Embed Size (px)
Citation preview
BILL REQUEST - CODE REVISER'S OFFICE
BILL REQ. #: Z-0075.2/19 2nd draftATTY/TYPIST: AF:aklBRIEF DESCRIPTION: Concerning maternal mortality reviews.
AN ACT Relating to maternal mortality reviews; amending RCW170.54.450, 70.02.230, and 68.50.104; and repealing 2016 c 238 s 42(uncodified).3
BE IT ENACTED BY THE LEGISLATURE OF THE STATE OF WASHINGTON:4
Sec. 1. RCW 70.54.450 and 2016 c 238 s 1 are each amended to5read as follows:6
(1) For the purposes of this section, "maternal mortality" or7"maternal death" means a death of a woman while pregnant or within8one year of delivering or following the end of a pregnancy, ((whether9or not the woman's death is related to or aggravated by the10pregnancy)) from any cause.11
(2) A maternal mortality review panel is established to conduct12comprehensive, multidisciplinary reviews of maternal deaths in13Washington to identify factors associated with the deaths and make14recommendations for system changes to improve health care services15for women in this state. The members of the panel must be appointed16by the secretary of the department of health, must include at least17one representative of tribal governments, must serve without18compensation, and may include:19
(a) An obstetrician;20(b) A physician specializing in maternal fetal medicine;21
Code Rev/AF:akl 1 Z-0075.2/19 2nd draft
(c) A neonatologist;1(d) A midwife with licensure in the state of Washington;2(e) A representative from the department of health who works in3
the field of maternal and child health;4(f) A department of health epidemiologist with experience5
analyzing perinatal data;6(g) A pathologist; and7(h) A representative of the community mental health centers.8(3) The maternal mortality review panel must conduct9
comprehensive, multidisciplinary reviews of maternal mortality in10Washington. The panel may not call witnesses or take testimony from11any individual involved in the investigation of a maternal death or12enforce any public health standard or criminal law or otherwise13participate in any legal proceeding relating to a maternal death.14
(4)(a) Information, documents, proceedings, records, and opinions15created, collected, or maintained by the maternity mortality review16panel or the department of health in support of the maternal17mortality review panel are confidential and are not subject to public18inspection or copying under chapter 42.56 RCW and are not subject to19discovery or introduction into evidence in any civil or criminal20action.21
(b) Any person who was in attendance at a meeting of the maternal22mortality review panel or who participated in the creation,23collection, or maintenance of the panel's information, documents,24proceedings, records, or opinions may not be permitted or required to25testify in any civil or criminal action as to the content of such26proceedings, or the panel's information, documents, records, or27opinions. This subsection does not prevent a member of the panel from28testifying in a civil or criminal action concerning facts which form29the basis for the panel's proceedings of which the panel member had30personal knowledge acquired independently of the panel or which is31public information.32
(c) Any person who, in substantial good faith, participates as a33member of the maternal mortality review panel or provides information34to further the purposes of the maternal mortality review panel may35not be subject to an action for civil damages or other relief as a36result of the activity or its consequences.37
(d) All meetings, proceedings, and deliberations of the maternal38mortality review panel may, at the discretion of the maternal39
Code Rev/AF:akl 2 Z-0075.2/19 2nd draft
mortality review panel, be confidential and may be conducted in1executive session.2
(e) The maternal mortality review panel and ((the secretary of))3the department of health may retain identifiable information4regarding facilities where maternal deaths occur, or facilities from5which ((the patient was transferred, occur)) a patient whose record6is or will be examined by the maternal mortality review panel was7transferred, and geographic information on each case ((solely)) for8the purposes of ((trending and analysis over time)) determining9trends, performing analysis over time, and for quality improvement10efforts. All individually identifiable information must be removed11before any case review by the panel.12
(5) The department of health shall review department available13data to identify maternal deaths. To aid in determining whether a14maternal death was related to or aggravated by the pregnancy, ((and))15whether it was preventable, and to coordinate quality improvement16efforts, the department of health has the authority to:17
(a) Request and receive data for specific maternal deaths18including, but not limited to, all medical records, autopsy reports,19medical examiner reports, coroner reports, and social service20records; and21
(b) Request and receive data as described in (a) of this22subsection from health care providers, health care facilities,23clinics, laboratories, medical examiners, coroners, professions and24facilities licensed by the department of health, local health25jurisdictions, the health care authority and its licensees and26providers, ((and)) the department of social and health services and27its licensees and providers, and the department of children, youth,28and families and its licensees and providers.29
(6) Upon request by the department of health, health care30providers, health care facilities, clinics, laboratories, medical31examiners, coroners, professions and facilities licensed by the32department of health, local health jurisdictions, the health care33authority and its licensees and providers, ((and)) the department of34social and health services and its licensees and providers, and the35department of children, youth, and families and its licensees and36providers must provide all medical records, autopsy reports, medical37examiner reports, coroner reports, social services records,38information and records related to sexually transmitted diseases, and39
Code Rev/AF:akl 3 Z-0075.2/19 2nd draft
other data requested for specific maternal deaths as provided for in1subsection (5) of this section to the department.2
(7) By ((July 1, 2017)) October 1, 2019, and ((biennially)) every3three years thereafter, the maternal mortality review panel must4submit a report to the secretary of the department of health and the5health care committees of the senate and house of representatives.6The report must protect the confidentiality of all decedents and7other participants involved in any incident. The report must be8distributed to relevant stakeholder groups for performance9improvement. Interim results may be shared at the Washington state10hospital association coordinated quality improvement program. The11report must include the following:12
(a) A description of the maternal deaths reviewed by the panel13((during the preceding twenty-four months)), including statistics and14causes of maternal deaths presented in the aggregate, but the report15must not disclose any identifying information of patients, decedents,16providers, and organizations involved; and17
(b) Evidence-based system changes and possible legislation to18improve maternal outcomes and reduce preventable maternal deaths in19Washington.20
(8) Upon the approval of the department of health and with a21signed written data-sharing agreement, the department of health may22release data and/or findings with indirect identifiers only to the23centers for disease control and prevention, regional maternal24mortality review efforts, or local health jurisdictions of Washington25state.26
(a) A written data-sharing agreement under this section must, at27a minimum:28
(i) Include a description of the proposed purpose of the request,29the scientific justification for the proposal, the type of data30needed, and the purpose for which the data will be used;31
(ii) Include the methods to be used to protect the32confidentiality and security of the data;33
(iii) Prohibit redisclosure of any identifiers without explicit34permission from the department of health;35
(iv) Prohibit the recipient of the data from attempting to36determine the identity of persons or parties whose information is37included in the data set or use the data in any manner that38identifies individuals or their family members, or health care39providers and facilities;40Code Rev/AF:akl 4 Z-0075.2/19 2nd draft
(v) State that ownership of data provided under this section1remains with the department of health, and is not transferred to2those authorized to receive and use the data under the agreement; and3
(vi) Require the recipient of the data to include appropriate4citations when the data is used in research reports or publications5of research findings.6
(b) The department of health may deny a request to share data7and/or findings that does not meet the requirements.8
(c) For the purposes of this subsection:9(i) "Direct identifier" means a single data element that10
identifies an individual person.11(ii) "Indirect identifier" means a single data element that on12
its own might not identify an individual person, but when combined13with other indirect identifiers is likely to identify an individual14person.15
(9) For the purposes of the maternal mortality review, hospitals16and birth centers must report all maternal deaths which occur during17pregnancy or within the first forty-two days after the end of18pregnancy to the local coroner or medical examiner:19
(a) Maternal deaths must be reported within thirty-six hours20after death.21
(b) Each reported maternal death must receive a death22investigation per guidelines established by the department of health23with autopsy strongly recommended.24
(c) All maternal death autopsies must follow the maternal death25investigation protocol published by the department of health.26
(d) Reimbursement of maternal death autopsies must be at one27hundred percent to the counties for pathology services.28
Sec. 2. RCW 70.02.230 and 2018 c 201 s 8002 are each amended to29read as follows:30
(1) Except as provided in this section, RCW 70.02.050, 71.05.445,3174.09.295, 70.02.210, 70.02.240, 70.02.250, and 70.02.260, or32pursuant to a valid authorization under RCW 70.02.030, the fact of33admission to a provider for mental health services and all34information and records compiled, obtained, or maintained in the35course of providing mental health services to either voluntary or36involuntary recipients of services at public or private agencies must37be confidential.38
Code Rev/AF:akl 5 Z-0075.2/19 2nd draft
(2) Information and records related to mental health services,1other than those obtained through treatment under chapter 71.34 RCW,2may be disclosed only:3
(a) In communications between qualified professional persons to4meet the requirements of chapter 71.05 RCW, in the provision of5services or appropriate referrals, or in the course of guardianship6proceedings if provided to a professional person:7
(i) Employed by the facility;8(ii) Who has medical responsibility for the patient's care;9(iii) Who is a designated crisis responder;10(iv) Who is providing services under chapter 71.24 RCW;11(v) Who is employed by a state or local correctional facility12
where the person is confined or supervised; or13(vi) Who is providing evaluation, treatment, or follow-up14
services under chapter 10.77 RCW;15(b) When the communications regard the special needs of a patient16
and the necessary circumstances giving rise to such needs and the17disclosure is made by a facility providing services to the operator18of a facility in which the patient resides or will reside;19
(c)(i) When the person receiving services, or his or her20guardian, designates persons to whom information or records may be21released, or if the person is a minor, when his or her parents make22such a designation;23
(ii) A public or private agency shall release to a person's next24of kin, attorney, personal representative, guardian, or conservator,25if any:26
(A) The information that the person is presently a patient in the27facility or that the person is seriously physically ill;28
(B) A statement evaluating the mental and physical condition of29the patient, and a statement of the probable duration of the30patient's confinement, if such information is requested by the next31of kin, attorney, personal representative, guardian, or conservator;32and33
(iii) Other information requested by the next of kin or attorney34as may be necessary to decide whether or not proceedings should be35instituted to appoint a guardian or conservator;36
(d)(i) To the courts as necessary to the administration of37chapter 71.05 RCW or to a court ordering an evaluation or treatment38under chapter 10.77 RCW solely for the purpose of preventing the39
Code Rev/AF:akl 6 Z-0075.2/19 2nd draft
entry of any evaluation or treatment order that is inconsistent with1any order entered under chapter 71.05 RCW.2
(ii) To a court or its designee in which a motion under chapter310.77 RCW has been made for involuntary medication of a defendant for4the purpose of competency restoration.5
(iii) Disclosure under this subsection is mandatory for the6purpose of the federal health insurance portability and7accountability act;8
(e)(i) When a mental health professional or designated crisis9responder is requested by a representative of a law enforcement or10corrections agency, including a police officer, sheriff, community11corrections officer, a municipal attorney, or prosecuting attorney to12undertake an investigation or provide treatment under RCW 71.05.150,1310.31.110, or 71.05.153, the mental health professional or designated14crisis responder shall, if requested to do so, advise the15representative in writing of the results of the investigation16including a statement of reasons for the decision to detain or17release the person investigated. The written report must be submitted18within seventy-two hours of the completion of the investigation or19the request from the law enforcement or corrections representative,20whichever occurs later.21
(ii) Disclosure under this subsection is mandatory for the22purposes of the federal health insurance portability and23accountability act;24
(f) To the attorney of the detained person;25(g) To the prosecuting attorney as necessary to carry out the26
responsibilities of the office under RCW 71.05.330(2),2771.05.340(1)(b), and 71.05.335. The prosecutor must be provided28access to records regarding the committed person's treatment and29prognosis, medication, behavior problems, and other records relevant30to the issue of whether treatment less restrictive than inpatient31treatment is in the best interest of the committed person or others.32Information must be disclosed only after giving notice to the33committed person and the person's counsel;34
(h)(i) To appropriate law enforcement agencies and to a person,35when the identity of the person is known to the public or private36agency, whose health and safety has been threatened, or who is known37to have been repeatedly harassed, by the patient. The person may38designate a representative to receive the disclosure. The disclosure39must be made by the professional person in charge of the public or40Code Rev/AF:akl 7 Z-0075.2/19 2nd draft
private agency or his or her designee and must include the dates of1commitment, admission, discharge, or release, authorized or2unauthorized absence from the agency's facility, and only any other3information that is pertinent to the threat or harassment. The agency4or its employees are not civilly liable for the decision to disclose5or not, so long as the decision was reached in good faith and without6gross negligence.7
(ii) Disclosure under this subsection is mandatory for the8purposes of the federal health insurance portability and9accountability act;10
(i)(i) To appropriate corrections and law enforcement agencies11all necessary and relevant information in the event of a crisis or12emergent situation that poses a significant and imminent risk to the13public. The mental health service agency or its employees are not14civilly liable for the decision to disclose or not so long as the15decision was reached in good faith and without gross negligence.16
(ii) Disclosure under this subsection is mandatory for the17purposes of the health insurance portability and accountability act;18
(j) To the persons designated in RCW 71.05.425 for the purposes19described in those sections;20
(k) Upon the death of a person. The person's next of kin,21personal representative, guardian, or conservator, if any, must be22notified. Next of kin who are of legal age and competent must be23notified under this section in the following order: Spouse, parents,24children, brothers and sisters, and other relatives according to the25degree of relation. Access to all records and information compiled,26obtained, or maintained in the course of providing services to a27deceased patient are governed by RCW 70.02.140;28
(l) To mark headstones or otherwise memorialize patients interred29at state hospital cemeteries. The department of social and health30services shall make available the name, date of birth, and date of31death of patients buried in state hospital cemeteries fifty years32after the death of a patient;33
(m) To law enforcement officers and to prosecuting attorneys as34are necessary to enforce RCW 9.41.040(2)(a)(((iii))) (iv). The extent35of information that may be released is limited as follows:36
(i) Only the fact, place, and date of involuntary commitment, an37official copy of any order or orders of commitment, and an official38copy of any written or oral notice of ineligibility to possess a39
Code Rev/AF:akl 8 Z-0075.2/19 2nd draft
firearm that was provided to the person pursuant to RCW 9.41.047(1),1must be disclosed upon request;2
(ii) The law enforcement and prosecuting attorneys may only3release the information obtained to the person's attorney as required4by court rule and to a jury or judge, if a jury is waived, that5presides over any trial at which the person is charged with violating6RCW 9.41.040(2)(a)(((iii))) (iv);7
(iii) Disclosure under this subsection is mandatory for the8purposes of the federal health insurance portability and9accountability act;10
(n) When a patient would otherwise be subject to the provisions11of this section and disclosure is necessary for the protection of the12patient or others due to his or her unauthorized disappearance from13the facility, and his or her whereabouts is unknown, notice of the14disappearance, along with relevant information, may be made to15relatives, the department of corrections when the person is under the16supervision of the department, and governmental law enforcement17agencies designated by the physician or psychiatric advanced18registered nurse practitioner in charge of the patient or the19professional person in charge of the facility, or his or her20professional designee;21
(o) Pursuant to lawful order of a court;22(p) To qualified staff members of the department, to the23
authority, to the director of behavioral health organizations, to24resource management services responsible for serving a patient, or to25service providers designated by resource management services as26necessary to determine the progress and adequacy of treatment and to27determine whether the person should be transferred to a less28restrictive or more appropriate treatment modality or facility;29
(q) Within the mental health service agency where the patient is30receiving treatment, confidential information may be disclosed to31persons employed, serving in bona fide training programs, or32participating in supervised volunteer programs, at the facility when33it is necessary to perform their duties;34
(r) Within the department and the authority as necessary to35coordinate treatment for mental illness, developmental disabilities,36alcoholism, or substance use disorder of persons who are under the37supervision of the department;38
(s) Between the department of social and health services, the39department of children, youth, and families, and the health care40Code Rev/AF:akl 9 Z-0075.2/19 2nd draft
authority as necessary to coordinate treatment for mental illness,1developmental disabilities, alcoholism, or drug abuse of persons who2are under the supervision of the department of social and health3services or the department of children, youth, and families;4
(t) To a licensed physician or psychiatric advanced registered5nurse practitioner who has determined that the life or health of the6person is in danger and that treatment without the information and7records related to mental health services could be injurious to the8patient's health. Disclosure must be limited to the portions of the9records necessary to meet the medical emergency;10
(u)(i) Consistent with the requirements of the federal health11insurance portability and accountability act, to:12
(A) A health care provider who is providing care to a patient, or13to whom a patient has been referred for evaluation or treatment; or14
(B) Any other person who is working in a care coordinator role15for a health care facility or health care provider or is under an16agreement pursuant to the federal health insurance portability and17accountability act with a health care facility or a health care18provider and requires the information and records to assure19coordinated care and treatment of that patient.20
(ii) A person authorized to use or disclose information and21records related to mental health services under this subsection22(2)(u) must take appropriate steps to protect the information and23records relating to mental health services.24
(iii) Psychotherapy notes may not be released without25authorization of the patient who is the subject of the request for26release of information;27
(v) To administrative and office support staff designated to28obtain medical records for those licensed professionals listed in (u)29of this subsection;30
(w) To a facility that is to receive a person who is31involuntarily committed under chapter 71.05 RCW, or upon transfer of32the person from one evaluation and treatment facility to another. The33release of records under this subsection is limited to the34information and records related to mental health services required by35law, a record or summary of all somatic treatments, and a discharge36summary. The discharge summary may include a statement of the37patient's problem, the treatment goals, the type of treatment which38has been provided, and recommendation for future treatment, but may39not include the patient's complete treatment record;40Code Rev/AF:akl 10 Z-0075.2/19 2nd draft
(x) To the person's counsel or guardian ad litem, without1modification, at any time in order to prepare for involuntary2commitment or recommitment proceedings, reexaminations, appeals, or3other actions relating to detention, admission, commitment, or4patient's rights under chapter 71.05 RCW;5
(y) To staff members of the protection and advocacy agency or to6staff members of a private, nonprofit corporation for the purpose of7protecting and advocating the rights of persons with mental disorders8or developmental disabilities. Resource management services may limit9the release of information to the name, birthdate, and county of10residence of the patient, information regarding whether the patient11was voluntarily admitted, or involuntarily committed, the date and12place of admission, placement, or commitment, the name and address of13a guardian of the patient, and the date and place of the guardian's14appointment. Any staff member who wishes to obtain additional15information must notify the patient's resource management services in16writing of the request and of the resource management services' right17to object. The staff member shall send the notice by mail to the18guardian's address. If the guardian does not object in writing within19fifteen days after the notice is mailed, the staff member may obtain20the additional information. If the guardian objects in writing within21fifteen days after the notice is mailed, the staff member may not22obtain the additional information;23
(z) To all current treating providers of the patient with24prescriptive authority who have written a prescription for the25patient within the last twelve months. For purposes of coordinating26health care, the department or the authority may release without27written authorization of the patient, information acquired for28billing and collection purposes as described in RCW 70.02.050(1)(d).29The department, or the authority, if applicable, shall notify the30patient that billing and collection information has been released to31named providers, and provide the substance of the information32released and the dates of such release. Neither the department nor33the authority may release counseling, inpatient psychiatric34hospitalization, or drug and alcohol treatment information without a35signed written release from the client;36
(aa)(i) To the secretary of social and health services and the37director of the health care authority for either program evaluation38or research, or both so long as the secretary or director, where39applicable, adopts rules for the conduct of the evaluation or40Code Rev/AF:akl 11 Z-0075.2/19 2nd draft
research, or both. Such rules must include, but need not be limited1to, the requirement that all evaluators and researchers sign an oath2of confidentiality substantially as follows:3
"As a condition of conducting evaluation or research concerning4persons who have received services from (fill in the facility,5agency, or person) I, . . . . . ., agree not to divulge, publish, or6otherwise make known to unauthorized persons or the public any7information obtained in the course of such evaluation or research8regarding persons who have received services such that the person who9received such services is identifiable.10
I recognize that unauthorized release of confidential information11may subject me to civil liability under the provisions of state law.12
/s/ . . . . . ."13(ii) Nothing in this chapter may be construed to prohibit the14
compilation and publication of statistical data for use by government15or researchers under standards, including standards to assure16maintenance of confidentiality, set forth by the secretary, or17director, where applicable;18
(bb) To any person if the conditions in RCW 70.02.205 are met;19(cc) To the secretary of health for the purposes of the maternal20
mortality review panel established in RCW 70.54.450.21(3) Whenever federal law or federal regulations restrict the22
release of information contained in the information and records23related to mental health services of any patient who receives24treatment for chemical dependency, the department or the authority25may restrict the release of the information as necessary to comply26with federal law and regulations.27
(4) Civil liability and immunity for the release of information28about a particular person who is committed to the department of29social and health services or the authority under RCW 71.05.280(3)30and 71.05.320(4)(c) after dismissal of a sex offense as defined in31RCW 9.94A.030, is governed by RCW 4.24.550.32
(5) The fact of admission to a provider of mental health33services, as well as all records, files, evidence, findings, or34orders made, prepared, collected, or maintained pursuant to chapter3571.05 RCW are not admissible as evidence in any legal proceeding36outside that chapter without the written authorization of the person37who was the subject of the proceeding except as provided in RCW3870.02.260, in a subsequent criminal prosecution of a person committed39
Code Rev/AF:akl 12 Z-0075.2/19 2nd draft
pursuant to RCW 71.05.280(3) or 71.05.320(4)(c) on charges that were1dismissed pursuant to chapter 10.77 RCW due to incompetency to stand2trial, in a civil commitment proceeding pursuant to chapter 71.093RCW, or, in the case of a minor, a guardianship or dependency4proceeding. The records and files maintained in any court proceeding5pursuant to chapter 71.05 RCW must be confidential and available6subsequent to such proceedings only to the person who was the subject7of the proceeding or his or her attorney. In addition, the court may8order the subsequent release or use of such records or files only9upon good cause shown if the court finds that appropriate safeguards10for strict confidentiality are and will be maintained.11
(6)(a) Except as provided in RCW 4.24.550, any person may bring12an action against an individual who has willfully released13confidential information or records concerning him or her in14violation of the provisions of this section, for the greater of the15following amounts:16
(i) One thousand dollars; or17(ii) Three times the amount of actual damages sustained, if any.18(b) It is not a prerequisite to recovery under this subsection19
that the plaintiff suffered or was threatened with special, as20contrasted with general, damages.21
(c) Any person may bring an action to enjoin the release of22confidential information or records concerning him or her or his or23her ward, in violation of the provisions of this section, and may in24the same action seek damages as provided in this subsection.25
(d) The court may award to the plaintiff, should he or she26prevail in any action authorized by this subsection, reasonable27attorney fees in addition to those otherwise provided by law.28
(e) If an action is brought under this subsection, no action may29be brought under RCW 70.02.170.30
NEW SECTION. Sec. 3. 2016 c 238 s 4 (uncodified) is repealed.31
Sec. 4. RCW 68.50.104 and 2001 c 82 s 2 are each amended to read32as follows:33
(1) The cost of autopsy shall be borne by the county in which the34autopsy is performed, except when requested by the department of35labor and industries, in which case, the department shall bear the36cost of such autopsy.37
Code Rev/AF:akl 13 Z-0075.2/19 2nd draft
(2)(a) Except as provided in (((c))) (b) of this subsection, when1the county bears the cost of an autopsy, it shall be reimbursed from2the death investigations account, established by RCW 43.79.445, as3follows:4
(((a))) (i) Up to forty percent of the cost of contracting for5the services of a pathologist to perform an autopsy;6
(((b))) (ii) Up to twenty-five percent of the salary of7pathologists who are primarily engaged in performing autopsies and8are (((i))) (A) county coroners or county medical examiners, or9(((ii))) (B) employees of a county coroner or county medical10examiner; and11
(((c))) (iii) Up to one hundred percent of the cost of autopsies12conducted under RCW 70.54.450(9).13
(b) When the county bears the cost of an autopsy of a child under14the age of three whose death was sudden and unexplained, the county15shall be reimbursed for the expenses of the autopsy when the death16scene investigation and the autopsy have been conducted under RCW1743.103.100 (4) and (5), and the autopsy has been done at a facility18designed for the performance of autopsies.19
(c) Payments from the account shall be made pursuant to biennial20appropriation: PROVIDED, That no county may reduce funds appropriated21for this purpose below 1983 budgeted levels.22
--- END ---
Code Rev/AF:akl 14 Z-0075.2/19 2nd draft
2019-21 Biennium BudgetDecision Package
Agency: 303 - Department of HealthDecision Package Code-Title: 1P - Con nue Maternal Mortality ReviewsBudget Session: 2019-21 RegularBudget Level: Policy LevelContact Info: Ryan Black
(360) [email protected]
Agency Recommendation SummaryMaternal mortality is on the rise in the United States, with minority communi es experiencing dispari escompared to the general popula on. Maternal mortality is also under- reported, leaving Washingtonwithout cri cal data to inform policy recommenda ons to reduce the rate of occurence. The Department ofHealth (DOH) requests funding to con nue the biennial Maternal Mortality Review Report and align statepolicy with na onal best prac ces.
Fiscal SummaryDollars in Thousands
Opera ng Expenditures FY 2020 FY 2021 FY 2022 FY 2023
Fund 001 - 1 $408 $399 $399 $399
Total Expenditures $408 $399 $399 $399
Biennial Totals $807 $798
Staffing FY 2020 FY 2021 FY 2022 FY 2023
FTEs 3.4 3.4 3.4 3.4
Average Annual 3.4 3.4
Object of Expenditure FY 2020 FY 2021 FY 2022 FY 2023
Obj. A $262 $261 $261 $261
Obj. B $91 $91 $91 $91
Obj. E $20 $20 $20 $20
Obj. G $7 $7 $7 $7
Obj. J $8 $0 $0 $0
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
1 of 12 9/19/2018 8:28 AM
Object of Expenditure FY 2020 FY 2021 FY 2022 FY 2023
Obj. T $20 $20 $20 $20
Package DescriptionWhat is the problem, opportunity or priority you are addressing with the request?
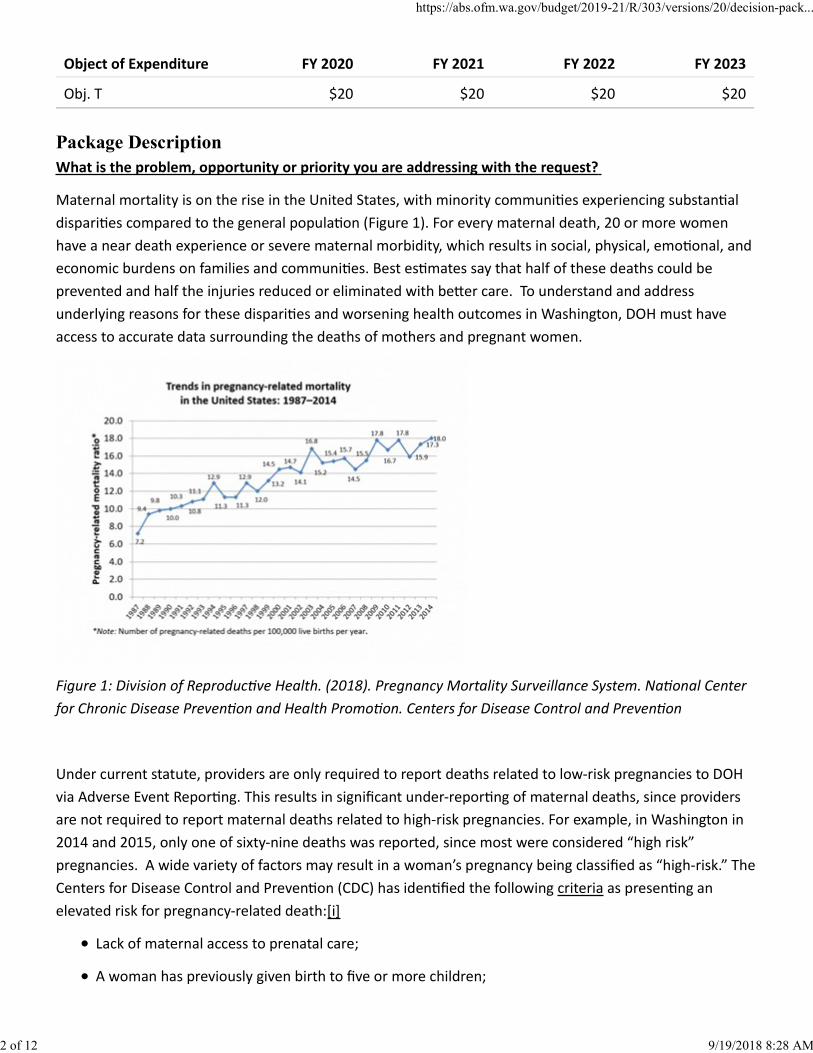
Maternal mortality is on the rise in the United States, with minority communi es experiencing substan aldispari es compared to the general popula on (Figure 1). For every maternal death, 20 or more womenhave a near death experience or severe maternal morbidity, which results in social, physical, emo onal, andeconomic burdens on families and communi es. Best es mates say that half of these deaths could beprevented and half the injuries reduced or eliminated with be er care. To understand and addressunderlying reasons for these dispari es and worsening health outcomes in Washington, DOH must haveaccess to accurate data surrounding the deaths of mothers and pregnant women.
Figure 1: Division of Reproduc ve Health. (2018). Pregnancy Mortality Surveillance System. Na onal Centerfor Chronic Disease Preven on and Health Promo on. Centers for Disease Control and Preven on
Under current statute, providers are only required to report deaths related to low-risk pregnancies to DOHvia Adverse Event Repor ng. This results in significant under-repor ng of maternal deaths, since providersare not required to report maternal deaths related to high-risk pregnancies. For example, in Washington in2014 and 2015, only one of sixty-nine deaths was reported, since most were considered “high risk”pregnancies. A wide variety of factors may result in a woman’s pregnancy being classified as “high-risk.” TheCenters for Disease Control and Preven on (CDC) has iden fied the following criteria as presen ng anelevated risk for pregnancy-related death:[i]
Lack of maternal access to prenatal care;
A woman has previously given birth to five or more children;
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
2 of 12 9/19/2018 8:28 AM
Pregnancy to a woman 35 years of age or older;
A pregnant woman is of African American or Hispanic heritage.
Under current statute, if a woman met any of these criteria and died during childbirth, her death is notrequired to be reported.
The Maternal Mortality Review Panel uses data from a variety of state and local government en es todetermine whether pregnancy or childbirth were a direct cause or contribu ng factor in each maternaldeath reviewed. The informa on gained from these reviews is then aggregated to iden fy pa erns orcommonali es among the maternal deaths reviewed, and whether policy, systems, or environmentalchanges may improve future health outcomes for women. The panel submits its recommenda ons toaddress these iden fied issues to DOH, the legislature, and relevant stakeholder groups in a biennial report,which is then used to inform maternal health policies and programs.
Since implementa on of this law, DOH has iden fied quality improvement efforts to align our state with CDCbest prac ces. These include:
Repor ng deaths from suicide, opioids and other injuries.
Exis ng law does not allow DOH to share de-iden fied informa on with the CDC, coun es, or healthsystems, thereby hindering the ability for federal or local-level public health organiza ons toaccurately formulate data-driven responses and quality improvement strategies when pa erns areobserved in the data.
Capturing complete maternal health data by requiring hospitals and birthing centers to report allmaternal deaths which occur within 42 days of giving birth, so valuable informa on is collectedrelated to cause of death, pregnancy or childbirth, and whether they were preventable. Because onlydeaths related to low-risk pregnancies are currently reported to DOH, the panel is unable to developreports that accurately reflect maternal mortality in the state, or policy recommenda ons that fullyaddress factors that contribute to maternal deaths.
The statute manda ng the comple on of the report expires in June 2020. Improving the health-caresystem overall is a cri cal component to reducing maternal mortality. Knowing the level of maternalmortality is not enough; we need to understand the underlying factors that led to the deaths. Eachmaternal death can provide indica ons on prac cal ways of addressing its causes and determinants.Without the mortality report as a permanent requirement, as well as funding to conduct maternalmortality reviews, the state will lose a vital source of informa on that shows us where the state isimproving and where it is not so that strategies and policy interven ons to prevent maternal deathscan be developed.
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
3 of 12 9/19/2018 8:28 AM
What is your proposed solu on?
DOH proposes revising RCW 70.54.450 to: extend the law, which is currently set to expire June 2020; requirehospitals and birthing centers to report the deaths of pregnant women and women who die within 42 daysa er the end of pregnancy to local county coroners or medical examiners, and fund autopsies for thosedeaths; allow DOH to consider, and upon approval, share deiden fied data related to the review with theCDC, regional maternal mortality review efforts, and local health jurisdic ons; and annual funding forthe cost of comple ng reviews, coordina ng quality improvement, and publishing biennial reports that alignwith best prac ces.
These revisions will allow DOH and the panel to con nue to review these deaths and track state trends tounderstand the issues that contribute to poor maternal healthoutcomes. The report will also enableproviders and facili es to address risk factors to prevent maternal mortality and morbidi es.
The total cost to complete the reviews and reports, and support implementa on of the panel’srecommenda ons is $410,000 per year, or $820,000 for the biennium.
The proposed changes would strengthen the law and the work that is being done and ensure theinforma on collected for the review process results in concrete ac vi es to address root causes of maternalmortality. The changes would also help align Washington with federal efforts to reduce maternal mortality.
What are you purchasing and how does it solve the problem?
The costs for this proposal are ongoing costs to staff and facilitate an ongoing maternal mortality review,associated quality improvement coordina on, and produce a biennial report with recommenda ons toreduce maternal deaths and improve maternal and infant health outcomes. Maternal death inves ga onsand autopsies are paid for under a designated account. Addi onal fiscal detail is provided in the a achedcost models.
What alterna ves did you explore and why was this op on chosen?
Alterna ve methods that do not require legisla ve changes have been explored and some have beena empted, including:
Implemen ng panel recommenda ons on preven ng maternal mortality without the ability to sharekey data and within the constraints of the law and current resources;
Passively par cipa ng in local, regional, and federal efforts without sharing data;
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
4 of 12 9/19/2018 8:28 AM
Comple ng a maternal mortality review and report based on the current meline;
Performing maternal mortality reviews without key records that must be obtained from theDepartment of Children, Youth, and Families, which is not men oned in the current law.
Performing maternal mortality reviews without key mental health records that must be obtained fromthe Health Care Authority. Currently law prevents DOH from accessing these records.
[i] Centers for Disease Control and Preven on. Gateway to Health Communica on & Social Marke ngPrac ce: Pregnancy and Prenatal Care. h ps://www.cdc.gov/healthcommunica on/toolstemplates/entertainmented/ ps/PregnancyPrenatalCare.html
Assumptions and Calculations
Expansion or altera on of a current program or service: This proposal is a con nua on of the current program that is scheduled to sunset. In addi on, we arereques ng increased state funding to cover the actual costs we incur annually to conduct the reviewsand develop the reports. In 2017, 2018, and 2019 we covered the gap between our state funding andactual costs using other funds.
Addi onal fiscal detail is a ached to this decision package.
Year General Fund State – MMR Maternal Child Health BlockGrant
Total Program Alloca on
2016 $0 $0 $0
2017 $230,000 $197,000 $427,000
2018 $227,000 $197,000 $427,000
2019 $227,000 $197,000 $427,000
2020 $227,000 $0 $227,000
2021 $227,000 $0 $227,000
Detailed assump ons and calcula ons:This mandate requires 2.5 FTE per year, including 0.80 FTE of a Health Services Consultant 3, 0.50 FTE ofa Public Health Nurse, 0.55 FTE of an Epidemiologist 3, 0.40 FTE of an Epidemiologist 2, 0.10 FTE of a
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
5 of 12 9/19/2018 8:28 AM
Health Services Consultant 4, 0.10 FTE of a Research Inves gator 3 and 0.05 FTE of a SeniorEpidemiologist. In addi on, es mated expenditures include .40 and .60 FTE in the 19-21 biennium toassist with increased division and agency workload.
There are four aspects to this mandate, including: iden fica on of maternal deaths and hospital/vitalrecords linkages; data collec on, analyses, and prepara on for the panel to review; convening theMaternal Mortality Review Panel and preparing the required report; and ini a ng implementa on ofthe panel recommenda ons. Below are the ac vi es by type of staff needed to complete this work.
Aspect 1 - Iden fica on of Maternal Deaths and Hospital/Vital Records Linkages
0.1 FTE Research Inves gator 3 to provide quality assurance of data, clarify cause of death, and conductfollow-up to confirm maternal deaths
0.35 FTE Epidemiologist 3 to link data from the birth records database with the death records databaseand the Comprehensive Hospital Abstract Repor ng System (CHARS) data, and to conduct data reviewand analysis for the report
0.05 FTE Senior Epidemiologist to supervise staff and provide quality assurance of the data
FTE = 0.5
Salaries = $48,000
Benefits = $17,000
Goods & Services = $1,000
Equipment = $1,550
Intra-Agency Reimbursement = $4,000
Total Direct Costs = $72,000
Indirects = $17,000
Total cost associated with the iden fica on of maternal deaths: $89,000
Aspect 2 - Data collec on, analyses, and prepara on for panel review
0.2 FTE Health Services Consultant (HSC)3 to request, collect, and manage all necessary records
0.2 FTE Nurse consultant to review medical records, iden fy records sources, summarize records for thepanel, and make clinical decisions related to data elements for data collec on
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
6 of 12 9/19/2018 8:28 AM

0.2 FTE MCH Epidemiologist 2 to iden fy medical facili es and other sources of data, review all sourcesof data, enter key data elements into the CDC database system, clean and prepare data, conduct dataanalyses, prepare charts and tables for report and presenta ons.
0.1 FTE MCH Epidemiologist 3 to provide subject ma er exper se, supervise data analysis ac vi es, andoversee the development of the data analysis and development of the surveillance system.
Coun es will incur a small cost due to expanding repor ng and autopsy requirements. The amountadded to the Forensic Inves ga on Council dedicated account is $25,000 per fiscal year based on anes mate from WACME of $2,500 per autopsy and 10 addi onal autopsies per year. This will be passedthru to coun es to absorb any new addi onal costs.
FTE = 0.7
Salaries = $61,000
Benefits = $21,000
Goods & Services = $1,000
Equipment = $2,000
Intra-Agency Reimbursement = $6,000
Total Direct Costs = $91,000
Indirects = $25,000
Total cost for data collec on, analyses, and prepara on for panel review: $116,000 per year.
Aspect – 3 Convene the Maternal Mortality Review Panel and Prepare the Report
0.1 FTE MCH Epidemiologist 2 to compile key data elements from various data sources to organize forreview by the panel and visual representa on in the report, present data to the the panel and otheraudiences, par cipate in review proceedings, analyze contribu ng factors to deaths, and assist withdevelopment of a biennial report for legislators and other stakeholders.
0.1 FTE MCH Epidemiologist 3 to provide subject ma er exper se and work with the MCHEpidemiologist 2 and the DOH team in implemen ng panelreviews, par cipate in review proceedings,and report wri ng.
0.1 FTE Public Health Nurse Consultant to provide expert consulta on to DOH staff implemen ng thereview, par cipate in all review proceedings, and to make key clinical decisions related to the reviewprocess.
0.3 FTE HSC 3 to manage administra ve and logis cal tasks related to the review prepara on andmee ngs, to recruit and facilitate appointment of panel members, to keep panel members informed ofreview processes and upcoming mee ngs and responsibili es, and to facilitate maternal mortality
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
7 of 12 9/19/2018 8:28 AM
review mee ngs
0.1 FTE HSC4 to supervise program and review proceedings and assist with troubleshoo ng internal andexternal barriers.
FTE = 0.7
Salaries = $57,000
Benefits = $20,000
Goods & Services = $11,000(Including Non-Employee travel to convene mee ng and publica on ofreport)
Equipment = $2,000
Intra-Agency Reimbursement = $6,000
Total Direct Costs = $96,000
Indirects = $26,000
Total cost to convene the the panel and complete the legisla ve report: $122,000
Aspect 4 - Ini ate Implementa on of Panel Recommenda ons
0.2 HSC 3 to assist with the implementa on of the panel recommenda ons as quality improvementefforts; disseminate informa on related to the review findings as well as general informa on aboutmaternal mortality and review processes at the DOH.
0.2 FTE Public Health Nurse Consultant to guide the overall implementa on of the review process and toini ate and provide guidance for state-wide efforts to reduce maternal mortality in Washington.
0.1 FTE MCH Epidemiologist 2 to par cipate in state-wide efforts related to the implementa on of thereview and general guidance around recommenda ons and best prac ces, and to collabora velydevelop an evalua on plan.
FTE = 0.5
Salaries = $42,000
Benefits = $15,000
Goods & Services = $1,000 (Including Non-Employee travel to convene mee ng and publica on ofreport)
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
8 of 12 9/19/2018 8:28 AM
Equipment = $2,000
Intra-Agency Reimbursement = $4,000
Total Direct Costs = $64,000
Indirects = $17,000
Total cost to ini ate implementa on of the recommenda ons: $81,000
Workforce Assump ons:Please see a ached Financial Calculator.
Strategic and Performance Outcomes
Strategic framework:The proposed changes support the governor’s priority of healthy and safe communi es and theHeathiest Next Genera on Ini a ve, as well as the Agency Strategic Plan. Na onally, maternal mortalityrates have been on the rise. In Washington, rates have remained more stable than the rest of thecountry, however the same inequi es in outcomes among popula ons seen in other parts of the US arealso present in Washington. The law requiring the maternal mortality review and report was created toiden fy those dispari es and make policy, systems, and environment recommenda ons to improveoutcomes for mothers and babies, and to iden fy ways to implement these recommenda ons.Protec ng women and improving maternal healthcare has an immediate and long-las ng impact on notonly a mother’s infant and children, but also on her family and community. Inves ng in mothers is aninvestment in communi es and in the state. This proposal strengthens exis ng law and allows theinforma on gleaned from the review to be more effec vely used to reduce maternal deaths.
Performance outcomes:Funding and staffing changes, the ability to access all records and data needed, the ability to share keyinforma on and data with key stakeholders, and suppor ng and coordina ng quality improvementefforts with providers, facili es, and larger health systems, have the poten al to greatly reduce thematernal mortality rate in Washington, and, more significantly, the maternal morbidity rate, which is ahuge economic burden on families, communi es, and healthcare and social systems, as well as aphysical and emo onal burden on women and their families. This work addresses several of the HealthyWashington performance outcomes and objec ves, including:
Healthy babies and mothers: The health of a mother directly impacts the health of her baby.Work to improve and expand access to maternal care for mothers during and a er pregnancy willhelp these women to be healthier. In turn, mothers can help their babies be healthier. Whenmothers and babies are healthy, they have the poten al to impact the health of communi es.Poten al outcomes overall include improved infant health and decreased rates of maternalmortality and morbidity. Outcomes related to Healthy People include the poten al to decrease
1.
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
9 of 12 9/19/2018 8:28 AM
infant mortality, decrease the number of infants born with low birth weight among allpopula ons, and decrease the rate of unintended pregnancies.
Healthy youth and adults: The panel made recommenda ons related to several key issuesiden fied as contribu ng to maternal mortality in Washington related to the Healthy WashingtonPerformance Outcomes for healthy youth and adults, including obesity and mental health careand treatment.
2.
a. Maternal deaths related to substance use and mental health accounted for nearly 25% ofall maternal deaths in Washington. The panel recommended that pregnant women andmothers with mental health and substance use disorders need be er access to high qualitymental health care services. The ability to coordinate quality improvement efforts thatsupport the development and/or expansion of these services would have a significantimpact on maternal health outcomes, and would decrease the state’s maternal mortalityrate. This could also impact outcomes related to Healthy People, including improvingreten on rates for outpa ent mental health services, improving the rate of service forpeople discharged from mental health care, and reducing the number of suicide and opioid-related overdose deaths in the state
b. For those deaths that were found to be directly related to pregnancy, the panel foundthat obesity directly contributed to the deaths in 31% of cases; 94% of the women who diedfrom pregnancy-related causes were overweight or obese. The panel recommended thathealthcare facili es, providers, and service providers need to improve maternal care forwomen who are overweight and obese. The ability to iden fy this as an issue in maternalhealth care and implement, support, and coordinate efforts to address maternal care forthis popula on has the poten al to help the state meet several Healthy Washingtonobjec ves related to chronic disease, including decreasing the percentage of adults whoreport fair or poor health and increasing the number of people who maintain healthyweights.
3. Access/Pay for quality: The findings of the maternal mortality review indicated that 100% of thewomen who died from pregnancy related causes were covered by some form of health insurance;75% were covered by Medicaid. The panel found that expanding healthcare coverage and theservices covered under insurance plans has the poten al to reduce maternal mortality and morbidityrates and prevent maternal deaths. Con nued inves ga on into healthcare coverage amongpregnant women and mothers allows DOH to focus a en on on areas and popula ons where issuesrelated to health care coverage and access remain. This informa on, combined with collabora veefforts to address these issues, has the poten al to increase Medicaid enrollment and perhaps thepercentage of residents who report they have a primary care provider.
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
10 of 12 9/19/2018 8:28 AM
Other Collateral Connections
Intergovernmental:The work in this proposal will have a minimal impact on tribal and local governments. DOH is reques ngtribal representa on in the proposed legisla on.DOH also requests expanding the maternal deaths thatmust be inves gated and autopsied to include deaths that occur within 42 days of giving birth. Coun eswill incur a small cost due to expanding repor ng and autopsy requirements. DOH asks that these costsbe reimbursed at 100%. Reimbursement will come from the Forensic Inves ga on Council dedicatedaccount, from which all autopsies are currently funded. DOH, in conjunc on with the WashingtonAssocia on of Coroners and Medical Examiners (WACME), determined this request would result in up to10 more death inves ga ons per year. Addi onal funding for these costs has been included in thisrequest. The amount added to the Forensic Inves ga on Council dedicated account is $25,000 per fiscalyear based on an es mate from WACME of $2,500 per autopsy and 10 addi onal autopsies per year.
Stakeholder response:A wide variety of stakeholders will be impacted by the proposed changes. DOH has worked extensivelywith stakeholders. Concerns expressed by stakeholders include the following, which are each addressedin turn.
Maternal deaths are rela vely rare. The legislature may have a difficulty jus fying inves ng statefunds to review an es mated 30 deaths per year. However, for every death, there are 50-100 ormore near deaths that result in severe maternal morbidity and have a heavy physical, emo onal,and socioeconomic burden on families and communi es. Currently, there is just enough fundingto conduct the reviews themselves; however, this funding does not account for the qualityimprovement ac vi es that must be done as a result of the review. Stakeholders and advocatesrely on DOH to lead the efforts related to the recommenda ons of the panel. Developing andcarrying out concrete steps to reduce maternal deaths and improve women’s healthcare in thestate is the crux of the maternal mortality review.
1.
2. Hospitals and providers may be reluctant to comply with addi onal repor ng requirements, whichmay be perceived as addi onal regulatory requirements. Mandatory repor ng of maternal deathswill ensure the data collected is accurate and that sufficient informa on is available to developpreven ve strategies.
3.County officials involved in death inves ga ons may have concerns about comple ng addi onalautopsies without guaranteed reimbursements to complete the work. This proposal requests thatrequired autopsies be 100% reimbursed to providers who perform them.
4. Data and iden ty the are pressing concerns that must be addressed if data is to be sharedbetween agencies. Only de-iden fied aggregated data will be shared. The data will be shared with afew key public health agencies, including CDC, local health jurisdic ons (LHJ) and regional maternalmortality efforts. DOH will also require a data user agreement with each en ty outlining how thedata can be used and how it must be protected
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
11 of 12 9/19/2018 8:28 AM
5. The need for access to behavioral health care records is not readily apparent. Legislatorsconcerned with privacy will likely require jus fica on for access to these records. Mental health-related issues are key to understanding deaths related to suicide and overdose, and how mentalhealth is affec ng maternal mortality as a whole.
Legal or administra ve mandates:N/A
Changes from current law:RCW 70.54.450 – see language changes in the document
This proposal expands the defini on of when autopsies are performed in maternal mortality cases to allincidences of maternal mortality within 42 days of the end of pregnancy, and requires coun es bereimbursed for 100% of associated costs.This change requires amending RCW 68.50.104 to disbursefunds from the death inves ga ons account to the forensic inves ga on council sufficient to reimbursecoun es for 100% of associated costs of autopsies.
State workforce impacts:N/A
State facili es impacts:N/A
Puget Sound recovery:N/A
Agency Questions
Did you include cost models and backup assump ons?See a ached backup.
Reference DocumentsCon nue Marternal Mortality Reviews - FnCal.xlsmFederal Efforts to Address Maternal Mortality.docxMaternal Mortality update-Fact Sheet Content Template.docx
IT Addendum
Does this Decision Package include funding for any IT-related costs, including hardware, so ware,(including cloud-based services), contracts or IT staff?No
https://abs.ofm.wa.gov/budget/2019-21/R/303/versions/20/decision-pack...
12 of 12 9/19/2018 8:28 AM



![BILL REQUEST - CODE REVISER'S OFFICE BILL REQ. #: Z … · 10 to the health of communities in Washington as a result of the 11 improved ... P v Ç W ï ì ï r u v } ( , o Z ]](https://img.pdfslide.us/doc/110x75/5c12924d09d3f224238b463c/bill-request-code-revisers-office-bill-req-z-10-to-the-health-of-communities.jpg)