Embed Size (px)
DESCRIPTION
Biliary Conditions. NUR-224. OBJECTIVES. Discus management of patient with cholelithiasis. Use the nursing process a framework for care of –patients with cholelithiasis and undergoing laparoscopic or open cholecystectomy. Differentiate between acute and chronic pancreatitis. - PowerPoint PPT Presentation
Citation preview

Biliary ConditionsNUR-224

OBJECTIVES• Discus management of patient with
cholelithiasis.• Use the nursing process a framework for care of
–patients with cholelithiasis and undergoing laparoscopic or open cholecystectomy.• Differentiate between acute and chronic
pancreatitis.• Describe the nursing management of patients
with acute pancreatitis.

GALLBLADDER• Pear shaped organ• Stores 30-50 mL of bile• Collects, concentrates and stores bile until
needed for digestion.• Releases bile into the duodenum via the
common bile duct when fat is present.


BILIARY CONDITIONS• Extremely common• Interfere with the normal drainage of
bile into the duodenum• 2 common problems: a. Cholecystitis b. Cholelithiasis • Common in Caucasians/Native
Americans

Risk Factors
• Sedentary lifestyle•Obesity
•Multiparous women

CHOLECYSTITIS• Acute inflammation of the gallbladder
May result from stones may obstructing the outflow of bile
S/S pain in the ® upper abdomen that may radiate to the ® shoulder, tenderness, rigidity ® upper abdomen

CHOLECYSTITISAcalculousAcalculous Gallbladder inflammation
without gallstones/absence of obstruction
Occurs after major surgical procedures, severe trauma & extensive burns

CHOLECYSTITIS
Calculous• Gallbladder inflammation &
stones that obstruct bile flow • Occurs in 90% of the clients

CHOLELITHIASISCalculi/gallstones— form from the solid constituents of
bile vary greatly in size, shape &
composition increasing prevalent after 40 yrs. of
age; esp. women

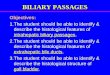
GALLSTONES

PATHOPHYSIOLOGY• Two major types of gallstones: Pigment StonesCholesterol Stones

CHOLESTEROL STONES• Account for 80% of gallbladder
disease .• There is a decrease in bile salts & an
increase in cholesterol. • Cholesterol saturated bile causes
gallstones.• This acts as an irritant that produces
inflammatory changes in the gallbladder.

CHOLESTEROL STONES• Are 2-3x more common in women.• Incidence increases with clients with diabetes.• Stones are usually smooth & are whitish yellow to tan in color.


CLINICAL MANIFESTATIONS

PAIN/BILIARY COLIC• Classic symptom• Spasms occur in order to move the
stone through the duct.• Excruciating ® upper abdominal pain• May occur 3-6 hours after a heavy
meal• May require analgesics meperidine

JAUNDICE• Appears when the Common Bile Duct
(CBD) obstruction is present.• Bile is no longer carried to the
duodenum– absorbed in the blood.• Pruritus • Concentration of bilirubin > 2.5

VITAMIN DEFICIENCY• Obstruction of bile flow interferes with
absorption of fat soluble vitamins intestines.• Vitamin A, D, E, K, deficiencies may be
seen.

CHANGES in URINE & STOOL COLOR
• Urine takes on a very dark color.• Stool no longer with bile pigments

DIAGNOSTIC FINDINGS
• Abdominal x-ray• Ultrasonography• Endoscopic Retrograde
Cholangiopancreatography – ERCP * nursing implications

ERCP• Flexible fiberoptic endoscope that
allows for visualization of the hepatobiliary system/place stents.• 90% of the clients do well with this
procedure.• The stone may be extracted or left in
the duodenum to pass naturally.




MEDICAL MANAGEMENTMajor Objective:1. Reduce the episode of gallbladder
pain & inflammation by supportive & dietary management.
2. Remove the cause of cholecystitis by pharmacological therapy, endoscopic procedures or surgical interventions.

NUTRITIONAL & SUPPORTIVE THERAPY
• Low- fat diet • Foods to avoid • Remind client that fatty foods may
bring on an episode of cholecystitis.

PHARMACOLOGIC THERAPY• Cholestyramine (Questran)• Urosdeoxycholic acid (Actigall) &
Chenodiol (Chenix) are medications used to dissolve small gallstones/composed of primarily cholesterol .• 6-12 months of therapy is required to
dissolve stones.• Indicated for clients who refuse
surgery/surgery is to risky.

NONSURGICAL REMOVAL of GALLSTONESExtracorporal Shock Wave Lithotripsya. Noninvasive procedureb. Uses repeated shock waves to
disintegrate gallstones.c. Requires no incision & no
hospitalization.d. Has been replaced – Laproscopic
Cholecystectomy


SURGICAL MANAGEMENTDone to:a. Relieve persistent symptomsb. Remove the cause of the biliary colicc. Treat acute cholecystitis

LAPROSCOPIC CHOLECYSTECTOMY• Standard of care for Rx. of gallstones.• Small incision is made through the
abdominal wall at the umbilicus.• 4 small incisions are made through the
abd. wall to introduce other surgical instruments.• Abdomen is insufflated with carbon
dioxide – assists in visualizing abd. structures.

LAPROSCOPIC CHOLECYSTECTOMY
Advantages :a. Short hospital stayb. Less invasive /shorter healing timec. Less post-op pain/less opiod used. Early ambulation e. Able to resume full activity in about 3-
4 days.f. Incision care is minimal



CHOLECYSTECTOMY• Gallbladder is removed through
abdominal incision.• Drain may be placed – near the gall
bladder bed & brought out through a puncture site for drainage.• Drain usually kept in placed for 24 hrs.
then removed.

CHOLECYSTECTOMYPost-op Nursing Interventions:• Relieve the pain • Improve the respiratory status• Improve the nutritional status• Skin integrity/drainage

NURSING INTERVENTION• Fowler’s position• May have NGT • NPO until bowel sounds return, then a soft,
low-fat, low-carbohydrate, high protein diet postoperatively• Care of biliary drainage system• Administer analgesics as ordered and
medicate to promote/permit ambulation and activities, including deep breathing • Turn, and encourage coughing and deep
breathing, splinting to reduce pain • Ambulation

Patient Teaching• Medications• Diet: at discharge, maintain a nutritious diet and
avoid excess fat. Fat restriction is usually lifted in 4–6 weeks.
• Instruct in wound care, dressing changes, care of T-tube
• Instruct patient and family to report signs of gastrointestinal complications, changes in color of stool or urine, fever, unrelieved or increased pain, nausea, vomiting, and redness/edema/signs of infection at incision site


PANCREAS• Located in upper abdomenFunctions• Exocrine function• Secrete digestive enzymes into the GI tract
through the pancreatic duct.• Amylase, trypsin, lipase
• Endocrine function• secretes insulin, glucagon, and somatostatin
directly into the blood stream

Pancreatitis• Characterized by the release of
pancreatic enzymes into the tissue of the pancreas itself hemorrhage and necrosis• Can be acute or chronic• Hospitalizations for acute pancreatitis
have increase over the last 15 years• Alcoholism and gall stones are the
primary risk factors.

Acute Pancreatitis• The pancreatic duct becomes obstructed
and enzymes back up into the duct, causing auto digestion and inflammation of the pancreas.• Minimal organ dysfunction is present.• Characterized by edema and inflammation
which is confined to the pancreas.• Affects all ages – common in middle-aged
men/women• 3x higher in Afro-Americans than
Caucasians

Risk Factors
• Gallstones – leading cause• Alcoholism• Trauma• Infection -- viral

Acute Pancreatitis• Self- digestion of the pancreas by its own
enzymes especially trypsin.
• This causes injury to the pancreatic cells or activation of the pancreatic enzymes in the pancreas rather than the intestines.
• Activated trypsin is in the pancreas. This enzyme can digest the pancreas and can activate other proteolytic enzymes.

Acute PancreatitisClinical Manifestations• Abdominal pain• Pain not relieved not by vomiting• Abdominal tenderness with muscle
guarding• Bowel sounds may be absent/diminished• Hypotension, fever, jaundice

Acute PancreatitisAssessment/Diagnostic Findings• Serum amylase and lipase levels
increased• Other findings – increase in liver
enzymes, bilirubin, triglycerides .• X-rays of the chest and abdomen• Abdominal ultrasound

Acute Pancreatitis Nursing managementRelieve pain and discomfort• Parenteral opioids• Nonpharmacologic interventions• Bedrest• Frequent oral care• NGT suction • Clouded sensorium

Acute PancreatitisNursing managementImprove breathing patterns• Semi-Fowler’s position• Change in position• Monitor pulse oximetry • C,DB/Incentive Spirometry

Acute PancreatitisNursing ManagementImprove nutritional status• Oral food/fluid intake in not permitted.• Monitor lab results/daily weights• Avoid heavy meals/alcoholic beverages• Diet – high CHO, low fats, low proteins.

CHRONIC PANCREATITIS• Progressive inflammatory disorder with
destruction of the pancreas. • Cells are replaced by fibrous tissue. • Repeated attacks of pancreatitis occur
that increase pressure within the pancreas. • Obstruction of the pancreatic and
common bile ducts and destruction of the secreting cells of the pancreas occur.

CHRONIC PANCREATITISEtiology• Excessive and prolonged alcohol
consumption• Malnutrition • Median age 35-45 years old

PANCREATITISacute
• Severe abdominal pain• Patient appears acutely ill• Abdominal guarding• Nausea and vomiting• Fever, jaundice,
confusion, and agitation may occur
• Ecchymosis in the flank or umbilical area may occur
• May develop respiratory distress, hypoxia, renal failure, hypovolemia, and shock
chronic
• Recurrent attacks of severe upper abdominal and back pain accompanied by vomiting• Weight loss• Steatorrhea

Chronic Pancreatitis
Assessment /Diagnostic Findings• Serum lipase and amylase slightly
elevated• Serum bilirubin increased• ERCP makes the diagnosis• Stool samples

Chronic PancreatitisGoals• Prevent further attacks• Relief of pain• Control of pancreatic
endocrine/exocrine insufficiency

Chronic PancreatitisNonsurgical management• Diet • Pancreatic enzyme products• Antacids/H2 antagonists

Chronic PancreatitisSurgical Management• Choledochojejunostomy • Roux-en-Y