulate cortexes. Functional MRI has great utility but has
limited applicability for real-time assessment of pain
owing to the time involved in making measurements as
well as the limitation that the machine itself poses to
the mobility of the patient.
Chemical Biomarkers of PainSeveral chemical biomarkers for pain have been impli-
cated in the literature (Table 1). Endogenous opioid
neuropeptides (enkephalins, endorphins, dynorphins)
have the ability to dampen the perception of pain
(Rittner, Brack, & Stein, 2008). These actions include
opiate-like activity that is involved in regulation of toler-
ance to pain within the central nervous system. b-Endor-phin is a neuropeptide producedby the pituitary starting
as early as 22 weeks’ gestation. It can be found in
amniotic fluid and fetal blood. Other substancesimplicated in the down-regulation of pain include epi-
nephrine, norepinephrine, serotonin, and g-aminobuty-
ric acid. Some chemical mediators dually implicated in
pain and inflammations include prostaglandins, hista-
mine, serotonin, cytokines, and chemokines (Abbadie,
2005). Chemokines function in activating or modi-
fiying nociceptive transmission. Increasing levels of
interleukin-8, one of the first chemokines studied, are as-sociated with increasing levels of hyperalgesia in rat
models (Cunha, 1991). Studies in humans have found
a positive relationship between spinal fluid levels of
interleukin-8 and back pain (Brisby, 2002). Further re-
search is warranted to delineate possible confounding
variables affecting the ultimate pain response.
b-Endorphins have been associated with pain and
stress response (Rittner et al., 2008). In addition, amni-otic fluid b-endorphin (AFBE) levels were studied as
a possible prognostic predictor of degree of intestinal
damage in fetuses with gastroschisis, which causes se-
vere pain response (Mahieu-Caputo et al., 2002). The
intent was to find a relationship between the level of

160 Arif-Rahu, Fisher, and Matsuda
b-endorphin and postnatal morbidity. Postnatal mor-
bidity was higher when AFBE exceeded 10 mg/L.That is, higher levels of AFBE were associated with
more severe cases of gastroschisis. Researchers believe
that the endorphin production is a result of prenatal
stress and/or pain from bowel injury (Mahieu-Caputo
et al., 2002). Limitations of this study include the rela-tively small sample size (13 infants with gastroschisis
versus 33 infants without gastroschisis). One must
weigh the limited benefit versus the risk of potentially
causing more fetal harm with repeated invasive studies
throughout the pregnancy. In summary, an increase in
b-endorphin may be associated with increased pain re-
sponse caused by injury, such as gastroschisis. Further
research is indicated to better delineate the optimalutility of testing amniotic fluid b-endorphin levels and
the impact on clinical outcomes after delivery.
A double-blind randomized trial compared the
analgesic effectiveness of continuous infusion opioid
versus intermittent bolus infusion of opioid in the
#36-month-old postsurgical population (n ¼ 204)
(Bouwmeester, Anand, van Dijk, Hop, Boomsma, &
Tibboel, 2001). Plasma concentrations of biologic var-iants (lactate, glucose, insulin, norepinephrine, and
epinephrine) known to be elevated in pain response
were measured at five time points (before surgery, at
end of surgery, and 6, 12, and 24 hours after surgery).
Presurgical levels of epinephrine were found to be
higher than postsurgical levels of epinephrine. Eleva-
tion in biologic variables (lactate, glucose, insulin, nor-
epinephrine, and epinephrine) was compared withpain assessment scales (visual analog scale and com-
fort). The two opioid treatment groups showed no sig-
nificant difference in pain response as measured by the
pain scales and the biologic variants. Further conclu-
sions included difference in surgical stress response
in neonates compared with older age groups. After sur-
gery, neonates showed higher glucose levels, lower
mean increases in epinephrine and norepinephrine,and higher insulin levels compared with older age
groups. Implications for further research include op-
portunities to compare and determine efficacy of other
analgesic interventions to assist in determining best
practice. Further study is warranted to examine the
variations in pain responses related to varying chrono-
logic age.
One deterrent to using biomarker levels as a unidi-mensional tool to assess pain is their concurrent rela-
tionship with inflammation and/or stress response.
Mousa, Straub, Schafer, and Stein (2007) found that
the amount of opioid receptors and endogenous opi-
oid agonists (b-endorphin and metenkephalin) corre-
lated with level of inflammation associated with
arthritis. Synovial fluid samples were subjected to
double immunohistochemical analysis of opioid pep-
tides with immune cell markers. The researchers found
that b-endorphin and metenkephalin were expressed
by macrophage-like cells within synovial lining layers.
Overall, b-endorphin and metenkephalin were more
prevalent in patients with rheumatoid arthritis than
in patients with osteoarthritis or joint trauma. Thisstudy further supports the relationship between in-
flammation and pain response.
The potential role of cytokine measurement in
pain assessment is limited by the potential difficulty
in collecting samples without causing serious harm
to the patient. Many of the cytokines are located within
the dorsal root ganglia or spinal cord or within the
tissues surrounding nerves and the site of injury(Zhang & An, 2007). The potential benefit of assessing
chemical biomarkers of pain appears to be in further-
ing our knowledge of the neurobiology of the pain re-
sponse. An understanding of the pathophysiologic
responses of the human body to painful stimuli may al-
low for the development of improved multidimen-
sional pain assessment tools.
Behavioral Measures of PainThe ASPMN guidelines (Herr et al., 2006) recommend
several clinical tools for use on ‘‘infants and preverbal
toddlers’’ and ‘‘pediatric intubated and/or unconscious
persons.’’ Table 2 presents these scales for the nonver-
bal behavioral assessment tools for pediatric patients.
Furthermore, the Pediatric Initiative on Methods, Mea-
surement, and Pain Assessment in Clinical Trials identi-
fied measures to use in pediatric pain clinical researchtrials (Cohen, Lemanek, Blount, Dahlquist, Lim,
Palermo, Mckenna, & Weiss, 2008). Those authors as-
sessed the validity of some clinical pain assessment
tools and suggested to select pain tools according to
the purpose and context of the setting.
The three approaches to measure pain include
self-report, behavioral, and physiologic. Self-report is
considered to be the gold standard of pain assessment(Schiavenato & Craig, 2010). In one study comparing
nurses’ pain ratings using the Face, Legs, Activity, Cry,
and Consolability (FLACC) scale (Merkel, Shayevitz,
Voepeol-Lewis, Malviya, 1997) with those of patients’
pain rating using the Wong-Baker FACES scale, no cor-
relation between the two scales (r ¼ 0.254; p ¼ .381)
were found in patients <5 years old (Willis, Merkel,
Voepel-Lewis, & Malviya, 2003). However, there wasa significant and positive correlation in children 5-7
years old (r ¼ 0.830; p ¼ .0001) demonstrating that
self-report should be used to validate pain if the target
population is developmentally capable of rating its
own pain (Willis et al., 2003).

TABLE 2.
Pediatric Behavioral Pain Scales
PainAssessment
Tool ContentAge
GroupDescriptionof Study
ScoringMeasures
No. ofSubjects Country Validity Reliability
FLACCMerkel,Shayevitsz,Voepel-Lewis,& Malviya(1997)
B 2 mo to 7 y Observed painafter varioussurgicalprocedures inPACU
5 behavioralitems: F, face;L, legs; A,activity; C,cry; C,consolability;each equallyweighted from0 to 2, score0-10
89: 30 IR, 29analgesiceffect, 30concurrentvalidity
USA Concurrentvalidity: r ¼ .80;p < .001(against OPS);constructvalidity:‘‘significantly’’higher atpreanalgesiathan at 10, 30,and 60 min(p < .001)
IR: kappa: range0.52-0.82(measuredeachassessmentcategoryseparately)
COMFORTAmbuel, Hamlett,Marx, & Blumer(1992)
B & P Infants(newbornto 204 mo)
Assessed level ofdistress onventilatedchildren inPICU
6 behavioralmeasures:alertness,calmness,muscle tone,movement,facialexpression,respiratoryresponse; 2physiologiccomponents:HR, MAP; 1-5points for each,score 8-40
37 USA Concurrentvalidity0.26-0.90,overall 0.75(against VAS)
IR: r 84, range0.51-0.93(kappa); IC:
Cronbach a 0.90
COMFORTVan Dijk et al.(2001)
B & P 0-3 y Assessed painafter majorabdomen orthoracicsurgery inPSICU
6 behavioralmeasures and 4physiologiccomponents:HR, MAP, HRV,MAPV; score8-40
204 Netherland CorrelationbetweenCOMFORT‘‘behavioral’’and 4physiologicitems: 0.44,0.48, 0.37, 0.49
Not tested
(Continued )
161
Pediatric
BiobehavioralPain
Measures
s

TABLE 2.Continued
PainAssessment
Tool ContentAge
GroupDescriptionof Study
ScoringMeasures
No. ofSubjects Country Validity Reliability
DSVNIDistress Scale forVentilatedNewbornInfants (original)
Sparshott (1996)
B & P Newborninfants
Assessedreaction topain/distresson ventilatedchildren
3 behavioralitems: facialexpression(0-3), bodymovement (0-3), color (0-2);4 physiologicchanges: HR,blood pressure,oxygenation,temperaturedifferential;behavioralscore 0-8, noscoring onphysiologic
N/A UK Assessmentcategoriesselected fromliterature review
Not tested
CRIESCrying, RequiresIncreasedOxygenAdministration,Increased VitalSigns,Expression,Sleeplessness(original)
Krechel & Bildner(1995)
B & P Neonates Assessed pain 3 behavioral and2 physiologicmeasures: C,crying; R,requiresincreasedoxygenadministration;I, increasedvital signs; E,expression; S,sleeplessness;score 0-10
24 USA Concurrentvalidity 0.72(against VAS)
IR 0.72
CHIPPSChildren’s andInfants’PostoperativePain Scale(original)
Buttner & Finke(2000)
B Newbornto 1.5 y
Assessed pain inthe firstpostoperativehours
5 behavioralmeasures:crying, facialexpression,posture of thetrunk, postureof the legs,motorrestlessness
584 Germany Sensitivity 97%,specificity 86%
IR 0.93; IC:Cronbach a:0.92 toddler,0.96 infants
B¼ behavioral; HR¼ heart rate; HRV¼ heart rhythm variability; IC¼ internal consistency; IR¼ interrater reliability; MAP¼mean arterial pressure; MAPV¼mean arterial pressure variability; OPS¼ objective pain
scale; P ¼ physiologic; PACU ¼ postanesthesia care unit; PICU ¼ pediatric intensive care unit; PSICU ¼ pediatric surgery intensive care unit; VAS ¼ visual analog scale.
162
Arif-R
ahu,Fish
er,andMatsu
da

TABLE 3.
Facial Expression Correlated with Pain by Using Facial Action Coding Systems
Description
Action Unit Facial Action Coding System Child Facial Coding System Neonate Facial Coding System
1 Inner brow raise Brow lower Brow bulge2 Outer brow raise Squint Eye squeeze4 Brow lower Eye squeeze Nasolabial furrow deepen5 Upper lid raise Nose wrinkle Open mouth6 Cheek raiser Nasolabial furrow Vertical stretch mouth7 Lid tightener Cheek raise Horizontal stretch mouth10 Upper lip raiser Upper lip raise Chin quiver12 Lip corner puller Lip corner pull Taut tongue17 Chin raiser Vertical mouth stretch Tongue protrusion18 Lip pucker Horizontal mouth stretch20 Lip stretch Blink23 Lip tightener Flared nostril24 Lip presser Open lips25 Lip part26 Jaw drop28 Lips suck45 Blink43 Eyes closed
163Pediatric Biobehavioral Pain Measures
Unfortunately, pain assessment is difficult in nonver-bal pediatricpatients such asneonates, infants, preverbal
toddlers, and intubated and/or unconscious cognitively
impaired patients. Nonverbal pediatric patients are un-
able to communicate pain or discomfort, because of lan-
guage, cognitive, developmental, or physiologic issues
(Breau, Camfield, McGrath, & Finley, 2004; Cohen
et al., 2008; Herr et al., 2006; Johnston, 1993; McGrath,
Rosmus, Camfield, Campbell, & Hennigar, 1998). Inthese contexts, observational methods that focus on
nonverbal behavior, including indices of facial, vocal,
and motor behaviors and physiologic measures, have
been identified.
Facial ExpressionsFacial expression is considered to be a more stable and
valid component for assessing acute and short-termpain (Breau, McGrath, Craig, Santor, Cassidy, & Reid,
2001; Craig, Hadjistavropoulos, Grunau, & Whitfield,
1994; Grunau & Craig, 1987). There are a number of
behavioral assessment tools developed to capture
facial expression (Table 3). The Facial Action Coding
System (FACS), developed by Ekman and Friesen
(1978), identifies facial expressions specific to pain
that have shown evidence for validity and reliability inadults and children (Craig, 1998; Craig et al., 1994;
Craig & Patrick, 1985; Oberlander, Gilbert, Chambers,
O’Donnell, & Craig, 1999). The FACS describes 44
specific facial muscle movements or action units
(AUs). The facial action units are typically identified
through the use of slow-motion stop-frame feedbackvideo to determine the presence and absence of
discrete facial actions. In a study by Larochette,
Chambers, and Craig (2006), the investigators used
the FACS to identify genuine, suppressed, and faked
facial expressions of pain in 50 healthy 8–12-year-old
children. They identified 18 AUs related to pain re-
sponse (Table 3). The interrater reliabilities for overall
frequency and intensity of AUs were 0.95 and 0.79, re-spectively. The results indicated that more frequent
and more intense lip corner puller (AU12), cheek raiser
(AU6), and lid tightened (AU7)were displayedwhen ex-
posed to cold water as a pain stimulus.
The Neonatal Facial Coding System (NFCS) devel-
oped by Grunau and Craig (1987) identifies specific
pain facial actions among newborns undergoing heel
lance procedures. Like the FACS, the NFCS assesses dis-crete facial actions using video played back in real time
with stop-frame capability. An expert coder identified
total facial activity and cluster-specific facial features
(brow bulge, eye squeeze, nasolabial furrow, and
open mouth) that have been shown to be significantly
associated with acute and postoperative pain in
infants (Craig, 1998; Craig, Whitfield, Grunau, Linton,
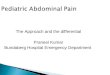
Hadjistavropoulos, 1993; Grunau and Craig, 1990).Figure 1 illustrates some of the common facial actions
corresponding to pain in infants.
Guinsburg, de Ara�ujo Peres, Branco de Almeida,
de C�assia Xavier Balda, C�assia Berenguel, Tonelotto,
and Kopelman (2000) used two pain assessment

FIGURE 1. - Facial expression correlated with pain using the Neonatal Facial Coding System.
164 Arif-Rahu, Fisher, and Matsuda
methods, the NFCS and the Neonatal Infant Pain Scale
(NIPS) (Lawrence, Alcock, McGrath, Kay, MacMurray,
& Dulberg, 1993). They coded distinct facial activities
that measure pain using NFCS, including presence orabsence of eight facial movements: brow bulge, eye
squeeze, nasolabial furrow deepened, open lips,
mouth stretch, lips pursed, taut tongue, and chin
quiver (1 point for each with a total score of 0-8
points). In addition, they used the NIPS, which is com-
posed of facial expression (0/1 point), cry (0/1/2
points), breathing pattern (0/1 point), position of
arms (0/1 point), position of legs (0/1 point), and stateof arousal (0/1 point). The interrater reliability was es-
tablished between two observers who scored the
NFCS and the NIPS using the number of actions agreed
upon by both observers divided by the number of ac-
tions scored by the two observers. The results indi-
cated interobserver reliability of k ¼ 0.94 for NFCS
and k ¼ 0.93 for NIPS. Furthermore, there was strong
agreement between the two coders for the vast major-ity of NFCS and NIPS items.
Similarly, the Child Facial Coding System (CFCS)
(Chambers, Cassidy, McGrath, Gilbert, & Craig, 1996)
was developed to assess acute pain responses in young
children aged 1-6 years. The CFCS codes 13 discrete
AUs adapted from both the FACS and the NFCS. Be-
cause there are less age-related differences in facial ac-
tivity beyond 1 year of age, CFCS has been used inadolescents to identify pain expressions (Lilley, Craig,
& Grunau, 1997). Breau et al., (2001) studied 123 chil-
dren aged 4-5 years undergoing routine diphtheria, per-
tussis, tetanus, and polio (DPT) immunization. The
purpose of the study was to establish sensitivity of
the CFCS during noxious stimuli. For the study, the
DPT immunization injection was the noxious stimulus.
They identified 13 facial actions, of which six reflected
the children’s acute pain experience. The results indi-cated that AU frequency and intensity for brow lower,
squint, flared nostril, nose wrinkle, lip corner pull, and
vertical mouth stretch occurred more often during im-
munization injection (the needle phase) than before
the injection (preneedle phase; p < .004 [frequency]
and p < .005 [intensity]).
Overall, these FACSs provide a comprehensive de-
scription of the facial expression during painful stimuliwhich could be used to develop better behavioral assess-
ment tools. One major limitation for use of the FACS in
the clinical setting is the extensive training and complex-
ityof coding that is required.Nonetheless, once the facial
expressions are narrowed down, FACS coding could be
used to assess facial expression during pain responses re-
lated to varying pediatric populations.
VocalThere have been cry features that have been exten-
sively studied using spectrographic devices. Short la-
tency to onset of cry, longer duration of the first cry
cycle, higher fundamental frequency, and greater in-
tensity in the upper ranges are pain-specific cry
features in infants and neonates during painful proce-
dures (Grunau, Johnston, & Craig, 1990; Johnsonton& Strada, 1986; Krechel & Bildner, 1995).
In a study by Runefors, Arnbj€ornsson, Elander, andMichelsson (2000), the researchers hypothesized that
a newborn infant’s cry can be used in conjunction
with an instrument to measure pain. They used heel

165Pediatric Biobehavioral Pain Measures
sticks as noxious stimuli to elicit pain response for phe-
nylketonuria screening in 50 healthy newborn infants.
Their cries of pain were recorded and analyzed acous-
tically with the assistance of a computer program espe-
cially designed for this purpose (Innomess Elektronik,
Berlin, Germany). The sound spectrogram, a well
tested instrument, is a visual diagram of the soundsignal. Time is recorded on the horizontal scale; fre-
quency is recorded on the vertical. The curve of
the lowest harmonic on the spectrogram gives the
fundamental frequency, and the upper lines give the
harmonic overtone multiples of the fundamental
frequency. The analysis showed that the crying sound
after the painful stimulus of the heel prick had a signi-
ficantly higher fundamental frequency and lasted lon-ger at the first cry (2.7 seconds) than at the fifth cry
(0.8 seconds; p < .001). The results indicated that
the first cry was more like a cry of pain, and the fifth
cry more resembled crying for reasons other than
pain. They suggested that newborn infants react to
pain in a recognizable way. However, they also sug-
gested that other stimuli may cause a similar reaction.
The researchers recommended that crying can be usedto measure pain in newborn infants only when the
cause of crying is known. A significant clinical practice
limitation of cry analyses is the need for a specialized
spectrographic apparatus that requires advanced train-
ing. The expense of the training and the apparatus con-
tributes to increased research costs. In addition, not all
infants will cry when in pain, such as patients with en-
dotracheal intubation or physiologic fatigue (Grunauet al., 1990; Johnston & Strada, 1986; van Dijk, Koot,
Abu Saad, Tibboel, & Passchier 2002).
Motor BehaviorsBody movement as a pain indicator focuses on observa-
tion of arm and leg activity. Body movement is included
in many pain assessment tools, but this behavioral
marker changes with development from the neonatal
stage through infancy and into adolescence. Increasedactivity, posture, and tense muscle tone are thought to
indicate more pain in neonates (Hummel & van Dijk,
2006). Muscle tone and breathing pattern take an inter-
mediate position between behavioral and physiologic
indicators (van Dijk et al., 2002). Muscle tone or pos-
ture may reflect tenseness due to abdominal pain but
may also reflect the behavior of a frightened child. Shal-
low and rapid breathing may reflect hyperventilationdue to anxiety or may be caused by pain after thoracic
or abdominal surgery (van Dijk et al., 2002). A major
limitation of assessing body movement is that children
may avoid moving because of pain (van Dijk et al.,
2002); therefore, special attention needs to be paid
to increased or decreased activity from a child’s
baseline.
Physiologic MeasuresPhysiologic measures of pain, which include heart rate,
respiratory rate, oxygen saturation, and blood pres-
sure, have been examined in neonates during acute
pain caused by heel lance (Johnston, Stevens, Yang,
& Horton, 1995) and circumcision (Howard, Howard,& Weitzman, 1994). The benefit of physiologic mea-
sures for pain assessment has been described by
Sweet and McGrath (1998) but it has been debated be-
cause of lack of specificity for pain (van Dijk, de Boer,
Koot, Duivenvoorden, Passchier, Bouwmeester, &
Tibboel, 2001). Fluctuations in heart rate, blood pres-
sure, and oxygen saturation may be influenced by
poor circulation due to blood loss, fluid intake, bodytemperature, and medical interventions. Several stud-
ies have concluded that physiologic pain indicators
are not ideal to assess pain and recommend that the
pain assessment tools be based on behavioral pain indi-
cators (Buchholz, Karl, Pomietto, & Lynn, 1998;
Buttner & Finke, 2000; McGrath & Unruh, 1994).
In a study by van Dijk et al. (2001), the researchers
examined the association between physiologic and be-havioral pain measures using the COMFORT scale in
children. The COMFORT scale consists of both behav-
ioral and physiologic components. The behavioral
components are described further in Table 2. Physio-
logic measures included mean arterial pressure, heart
rate, heart rate variability, and mean arterial pressure
variability. The researchers studied 204 subjects and
found that as children between 0 and 3 years old in-crease in age, their respiratory and heart rates decrease
and their overall blood pressure increases in response
to postoperative pain. That study also found moderate
correlations between crying and heart rate as well as
between facial expressions and heart rate variability
in nonverbal children. A low correlation between the
physiologic measures made during the study seems
to indicate that the measurements were independentof each other. Intermittent noninvasive measuring of
heart rate and blood pressure could induce distress
or anger in infants and children, which would increase
the unreliability of such pain indicators (van Dijk,
2001).
In summary, the means for validating the pain as-
sessment tools are provided in Table 2. Although all
of the tools have behavioral components, the Crying,Requires Oxygen, Increased Vital Signs, Expression,
and Sleep (CRIES) scale (Krechel & Bildner, 1995)
and the COMFORT scale are the only ones that contain
both physiologic and behavioral measures of pain. The
correlations of the physiologic measures are lower on

166 Arif-Rahu, Fisher, and Matsuda
the studies that tested with the COMFORT scale
(Ambuel, Hamlett, Marx, & Blumer, 1992; van Dijk,
de Boer, Koot, Tibboel, Passchier, & Duivenvoordent,
2000). Ambuel et al., (1992) pointed out that heart
rate and arterial blood pressure had the lowest inter-
rater reliabilities due to the way they were measured.
The researchers predict that the inter-rater reliabilitywould increase if the physiological measures are ob-
served for two minutes and the trend is measured
(Ambuel et al., 1992). In addition, van Dijk et al.
(2000) pointed out the limited validity of heart rate
and mean arterial pressure as a measurements of pain
and suggested the need for further research with clin-
ical data to support these measures, because they are
frequently used as indicators of pain in clinical settings.However, from a research perspective, the physiologic
measures may or may not be appropriate depending on
the specific pediatric population.
CONCLUSIONS
Assessment of pain in the noncommunicative pediatric
population provides many challenges for health careproviders and researchers. Results of the present liter-
ature review indicate many avenues for future studies,
including validation in the pediatric population. Clini-
cal implications of the use of objective markers for
pain measurement in the noncommunicative pediatric
patient may include improved individualized titration
of analgesia, decreased physiologic stress response
from inadequate analgesia, and avoidance of chronic
pain conditions secondary to inadequate management
of acute pain. Further research on pain assessment isneeded in the pediatric population by using a variety
of markers for pain. Additional studies of interest in-
clude comparison of chemical and mechanical bio-
markers for pain with validated behavioral markers
for pain in the pediatric population. One such study
may measure the correlation between EEG, serum
b-endorphin, and the FLACC behavioral pain assess-
ment tool during painful stimulus. Implications for fur-ther research include opportunities to improve validity
and reliability of these pain assessment tools by using
advanced methods such as analyses of facial expres-
sion, spectrographic devices, neuromuscular activity,
or chemical markers.
Acknowledgments
The authors thank Cindy Munro, RN, PhD, Professor, Depart-
ment of Adult Health, Virginia Commonwealth University
School of Nursing, for her insightful comments in this litera-
ture review.
REFERENCES
Abbadie, C. (2005). Chemokines, chemokine recep-tors, and pain. Trends in Immunology, 26(10),529–534.
Ambuel, B., Hamlett, K. W., Marx, C. M., & Blumer, J. L.(1992). Assessing distress in pediatric intensive care envi-ronments: The COMFORT scale. Journal of Pediatric Psy-chology, 17(1), 95–109.
Apkarian, A. V., Bushnell, M. C., Treede, R., & Zubieta, J.(2005). Human brain mechanisms of pain perception andregulation in health and disease. European Journal of Pain,
9, 463–484.Breau, L. M., Camfield, C., McGrath, P. J., Rosmus, C., &
Finley, G. A. (2004). Measuring pain accurately in childrenwith cognitive impairments: Refinement of a caregiver scale.Journal of Pediatrics, 138(5), 721–727.
Breau, L. M., McGrath, P. J., Craig, K. D., Santor, D.,Cassidy, K. L., & Reid, G. J. (2001). Facial expression ofchildren receiving immunizations: A principal componentsAnalysis of the Child Facial Coding System. The ClinicalJournal of Pain, 17, 178–186.
Bouwmeester, N. J., Anand, K. J. S., van Dijk, M.,Hop, W. C. J., Boomsma, F., & Tibboel, D. (2001). Hormonaland metabolic stress responses after major surgery in chil-dren aged 0-3 years: A double-blind, randomized trial com-paring the effects of continuous versus intermittentmorphine. British Journal of Anaesthesia, 87(3),390–399.
Brisby, H. (2002). Proinflammatory cytokines in ce-rebrospinal fluid and serum in patients with disc her-
niation and sciatica. European Spine Journal, 11,62–66.Buchholz, M., Karl, H. W., Pomietto, M., & Lynn, A. (1998).
Pain scores in infants: A modified infant pain scale versusvisual analogue. Journal of Pain Symptom Management,
15, 117–124.Buttner, W., & Finke, W. (2000). Analysis of behavioural
and physiological parameters for the assessment ofpostoperative analgesic demand in newborns, infantsand young children: A comprehensive report onseven consecutive studies. Pediatric Anaesthesia, 10,303–318.Chambers, C. T., Cassidy, K. L., McGrath, P. J.,
Gilbert, C. A., & Craig, K. D. (1996). The Child Facial Coding
System manual. Nova Scotia and Vancouver: DalhousieUniversity and University of British Columbia.Cohen, L. L., Lemanek, K., Blount, R. L., Dahlquist, L. M.,
Lim, C. S., Palermo, T. M., Mckenna, K. D., & Weiss, K. E.(2008). Evidence-based assessment of pediatric pain. Jour-nal of Pediatric Psychology, 33(9), 939–955.Craig, K. D. (1998). The facial display of pain. In
G. A. Finley, & P. J. McGrath (Eds.), Measurement of pain in
infants and children. Progress in pain research and man-
agement (pp. 103–122). Seattle: IASP Press.Craig, K. D., & Patrick, C. J. (1985). Facial expression
during induced pain. Journal of Personality & Social
Psychology, 48(4), 1080–1091.Craig, K. D., Whitfield, M. F., Grunau, R. V. E., Linton, J., &
Hadjistavropoulos, H. D. (1993). Pain in the preterm

167Pediatric Biobehavioral Pain Measures
neonate: Behavioural and physiological indices. Pain, 52(3),287–299.
Craig, K. D., Hadjistavropoulos, H. D., Grunau, R. V. E., &Whitfield, M. F. (1994). A comparison of two measures offacial activity during pain in the newborn child. Journal ofPediatric Psychology, 19, 305–318.
Cram, J. R., & Steger, J. C. (1983). EMG scanning in thediagnosis of chronic pain. Biofeedback and Self-Regulation,
8, 229–241.Cunha, F. Q. (1991). Interleukin-8 as a mediator of
sympathetic pain. British Journal of Pharmacology, 104,765–767.
Davis, K. D., Taylor, S. J., Crawley, A. P., Wood, M. L., &Mikulis, D. J. (1997). Functional MRI of pain and attention-related activations in the human cingulate cortex. Journal ofNeurophsiology, 77, 3370–3380.
Degenhardt, B. F., Darmani, N. A., Johnson, J. C.,Towns, L. C., Rhodes, D. C. J., Trinh, C., McClanahan, B., &DiMarzo, V. (2007). Role of osteopathic manipulativetreatment in altering pain biomarkers: A pilot study. TheJournal of the American Osteopathic Association, 107(9),387–400.
Dowman, R., Rissacher, D., & Schuckers, S. (2008).EEG indices of tonic pain-related activity in the somato-sensory cortices. Clinical Neurophysiology, 119, 1201–1212.
Ekman, P., & Friesen, W. V. (1978). Investigator’s guide tothe Facial Action Coding System. Palo Alto, CA: ConsultingPsychologists Press.
Gregg, T. L. (1998). Pediatric pain management in anadult critical care unit. Critical Care Nurse Quarterly, 21(2),42–54.
Grunau, R. V. E., & Craig, K. D. (1987). Pain expression inneonates: Facial action and cry. Pain, 28, 395–410.
Grunau, R. V. E., & Craig, K. D. (1990). Facial activity asa measure of neonatal pain expression. In D. C. Tyler, &E. J. Krane (Eds.), Advances in pain research and therapy
(pp. 147–155). New York: Raven Press.Grunau, R. V. E., Johnston, C. C., & Craig, K. D. (1990).
Neonatal facial and cry responses to invasive and noninva-sive procedures. Pain, 42(3), 295–305.
Guinsburg, R., de Ara�ujo Peres, C., Branco deAlmeida, M. F., de C�assia Xavier Balda, R., C�assiaBerenguel, R., Tonelotto, J., & Kopelman, B. I. (2000). Dif-ferences in pain expression between male and female new-born infants. Pain, 85(1-2), 127–133.
Henderson, L. A., Gandevia, S. C., & Macefield, V. G.(2008). Gender differences in brain activity evoked by mus-cle and cutaneous pain: A retrospective study of single-trialfMRI data. NeuroImage, 39, 1867–1876.
Herr, K., Coyne, P. J., Key, T., Manworren, R.,McCaffery, M., Merkel, S., Pelosi-Kelly, J., & Wild, L. (2006).Pain assessment in the nonverbal patient: Position statementwith clinical practice recommendations. Pain Management
Nursing, 7(2), 44–52.Howard, C. R., Howard, F. M., & Weitzman, M. L. (1994).
Acetaminophen analgesia in neonatal circumcision: Theeffect on pain. Pediatrics, 93(4), 641–646.
Hummel, P., & van Dijk, M. (2006). Pain assessment:Current status and challenges. Seminars in Fetal &Neonatal
Medicine, 11(4), 237–245.Jancke, L., Vogt, J., Musial, F., Lutz, K., & Theodor, K.
(1996). Facial EMG responses to auditory stimuli. Interna-tional Journal of Psychophysiology, 22, 85–96.
Johnston, C. C., Stevens, B. J., Yang, F., &Horton, L. (1995).Differential response to pain by very premature neonates.Pain, 61, 471–479.Johnston, C. C., & Strada, M. E. (1986). Acute pain re-
sponse in infants: A multidimensional description. Pain, 24,373–382.Johnston, C. C. (1993). Development of psychological re-
sponses to pain in infants and toddlers. In N. L. Schechter,C. B. Berde, & M. Yaster (Eds.), Pain in infants, children,
and adolescents (pp. 65–74). Baltimore/Philadelphia:Williams & Wilkins.Krechel, S. W., & Bildner, J. (1995). CRIES: A new neonatal
postoperative pain measurement score. Initial testing ofvalidity and reliability. Paediatric Anaesthesia, 5, 53–61.Labus, J., Keefe, F., & Jensen,M. (2003). Self-reports of pain
intensity and direct observations of pain behavior: When arethey correlated? Journal of Pain, 102, 109–124.Larochette, A. C., Chambers, C. T., & Craig, K. D. (2006).
Genuine, suppressed and faked facial expressions of pain inchildren. Pain, 126, 64–71.Lawrence, J., Alcock, D., McGrath, P., Kay, J.,
MacMurray, S. B., & Dulberg, C. (1993). The developmentof a tool to assess neonatal pain. Neonatal Network, 12(6),59–66.Lilley, C. M., Craig, K. D., & Grunau, R. V. E. (1997). The
expression of pain in infants and toddlers: Developmentalchanges in facial action. Pain, 72, 161–170.Machelska, H. (2007). Targeting of opioid-producing
leukocytes for pain control. Neuropeptides, 41, 355–363.Mahieu-Caputo, D., Muller, F., Jouvet, P., Thalabard, J.,
Jouannic, J., Nihoul-Fekete, C., Dumez, Y., &Dommergues, M. (2002). Amniotic fluid b-endorphin:A prognostic marker for gastroschisis? Journal of PediatricSurgery, 37(11), 1602–1606.McGrath, P. J., Rosmus, C., Camfield, C., Campbell, M. A., &
Hennigar, A. (1998). Behaviours caregivers use to determinepain in nonverbal, cognitively impaired individuals. Devel-opmental Medicine and Child Neurology, 40, 340–343.McGrath, P. J., & Unruh, A. M. (1994). Measurement and
assessment of paediatric pain. In P. D. Wall, & R. Melzack(Eds.), Textbook of pain, (3rd ed) (pp. 303–313). Edinburgh:Churchill Livingstone.Merkel, S. I., Shayevitz, J. R., Voepel-Lewis, T., & Malviya, S.
(1997). The FLACC: A behavioral scale for scoring postop-erative pain in young children. Pediatric Nursing, 23(3),293–297.Mousa, S. A., Straub, R. H., Schafer, M., & Stein, C. (2007).
b-Endorphin, met-enkephalin and corresponding opioidreceptors within synovium of patients with joint trauma,osteoarthritis and rheumatoid arthritis. Annals of Rheuma-
toid Disease, 66, 871–879.Oberlander, T. F., Gilbert, C. A., Chambers, C. T.,
O’Donnell, M. E., & Craig, K. D. (1999). Biobehavioralresponses to acute pain in adolescents with a significantneurologic impairment. The Clinical Journal of Pain, 15(3),201–209.Ong, J. C., Nicholson, R. A., & Gramling, S. E. (2003). EMG
reactivity and oral habits among young adult headachesufferers and painfree controls in a scheduled-waiting task.Applied Psychophysiology and Biofeedback, 28, 255–265.Owen, D. G., Bureau, Y., Thomas, A. W., Prato, F. S., & St.
Lawrence, K. S. (2008). Quantification of pain-inducedchanges in cerebral blood flow by perfusion MRI. Pain,136(1-2), 85–96.

168 Arif-Rahu, Fisher, and Matsuda
Ramelet, A., Abu-Saad, H. H., Rees, N., & McDonald, S.(2004). The challenges of pain measurement in critically illyoung children: A comprehensive review. AustralianCritical Care, 17(1), 33–45.
Raux, M., Ray, P., Prella, M., Duguet, A., Demoule, A., &Similowski, T. (2007). Cerebral cortex activation duringexperimentally induced ventilator fighting in normalhumans receiving noninvasive mechanical ventilation.Anesthesiology, 107, 746–755.
Rittner, H. L., Brack, A., & Stein, C. (2008). Pain and theimmune system. British Journal of Anesthesia, 101(1), 40–44.
Runefors, P., Arnbj€ornsson, E., Elander, G., &Michelsson, K.(2000). Newborn infants’ cry after heel-prick: Analysis withsound spectrogram. Acta Paediatrica, 89(1), 68–72.
Schiavenato, M., & Craig, K. D. (2010). Pain assessment asa social transaction: Beyond the ‘‘gold standard.’’. ClinicalJournal of Pain, 26(8), 667–676.
Sonnby-Borgstrom, M. (2002). The facial expression saysmore than words. Is emotional ‘‘contagion’’ via facial ex-pression the first step toward empathy? Lakartidningen, 99,1438–1442.
Sparshott, M. M. (1996). The development of a clinicaldistress scale for ventilated newborn infants: Identificationof pain and distress based on validated behavioral scores.Journal of Neonatal Nursing, 2, 5–11.
Sweet, S. D., & McGrath, P. J. (1998). Physiologicalmeasures of pain. In G. A. Finley, & P. J. McGrath (Eds.),Measurement of pain in infants and children. Progress
in pain research and management, (pp. 59–81). Seat-tle, WA: IASP Press.
van Dijk, M., de Boer, J., Koot, H. M., Tibboel, D.,Passchier, J., & Duivenvoorden, H. J. (2000). The reli-
ability and validity of the COMFORT scale as a postoper-ative pain instrument in 0 to 3-year-old infants. Pain, 84,367–377.van Dijk, M., de Boer, J., Koot, H. M., Duivenvoorden, H. J.,
Passchier, J., Bouwmeester, N., & Tibboel, D. (2001). Theassociation between physiological and behavioral painmeasures in 0- to 3-year-old infants after major surgery.Journal of Pain and Symptom Management, 22(1),600–609.van Dijk, M., Koot, H. M., Abu Saad, H. H., Tibboel, D., &
Passchier, J. (2002). Observational visual analog scale inpediatric pain assessment: Useful tool or good riddance? TheClinical Journal of Pain, 18, 310–316.Verri, W. A., Cunha, T. M., Parada, C. A., Poole, S.,
Cunha, F. Q., & Ferreira, S. H. (2006). Hypernociceptive roleof cytokines and chemokines: Targets of analgesic drug de-velopment? Pharmacology & Therapeutics, 112, 116–138.Weyers, P., Muhlberger, A., Hefele, C., & Pauli, P.
(2006). Electromyographic responses to static anddynamic avatar emotional facial expressions. Psychophys-iology, 43, 450–453.Willis, M. H. W., Merkel, S. I., Voepel-Lewis, T., &
Malviya, S. (2003). FLACC behavioral pain assessment scale:A comparisonwith the child’s self-report. Pediatric Nursing,29(3), 195–198.Wolf, K., Raedler, T., Henke, K., Kiefer, F., Mass, R.,
Quante, M., & Wiedemann, K. (2005). The face of pain—A pilot study to validate the measurement of facial painexpression with an improved electromyogrammethod. PainResearch & Management, 10(1), 15–19.Zhang, J. M., & An, J. (2007). Cytokines, inflammation and
pain. International Anesthesiology Clinics, 45(2), 27–37.