Embed Size (px)
Citation preview

Bilateral Vestibulopathy: Clinical Characteristics andDiagnostic Criteria
*†Seonhye Kim, *Young-Mi Oh, ‡Ja-Won Koo, and *Ji Soo Kim
*Department of Neurology, Seoul National University College of Medicine, Seoul National University BundangHospital, Gyeonggi-do; ÞDepartment of Neurology, Pusan National University School of Medicine, PusanNational University Yangsan Hospital, Yangsan; and þDepartment of Otolaryngology, Seoul NationalUniversity College of Medicine, Seoul National University Bundang Hospital, Gyeonggi-do, Korea
Objectives: To define clinical and laboratory characteristics ofbilateral vestibulopathy (BV) and to propose diagnostic criteriaof this disorder based on clinical and laboratory findings.Study Design: Retrospective case series review.Materials and Methods: We recruited 108 patients with a clin-ical suspicion of BV based on presenting symptoms (unsteadi-ness or oscillopsia during locomotion) and bedside (dynamicvisual acuity or head impulse tests) and laboratory (bithermalcaloric or rotatory chair tests) findings after excluding the patientswith other disorders that may explain the symptoms. Definitediagnosis of BV was made when the patients showed abnormalfindings on both bedside and laboratory tests in addition to thesymptoms, whereas probable diagnosis was obtained when eitherthe bedside or laboratory findings were abnormal along with thesymptoms.Results: All patients had unsteadiness, and 36 (33%) reportedoscillopsia. Diminished vestibulo-ocular responses to head im-
pulse in both horizontal directions were present in 45 of the 100patients evaluated. Dynamic visual acuity was impaired in 65(95%) of the 68 patients who underwent testing. Fifty-one(57%) patients showed bilateral hyporesponsiveness during bi-thermal caloric tests. Forty-eight (53%) patients had reducedgain of the vestibulo-ocular reflex during rotatory chair test.By adopting our diagnostic criteria, 93 patients (86%) werediagnosed as having BV, definite in 49 (45%), and probable in44 (41%).Conclusion: The proposed diagnostic criteria encompassthe symptoms and findings of both bedside and laboratoryevaluations and may provide a valuable tool for investigat-ing BV. Key Words: Bilateral vestibulopathyVOscillopsiaVUnsteadinessVVertigoVVestibulo-ocular reflex.
Otol Neurotol 32:812Y817, 2011.
Bilateral vestibulopathy (BV) is characterized by os-cillopsia and unsteadiness, mostly during locomotion(1Y5). Although various diagnostic tools have been pro-posed, BV remains a diagnostic challenge because eachdiagnostic test has its own limitation without unifieddiagnostic criteria. For example, absent or reduced re-sponses during bithermal caloric stimulation have been
adopted as a diagnostic criterion of BV (6Y8). However,because caloric stimulation corresponds to a sinusoidalstimulus frequency of 0.003 Hz and does not reflectnatural rotational frequency of the head during locomo-tion (8,9), bilateral absence of caloric responses does notnecessarily indicate a complete absence of the vestibularfunction (10). Reduced gain, increased phase lead, andshortened time constants of the vestibulo-ocular reflex(VOR) in response to low-frequency rotation are char-acteristic of BV (11Y14). However, the highest rotationalfrequency achievable is less than 1.0 Hz in most equip-ment commercially available for human study (15). Afew studies embraced clinical symptoms and bedsideneurologic examinations, such as head impulse (HIT) ordynamic visual acuity (DVA) test, for diagnosis of BV(7,16Y20). HIT is useful in detecting vestibular hypo-function in BV (21). However, covert saccades mayconceal BV even in patients with total vestibular loss(21). DVA has been used as an indirect indicator for
Address correspondence and reprint requests to Ji Soo Kim, M.D.,Ph.D., Department of Neurology, College of Medicine, Seoul NationalUniversity, Seoul National University Bundang Hospital, 300 Gumi-dong,Bundang-gu, Seongnam-si, Gyeonggi-do, 463-707, Korea; E-mail: [email protected] statistical analyses were conducted by Seonhye Kim, MD,
Department of Neurology, Seoul National University Bundang Hospital,in consultation with Medical Research Collaborating Center SeoulNational University Hospital.This study was supported by a grant from the Korea Health 21 R&D
Project, Ministry of Health & Welfare, Republic of Korea (A080750).The authors report no disclosure.
Otology & Neurotology32:812Y817 � 2011, Otology & Neurotology, Inc.
812
Copyright © 2011 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.

effectiveness of the VOR in stabilizing gaze during headrotation (22,23). DVA may be a better measure of func-tional vestibular impairments and can be easily performed(24). However, DVA test can display false-negative re-sults when other mechanisms compensate for the retinalinstability during head movements (7). Accordingly, di-agnosis of BV should be based on comprehensive eva-luation of the vestibular function using both clinical andlaboratory findings. Nevertheless, no study has attemptedto incorporate all these clinical symptoms, bedside ex-amination, and laboratory tests in diagnosing BV. In thisstudy, we propose diagnostic criteria of BV that incorpo-rate both clinical and laboratory findings.
MATERIALS AND METHODS
SubjectsAt the Dizziness Clinic of Seoul National University Bundang
Hospital, 108 consecutive patients with unsteadiness or oscil-lopsia only during locomotion had been recruited from May2003 to February 2007. We reviewed the medical records ofthe patients and performed an additional telephone interviewin 64 patients whose medical records did not include sufficientinformation on the symptoms and possible causes of vestibu-lopathy. We especially excluded the patients with unsteadinessor oscillopsia because of cerebellar disorders without bilateralvestibular failure, intoxication, phobic postural vertigo, vestibularparoxysmia, perilymph fistula, orthostatic hypotension, hyper-ventilation syndromes, visual disorders, and unilateral vestibularloss (16). Most patients underwent evaluation of the vestibularfunction, including HIT, bithermal caloric, and rotatory chair testsin addition to routine neurologic and otologic examinations by theauthors (J. W. K. and J. S. K.). However, DVA was measuredonly in 68 (63%) patients because it was applied only by a neu-rologist (J. S. K.).
Head Impulse TestHIT was performed manually with rapid rotation of the head
of approximately 20-degree amplitude in the yaw plane. HIT wasconsidered abnormal if an obvious corrective saccade supple-mented the inadequate slow phase in both directions (21,25).
Dynamic Visual Acuity TestDVA was measured with a Rosenbaum card which was held
14 inches from the eyes. Reference visual acuity was determinedduring head stabilization. After then, the patient was again sub-jected to measurement of visual acuity, whereas the head wasoscillated approximately at 2.5 Hz in the horizontal plane withestimated amplitudes of 10 degrees. Loss of 3 or more lines ascompared with the reference level was considered abnormal (1).
Bithermal Caloric TestsThe caloric stimuli comprised alternate irrigation for 25 seconds
with 50 ml of cold and hot water (30-C and 44-C) (25). Nystagmuswas recorded binocularly using video-oculography (NCI-480; ICSMedical, Schaumburg, IL, USA). BV was defined by summatedslow phase velocity (SPV) of the nystagmus of less than 20 degreesper second during 4 stimulation conditions.
Rotatory Chair TestRotatory chair test were performed in darkness using a
rotatory chair system (CHARTR; ICS Medical, Dallas, TX,
USA). Detailed methods and normative data were describedelsewhere (26).
Diagnostic Criteria of BVWe proposed our own diagnostic criteria for BV, which
incorporated symptoms (Criteria 1, unsteadiness or oscillopsiaduring locomotion), results of bedside evaluation (Criteria 2,HIT or DVA) and laboratory tests (Criteria 3, bithermal caloricor rotatory chair tests), and absence of other causes (Criteria 4;Table 1). Definite diagnosis of BV was made when the patientsmet all 4 diagnostic criteria, whereas probable diagnosis wasobtained when the patients experienced the symptoms (Criteria 1)without other identifiable causes (Criteria 4) and exhibited ab-normal results during either the bedside (Criteria 2) or laboratorytests (Criteria 3).
Evaluation of Diagnostic PropertiesWe also compared the diagnostic yield of our criteria with
those reported previously (2,6,7,10,18,19,27). Selection of thesecriteria was based on similarities of the testing methods forbithermal caloric and rotatory chair tests. To evaluate sensitivityand specificity of each diagnostic criteria, we plotted receiveroperating characteristic (ROC) curves with true positives on thevertical axis (sensitivity) and false positives on the horizontalaxis (1-specificity). The area under the curve is a quantitativemeasure of the test capacity. The area under the curve value of0.5 indicates that the true-positive rate equals the false-positiverate, and the test result is not better than a chance. Becauseconfirmatory tests are not available for BV, we were unable toplot the ROC curves for our diagnostic criteria. Instead, weestimated the sensitivity and specificity of the previouslyadopted diagnostic criteria (Models 2Y6) using our own criteriaas a reference standard.
Statistical AnalysesWe used t test to compare the continuous variable (age) and
W2 test for dichotomous variable (sex) between the groups.
Spearman’s correlation also was used to compare the VOR gainduring rotation at 0.04 Hz and summated SPV during bithermalcaloric tests. All tests were performed using SPSS (version 15;SPSS, Inc., Chicago, IL, USA), and p G 0.05 was consideredsignificant.
TABLE 1. Proposed diagnostic criteria forbilateral vestibulopathy
Criteria 1. Symptoms only during locomotion (either A or B)A. UnsteadinessB. Oscillopsia
Criteria 2. Findings of bedside evaluations (either A or B)A. Positive head impulse test in both horizontal directionsB. Impaired dynamic visual acuity
Criteria 3. Results of laboratory tests (either A or B)A. Reduced responses (summated slow phase velocity of the
nystagmus G20 degrees per second) during bithermal calorictests
B. Reduced vestibulo-ocular reflex gain during rotatory chair testCriteria 4. Other causes excluded
Definite diagnosis: met all 4 diagnostic criteria.Probable diagnosis: met the criteria 2 or 3 in addition to Criteria 1
and 4.
813BILATERAL VESTIBULOPATHY
Otology & Neurotology, Vol. 32, No. 5, 2011
Copyright © 2011 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.

RESULTS
Demographic and Clinical CharacteristicsPatients included 60 women and 48 men without dif-
ference in age between women and men (Table 2). Therewas no difference in age and sex between the idiopathicand secondary groups (Table 2). Other clinical char-acteristics and causes were summarized in Table 2.
Bedside and Laboratory Vestibular Function TestsHorizontal HIT was performed in 100 patients, and 45
of them showed corrective catch-up saccades in bothdirections, whereas 17 patients exhibited positive resultsonly unilaterally. DVA was impaired in 65 (96%) of the68 patients tested.
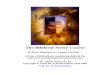
Bithermal caloric tests showed reduced response in 51(57%) of 89 patients, including no response in 4 of them.Results of rotatory chair test were abnormal in 48 (53%)of 91 patients (Fig. 1). All the patients with abnormalrotatory responses exhibited reduced gain and increasedphase leads during lower (0.02 and 0.04 Hz) frequencyrotations, and most of them (n = 42 [88%]) also showedabnormalities during higher (0.08, 0.16, and 0.32 Hz)frequency rotations (Fig. 1). The summated SPV of thenystagmus induced during bithermal caloric stimulishowed a positive linear correlation with the VOR gain at0.04 Hz during rotatory stimulation (Spearman’s corre-lation, r = 0.670, p G 0.001; Fig. 2).
Evaluation of Diagnostic PropertiesAccording to our diagnostic criteria, 44 (40.7%)
patients met the definite criteria of BV, whereas 49(45.4%) had the diagnosis of probable BV (Table 3).Overall, definite or probable diagnosis of BV could be
TABLE 2. Clinical characteristic and causes ofbilateral vestibulopathy
Patients age Mean T SD Range p value
Total (n = 108) 62.9 T 16.4 12Y88Men (n = 48) 62.7 T 17.8 12Y88 90.05Women (n = 60) 63.2 T 15.4 18Y88Idiopathic group (M:W = 23:21) 65.4 T 16.5 15Y86 90.05Secondary group (M:W = 37:27) 61.3 T 16.3 12Y88
Clinical symptoms No. Percentage (%)Unsteadiness 108 100Oscillopsia 36 33Transient vertigo 30 28Bilateral hearing loss 20 19Tinnitus 13 12
CausesIdiopathic 51 47.2Secondary 57 52.8Ototoxicity 21 19.4Bilateral Meniere’s disease 12 11.1Bilateral sequential vestibular
neuritis4 3.7
Head trauma 4 3.7Bilateral chronic otitis media 1 0.9Autoimmune disorder 1 0.9Neurologic diseases 14 13.0Central nervous system
infection(3)
Cerebellar infarction (2)Cerebellar degeneration (2)Superficial siderosis (3)Tumor (2)Neuropathy (2)
FIG. 1. Gains of the VOR in 48 patients that exhibited reducedgains during sinusoidal harmonic accelerations. All of themshowed reduced gain at lower (0.02 and 0.04 Hz) frequencyrotations, and most of them (n = 42 [88%]) also exhibited dimin-ished gain at higher (0.08, 0.16, and 0.32 Hz) frequency rotations.The gray box indicates reference ranges (mean, T2 standarddeviation) of the VOR gain at each frequency.
FIG. 2. The summated SPV of the nystagmus induced duringbithermal caloric stimuli shows a positive linear correlation withthe gain of the VOR during sinusoidal harmonic acceleration at0.04 Hz with a peak velocity of 50 degrees per second (r = 0.670,p G 0.001).
814 S. KIM ET AL.
Otology & Neurotology, Vol. 32, No. 5, 2011
Copyright © 2011 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.

made using our criteria in 93 (86.1%) of 108 patientsthat experienced unsteadiness or oscillopsia only duringlocomotion without other identifiable disorders. Whenapplying the previously reported diagnostic criteria,diagnosis of BV could be made in 3.4% to 58.6% of thepatients that underwent the tests adopted in those criteria(Table 3). We also determined the sensitivity and speci-ficity of the previously reported criteria using our criteriaas a reference standard (2,6,7,10,18,19,27). The sensi-tivity of the previous criteria ranged from 3.0 to 64.6%,whereas the specificity was uniformly 100% (Table 3).
DISCUSSION
In this study, we proposed diagnostic criteria of BVthat incorporated clinical symptoms and results of bothbedside examination and laboratory tests. Using our cri-teria, we were able to diagnose BV in 86% of the patientswith oscillopsia and unsteadiness only during locomotionafter excluding the patients with other disorders that mayexplain the symptoms.
In BV, the most common and most important com-plaints are unsteadiness and oscillopsia during locomo-tion. The unsteadiness typically worsens in darkness oron uneven surfaces (5,16). Unsteadiness is a reflectionof impaired vestibulo-spinal reflex, hindering the multi-sensory process of postural control (28). Unsteadiness alsooccurs with high-frequency head movements because de-tection of high-frequency head rotation is a domain of thevestibular apparatus (28,29). Oscillopsia also occurs in BV
because of bilaterally impaired VOR that reduces stabili-zation of the images on the retina (retinal slip) during lo-comotion and head movements (1,16). All our patientsexperienced unsteadiness during locomotion. However,only 36 (33%) of them reported oscillopsia. In the previ-ous reports, the oscillopsia also was described in only 25%to 50% of the patients with BV (1). In patients with ves-tibular disorders, the degree of subjective complaints maynot follow the severity of vestibular dysfunction measuredusing objective tests (1). Impaired VOR may be compen-sated by other mechanisms (7,30Y32).
Caloric and rotatory chair tests have been adoptedin diagnosing BV (1,2,4,6,13,14). However, absent re-sponses during bithermal caloric stimulation does notnecessarily indicate a complete loss of the vestibular func-tion (33). To determine any vestibular function remained,previous studies introduced ice-water stimulation in case ofabsent responses during bithermal caloric irrigation (6,7,34).However, ice-water irrigation is unpleasant and painful andmay produce pseudocaloric nystagmus by activating latentspontaneous nystagmus (35,36). Furthermore, there hasbeen no consensus on the range of responses (nystagmus)required for diagnosis of BV during caloric stimulation(1,27,37).
Rotatory chair test adopts more physiologic stimuli over abroad frequency range and has been regarded a bettermethod for identifying patients with BV (10,13,38Y40).However, commercially available rotatory chairs forhuman study do not readily evaluate the VOR at fre-quencies above 1 Hz where the head usually oscillates
TABLE 3. Diagnostic accuracy of our own and previously proposed criteria for bilateral vestibulopathy
Model Diagnosis of BV (%) Sensitivity (%)a Specificity (%)a AUC
Model 1 93/108 (86.1)1. Unsteadiness or oscillopsia2. DVA or HIT3. Caloric test (reduced caloric responses G20 degrees per second)
or rotatory chair test (decreased gain at lower frequency stimulation: G0.2)Definite (n = 44)Probable (n = 49)
h Definite: 1 + 2 + 3 and other causes were excludedh Probable: 1 + either 2 or 3 when other causes were excluded
Model 2 (6,7) 3/87 (3.4) 5.1 100 0.525Absent caloric response
Model 3 (27) 51/87 (58.6) 64.6 100 0.823Reduced caloric response (G24 degrees per second)
Model 4 (2) 4/77 (5.2) 17.7 100 0.589Absent or reduced caloric response (SPV, G5 degrees per second)+Decreased gain at low-frequency rotatory chair test
Model 5 (10) 10/77 (13.0) 13.7 100 0.586Absent or reduced caloric response (SPV, G10 degrees per second)+Decreased gain (0.1) at low-frequency rotational chair test
Model 6 (18,19) 46/79 (58.2) 63.0 100 0.815HIT + absent or reduced caloric response (SPV, G5 degrees per second)h Complete: pathologic HIT + absence of caloric responseh Incomplete; Complete (n = 3)1. Bilateral pathologic HIT + reduced caloric response
(SPV, G5 degrees per second)Incomplete (n = 43)
2. Bilateral pathologic HIT + caloric responses 95 degrees per secondon 1 or both sides
3. Normal HIT + absence or reduced caloric responses (G5 degrees per second)
AUC indicates area under the curve; BV, bilateral vestibulopathy; DVA, dynamic visual acuity; HIT, head impulse test; SPV, slow phase velocity.aReceiver operating characteristic curves were used to measure the sensitivities and specificities of the previously reported diagnostic criteria using our
own criteria as reference standards.
815BILATERAL VESTIBULOPATHY
Otology & Neurotology, Vol. 32, No. 5, 2011
Copyright © 2011 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.

during daily activities (15,41). Thus, it would be inade-quate to determine the vestibular dysfunction with onlythe results of caloric or rotatory chair test. Indeed, reducedcaloric responses were observed only in 57% and de-creased VOR gain in 52% of our patients with unsteadi-ness and oscillopsia only during locomotion.
HIT and DVA can evaluate the VOR function at thephysiologic head oscillation frequencies during locomo-tion (20,21,40,42). However, only a few previous studiesadopted the results of HIT or DVA for diagnosis of BV(16Y18,43). In the present study, the sensitivity of DVAwas 96% during passive head rotation, which was higherthan that (66%Y75%) in the previous studies (1) and wassimilar to that of computerized DVA (20). DVA is knownto decline with aging both in healthy persons and inpatients with BV, although there are no reference valuesby age for the clinical DVA test (20). Because the averageage of our patients (63 yr) was higher than that of theprevious study (54 yr) (1), inclusion of more aged patientsmay explain the higher proportion of abnormal DVA inthis study. Also, false negatives are unknown for the largenumber of patients who did not have DVA test.
Our diagnostic criteria for BV improved diagnosticyields of this disorder (Table 3). Previously, most studieshad adopted the results of only caloric or rotatory chairtest in diagnosing BV (6,7), which would have resultedin lower sensitivity. Especially, adoption of absent re-sponses or summated SPV below 5 degrees per secondduring bithermal caloric stimulation would have loweredthe sensitivity further (Table 3). During caloric stimula-tion, we estimated the positive likelihood ratio of thesummated SPV using ROC with decreased gains at lowerfrequency rotations as a reference standard. We foundthat likelihood ratio was highest when the summated SPVof the nystagmus was below 20 degrees per second. Thus,we adopted the value of less than 20 degrees per secondas an indicator for decreased VOR function during bi-thermal caloric tests.
This study had some limitations. First of all, we de-termined the abnormality of HIT bedside without quan-titative analyses. Bedside HIT is less sensitive thanquantitative HIT especially when the vestibular deficitsare partial (44). Also, covert saccades during HIT maymask the corrective catch-up saccades and prevent accu-rate identification of the vestibular impairments (21,45).However, bedside HIT is feasible, and the sensitivity isclinically acceptable in the hands of both neuro-otologicexperts and nonexperts (46). Second, the function of thevertical semicircular canals was not investigated. Giventhat the vertical HIT and DVA during vertical head oscil-lation may evaluate the function of the vertical semicircularcanals, the findings and diagnostic use of these testsshould be validated further in BV. Finally, otolithic dys-function remains an area of further exploration in BV. Thesaccular function, as determined by cervical vestibularevoked myogenic potential, may be impaired in BV (47).In patients with suspected BV, cervical vestibular evokedmyogenic potential may be abnormal bilaterally in thepresence of normal caloric responses (48).
REFERENCES
1. McGath JH, Barber HO, Stoyanoff S. Bilateral vestibular loss andoscillopsia. J Otolaryngol 1989;18:218Y21.
2. Telian SA, Shepard NT, Smith-Wheelock M, Hoberg M. Bilateralvestibular paresis: diagnosis and treatment. Otolaryngol Head NeckSurg 1991;104:67Y71.
3. Vibert D, Liard P, Hausler R. Bilateral idiopathic loss of peripheralvestibular function with normal hearing. Acta Otolaryngol 1995;115:611Y5.
4. Rinne T, Bronstein AM, Rudge P, Gresty MA, Luxon LM. Bilateralloss of vestibular function: clinical findings in 53 patients. J Neurol1998;245:314Y21.
5. Baloh RW, Honrubia V. Clinical Neurophysiology of the Ves-tibular System. New York, NY: Oxford University Press, 2001:125Y6.
6. Simmons FB. Patients with bilateral loss of caloric response.Ann Otol Rhinol Laryngol 1973;82:175Y8.
7. Chambers BR, Mai M, Barber HO. Bilateral vestibular loss, oscil-lopsia, and the cervico-ocular reflex. Otolaryngol Head Neck Surg1985;93:403Y7.
8. Honrubia V, Marco J, Andrews J, Minser K, Yee RD, Baloh RW.Vestibulo-ocular reflexes in peripheral labyrinthine lesions: III.Bilateral dysfunction. Am J Otolaryngol 1985;6:342Y52.
9. Hamid MA, Hugher GB, Kinney SE. The Vestibular System:Neurophysiologic and Clinical Research. New York, NY: RavenPress, 1987:115Y8.
10. Furman JM, Kamerer DB. Rotational responses in patients withbilateral caloric reduction. Acta Otolaryngol 1989;108:355Y61.
11. Rinne T, Bronstein AM, Rudge P, Gresty MA, Luxon LM. Bilateralloss of vestibular function. Acta Otolaryngol Suppl 1995;520(Pt 2):247Y50.
12. Baloh RW, Hess K, Honrubia V, Yee RD. Low and high frequencysinusoidal rotational testing in patients with peripheral vestibularlesions. Acta Otolaryngol Suppl 1984;406:189Y93.
13. Hess K, Baloh RW, Honrubia V, Yee RD. Rotational testing inpatients with bilateral peripheral vestibular disease. Laryngoscope1985;95:85Y8.
14. Sargent EW, Goebel JA, Hanson JM, Beck DL. Idiopathic bi-lateral vestibular loss. Otolaryngol Head Neck Surg 1997;116:157Y62.
15. Goebel JA, Hanson JM, Langhofer LR, Fishel DG. Head-shakevestibulo-ocular reflex testing: comparison of results with rotationalchair testing. Otolaryngol Head Neck Surg 1995;112:203Y9.
16. Brandt T. Bilateral vestibulopathy revisited. Eur J Med Res 1996;1:361Y8.
17. Herdman SJ, Hall CD, Schubert MC, Das VE, Tusa RJ. Recovery ofdynamic visual acuity in bilateral vestibular hypofunction. ArchOtolaryngol Head Neck Surg 2007;133:383Y9.
18. Zingler VC, Weintz E, Jahn K, et al. Follow-up of vestibularfunction in bilateral vestibulopathy. J Neurol Neursurg Psychiatry2008;79:284Y8.
19. Zingler VC, Cnyrim C, Jahn K, et al. Causative factors and epide-miology of bilateral vestibulopathy in 255 patients. Ann Neurol 2007;61:524Y32.
20. Herdman SJ, Tusa RJ, Blatt P, Suzuki A, Venuto PJ, Roberts D.Computerized dynamic visual acuity test in the assessment of ves-tibular deficits. Am J Otol 1998;19:790Y6.
21. Halmagyi GM, Weber KP, Aw ST, Todd MJ, McGarvie LA,Curthoys IS. Horizontal head impulse test detects gentamicin ves-tibulotoxicity. Neurology 2009;72:1417Y24.
22. Longridge NS, Mallinson AI. A discussion of the dynamic illegible‘‘E’’ test: a new method of screening for aminoglycoside vestibu-lotoxicity. Otolaryngol Head Neck Surg 1984;92:671Y7.
23. Burgio DL, Blakley BW, Myers SF. The high-frequency oscillopsiatest. J Vestib Res 1992;2:221Y6.
24. Demer JL, Honrubia V, Baloh RW. Dynamic visual acuity: a test foroscillopsia and vestibulo-ocular reflex function. Am J Otol 1994;15:340Y7.
25. Choi KD, Oh SY, Kim HJ, Koo JW, Cho BM, Kim JS. Recovery ofvestibular imbalances after vestibular neuritis. Laryngoscope 2007;117:1307Y12.
816 S. KIM ET AL.
Otology & Neurotology, Vol. 32, No. 5, 2011
Copyright © 2011 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.

26. Jeong SH, Oh SY, Kim HJ, Koo JW, Kim JS. Vestibular dys-function in migraine; effects of associated vertigo and motionsickness. J Neurol 2010;257:905Y12.
27. Myers SF. Patterns of low-frequency rotational responses in bilat-eral caloric weakness patients. J Vestib Res 1992;2:123Y31.
28. Glasauer S, Amorim MA, Vitte E, Berthoz A. Goal-directed linearlocomotion in normal and labyrinthine-defective subjects. ExpBrain Res 1994;98:323Y35.
29. El-Kashlan HK, Telian SA. Diagnosis and initiating treatment forperipheral system disorders: imbalance and dizziness with normalhearing. Otolaryngol Clin North Am 2000;33:563Y78.
30. Gresty MA, Hess K, Leech J. Disorders of the vestibulo-ocularreflex producing oscillopsia and mechanisms compensating for lossof labyrinthine function. Brain 1977;100:693Y716.
31. Dichgans J, Schmidt CL, Graf W. Visual input improves thespeedometer function of the vestibular nuclei in the goldfish. ExpBrain Res 1973;18:319Y22.
32. Kasai T, Zee DS. Eye-head coordination in labyrinthine-defectivehuman beings. Brain Res 1978;144:123Y41.
33. Barber HO, Stockwell CW. Manual of Electronystagmography.St Louis, MO: CV Mosby Company, 1980.
34. Schuknecht HF, Witt RL. Acute bilateral sequential vestibularneuritis. Am J Otolaryngol 1985;6:255Y7.
35. Greisen O. Pseudocaloric nystagmus. Acta Otolaryngol 1972;73:341Y3.
36. Schmal F, Lubben B, Weiberg K, Stoll W. The minimal ice watercaloric test compared with established vestibular caloric test pro-cedures. J Vestib Res 2005;15:215Y24.
37. Moller C, Odkvist LM. The plasticity of compensatory eye move-ments in bilateral vestibular loss. A study with low and high fre-quency rotatory tests. Acta Otolaryngol 1989;108:345Y54.
38. Baloh RW, Honrubia V, Yee RD, Hess K. Changes in the humanvestibulo-ocular reflex after loss of peripheral sensitivity. AnnNeurol 1984;16:222Y8.
39. Baloh RW, Jacobson K, Honrubia V. Idiopathic bilateral vestibu-lopathy. Neurology 1989;39:272Y5.
40. Fife TD, Tusa RJ, Furman JM, et al. Assessment: vestibular testingtechniques in adults and children: report of the Therapeutics andTechnology Assessment Subcommittee of the American Academyof Neurology. Neurology 2000;55:1431Y41.
41. Grossman GE, Leigh RJ, Abel LA, Lanska DJ, Thurston SE. Fre-quency and velocity of rotational head perturbations during loco-motion. Exp Brain Res 1988;70:470Y6.
42. Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. ArchNeurol 1988;45:737Y9.
43. Gillespie MB, Minor LB. Prognosis of bilateral vestibular hypo-function. Laryngoscope 1999;109:35Y41.
44. Perez N, Rama-Lopez J. Head-impulse and caloric tests in patientswith dizziness. Otol Neurotol 2003;24:913Y7.
45. Weber KP, Aw ST, Todd MJ, McGarvie LA, Curthoys IS,HalmagyiGM.Head impulse test in unilateral vestibular loss: vestibulo-ocular reflex and catch-up saccades. Neurology 2008;70:454Y63.
46. Jorns-Haderli M, Straumann D, Palla A. Accuracy of the bedsidehead impulse test in detecting vestibular hypofunction. J NeurolNeursurg Psychiatry 2007;78:1113Y8.
47. Zingler VC, Weintz E, Jahn K, et al. Saccular function less affectedthan canal function in bilateral vestibulopathy. J Neurol 2008;255:1332Y6.
48. Fujimoto C, Murofushi T, Chihara Y, Suzuki M, Yamasoba T,Iwasaki S. Novel subtype of idiopathic bilateral vestibulopathy:bilateral absence of vestibular evoked myogenic potentials in thepresence of normal caloric responses. J Neurol 2009;256:1488Y92.
817BILATERAL VESTIBULOPATHY
Otology & Neurotology, Vol. 32, No. 5, 2011
Copyright © 2011 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.





![VITAMIN E AMELIORATES THE TOXIC EFFECT OF AMIODARONE ON THYROID GLAND ... · peripheral neuropathy and thyroid dysfunction[4,5,6,7]. Recently, bilateral vestibulopathy was described](https://img.pdfslide.us/doc/110x75/5e77c33b15630f2b0e6f2b60/vitamin-e-ameliorates-the-toxic-effect-of-amiodarone-on-thyroid-gland-peripheral.jpg)