Embed Size (px)
Citation preview

BILATERAL GUAIFENESIN URETERAL CALCULI
CHRIS WHELAN AND BRADLEY F. SCHWARTZ
ABSTRACTWe report on a patient with bilateral ureteral calculi composed of guaifenesin metabolite as determined byinfrared spectroscopy. These stones may be associated with excessive guaifenesin intake related to thecurrent popularity of ephedrine preparations. UROLOGY 63: 175x–175xi, 2004. © 2004 Elsevier Inc.
A22-year-old man with an unremarkable pastmedical history presented with acute bilateral
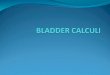
flank pain and microscopic hematuria. Abdominalcomputed tomography demonstrated bilateral ure-teral calculi with hydronephrosis. The left calculusmeasured 4 mm and was located in the distal ureter(Fig. 1A). The right calculus measured 8 mm andwas located in the middle third ureter (Fig. 1B). Hewas admitted and treated conservatively with hy-dration and pain control, anticipating that his leftstone would pass. Twenty-four hours later, he un-derwent bilateral ureteroscopy with basket extrac-tion of his left stone and holmium laser lithotripsyof his right stone. He had an uneventful recovery.Infrared spectroscopy of the stone revealed itscomposition as guaifenesin metabolite. Whenquestioned further about his habits, he admittedtaking 6 to 12 “speed” pills daily. These pills con-tained 12.5 mg of ephedrine and 200 mg ofguaifenesin.
COMMENT
Urinary stone disease is estimated to affect 2% to3% of the population. Approximately 97% of uri-nary stones are composed of calcium, uric acid,struvite, or cystine, and 1% to 3% of stones areclassified as miscellaneous. This latter class in-cludes the crystallized metabolites of medicationssuch as indinavir, topiramate, zonisamide, vitaminD analogues, and ephedrine. Pickens and associ-ates1 have recently described that an excess of beta-
(2-methoxyphenoxy)-lactic acid, a metabolite ofguaifenesin, can result in urolithiasis.
In 1994, the Food and Drug Administration re-stricted the use of pure ephedrine as an over-the-counter drug. Drug manufacturers responded by
From the Division of Urology, Southern Illinois University Schoolof Medicine, Springfield, Illinois
Address for correspondence: Bradley F. Schwartz, D.O., Divi-sion of Urology, Center for Laparoscopy and Endourology, South-ern Illinois School of Medicine, Box 19665, Springfield, IL 62794-9665
Submitted: August 4, 2003, accepted: September 15, 2003
FIGURE 1. Computed tomography scan revealing (A)4-mm calculus in left distal ureter (arrow) and (B) 8-mmcalculus in right middle third ureter (arrow).
CASE REPORT
© 2004 ELSEVIER INC. 0090-4295/04/$30.00175x ALL RIGHTS RESERVED doi:10.1016/j.urology.2003.09.047

developing new over-the-counter drugs containinga mixture of ephedrine and guaifenesin. Thesewere marketed for asthma relief and typically con-tained 12.5 mg of ephedrine and 200 mg ofguaifenesin. Those who used ephedrine prepara-tions as a stimulant switched to the new formula-tions, inadvertently consuming high doses ofguaifenesin. Individuals who presently abuseephedra-containing herbal supplements may turnto ephedrine-containing medications as lawmak-ers threaten tougher ephedra legislation. The stateof Illinois recently took the lead in this movementby banning the sale of ephedra-containing herbalsupplements.
Throughout the 1990s, a growing number of uri-nary stones were found to contain an unknownorganic component. Pickens and associates1 usednuclear magnetic resonance spectroscopy to iden-tify the unknown as beta-(2-methoxyphenoxy)-lactic acid. They were subsequently able to providethe infrared spectrum for this compound for iden-tification use in other laboratories.
Our patient presented with a stone composed ofguaifenesin metabolite. Analysis was performedusing infrared spectrophotometry to obtain a spec-trum identical to the one provided by Pickens andassociates.1 Guaifenesin stones are radiolucent onradiographs, opaque on noncontrast computed to-mography, and fragment easily with holmium laserdevices.
Previous studies have identified abuse ofguaifenesin-containing products to be the primary
cause for guaifenesin stones. Assimos and associ-ates2 used 2-methoxyphenoxy-lactic acid levels inurine to correlate stone formation with guaifenesinconsumption. They found that patients withguaifenesin stones were consuming at least 10.4g/day of guaifenesin, the equivalent of 52 tablets.Our patient admitted only to taking 6 to 12 pills perday. Although it is likely he was taking more, anunknown mechanism may exist that predisposedhim to stone formation with a lower guaifenesinconsumption.
CONCLUSIONS
This case illustrates that abuse of ephedrine-con-taining medications may result in additional con-sequences secondary to excessive guaifenesin in-take. It also underlines the importance of obtaininga complete social history from patients presentingwith stone disease. As ephedra-containing herbalsupplements face additional legislative pressures,more individuals may turn to ephedrine-contain-ing medications, potentially increasing the inci-dence of guaifenesin stones.
REFERENCES1. Pickens CL, Milliron AR, Fussner AL, et al: Abuse of
guaifenesin-containing medications generates an excess of acarboxylate salt of beta-(2-methoxyphenoxy)-lactic acid, aguaifenesin metabolite and results in urolithiasis. Urology 54:23–27, 1999.
2. Assimos DG, Langenstroer P, Leinbach RF, et al:Guaifenesin- and ephedrine-induced stones. J Endourol 13:665–667, 1999.
UROLOGY 63 (1), 2004 175xi