Embed Size (px)
Citation preview

8 Indian Journal of Ophthalmology Vol. ??? No. ???
IJO_343_10R7
DepartmentofOphthalmologyand1Pathology,HospitaldasClinicas,UniversityofSaoPauloMedicalSchool,SaoPaulo,Brazil
Correspondence to: Dr. Allan C. Pieroni Gonçalves, MD,Rua Bahia 70 ap 3-Higienópolis, Sao Paulo Brazil 01244-000. E-mail:[email protected]
Manuscriptreceived:05.06.10;Revisionaccepted:20.08.11
B i l a t e r a l e x t r a o c u l a r m u s c l e s enlargement from Kimura’s disease of the orbit
Allan Christian Pieroni Gonçalves, Rodrigo B. Moritz, Vera L. Aldred1, Mário Luiz Ribeiro Monteiro
Kimura’sdisease(KD) isararechronic inflammatorydiseaseofunclearetiology,characterizedbysubcutaneousnodules,mainlyintheheadandneckregion,frequentlyassociatedwithregionallymphadenopathy.Orbital involvement is infrequent andwhenit occurs, usually affects the eyelid or the lacrimal gland.Wereport a caseof a44-year-oldman thatpresentedwithbilateralslowlyprogressiveproptosis thatwas initiallymisdiagnosed asGraves’Ophthalmopathy.15monthsofworseningproptosisandthe development of facial and temporal swelling led to furtherinvestigation. Computed tomography and magnetic resonanceimaging showed enlargement of all recti muscles and diffuseorbital infiltration.An orbital biopsy was performed and wasconsistentwiththediagnosisofKD.Longtermoralcorticosteroidshowedmarked improvement of proptosis and facial swelling.This case serves to emphasize that KD should be included inthe differential diagnosis of inflammatory diseases of the orbit,even when characterized by predominant involvement of theextraocularmuscles.
Key words: Angiolymphoid hyperplasia with eosinophilia,extraocularmusclesenlargement,Kimura’sdisease
Cite this article as:
Access this article onlineQuick Response Code: Website:
www.ijo.in
DOI:
***PMID: ***
Kimura’sdisease(KD)isarare,chronicinflammatorydisorder,whichoccurspredominantlyinAsians.Itusuallypresentsasadeepsubcutaneousmass in theheadandneckregionandis frequently associatedwith regional lymphadenopathyorsalivary gland involvement.KD is often accompanied byraisedserumeosinophilscountandmarkedlyelevatedserumimmunoglobulinE(IgE)levels.[1]Histologically,thelesionsarecharacterizedbyproliferatingbloodvesselsandeosinophilic
infiltration. The etiology is unknown, but histopathologicand laboratoryfindings suggest an inflammatory responseassociatedwith a self-limited allergic or an autoimmunereactiontoanantigenicstimulus.
Since early reports, KDhas been closely relatedwithangiolymphoidhyperplasiawitheosinophilia (ALHE)andwere even included as part of its spectrum.[2]However,therearemanyclinicalandpathologicaldifferencesbetweenthese2entitiesthatstronglysuggestKDisanindependentdisorder.[3]
ThelacrimalglandsortheeyelidsareusuallyaffectedintheorbitalinvolvementofKD.[4,5]Extraocularmuscleenlargementhasbeendescribedpreviouslybutnotinvolvingbothorbits. [6] Thepurpose of this paper is to document a patientwithKD thatpresentedwithbilateral severe involvementof theorbits,reviewthedifferentialdiagnosisandtreatmentofthiscondition.
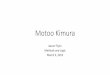
Case ReportA44-year-oldmanhadbilateralproptosiswithgradualonsetfor15months.Atthattime,adiagnosisofGraves’Orbitopathywasestablishedelsewhere,andmoderateimprovementwasobtainedwithcorticosteroidtreatment.3weekspriortoourexamination,hedevelopedworseningproptosisandbilateralpainlessswellingofthefaceandtemporalareaaswellaseyelidedemaandchemosis[Fig.1]andwasadmittedtothehospital.Hehadnohistoryofallergiesoratopy,neoplasiasorotherssystemicdiseases.
Hisbestcorrectedvisualacuitywas20/40intherighteye(OD)and20/25inthelefteye(OS).Hertelexophthalmometryshowed30mmODand28mminOS.Therewasarightrelativeafferentpupillary reflex andmild extraocularmovementsrestriction in all gaze directions. Slit lamp examination,intraocular pressuremeasurements and fundoscopywereunremarkable.
Figure 1: (a) Initial presentation (b) 6 months after corticosteroids treatment
b
a
8 Indian Journal of Ophthalmology Vol. ??? No. ???

AOP*** BriefCommunications 9
Generalphysicalexaminationrevealedbilateralpalpablebutnotwell-defined,non-fluctuating,firmandimmobilemass,involvinganareafromchintothezygomaticandpre-auricularregion.Rightand leftpalpable cervical and submandibularlymphadenopathieswere present. Blood tests revealedhypereosinophiliaandhyperproteinemia.Biochemicalprofile,serumureaandcreatinine levelsand thyroid function testswerenormalornegative.
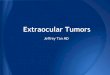
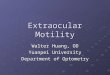
Orbitalcomputedtomographyscanrevealedenlargementofallextraocularmuscleswithsparingoftendons,diffuseapicalorbitalmassinbothorbits,temporalismuscleandeyelidedema[Fig.2].Magneticresonanceimaging(MRI)onT1-weightedimagesrevealedadiffusethickenedsubcutaneoushypointensemass, bilateral enlargementof the temporalismuscles andenlargementofallextraocularmuscles.Themasswasslightlyhyperintense onT2-weighted images and showed intenseandslightlyheterogenousenhancementonpostgadoliniuminjectionT1-weightedimages[Fig.3].
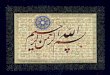
Biopsyspecimensfromtheorbitalfat,theinferiorrectusandthetemporalsubcutaneousregionwereperformedaswellofthecervicallimphonodes.Thehistopathologicfindingoftheperiorbitaltissuewerereplacementofsubcutaneousadiposetissuebyfibrousstromacontainingincreasedbloodvessels,lined by plumped endothelial cells, dense inflammatoryinfiltrate rich in lymphocytes, eosinophils,plasmacellsandseveralreactive lymphoidfollicles [Fig.4].The lymphnodeshowedfollicularhyperplasiawitheosinophilprecipitate in
thegerminalcenter;intheinterfollicularzone,therewasanincrease of eosinophils among the lymphoid cells and thediagnosisofKDwasestablished[Fig.5].
Treatmentstartingwith80mgoforalprednisoneperdayfollowedbyslowtaperingledtoasignificant improvementafter 6months [Fig. 1].After 2 years of treatmentwhenthe corticosteroidwasdiscontinued, thepatient hadmildrecurrencesofeyelidedemaandhadtobemaintainedwithlowdoseoralcorticosteroidtreatment.Hisfinalvisualacuitypresentedslightimprovementto20/30inODandnochangeofthe20/25inOS.
DiscussionKimura’s disease is chronic inflammatory disorder ofunknownetiology,whichpresentswithtumor-likeswellings,mainly in theheadandneck region. It is consideredmuchmoreprevalent inyoungmalesofAsian lineage.Althoughinfectiousetiologieshavebeenpostulated,KDisnowbelievedtoberelatedtoanautoimmuneoradelayedhypersensitivityreaction.Anaberrantallergicresponseisfurthersupportedbytheassociationwithasthma,allergicrhinitisandconjunctivitis,atopicdermatitis,andperipheralhypereosinophiliaaswellasraisedserumIgElevels.[4]
Most caseshavebeen reported in thedermatology,oralsurgery andpathology literature.[6] Itwas first describedin the Chinese literature as “eosinophilic hyperplasticlymphogranuloma”,[1]butbecamewidelyknownasKDafter
Figure 2: (a) axial CT scan (b) Coronal CT scan
a b
Figure 3: (a) MR T1 weighted with contrast (b) MR T2 weighted
a b

10 Indian Journal of Ophthalmology Vol. ??? No. ???
Kimuraet al.[7]reportedsimilarcases.Itisusuallyalocalizedprocesswithout systemicmanifestations, but associatedconditionshavebeendescribed includingallergicdiseasesandnephroticsyndrome.Regionallymphnodeinvolvementoccursinupto75%ofcases.[3]
Kimura’sdiseaseisrarelyanocularcondition.Itappearsto be situatedusually in the superior orbit and is largelyasymptomatic apart from itsmass effect.[5] The conditionmaymimic specificandnon-specific inflammationsof theorbit,neoplasiasandGraves’orbitopathyasexemplifiedinourcase.
Histopathologicalfindingsintheorbitorelsewhereinthebody areproliferationof lymphoid follicles andgerminalcenters, showing interfollicular infiltration by eosinophils.Computed tomography scanfindings arenon-specific andconsistofhomogenouslyenhancing lymphadenopathyandenlarged salivaryglands,with an ill-defined subcutaneousmass extending from the salivary gland.[8]Orbital lesionsarealsonon-specific.OnMRI studies,KDusuallypresentshypointensityonT1-weightedimages,butmayhavedifferentpatterns of signal intensityonT2-weighted,dependingonthevariabilityoffibrosisandvascularity.Thedegreeofpost-contrastenhancementcanalsobevariableandisnotrelatedtothedegreeofhyperintensityonT2-weightedimages.[9]
ThetreatmentmodalitiesforKDincludesurgicalexcision,oralcorticosteroid,cytotoxicdrugsandradiationtherapy.[10] Inthepresentcase,anoralcorticosteroidgreatlyreducedtheswellingoftheeyelidsandrectusmuscleswithmildrecurrenceafterdiscontinuityofcorticosteroidhormone.
Inconclusion,thispaperdocumentstheoccurrenceofseverebilateral involvementofallrectimusclescausedbyKDandservestoemphasizetheneedtoincludeKDinthedifferentialdiagnosis of diffuse extraocularmuscle enlargement.Our
casealsosupportstheuseofsystemicsteroidsasavaluabletreatmentmodalityofsuchcondition.
AcknowledgementsThePatientagreedwiththepublishingofhispicture.Therearenotanyfinancialinterestsinthismanuscript.
References1. ChenH,ThompsonLD,AguileraNS,AbbondanzoSL.Kimura
disease:aclinicopathologicstudyof21cases.AmJSurgPathol2004;28:505-13.
2. Olsen TG, Helwig EB.Angiolymphoid hyperplasia witheosinophilia.Aclinicopathologicstudyof116patients.JAmAcadDermatol.1985;12:781-96.
3. KuoTT, ShihLY,ChanHL.Kimura’sdisease. Involvement ofregional lymph nodes and distinction from angiolymphoidhyperplasiawitheosinophilia.AmJSurgPathol1988;12:843-54.
4. YoganathanP,MeyerDR,FarberMG.Bilateral lacrimalglandinvolvementwithKimuradiseaseinanAfricanAmericanmale.ArchOphthalmol2004;122:917-9.
5. FrancisIC,KappagodaMB,SmithJ,KnealeK.Kimura’sdiseaseoftheorbit.OphthalPlastReconstrSurg1988;4:235-9.
6. Kanazawa S, GongH, Kitaoka T,Amemiya T. Eosinophilicgranuloma(Kimura’sdisease)oftheorbit:Acasereport.GraefesArchClinExpOphthalmol1999;237:518-21.
7. KimuraT,YoshimuraS, IshikuraE.Unusualgranulationtissuecombinedwithhyperplasticchangeoflymphatictissue.TransSocPatholJpn1948;37:179-80.
8. TakahashiS,UedaJ,FurukawaT,TsudaM,NishimuraM,OritaH,et al.Kimuradisease:CTandMRfindings.AJNRAmJNeuroradiol1996;17:382-5.
9. OguzKK,OzturkA,CilaA.MagneticresonanceimagingfindingsinKimura’sdisease.Neuroradiology2004;46:855-8.
10. AmemiyaT.Eosinophilicgranulomaofthesofttissueintheorbit.Ophthalmologica1981;182:42-8.
Figure 4: A reactive lymphoid follicle in the periorbital subcutaneous adipose tissue
Figure 5: High-power view of the inflammatory infiltrate rich in eosinophils