Embed Size (px)
Citation preview

Clinical and Experimental Ophthalmology
2005;
33
: 285–287
�
Correspondence:
Dr Peter Macken, Suite 8, 70 Bowral Street, Bowral, NSW 2576, Australia. Email: [email protected]
This paper was presented at the RANZCO 36th Annual Scientific Congress 2004, Melbourne, Australia.
Clinicopathological Report
Bilateral benign lymphoid hyperplasia of the conjunctiva in a paediatric patient
Peter Kim
MB BS(Hons)
,
1
Peter L Macken
FRANZCO
,
1
Simon Palfreeman
FRCPA
,
2
William D Rawlinson
PhD
3
and Frank Martin
FRANZCO
4
1
Department of Ophthalmology, Liverpool Hospital,
2
Douglass Hanly Moir Pathology,
3
Virology Division, Department of Microbiology, South-eastern Area Laboratory Services, Prince of Wales Hospital, and
4
Department of Ophthalmology, The Children’s Hospital at Westmead, Sydney, New South Wales, Australia
C
ASE
REPORT
A 14-year-old Caucasian boy presented in March 2002 witha 6-month history of bilateral slowly enlarging conjunctivalmasses. There was no associated ocular or systemic symp-tomatology. He was not on any medications and was other-wise well, with no significant past medical or family history.
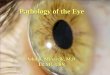
Examination revealed bilateral asymmetric (right
>
left)hypertrophic salmon-pink nodules involving the bulbar con-junctiva near the medial canthus (Fig. 1). The remainder ofhis ocular examination including visual acuity, ocular move-ments, anterior segment and fundus examination was unre-markable. There was no evidence of proptosis and noregional or generalized lymphadenopathy.
Full blood count, urea, creatinine and electrolytes, liverfunction tests, erythrocyte sedimentation rate, serum proteinelectrophoresis and lactate dehydrogenase were within nor-mal limits. Computed tomography scan of the orbits, withcontrast enhancement, confirmed the bilateral conjunctivallesions but there was no evidence of local extension or bonyerosion. The globe, optic nerve and extraocular muscleswere normal; in particular, there were no intraconal or extra-conal mass lesions. Computed tomography scan of the neck/chest/abdomen/pelvis and whole body gallium scan werenormal.
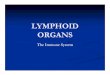
Subsequently, excision biopsy of the bilateral conjunctivallesions was performed. Histopathological examinationshowed a prominent lymphoid infiltrate involving the sub-conjunctival connective tissue. The infiltrate had a promi-nent follicular pattern (Fig. 2). The germinal centres showednumerous macrophages containing scattered debris (tingi-ble bodies) (Fig. 2). The interfollicular zone was mildlyexpanded with predominantly small mature lymphocytes.Although there were very occasional lymphocytes in theoverlying epithelium, no definite lymphoepithelial lesions
A
BSTRACT
A 14-year-old boy presented with a 6-month history ofbilateral slowly enlarging conjunctival lesions. There was noassociated ocular or systemic symptomatology. Examinationrevealed bilateral salmon-coloured nodular lesions of the bul-bar conjunctiva. The remainder of his ophthalmic and generalexaminations were normal. Extensive investigation excludedregional or systemic involvement. Excision biopsy of thelesions showed a predominantly mature B lymphocyte infil-trate with immunohistochemistry and flow cytometry consis-tent with reactive lymphoid hyperplasia. Polymerase chainreaction testing for Epstein–Barr virus was negative. At 2 yearsfollow-up, the patient remained healthy and there was noevidence of recurrence. Benign lymphoid hyperplasia of theconjunctiva with bilateral involvement is extremely rare inchildren. Only a few case reports have been documented inthe literature.
Key words:
conjunctiva
,
paediatric
,
reactive lymphoidhyperplasia
.
I
NTRODUCTION
Benign lymphoid hyperplasia (BLH) of the conjunctiva withbilateral involvement is very rare in children, with only casereports documented in the literature.
1,2
We describe a 14-year-old boy who presented with bilateral salmon-pinklesions, diagnosed as BLH following excision biopsy. Thenatural history of this condition in children and adolescentsis not well established.
1
As is the case with our patient, therehave been no reported cases of recurrence following excisionin children.
1–3

286 Kim
et al.
were noted. No Dutcher bodies were seen. Immediatelybeneath the conjunctiva there were a small number of plasmacells. No atypical lymphocytes nor any significant popula-tion of large immature lymphocytes were noted.
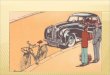
Immunoperoxidase stains showed a mixture of B (CD20and CD79a) and T (CD3) lymphocytes with a predominanceof B lymphocytes. Kappa and lambda stains show no evi-dence of monoclonality within plasma cells. Bcl-2 stainingwas negative within the follicles (Fig. 3). No significant sub-population was seen with CD10, CD23, CD5 or cyclin D1.Flow cytometry showed predominantly B cells (CD19,CD20, DR and CD23) with a small number of cells notexpressing CD23. There was a small population of T cells(19% CD3 positive). No light chain restriction was seen.
Polymerase chain reaction testing on paraffin-embeddedbiopsy tissue for Epstein–Barr virus infection was negative.
A diagnosis of reactive lymphoid hyperplasia was madebased on the morphological and immunophenotypicalfeatures. At 2 years follow-up, the patient has remainedhealthy with no evidence of local recurrence or systemicinvolvement.
D
ISCUSSION
Conjunctival mass lesions can prove to be difficult diagnosticdilemmas, and often cannot be definitively identified unlesshistopathological studies are performed. The differentialdiagnosis of such lesions include viral infections such asEpstein–Barr virus, hyperplastic lesions such as pseudocar-cinomatous hyperplasia and BLH and malignant lesionssuch as Ewing sarcoma, Burkitt’s lymphoma, rhabdomyosar-coma, systemic leukaemia, lymphoma and squamous cellcarcinoma.
2,4
Lymphoproliferative disorders of the ocular adnexa covera spectrum of diseases ranging from BLH, atypical lymphoidhyperplasia to lymphoma.
3,5
In a series of 112 adult cases oflymphoproliferative lesions of the ocular adnexa by Coup-land
et al.
, approximately 10% of conjunctival lesions werehistologically BLH.
6
Similarly, McKelvie
et al.
in theirAustralian adult series had six of 73 (8.2%) ocular adnexallymphoproliferative lesions having a histological diagnosisof BLH.
7
Studies have shown that approximately one-third to one-half of patients with ocular adnexal lymphoma may developsystemic lymphoma.
7,8
Importantly, conjunctival BLH inadults similarly appears to be associated with systemic lym-phoma with approximately one-third to one-half of casesdeveloping systemic involvement. Therefore careful evalua-tion and follow-up in these patients is recommended.
3,6,7,9
Inadults, it appears that lymphoid infiltrates of the conjunctivamay have lower incidence of extraocular lymphoma thanthose involving the orbital and eyelid structures.
8
Figure 1.
Bilateral asymmetric (right
>
left) hypertrophicsalmon-pink coloured nodules involving the bulbar conjunctiva.
Figure 2.
Low magnification section of the conjunctival biopsy.(original magnification
¥
4, haematoxylin–eosin).
Figure 3.
Immunohistochemical stains are negative for Bcl-2 con-sistent with reactive germinal centres. (original magnification
¥
4).

Conjunctival lymphoid proliferation in a child 287
The literature regarding conjunctival BLH in paediatricpatients and the risk of associated systemic disease is far lesscomplete. Only case reports of BLH in children appear inthe literature, and its incidence is not known.
1,2
To ourknowledge, there have been no cases of recurrence reportedwith follow-up ranging from 1 to 3.5 years, including ourcase at 2 years follow-up.
1–3
Further longer term follow-up isrequired to determine the natural history of the condition,although anecdotal evidence suggests that it may be benignand have a self-limited course.
1,2
We suggest paediatricpatients be referred to a paediatric oncologist for compre-hensive clinical evaluation, appropriate investigations andfollow-up, until the natural history of such lesions is betterunderstood.
2,3
Following excisional biopsy of the conjunctival BLHlesion in our patient, no chemotherapeutics were startedfollowing close consultation with a paediatric oncologist.Our patient has been closely observed for 2 years for anysigns of local recurrence or systemic disease and the resultshave been unremarkable. Other reported cases of paediatricconjunctival BLH in the literature, having been similarlytreated with excisional biopsy and no adjuvant therapy, haveshown no recurrences.
1–3
Our patient had isolated bilateral conjunctival lesionswith no evidence of local extension into the surroundingorbital or eyelid structures clinically or radiologically. Nei-ther was there any evidence of systemic spread. Interestingly,the lack of systemic involvement (stage of disease) at thetime of presentation in adult populations appears to bea negative predictor for subsequent systemic involvementand therefore a more favourable clinical prognosis.
6–8
How-ever, this association has not been confirmed in paediatricpopulations.
The precise cause of BLH is not known, although thereis some anecdotal evidence for an allergic or viral aetiol-ogy.
3,4
Further, the conjunctiva-associated lymphoid tissuemay be important as the afferent limb of the acquiredimmune response for the ocular surface.
10,11
However, ourpatient denied any prodromal ocular or systemic symptom-
atology; ophthalmic and general physical examination werenormal, including no evidence of lymphadenopathy, andblood tests and radiological assessment were unremarkable.
Conjunctival BLH in children is rare, and only a few casereports of bilateral disease have been documented in theliterature.
3,9
R
EFERENCES
1. McLeod SD, Edward DP. Benign lymphoid hyperplasia of theconjunctiva in children.
Arch Ophthalmol
1999;
117
: 832–5.2. Tang J, Rodgers IR, Basham KL, Goh J. Rare case of exuberant
benign lymphoid hyperplasia involving the conjunctiva, carun-cle, and plica in a child with tonsilar enlargement.
J AAPOS
2003;
7
: 293–4.3. Feinberg AS, Spraul CW, Holden JT, Grossniklaus HE. Con-
junctival lymphocytic infiltrates associated with Epstein-Barrvirus.
Ophthalmology
2000;
107
: 159–63.4. Weisenthal RW, Streeten BW, Dubansky AS
et al.
Burkitt lym-phoma presenting as a conjunctival mass.
Ophthalmology
1995;
102
: 129–34.5. Liesegang TJ. Ocular adnexal lymphoproliferative lesions.
Mayo Clin Proc
1993;
68
: 1003–10.6. Coupland SE, Krause L, Delecluse HJ
et al.
Lymphoproliferativelesions of the ocular adnexa.
Ophthalmology
1998;
105
: 1430–41.
7. McKelvie PA, McNab A, Francis IC, Fox R, O’Day J. Ocularadnexal lymphoproliferative disease: a series of 73 cases.
ClinExperiment Ophthalmol
2001;
29
: 387–93.8. Knowles DM, Jakobiec FA, McNally L, Burke JS. Lymphoid
hyperplasia and malignant lymphoma occurring in the ocularadnexa (orbit, conjunctiva and eyelids): a prospective multi-parametric analysis of 108 cases during 1977–1987.
Hum Pathol
1990;
21
: 959–73.9. Sigelman J, Jakobiec FA. Lymphoid lesions of the conjunctiva:
relation of histopathology to clinical outcome.
Ophthalmology
1978;
85
: 818–43.10. Chodosh J, Kennedy RC. The conjunctival lymphoid follicle
in mucosal immunology.
DNA Cell Biol
2002;
21
: 421–33.11. Knop N, Knop E. Conjunctiva-associated lymphoid tissue in
the human eye.
Invest Ophthalmol Vis Sci
2000;
41
: 1270–9.










![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.pdfslide.us/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)