Embed Size (px)
Citation preview

CASE REPORT AND CLINICAL REVIEW
Bilateral skin fold rotation–advancement flaps for the closure oflarge lumbosacral wounds in three dogsavj_704 174..179
A Dunn,a* E Buffa,a R Mitchellb and G Huntc
Three dogs were presented for the management of disease pro-cesses resulting in large skin defects over the dorsal lumbosacralregion. One had severe dog bite wounds, one had a large burnsustained from a heating pad and one had a large myxosarcoma inthe region. In each case, the extent and location of the resultingskin defect were assessed as factors likely to prevent reconstructionusing simple tension-relieving techniques alone or in combinationwith established reconstructive techniques, such as axial patternflaps or skin stretching devices. Bilateral skin fold rotation–advancement flaps (SFRAFs) based on the flank folds were mobil-ised dorsally and allowed complete wound closure in two dogs andsubtotal closure in the other dog. All wounds healed without majorcomplications and an acceptable cosmetic outcome was achievedin each case. Minor flap debridement was required in two dogs. Theuse of bilateral SFRAFs is a useful technique alone or in combinationwith other reconstructive techniques for the closure of large dorsallumbosacral skin defects when existing techniques are not suffi-cient. Small flank folds, such as those of obese dogs, may yieldunexpectedly large SFRAFs.
Keywords dogs; flank fold; skin fold advancement flap; skinreconstruction
Abbreviations DCIA, deep circumflex iliac artery; SFRAFs, skinfold rotation–advancement flapsAust Vet J 2011;89:174–179 doi: 10.1111/j.1751-0813.2011.00704.x
Dog bite wounds, thermal and electrical burns, and neoplasiaare some of the conditions that may destroy or require sur-gical excision of extensive areas of dorsal trunk skin in the
dog.1–4 The general laxity and abundance of trunk skin varies mark-edly between breeds and individuals;1,2,4 however, the majority ofdorsal trunk wounds can be closed with simple tension-relieving tech-niques.1,2,4,5 If such techniques are insufficient to allow minimaltension closure, they may be combined with the use of skin-stretchingdevices, which mobilise local skin to the surgical site, allowing theclosure of many large trunk wounds.4,6
Wounds over the dorsal lumbosacral region are less amenable tolateral undermining and advancement, because of the less mobilelateral thigh skin, which lacks a panniculus muscle layer.7 Similarly,skin-stretching devices, which rely on a reasonable source of local skin
for wound closure,6 may be insufficient to effect tension-free closurein this area. Axial pattern flaps, or island arterial flaps, based on theventral branch of the deep circumflex iliac artery (DCIA) can be usedto cover problematic wounds in the dorsal lumbosacral region if thisvessel is intact on at least one side.8
Large dorsal lumbosacral wounds in which the both DCIAs are com-promised are uncommon, but present a significant management chal-lenge. Meshed full thickness or partial thickness free grafts can be usedto cover large trunk wounds;3,9,10 however, a lack of inherent vascularsupply, intensive postoperative wound care and inferior cosmeticoutcome make these techniques a last resort in large trunk wounds.Microvascular anastomosis of full-thickness donor skin to the deepcircumflex iliac artery is feasible;11 however, the need for specialisedequipment and training in microsurgical techniques limits the avail-ability of this technique, with the added problem of closing a large,full-thickness donor wound.
Additional techniques allowing coverage of large dorsal lumbosacralwounds with full-thickness skin may be welcomed by the surgeonfaced with extremely large lumbosacral wounds where adjacent skin isinsufficient for skin stretching, combined with bilateral compromiseof DCIAs preventing axial pattern flap use.
The purpose of this article is to describe the single session closure ofextensive wounds over the dorsal lumbosacral region in three dogswith a variation of a previously described reconstructive techniqueusing flank fold skin (Figure 1).12,13
Case reports
Surgical techniqueAn anal purse string suture was placed. The trunk caudal to the mid-thoracic level, and both hind limbs proximal to the tarsal joints, wereprepared for surgery. Sterile waterproof wraps were placed on thedistal limbs and the caudal half of the dog was draped in to thesurgical field with the dog positioned in sternal recumbency. Prepa-ration of the caudal half of the dog removed the need to prepareadditional areas of skin intraoperatively and apply fresh surgicaldrapes after each re-positioning of the dog, thus reducing the risk ofwound contamination. Tumour excision, wound debridement orscar excision were performed on the lumbosacral skin as the caserequired. The recipient bed was covered with saline-soaked abdomi-nal sponges and the caudal half of the dog rolled laterally to provideaccess to the flank fold. The flank fold attachment at the cranialaspect of the thigh was palpated to subjectively estimate the availableskin for flap formation. A sterile marker was used to mark linesalong the lateral and medial skin fold attachments to the thigh. The
*Corresponding author: Small Animal Specialist Hospital, 1 Richardson Place, NorthRyde, New South Wales, 2113, Australia; [email protected] of Sydney Veterinary Teaching Hospital, Camden, NSW, AustraliabNorth Coast Veterinary Specialists, Tanawha, Queensland, AustraliacUniversity of Sydney Veterinary Teaching Hospital, Sydney, NSW, Australia
SMALL ANIMALS
SMAL
LAN
IMAL
S
© 2011 The AuthorsAustralian Veterinary Journal © 2011 Australian Veterinary AssociationAustralian Veterinary Journal Volume 89, No 5, May 2011174

a
b
c
e
d
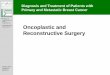
Figure 1. Diagrammatic representation of bilateral skin fold rotation–advancement flaps for closure of caudodorsal trunk wounds. (a) Lateral skinincision; A and B are reference points for the following diagrams. (b) The medial skin incision is carried proximally to the inguinal crease. (c) The flankfold is unfolded and the lateral abdominal skin undermined allowing flap rotation. Direction of flap rotation is indicated by the curved arrow in theinset diagram. Once rotated, the flap is advanced in the direction of the straight arrows. (d) Thigh wound closure is performed with gentle tension onthe flap (arrows). (e) Wound closure is completed with undermining and advancement of the cranial wound margin (arrows). The flaps may cometogether end-on as illustrated; however, care must be taken to avoid placement of this suture line directly along the dorsal spinous processes. Whereflap length permits, a side-to-side closure is preferred.
SMALL ANIMALS
SMAL
LAN
IMAL
S
© 2011 The AuthorsAustralian Veterinary Journal © 2011 Australian Veterinary Association Australian Veterinary Journal Volume 89, No 5, May 2011 175

lines converged just proximal to the stifle and care was taken toleave sufficient skin medially and laterally to allow donor bedclosure.12
The medial and lateral attachments of the flank fold were incisedalong the marked lines, with the lateral thigh incision continuingdorsally as a bridging incision to connect the donor bed to the caudaledge of the recipient bed (Figure 1a). The medial incision extendedproximally to the level of the inguinal crease to allow sufficient releaseof the flap from the upper limb (Figure 1b).
The lateral trunk skin extending from the recipient wound to the flankfold was carefully undermined deep to the panniculus muscle layer,taking care to preserve any direct cutaneous vessels. Stay sutures wereused to handle the skin edges. The double-layered flank fold wasunfolded with combined blunt and sharp dissection. The flap wasrotated and advanced on to the recipient bed (Figure 1c). The donorbed was closed in two layers by apposing the medial and lateral edgesof the thigh wound while gentle tension was placed on the flap(Figure 1d). The dog was repositioned and the contralateral flank foldreleased and the donor wound closed in an identical manner. Finally,the dog was returned to sternal recumbency. The flaps met dorsallyand were apposed either end to end (Figure 1e) or, if flap lengthpermitted, side to side. Undermining and advancement of the cranialand caudal wound margins assisted in wound closure. Wounds wereclosed in two layers: a continuous intradermal layer of absorbablesuture, such as polydioxanone, and a skin layer of interrupted non-absorbable suture, such as polypropylene, or skin staples. Fenestrateddrains were placed, the tips extending to dependent positions on thecranial thigh. The exit site was chosen so as not to interfere with bloodsupply to the base of the skin flaps. Drains were attached to closedcontinuous suction devices, and were removed in 2–5 days as dictatedby wound fluid production.
Case 1An obese 9-year-old spayed female Shetland Sheepdog weighing10.2 kg was presented for management of dog fight wounds sustainedto the trunk 4 days previously. Prior management had consisted ofamoxicillin/clavulanate 12.5 mg/kg twice daily and carprofen 2 mg/kgonce daily.
Hair was clipped from the caudodorsal trunk. An oval-shaped area ofpurple to black skin measuring 20 ¥ 17 cm was located dorsally,extend-ing from the caudal thoracic to the caudal sacral region. The lateralextents of the wound were the mid-abdominal wall on the right and thedorsal third of the abdominal wall on the left. There was purulentdischarge from multiple puncture wounds over the region. The skinhad a leathery texture and was starting to slough along a well-demarcated boundary with healthy skin. Medical management prior tosurgery included a fresh frozen canine plasma (Caniplas; Plasvacc,Kalbar, Australia) transfusion to address hypoproteinaemia, isotoniccrystalloid fluid therapy and intravenous cephazolin at 22 mg/kg.Anal-gesia was provided by a transdermal fentanyl patch delivering 50 mg/hand morphine constant-rate infusion (0.1 mg/kg/h) for the first 12 h.
Anaesthesia was induced with alfaxalone 2 mg/kg IV given 15 minafter premedication with methadone 0.2 mg/kg IV. Anaesthesia wasmaintained with isoflurane in oxygen. The wound was sharply
debrided of devitalised skin and necrotic subcutaneous fat, andlavaged with sterile saline. Both DCIAs were noted to be thrombosedand non-viable. The resulting defect measured 23 ¥ 20 cm. Open-wound management was initiated with wet-to-dry dressings changedtwice daily for the first 2 days to complete surface debridement.Ongoing open-wound management was favoured over early woundreconstruction because of the cooperative nature of the dog and theowners’ desire to avoid surgery. Sterile hydrogel (Solu-Gel; Johnsonand Johnson Medical, North Ryde, NSW, Australia) covered by a non-adherent sterile dressing (Melolin; Smith & Nephew Pty Ltd, NorthRyde, NSW, Australia) and a layer of cotton padding (Combine dress-ing; Smith & Nephew Pty Ltd) were used. Wound dressings weresecured with a tie-over dressing4 and dressings were changed every4 days or sooner if wound fluid strike-through occurred.
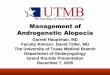
No appreciable reduction in wound size occurred beyond day 45 ofopen-wound management by which time the wound measured 13 ¥11 cm, with a central non-epithelialised area and significant tension inthe surrounding skin (Figure 2). Wound excision was performed onday 48. Skin edge recoil resulted in an increase in the wound’s dimen-sion to 16 ¥ 15 cm. Wound closure without significant tension wasperformed using bilateral SFRAFs as described above (Figure 3a, b).
By day 4 an area of skin necrosis, 0.5 cm diameter, had formed at thejunction of the advancement flaps and the caudal wound margin. Thenecrotic section was allowed to remain in situ, where it formed a hardscab under which epithelialisation had occurred by the time the scablifted off on day 14. The remainder of the wound healed withoutcomplication and sutures were removed 14 days after surgery. Hairregrowth with excellent cosmesis was evident at a 4-month postop-erative recheck (Figure 4).
Figure 2: Case 1: skin deficit after 48 days of open wound management.
SMALL ANIMALS
SMAL
LAN
IMAL
S
© 2011 The AuthorsAustralian Veterinary Journal © 2011 Australian Veterinary AssociationAustralian Veterinary Journal Volume 89, No 5, May 2011176

Case 2An obese 13-year-old male neutered Border Collie weighing 26 kgpresented with a large subcutaneous mass over the right dorsallumbosacral region. The dog was otherwise healthy. An incisionalbiopsy yielded a histological diagnosis of myxosarcoma. Magneticresonance imaging showed the tumour to be situated superficial tothe lumbar fascia. No evidence of metastases was discovered on pre-operative staging, which included haematology, serum biochemistry,thoracic radiography, abdominal ultrasound and peripheral lymphnode aspiration.
The tumour was resected with 3-cm lateral margins. Resection of thesuperficial lumbodorsal fascia, multifidus lumborum muscles anddorsal spinous processes of L3–L6 was required to obtain adequate
deep margins. The resultant skin defect was 18 ¥ 22 cm, extendingfrom the mid-lumbar to sacral region with lateral wound margins atthe level of the mid-abdominal wall. The left and right DCIA werewithin the resected tissue margins. The wound was closed directly asdescribed. A 6 ¥ 6 cm defect remained at the most cranial extent ofthe defect and was partly closed using a transposition flap from thedorsal thorax. A small area was left to heal by second intention.
In the week following surgery there was necrosis of the terminal 3 cm ofboth advancement flaps, exposing the remnants of the spinous pro-cesses. Necrotic skin was trimmed and the resultant defect had com-pletely healed after an additional 2 weeks of open-wound management.Histopathological examination of the excised tissue confirmedtumour-free margins. No tumour regrowth occurred during 2 years offollow up.
Case 3A 5-year-old female neutered Border Collie dog weighing 21 kg waspresented for management of a non-healing thermal burn woundover the dorsal lumbosacral region. The burn was sustained from aheating pad during surgery in dorsal recumbency and had beenmanaged as an open wound for 4 weeks by the referring veterinarian,by which time the wound measured 18 ¥ 22 cm. Wound closure hadbeen attempted by using a single pedicle advancement flap from thedorsal trunk. By day 10 post-surgery the terminal 50% of the flap hadbecome non-viable because of a paucity of direct cutaneous vesselssupplying the flap via the subdermal plexus.
After surgical debridement of the failed flap, the skin defect measured25 ¥ 20 cm and neither DCIA was intact.
Open-wound management with wet-to-dry dressings for 5 days wasfollowed by wound closure with bilateral SFRAFs. Multiple tension-relieving stab incisions were made in the skin bordering the cranialaspect of the wound to facilitate wound closure. Negative pressure
a b
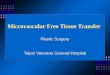
Figure 3. Case 1: postoperativeappearance. (a) Note that the medialflank fold skin incision (see Figure 1b)has extended into the inguinal region,enabling complete division of theflank fold from the limb and reducingthe tension on the wound edgesduring ambulation. (b) The right skinfold rotation–advancement flap(SFRAF) was smaller than the leftbecause of the extension of thewound to the level of the right lateralmid-abdominal wall.
Figure 4. Case 1: appearance at 4 months after surgery.
SMALL ANIMALS
SMAL
LAN
IMAL
S
© 2011 The AuthorsAustralian Veterinary Journal © 2011 Australian Veterinary Association Australian Veterinary Journal Volume 89, No 5, May 2011 177

could not be maintained with a continuous suction device, because ofthe presence of the relieving incisions, so Penrose drains covered withsterile dressing were use to provide wound drainage. Drains wereremoved 5 days post-surgery.
A 2 ¥ 2 cm area of skin necrosis was present at the tip of the right flapby postoperative day 6. It was debrided and re-sutured under generalanaesthesia. Further wound healing was uneventful, with all suturesremoved 14 days post-surgery. The cosmetic outcome was consideredexcellent at 6-month recheck.
Discussion
Canine skin is abundant, with a high dermal elastin concentration,14
so healing of skin wounds by contraction and epithelialisation is oftensuccessful. In the case of large trunk wounds the force of myofibro-blast contraction is often equalled by tension in the surrounding skinprior to skin edge apposition, and large unsightly scars that are proneto trauma and solar dermatitis are common.15 Vacuum-assistedwound closure has been used to hasten granulation tissue formationin large trunk wounds prior to reconstruction16,17 and may havereduced the period of wound management prior to reconstruction incase 1; however, vacuum-assisted wound closure does not replacereconstructive surgery of large wounds.
Of the many skin closure techniques at the disposal of the surgeon, thesimplest and safest technique that allows wound closure and restora-tion of function should be chosen. The scale of the skin defects in eachof the present cases prevented wound closure using simple tension-relieving techniques such as undermining and advancement withwalking sutures.1,2,4,5 Skin-stretching devices in combination withsimple tension-relieving techniques are useful for wounds in the tho-racolumbar region when the pre-surgical assessment of skin elasticitysuggests there is sufficient local skin.6 In each of the clinical casesdescribed here, a significant portion of the wound was over the iliumand sacrum, with taut lateral skin margins, and after careful preopera-tive skin tension assessment it was considered that the use of the flankfolds represented the best opportunity for single-session woundclosure. Skin-stretching devices could have been used prior to or afterthe surgery was performed in these cases and may have facilitatedcomplete wound closure and prevented flap tip necrosis in case 2by maximising flap elongation via mechanical creep and stressrelaxation.6
If the ventral branch of the DCIA is intact, unilateral or bilateral axialpattern flaps or island flaps based on this vessel can be used to closedorsal and lateral wounds in the lumbosacral region;8 however, ineach of these three cases the DCIAs could not be salvaged eitherbecause of the primary disease process (cases 1 and 3) or because bothDCIAs were within the resected tumour margins (case 2).
Simultaneous bilateral caudal superficial epigastric axial pattern flapshave been used for wound reconstruction.18 This technique has notbeen reported for closure of dorsal trunk wounds and although flapdimensions may have been adequate to permit wound closure, donorbed closure in the patients described here would not have been pos-sible without creating extreme tension at the wound reconstructionsite. An axial pattern flap based on bilateral lateral caudal arteries of
the tail has been described in dogs.19 However, based on the descrip-tions of flap dimensions in experimental dogs,20 this technique wouldnot have allowed wound closure in our cases. A full-thickness, freemeshed graft combined with an omental pedicle graft has been used tocover a comparable caudodorsal trunk wound in an obese dog.3 Thattechnique required two major procedures in addition to surgicaldebridement, with 66 days of bandaging after wound reconstruction,thus showing no advantage over the technique described here. Partialthickness, meshed free grafts have been used to cover large trunkdefects, but hair growth over both donor and recipient beds is sparseat best, leading to poor cosmesis compared with techniques that usefull-thickness skin.9,10
Skin fold flaps based on the flank and axillary folds were initiallydescribed for the coverage of large ventral trunk defects in dogs andcats,12 and later shown to be useful in the closure of proximal limb andlateral trunk defects.13 The novel dorsal use of bilateral SFRAFsallowed the complete closure of substantial dorsal lumbosacralwounds in cases 1 and 3, and subtotal closure of the wound in case 2.
A skin fold flap has been used for the closure of a dorsal trunk woundin a cat,13 but in our experience the feline flank folds are of propor-tionally greater dimensions compared with dogs and, furthermore,feline skin is thinner and generally more abundant and elastic thanthat of the dog, allowing easier closure of comparable wounds suchthat advanced trunk skin reconstructive techniques are rarelyrequired in the cat.21,22
A varying degree of flap necrosis was experienced in each dog, withminor flap debridement required in cases 2 and 3; however, allwounds had healed by 3 weeks post-surgery, with dogs 1 and 3 healedwithin 2 weeks. Factors contributing to flap necrosis may haveincluded an unacceptably high level of stretching, kinking of the flapas it crossed the dorsal spinous processes, or compromise of the vas-cular supply during flap development. The flaps were transferred dor-sally in relation to their base, so gravity is unlikely to have had asignificant negative effect on flap survival.23 In fact, elevated flaps mayhave superior survival compared with dependent flaps, because of theimproved venous drainage.24
The ventral branch of the DCIA supplies the skin of the lateral thighand flank25 and is thought to contribute to the vascular supply of theflank fold.26 In all three cases the DCIAs were not intact, thus smallerdirect cutaneous branches from the caudal superficial epigastric, inter-costal and internal thoracic vessels were the most likely source ofvascular supply to the subdermal plexus of the SFRAFs.25
Used in the manner described, the SFRAF acts as a combined advance-ment and rotation flap. The skin forming the flank fold proper doesnot extend on to the dorsally located recipient bed; rather it is relo-cated dorsally to cover the caudolateral abdominal wall, allowing skinfrom the lateral abdomen to be translated dorsally on to the woundbed. Relocation of the sparsely haired flank fold skin to a more con-spicuous location on the lateral abdomen was cosmetically pleasing inour patients, which were all long-haired breeds. The cosmetic resultin short-haired dogs may be less than ideal and owners should beforewarned.
In addition to bilateral SFRAFs, a transposition flap and partial openwound management (case 2) and multiple relaxing incisions (case 3)
SMALL ANIMALS
SMAL
LAN
IMAL
S
© 2011 The AuthorsAustralian Veterinary Journal © 2011 Australian Veterinary AssociationAustralian Veterinary Journal Volume 89, No 5, May 2011178

facilitated wound closure. This illustrates that, although SFRAFsprovide additional skin for caudodorsal trunk wound closure, thesurgeon should be prepared to use additional reconstructive tech-niques and partial open-wound management if necessary.
The original report of skin fold flaps based on the flank folds suggestedthat only dogs with well-developed skin folds are appropriate candi-dates for this technique.12 The dogs in cases 1 and 2 were obese withpoorly developed flank folds; however, of the six flaps created in thethree patients, all but one flap had sufficient length to cross the dorsalmidline while maintaining adequate width, thus we believe the use ofSFRAFs should be considered even in animals with poorly developedflank folds. Early characterisation of the canine integument found thatthe skin in the flank region has small, loosely packed collagen bundlesand more densely packed elastic fibres compared with skin in otherareas.14 Additionally, the inguinal skin forming the medial surface ofthe flank fold is the thinnest and among the most pliable skin of thedog.14 These properties, together with the unfurling of the double layerforming the flank fold, in our opinion accounted for the flap’s abilityto extend beyond what might be expected.
Conclusion
The use of bilateral flank SFRAFs is a useful technique alone or incombination with other reconstructive techniques for the closure oflarge lumbosacral skin defects. The technique should be reserved forcases where established reconstructive techniques appropriate for theregion are not possible.
Subjectively, small flank folds such as those of obese dogs may yieldunexpectedly large SFRAFs.
References
1. Hedlund CS. Large trunk wounds. Vet Clin North Am Small Anim Pract2006;36:847.2. Swaim SF, Henderson RA. Management of skin tension. In: Swaim SF, Hender-son RA, editors. Small animal wound management. 2nd edn. Williams and Wilkins,Baltimore, 1997;143–190.3. Smith BA, Hosgood G, Hedlund CS. Omental pedicle used to manage a largedorsal wound in a dog. J Small Anim Pract 1995;36:267–270.4. Pavletic MM, editor. Atlas of small animal reconstructive surgery. 2nd edn. Lip-pincott, Philadelphia,1993;65–122, 131–190.
5. Johnston DE. Tension relieving techniques. Vet Clin North Am Small Anim Pract1990;20:67–80.6. Pavletic MM. Use of an external skin-stretching device for wound closure indogs and cats. J Am Vet Med Assoc 2000;217:350.7. Evans HE. The muscular system. In: Evans HE, editor. Miller’s anatomy of the dog.3rd edn. Saunders, Philadelphia, 1993;258–384.8. Pavletic MM. Canine axial pattern flaps, using the omocervical, thoracodorsal,and deep circumflex iliac direct cutaneous arteries. Am J Vet Res 1981;42:391–406.9. Swaim SF. Principles of Mesh Skin Grafting. Compend Cont Educ Pract Vet1982;4:194–200.10. Aragon CL, Harvey SE, Allen SW. Partial-thickness skin grafting for largethermal skin wounds in dogs. Compend Cont Educ Pract Vet 2004;26:200–212.11. Jackson AH, Degner DA, Jackson IT et al. Deep circumflex iliac cutaneous freeflap in cats. Vet Surg 2003;32:341–349.12. Hunt GB. Skin fold advancement flaps for closing large sternal and inguinalwounds in cats and dogs. Vet Surg 1995;24:172–175.13. Hunt GB, Tisdall PLC, Liptak JM et al. Skin-fold advancement flaps for closinglarge proximal limb and trunk defects in dogs and cats. Vet Surg 2001;30:440–448.14. Webb AJ, Calhoun ML. The microscopic anatomy of the skin of mongrel dogs.Am J Vet Res 1954;15:274–280.15. Johnston DE. Wound healing in skin. Vet Clin North Am Small Anim Pract1990;20:1–25.16. Owen LJ, Hotston-Moore A, Holt PE. Vacuum-assisted wound closure follow-ing urine-induced skin and thigh muscle necrosis in a cat. Vet Comp OrthopTraumatol 2009;22:417–421.17. Guille AE, Tseng LW, Orsher RJ. Use of vacuum-assisted closure for manage-ment of a large skin wound in a cat. J Am Vet Med Assoc 2007;11:1669–1673.18. Mayhew PD, Holt DE. Simultaneous use of bilateral caudal superficial epigas-tric axial pattern flaps for wound closure in a dog. J Small Anim Pract 2003;44:534–538.19. Smith MM, Carrig CB, Waldron DR. Direct cutaneous arterial supply to the tailin dogs. Am J Vet Res 1992;53:145–148.20. Saifzadeh S, Hobbenaghi R, Noorabadi M. Axial pattern flap based on thelateral caudal arteries of the tail in the dog: An experimental study. Vet Surg2005;34:509–513.21. Strickland JH, Calhoun ML. Integumentary system of cat. Am J Vet Res1963;24:1018.22. Freeman LJ, Hegreberg GA, Robinette JD. Ehlers-Danlos syndrome in dogsand cats. Semin Vet Med Surg Small Anim 1987;2:221–227.23. Hynes W. The blood-vessels in skin tubes and flaps. Br J Plast Surg 1950;3:165–175.24. Cherry GW, Myers MB, Ardran G et al. The effects of gravity on delayed andtransplanted delayed tubed flaps. Plast Reconstr Surg 1979;64:156–162.25. Evans HE. The systemic arteries. In: Evans HE, editor. Miller’s anatomy of thedog. 3rd edn. Saunders, Philadelphia, 1993;602–681.26. Pavletic MM. Pedicle grafts. In: Slatter DH, editor. Textbook of small animalsurgery. 3rd edn. Saunders, Philadelphia, 2003;292–320.
(Accepted for publication 5 October 2010)
SMALL ANIMALS
SMAL
LAN
IMAL
S
© 2011 The AuthorsAustralian Veterinary Journal © 2011 Australian Veterinary Association Australian Veterinary Journal Volume 89, No 5, May 2011 179