Embed Size (px)
Citation preview

Bibliography
Allman RM, Laprade CA, Noel LB, et al: Air fluidized beds or conventional therapy for pressure sores-a randomized trial. Ann Intern Med 107:641, 1987
Au WY, Dutt AK, DeSoyza N: Theophylline kinetics in chronic obstructive airway disease in the elderly. Clin Pharmacol Ther 37:472,1985
Bayer AJ, Chadha JS, Farag RR, et al: Changing presentation of myocardial infarction with increasing old age. J Am Geriatr Soc 34:263, 1986
Berman P, Hogan DB, Fox RA: The atypical presentation of infection in old age. Age Ageing 16:201, 1987
Blazer DG II, Federspiel CF, Ray WA, et al: The risk of anticholinergic toxicity in the elderly: a study of prescribing practices in two populations. J Gerontol 38:31,1983
Boscia JA, Kobasa WD, Knight RA, et al: Therapy versus no therapy of bacteriuria in elderly ambulatory non-hospitalized woman. JAMA 257:1067, 1987
Brocklehurst JC, Rubenstein LZ, Clark AN, Lipsitz LA: The natural history of drop attacks. NeuroI36:1029, 1986
Burke W J, Rubin EH, Zorumski CF, Wetzel RD: The safety of ECT in geriatric psychiatry. J Am Geriatr Soc 35:516,1987
Carskadon MA, Seidel WF, Greenblatt DJ, et al: Daytime carryover of triazolam and flurazepam in elderly insomniacs. Sleep 5:361, 1982
Clarfield AM: The reversible dementias: do they reverse? Review. Ann Intern Med 109:476, 1988
Cobden I, Lendrum R, Venables CWO et al: Gallstones presenting as mental and physical debility in the elderly. Lancet 1:1062, 1984
Cummings JL: Subcortical dementia: neuropsychology, neuropsychiatry, and pathophysiology. Br J Psych 149:682, 1986
Eslinger PJ, Damasio AR, Benton AL, et al: Neuropsychologic detection of abnormal mental decline in older persons. JAMA 253:670, 1985
Fox DA, Jick H: Nonsteroidal anti-inflammatory drugs and renal disease. JAMA 251:1299, 1984
Georgotas A, Friedman E, McCarthy M, et al: Resistant geriatric depressions and therapeutic response to monoamine oxidase inhibitors. BioI Psychiatry 18:195, 1983
147
148 Protocols in Primary Care Geriatrics
Gjorup T, Hendriksen C, Lund E, Stromgard E: Is growing old a disease? A study of the attitudes of elderly people to physical symptoms. J Chron Dis 40:1095,1987
Gosney M, Tallis R: Prescription of contraindicated and interacting drugs in elderly patients admitted to hospital. Lancet 2:564, 1984
Groth-Juncker A, McCusker J: Where do elderly patients prefer to die? J Am Geriatr Soc 31:457,1983
Guam L, Ricciotti NA, Fair WR: Endoscopic bladder neck suspension for stress urinary incontinence. J UroI132:1119, 1984
Ham, Richard: Primary Care Geriatrics. Boston, John Wright, 1983 High DM: Planning for decisional incapacity: a neglected area in ethics and
aging. J Am Geriatr Soc 35:814, 1987 Kane RL, Bernstein L, Wales J, et al: Hospice effectiveness in controlling pain.
JAMA 253:2683, 1985 Koenig HG, Meador KG, Cohen HJ: Depression in hospitalized elderly pa
tients with medical illness. Arch Intern Med 148:1929, 1988 Lakshmanan M, Mion LC, Frengley JD: Effective low dose tricyclic antide
pressant treatment for depressed geriatric rehabilitation patients: a doubleblind study. J Am Geriatr Soc 34:421, 1986
Levinstein MR, Ouslander JG, Rubenstein LZ, Forsythe SB: Yield of routine annual laboratory tests in a skilled nursing home population. JAMA 258: 1909,1987
Lewis MA, Kane RL, Cretin S, et al: The immediate and subsequent outcomes of nursing home care. Am J Public Health 75:758, 1985
Lindeman RD, Tobin J, Shock NW: Longitudinal studies on the rate of decline in renal function with age. J Am Geriatr Soc 33:278, 1985
Magen RF: Preparing Instructional Objectives (2nd eel) Belmont, California John Wright, 1983
Messerli FH, Ventura HO, Amodeo C: Osler's maneuver and pseudohypertension. N Engl J Med 312:1548, 1985
N ordenstam G R, Brandberg CA, Oden AS, et al: Bacteriuria and mortality in an elderly population. N Engl J Med 314:1152, 1986
Ouslander JG, Blaustein J, Connor A, Pitt A: Habit training and oxybutynin for incontinence in nursing home patients: a placebo-controlled trial. J Am Geriatr Soc 36:40,1988
Overstall pw, Hazell JWP, Johnson AL: Vertigo in the elderly. Age Ageing 10:105, 1981
Parry F: Physical rehabilitation of the old, old patient. J Am Geriatr Soc 31:482, 1983
Pinchcofsky-Devin GD, Kaminski MV: Correlation of pressure sores and nutritional status. J Am Geriatr Soc 34:435, 1986
Ray WA, Griffin MR, et al: Psychotropic drug use and the risk of hip fracture. N Engl J Med 316:363, 1987
Risse SC, Barnes R: Pharmacologic treatment of agitation associated with dementia. J Am Geriatr Soc 34:368,1986
Robbins LJ, Boyko E, Lane J, et al: Binding the elderly: a prospective study of the use of mechanical restraints in an acute care hospital. J Am Geriatr Soc 35:290,1987
Roose SP, Glassman AH, Giarding EG, et al: Tricyclic antidepressants in
Bibliography 149
depressed patients with cardiac conduction disease. Arch Gen Psychiatry 44:273,1987
Sandman PO, Adolfsson R, Hallmans G, et al: Treatment of constipation with high-bran bread in long-term care of severely demented elderly patients. J Am Geriatr Soc 31:289, 1983
Satinsky JD: Chronic heart failure in the elderly: vasodilator therapy. Angiology 34:509,1983
Schiedermayer DL: The decision to forgo CPR in the elderly patient. JAMA 260:2096,1988
Schneider EL, Brody JA: Aging, natural death, and the compression of morbidity: another view. N Engl J Med 309:854, 1983
Stead ww, Lofgren JP, Warren E, et al: Thberculosis as an endemic and nosocomial infection among the elderly in nursing homes. N Engl J Med 312: 1483,1985
Steele K: Iatrogenic disease on a medical service. J Am Geriatr Soc 32:445, 1984
Sudarsky L, Ronthal M: Gait disorders among elderly patients: a survey study of 50 patients. Arch NeuroI40:740, 1983
Taffet GE, Teasdale TA, Luchi RJ: In-hospital cardiopulmonary resuscitation. JAMA 260:2069, 1988
Teri L, Larson EB, Reifler BV: Behavioral disturbance in dementia of the Alzheimer's type. J Am Geriatr Soc 36:1,1988
Tibaldi JM, Barzel US, Albin J, Surks M: Thyrotoxicosis in the very old. Am J Med 81:619, 1986
Tinetti ME: Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc 34:119,1986
Tinetti ME, Williams TF, Mayewski R: Fall risk index for elderly patients based on number of chronic disabilities. Am J Med 80:429, 1986
Volicfer L, Rheaume Y, Brown J, et al: Hospice approach to the treatment of patients with advanced dementia of the Alzheimer type. JAMA 256:2210, 1986
Ware JA, Snow E, Luchi JM, et al: Effect of digoxin on ejection fraction in elderly patients with congestive heart failure. J Am Geriatr Soc 32:631, 1984
Whitehead WE, Burgio KL, Engel BT: Biofeedback treatment of fecal incontinence in geriatric patients. J Am Geriatr Soc 33:320,1985
Woodhouse KW, Mutch E, Williams FM, et al: The effect of age on pathways of drug metabolism in human liver. Age Ageing 13:328, 1984
Part II Notes on Geriatrics
Chapter 1-Essentials of Geriatrics and Aging
I OVERVIEW OF THE SUBJECT: the "6 Ds" DRUGS are a major focus of concern. DISEASES accumulate (MULTIPLE PATHOLOGY). DISABILITY is often the reason for treatment rather than
illness per se. DIFFERENCE: heterogeneity is the rule in nearly every
thing you can measure. DECISIONS about care: ethical questions to consider when
patients can't speak for themselves. DEMOGRAPHY makes geriatric knowledge a must for the
year 2000 and beyond.
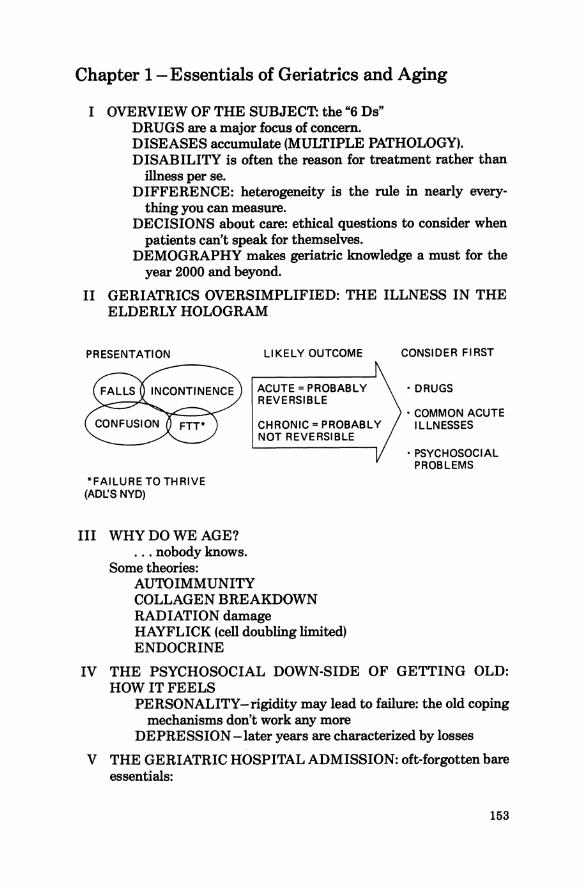
II GERIATRICS OVERSIMPLIFIED: THE ILLNESS IN THE ELDERLY HOLOGRAM
PRESENTATION LI KEL Y OUTCOME CONSIDER FIRST
ACUTE = PROBABLY • DRUGS REVERSIBLE
• COMMON ACUTE CHRONIC = PROBABLY ILLNESSES
*FAILURE TO THRIVE (ADL.:S NYD)
III WHY DO WE AGE? ... nobody knows.
Some theories: AUTOIMMUNITY
NOT REVERSIBLE
COLLAGEN BREAKDOWN RADIATION damage HAYFLICK (cell doubling limited) ENDOCRINE
• PSYCHOSOCIAL PROBLEMS
IV THE PSYCHOSOCIAL DOWN-SIDE OF GETTING OLD: HOW IT FEELS
PERSONALITY-rigidity may lead to failure: the old coping mechanisms don't work any more
DEPRESSION -later years are characterized by losses
V THE GERIATRIC HOSPITAL ADMISSION: oft-forgotten bare essentials:
153
154 Protocols in Primary Care Geriatrics
• COG NITIVE FUNCTION on admission (MMSE or MSQ) • ACTIVITIES OF DAILY LIVING - What could the patient
do pre-illness? What is the likely best and worst outcome? Planning required?
• DECISIONS: code/no code, etc.: take the decision, stick to it, review it regularly.
Notes on Geriatrics 155
Chapter 2 - Comprehensive Geriatric Assessment I GENERAL WISDOM
A Differs from working up a younger adult, whether in office, special unit or nursing home.
B Who needs it? Any elderly patient: • Newtoyou • Newly disabled • On multiple medication • Newly confused, incontinent, or falling
C The "money" here is in identifying reversible causes of disability.
D What do you assess? 1. COGNITIVE FUNCTION 2. ADLsIIADLs (Activities of Daily Livingllnstrumental
Activities of Daily Living) 3. GENERAL MEDICAL CONDITION ... You must be able to measure the first two to decide whether your interventions with the third are useful or not.
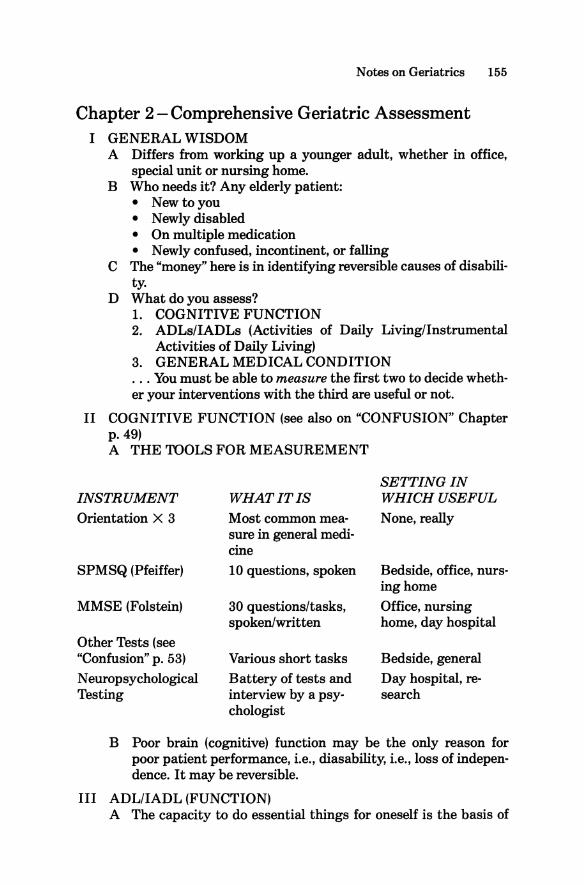
II COGNITIVE FUNCTION (see also on "CONFUSION" Chapter p.49) A THE TOOLS FOR MEASUREMENT
SETTING IN INSTRUMENT Orientation X 3
WHAT IT IS WHICH USEFUL Most common mea- None, really
SPMSQ (Pfeiffer)
MMSE (Folstein)
Other Tests (see "Confusion" p. 53) Neuropsychological Testing
sure in general medi-cine 10 questions, spoken
30 questions/tasks, spoken/written
Various short tasks Battery of tests and interview by a psychologist
Bedside, office, nursinghome Office, nursing home, day hospital
Bedside, general Day hospital, research
B Poor brain (cognitive) function may be the only reason for poor patient performance, i.e., diasability, i.e., loss of independence. It may be reversible.
III ADLIIADL (FUNCTION) A The capacity to do essential things for oneself is the basis of
156 Protocols in Primary Care Geriatrics
independence. Independence is what keeps a capable, freeliving person out of nursing homes, hospitals, TROUBLE.
B To determine whether a medical intervention is valuable to the patient, ask ''What will this do to ADL/IADL?" and you usually have your answer.
C ADLs: the intimate personal "nursing home" activities (mne-monic "DEATH")
Dressing Eating Ambulating (all forms of mobility) Toileting (usually subject to mobility) Hygiene (bath, grooming)
D IADLs: the community-capable, fully independent activities (mnemonic "SHAFT")
Shopping Housework Accounting (bank book balancing, paying bills) Food preparation (cooking) Transport (bus, taxi, own car)
E MEASUREMENT Scales of ADL abound, but except for researchers and fulltime professionals, history (including collateral) and observations are your best index.
F Speed of performance and safety are other important variables to consider in ADL assessment.
G Try to assess PERFORMANCE directly, rather than reports of same by other observers.
IV THE MEDICAL ASSESSMENT The history and physical exam are as for any other in-depth medical assessment, with the following high-spots not to be forgotten: HISTORY A Affect: is the patient depressed/well motivated/frightened? B Bad drugs (and good ones): remember medication is more
often part of the problem than part of the solution. C Continence: elderly patients may deny this self-esteem-des
troying problem. D Dolor: any painful condition impairs function. E Eyes and ears: to be alert and to navigate, sensory input
must be maximized. F Function: ADLsIIADLs. PHYSICAL A Awareness of safety BP Orthostatic hypotension C Cognitive function, as we call it
Notes on Geriatrics 157
D Do the ADLlIADLs, don't buy reported performance E Extrapyramidal: obvious or occult, idiopathic or drug-in
duced F Force: means MUSCLE POWER (fits into the mnemonic) G Gait: ataxic, antalgic, Parkinsonian, fearful, etc.
V THE PROCESS OF ASSESSMENT/INTERVENTION Constant, tireless return to medical/surgical basics, with reference to cognitive function and ADLs every time an intervention is made. Good geriatric medicine is medicine that helps your patient THINK clearly, and DO more. Everything else is, at best, irrelevant; more likely, ultimately harmful.
158 Protocols in Primary Care Geriatrics
Chapter 3 - Rehabilitation of Elderly Patients
I GENERAL WISDOM A The elderly lose 3 % of power for every day in bed. Therefore
immobility in the elderly is a near-emergency: think of it as you would convergent strabismus in children.
B Every hospitalized elderly needs rehabilitation, not only hips and strokes.
C Make the rehabilitation diagnosis on admission and on discharge. It's as critical as the traditional medical one ("impaired balance, L. hemi-weakness, safety awareness:' etc.)
D Ordering occupational or physiotherapy is no substitute for a capable, informed, PHYSICALLY INVOLVED M.D. The patient responds when you stand at the bedside and daily put him/her through the paces. Time-consuming; pays off in the end.
II STARTING WITH ONE HAND TIED BEHIND YOUR BACK The elderly, typically, may be:
MULTIPLY PATHOLOGICAL ON MANY MEDICATIONS CONFUSED UNSTEADY AT BEST BLIND, DEAF, PROPRIOCEPTIVELY IMPAIRED HOMEOSTATICALLY BLUNTED DEPRESSED/AFRAID ( ... we never said it was easy.)
III THE IMMOBrLITY TRAP To succeed at rehabilitation, you must break a powerful vicious cycle: the consequences of immobility are also its' contributing causes (mnenomic "DISASTERS")
CAUSES DOLOR (pain) INCONTINENCE STRENGTH POOR AFFECT: DEPRESSION and
FEAR STIFFNESS THOUGHT: CONFUSION EQUILIBRIUM PROBLEMS R - PRESCRIPTION DRUGS
SEEING and HEARING IMPAIRED
CONSEQUENCES PAIN INCONTINENCE STRENGTH LOST DEPRESSION and FEAR
STIFFNESS CONFUSION BALANCE LOSS MORE PRESCRIPTION
DRUGS LOSS OF VISION and
HEARING
Notes on Geriatrics 159
IV ADVANCED IMMOBILITY-the consequences which further clinch irreversibility
INFECTIONS (UTI, CHEST) CALCULI CONSTIPATIONIIMPACTION/FECAL INCONTINENCE DECUBITI HYPOTHERMIA FLUID and ELECTROLYTE DISTURBANCE OSTEOPOROSIS and FRACTURES VENOUS THROMBOSIS EMBOLI, CVA, MI, P.E.
V THE REHABILITATION PROCESS ("DARTS") DIAGNOSIS of disabling condition including rehabilitation
diagnosis ASSESSMENT (Please see chapter on Assessment) REALISTIC GOAL-SETTING TREATMENT (yet another mnemonic: "SPREAD")
SPecific disease treatment PRevention of second disability REstoration of previous level of function, if possible ADaption to persisting disability
SOCIAL SERVICE assists with placement if required.
160 Protocols in Primary Care Geriatrics
Chapter 4 - Atypical Presentation of Disease
I GENERAL WISDOM A The mechanisms that produce textbook signs and symptoms
age along with the rest of the physiology. Result: the elderly rarely show classical evidence of illness.
B Falling, incontinence, confusion, and "geriatric failure to thrive" are more typical disease manifestations.
C "Uncommon presentation of common conditions is more common than common presentation of uncommon conditions" (NOTE: this is not an excuse to forget rare diseases ... ).
II A FEW EXAMPLES A ACUTE ABDOMEN
1. Often silent (no pain, no tenderness, no fever, no leukocytosis).
2. You'd naturally think of pancreatitis, cholecystitis, cholangitis, appendicitis, perforated ulcer. But don't forget VASCULAR conditions in the abdomen and DIVERTICULAR DISEASE consequences.
3. Serial physical, plain films of abdomen, high index of suspicion may be useful.
B THYROID DISEASE-really requires screening. Remember to obtain TSH if T4 in low-normal range and unexplained problems present.
C DRUG REACTIONS-usually not what you expect from reading the pharmacy manual. The only way to rule it out may be to stop the drug, carefully.
D PULMONARY EMBOLISM-hard to diagnose at the best of times; suspect in all P.E. high-risk elderly who deteriorate.
E INFECTIONS - common things are common, but remember SYPHILIS, SBE, TB, AIDS. Temperature and white count are of limited use.
F CARDIOVASCULAR DISEASE 1. ARRHYTHMIA-presents as falls 2. MI-often silent, or presents as emboli, CVA, GI symp
toms, confusion 3. CHF-very tricky condition:
• UNDERPRESENTATION -elderly patient "goes off' with no tachypnea, edema, or physical findings, has a surprise chest X-ray.
• OVERPRESENTATION -well-intentioned doctor treats basilar rales and ankle edema with toxic drugs and patient deteriorates.
• Typical problem is patient with known congestive heart

Notes on Geriatrics 161
failure who is fatigued: is it the disease or is it medications? Titrate to ADLs, exercise tolerance, cognitive function.
G CANCER- commonest presentation is the SILENT MASS. Make you physical examination thoroughly, do your screening tests.
162 Protocols in Primary Care Geriatrics
Chapter 5 - Falls and Instability
I GENERAL WISDOM A One of the great nonspecific presentations of disease: a "geri
c atric giant:' B We lose stability as we age (our "sway diagram" widens). C We are less likely to successfully compensate for being pushed
off-balance, as we age. D IMMOBILIZING at-risk patients is a dangerous easy way
out, but unfortunately true reversible causes of falling are not all that common.
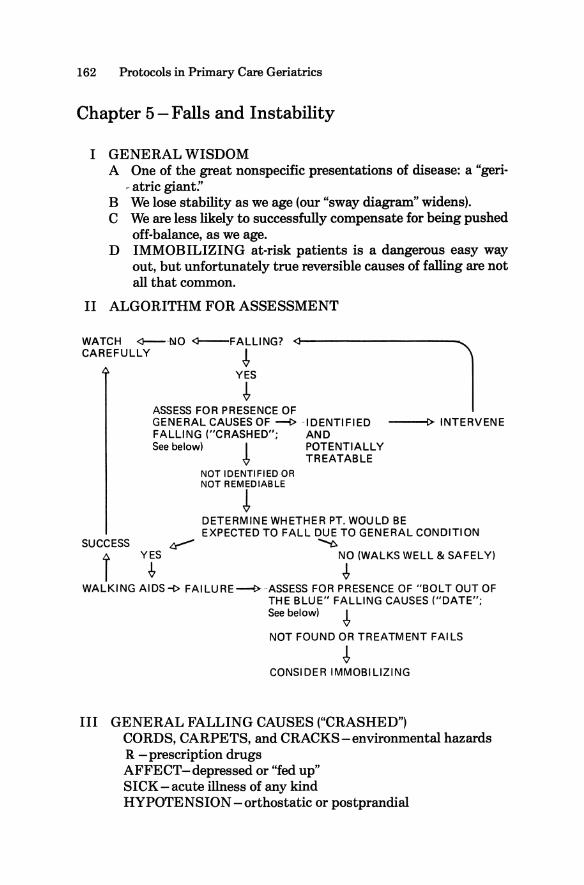
II ALGORITHM FOR ASSESSMENT
WATCH <i---NO <l--FALLlNG? <l----------l CAREFULLY ~
YES
~ ASSESS FOR PRESENCE OF GENERAL CAUSES OF --i> -IDENTIFIED FALLING ("CRASHED"; AND See below) I POTENTIALLY
-& TREATABLE NOT IDENTIFIED OR NOT REMEDIABLE
!
---!>INTERVENE
DETERMINE WHETHER PT. WOULD BE EXPECTED TO FALL DUE TO GENERAL CONDITION
SUCCESS ~ ~ YES NO (WALKS WELL & SAFELY)
~ ~ r WALKING AIDS-\> FAILURE~ASSESS FOR PRESENCE OF "BOLT OUT OF
THE BLUE" FALLING CAUSES ("DATE"; See below) ~
NOT FOUND OR TREATMENT FAILS
~ CONSIDER IMMOBILIZING
III GENERAL FALLING CAUSES ("CRASHED") CORDS, CARPETS, and CRACKS-environmental hazards R - prescription drugs AFFECT-depressed or "fed up" SICK-acute illness of any kind HYPOTENSION -orthostatic or postprandial
Notes on Geriatrics 163
EYES -vision problems DIZZINESS - any cause of true vertigo
IV "BOLT OUT OF THE BLUE" FALLING CAUSES ("DATE") DROP ATTACK ARRHYTHMIA (especially bradyarrhythmia) TIA EPILEPSY-seizures
164 Protocols in Primary Care Geriatrics
Chapter 6 - Incontinence
I URINARY A GENERAL WISDOM
1. Common and self-esteem-destroying, especially to this Victorian generation of elderly.
2. Caregivers, no matter how good, involuntarily don't like looking after smelly, wet people.
3. Like confusion, OFTEN reversible when acute.
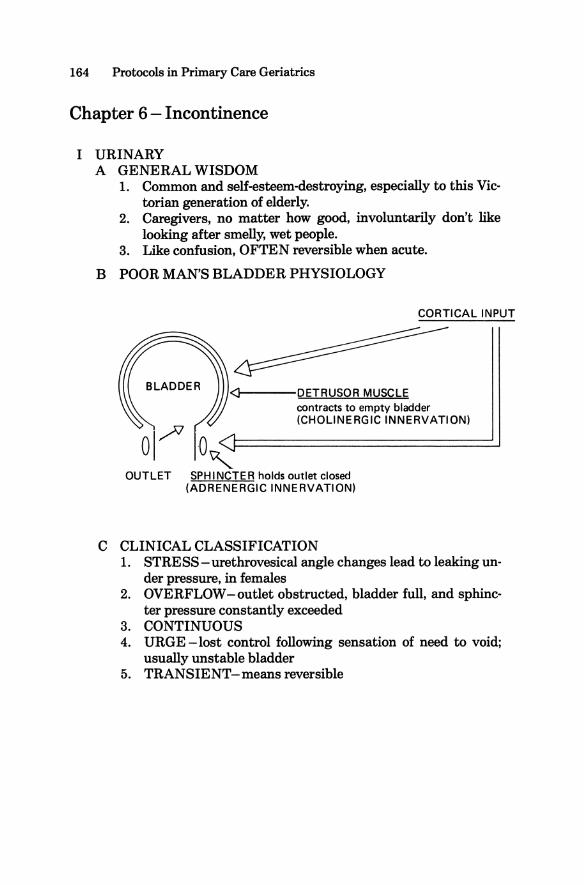
B POOR MAN'S BLADDER PHYSIOLOGY
o,/l 0 , ~--DETRUSOR MUSCLE
contracts to empty bladder (CHOLINERGIC INNERVATION)
OUTLET SPHINCTER holds outlet closed (ADRENERGIC INNERVATION)
C CLINICAL CLASSIFICATION 1. STRESS - urethrovesical angle changes lead to leaking un
der pressure, in females 2. OVERFLOW-outlet obstructed, bladder full, and sphinc
ter pressure constantly exceeded 3. CONTINUOUS 4. URGE -lost control following sensation of need to void;
usually unstable bladder 5. TRANSIENT-means reversible
Notes on Geriatrics 165
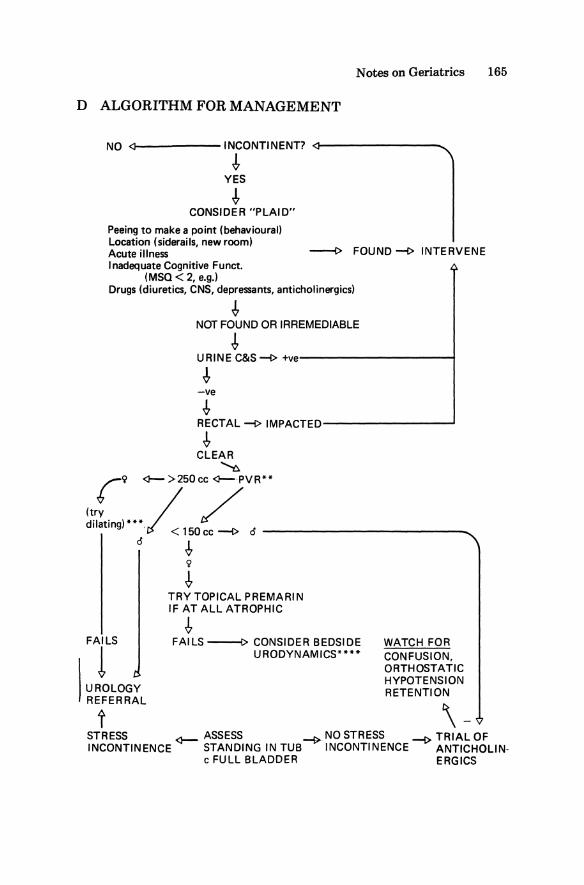
D ALGORITHM FOR MANAGEMENT
NO <)-----INCONTINENT? <)--------.... !
YES
! CONSIDER "PLAID"
Peeing to make a point (behavioural) Location (siderails, new room) Acute illness ---i> FOUND --(> INTERVENE Inadequate Cognitive Funct.
(MSQ < 2, e.g.) Drugs (diuretics, CNS, depressants, anticholinergics)
! NOT FOUND OR IRREMEDIABLE
! URINE C&S~ +ve-----------f
~ -ve
-!, RECTAL~IMPACTED------------~
! CLEAR ~ r9 <I-->250cc <l--PVR**
~~y. )*** / / I atm9 ./ < 150cc --i> 0 ____________ _
o -!, 9
FAILS
1 UROLOGY REFERRAL
t
! TRY TOPICAL PREMARIN IF AT ALL ATROPHIC
! FAILS ----t> CONSIDER BEDSIDE WATCH FOR
URODYNAMICS**** CONFUSION, ORTHOSTATIC HYPOTENSION RETENTION
\-STRESS <I- ASSESS ~ NO STRESS -I> TRIAL OF INCONTINENCE STANDING IN TUB INCONTINENCE ANTICHOLIN·
e FULL BLADDER ERGICS
166 Protocols in Primary Care Geriatrics
NarES ON ALGORITHM * "PLAID" considerations bear on incontinence indirectly. If
present, they may be the only problem. ** POSTVOID RESIDUAL-in + out catheterization following
void/incontinence. 150-250 cc gray area: use your judgement. *** PRATT DILATORS.with topical lidocaine: a simple office or out
patient skill worth learning for stricture in 9 'so **** 60 cc syringe on end of foley, held aloft, and filled with saline.
Slow, intermittent rising and falling of fluid represent the uncoordinated contractions of unstable bladder.
Notes on Geriatrics 167
II FECAL INCONTINENCE Fecal impaction (commonest cause in extended care: cleanout
solves problem, temporarily) Excess laxatives (commonest cause in acute care - too many cooks) Consciousness impaired - has to be VERY obtunded All diarrhea causes I Sigmoidoscopy
when all else Local (villous adenoma/Cal fails
168 Protocols in Primary Care Geriatrics
Chapter 7 - Confusion
I GENERAL WISDOM A One of the "geriatric giants:' and a major nonspecific presenta
tion of disease in the elderly. B Essentially the medical task is to rule out and treat reversible
causes; once that's done, things get a lot more difficult. C The elderly get confused easily because their brains function
with low reserves.
II TERMINOLOGY A Currently, "cognitive impairment" is considered the correct
term for problems with higher brain function. B "Confusion" should always be used in quotations. It is an inex
act, lay term; a presenting complaint. C This table outlines the various terms and their uses:
ACUTE, REVERSIBLE
SOURCE SYNDROME DSM-II Acute organic
brain syndrome DSM-III(R) Delirium Neuropsychology Cognitive
impairment
CHRONIC IRREVERSIBLE
SYNDROME Chronic organic
brain syndrome Dementia
Medical model Acute brain failure Chronic brain failure
III DELIRIUM A Essentially acute brain failure, usually due to physical cause,
often reversible. B Usually cognitive function varies, onset is rapid, setting is one
of acute illness, BUT C The ONLY CONSISTENT FEATURE distinguishing deliri
um from dementia is CLOUDING OF THE STATE OF CONSCIOUSNESS: 1. Attention wanders 2. Speech is often impaired 3. The most familiar model of delirium is a person who has
had 10 beers: an ACUTE DRUNK. D Causes of delirium include must-treat emergencies (sepsis,
TB, subdural, appendicitis, occult fractures, drug toxicities, ketoacidosis, etc.)
E Our mnemonic for the common causes: (CAMP)2
CVA, subdural CHF ALCOHOL ACUTE ABDOMEN
Notes on Geriatrics 169
METABOLIC (Na, K, glucose, O2, T4, etc.) MEDS PYREXIAL (infection) PSYCHOLOG ICAL
IV DEMENTIA A Global intellectual deterioration which is not delirium. B Only very rarely reversible. Much more commonly an irrevers
ible dementia coexists with one of the "reversible" causes (T 4'
B12, syphilis, etc.) C The famous mnemonic for reversible causes is still worth con-
sidering: Drugs Emotional (depression) Metabolic (Na, K, O2, glucose, T4, system failure) Eyes and ears (blind/deaf) Nutritional (B12, pellegra, etc.) 'lUmors/trauma Infection (common ones, but remember SBE, TB, syphilis,
AIDS) Acute abdomen, alcohol, ASHD (MI, CHF, arrhythmia, PE,
CVA) D MOST (about 70%) dementias are ALZHEIMER's.
SOME (about 15%) are CIRCULATORY (multiple infarct). SOME (about 10%) are ALCOHOLIC or TRAUMATIC. MANY are MIXED. A FEW are canaries (HUNTINGTON'S, PICK'S, etc.). A FEW are reversible.
E Other Tests (mnemonic "JAMAU') 1. JUDGEMENT
Understanding of medical problems Understanding financial situation Hypothetical problems (fire in theater, child on end of
pier) , 2. ATTENTION
DIGIT SPAN: repeat numbers forward and backward. Normal: 7 ::I:: 2 forward, 5::1:: 2 backward. Lift Your Hand whenever you hear "Pl'
3. MENTAL CONTROL-list months in reverse order 4. ABSTRACTION -proverbs
differences (child/midget)
170 Protocols in Primary Care Geriatrics
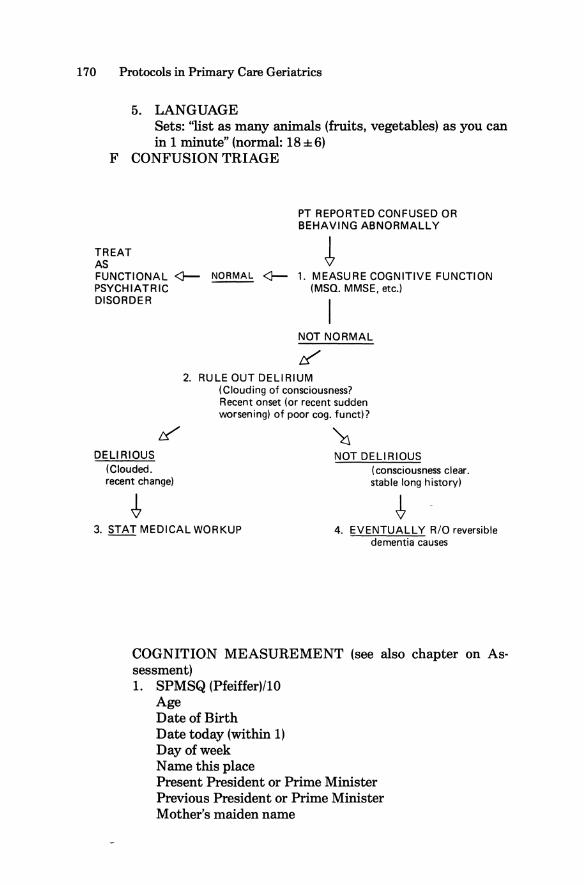
5. LANGUAGE Sets: ''list as many animals (fruits, vegetables) as you can in 1 minute" (normal: 18 ± 6)
F CONFUSION TRIAGE
TREAT AS
PT REPORTED CONFUSED OR BEHAVING ABNORMALLY
FUNCTIONAL <}PSYCHIATRIC DISORDER
NORMAL <}- 1. MEASURE COGNITIVE FUNCTION (MSQ. MMSE, etc.)
I NOT NORMAL
If 2. RULE OUT DELIRIUM
(Clouding of consciousness? Recent onset (or recent sudden worsening) of poor cog. funcd?
DELIRIOUS (Clouded. recent change)
3. STAT MEDICAL WORKUP
~ NOT DELIRIOUS
(consciousness clear. stable long history)
4. EVENTUALLY R/O reversible dementia causes
COGNITION MEASUREMENT (see also chapter on Assessment) 1. SPMSQ (Pfeiffer)/I0
Age Date of Birth Date today (within 1) Day of week Name this place Present President or Prime Minister Previous President or Prime Minister Mother's maiden name
Notes on Geriatrics 171
Any phone number (or series 7 digits, repeated later) Serial 3s from 20
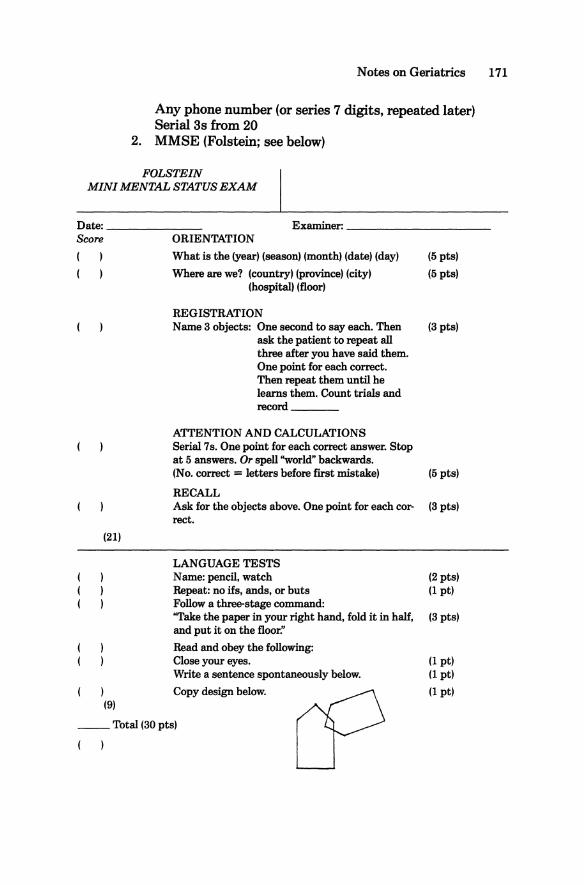
2. MMSE (Folstein; see below)
FOLSTEIN MINI MENTAL STATUS EXAM
Date: Examiner: Score ORIENTATION
What is the (year) (season) (month) (date) (day) (5pts)
Where are we? (country) (province) (city) (5pts) (hospital) (floor)
REGISTRATION Name 3 objects: One second to say each. Then (3 pts)
ask the patient to repeat all three after you have said them. One point for each correct. Then repeat them until he learns them. Count trials and record
ATTENTION AND CALCULATIONS Serial 7s. One point for each correct answer. Stop at 5 answers. Or spell "world" backwards. (No. correct = letters before first mistake) (5pts)
RECALL Ask for the objects above. One point for each cor- (3pts) recto
(21)
LANGUAGE TESTS Name: pencil, watch (2pts) Repeat: no ifs, ands, or buts (1pt) Follow a three-stage command: "Take the paper in your right hand, fold it in half, (3pts) and put it on the floor."
Read and obey the following: Close your eyes. (1 pt) Write a sentence spontaneously below. (1 pt)
) Copy design below. (1 pt) (9)
__ Total (30 pts)
( )
172 Protocols in Primary Care Geriatrics
Chapter 8 - Depression
I GENERAL WISDOM A Very common in the elderly, and its most serious consequence,
suicide, is COMMONEST in this age group. High risk: loners, males, recent negative change, no support, previous Hx depression.
B To appreciate why depression is common with aging, picture yourself with no future, no job, low self-esteem, no family, no friends, no standing in the community, and sick with problems the doctor isn't even interested in, much less able to cure.
C There is a complex relationship between depression and cognitive impairment (see chapter on Confusion; see "cognitive/affective syndrome:' below)
D Presents atypically, like most other things.
II SECONDARY DEPRESSION - always consider and rule it out: it's relatively easy to treat, and resistant to depression therapy. A Pain - any cause, especially musculoskeletal. B Drugs (the "As;
ALCOHOL (may be secondary to depression, or depression secondary to it.)
ANTI INFLAMMATORIE S ANTIHYPERTENSIVES (especially beta-blockers, methyl
dopa, clonidine, hydralazine) ACTING ON THE CNS
Neuroleptics (especially haloperidol) Benzodiazepines (especially long-acting)
ADRENOCORTICOSTEROIDS Prednisone Estrogens (well, it's a kind of steroid ... )
ANTIPARKINSON'S-L-dopa ANY OTHERS
III ATYPICAL PRESENTATION OF DEPRESSION A Recall DSM-III(R) definition of major depressive episode:
DYSPHORIA (feeling bad) PLUS ANHEDONIA (no pleasure from anything) PLUS Any three
of "GET PAST" Guilt Energy Loss Thought disorder Psychomotor Rate Change Anorexia - weight loss Sleep disturbance Thoughts of suicide
Notes on Geriatrics 173
B In the elderly, DSM -III(R) gives • False + ve's (many normal old people are anorexic,
lack energy, move slowly, don't enjoy sex, etc.) • False - ve's (you often don't/can't get the history
straight) Certain more typical HINTS may alert you to treatable affective disorders in aged ("BAD NEWS").
Behavior problems (AGITATION) ADL deterioration ("geriatric failure to thrive") Deterioration in dementia (cognitive-affective syndrome) Neglect (self-care suffers) Expectation of doom (pessimism, hopelessness) Withdrawal (social isolation) Somatization
IV DEPRESSION AND DEMENTIA A A depressed person may perform poorly on tests of cognitive
function and appear confused, leading to misdiagnosis as cognitive impairment, or dementia.
B Probably more common is coexistence of dementia and depression (cognitive-affective syndrome).
C In either case, the situation is amenable to treatment.
V TREATMENT OF DEPRESSION IN ELDERLY A TRICYCLICS
1. Still drug of first choice 2. Side effects most commonly seen:
• cognitive impairment • orthostatic hypotension • urinary retention
3. NORTRIPTYLINE (sedating, less anticholinergic) DESIPRAMINE (not sedating, more anticholinergic) TRAZADONE (minimally anticholinergic, slightly sedat
ing) ... are current favourites.
Start low, go slow. B MAO Is are next choice
1. Diet problems overstated. 2. OTC drugs (adrenergic agonists) interactions very danger
ous. 3. PHENELZINE is our favourite MAOI.
C LITHIUM 1. Useful as prevention of recurrent depression, or in addi
tion to first line drugs to potentiate effect 2. Fewer side effects, but confusogenic 3. Lower blood levels appropriate (0.3-0.6)
174 Protocols in Primary Care Geriatrics
D ECT 1. Were it not for its terribly bad press, it might be the
treatment of choice. 2. Very useful in elderly who don't tolerate drugs. 3. Try to use pulsed ECT, EEG readout for safety and effica
cy. E SEROTONIN ANTAGONISTS
New, promising; jury still out at time of writing. F AMPHETAMINES/METHYLPHENIDATE
Occasionally useful, short-term, especially for poor motivation/rehabilitation failure.
Notes on Geriatrics 175
Chapter 9 - Constipation
I GENERAL WISDOM A Expand your definition of normal: as long as a bowel move
ment occurs EVENTUALLY, and there are no real associated symptoms, it's NORMAL.
B The current generation of elderly were raised on the doctrine of "autotoxicity": stool is POISON; 24 hours with no BM to them is like smoking three packs of cigarettes a day to us: dangerous and ill-advised.
C Result: lots of chronic laxative abu·se.
II THE NEVER (well, almost)-FAIL RECIPE for: HARD, INFREQUENT MOVERS LAXATIVE ABUSERS EXTENDED CARE IMPACTED OOZERS
A REGULARIZING MEASURES FOR ALL (establish these first) 1. Fluid p.o.: 6 glasses a day, more in summer 2. Activation: nothing like a nice, easy stroll 3. Bran, bulk, fiber, etc. with true obsessive persistence
B CLEANOUT 1. Next, get the ball rolling. 2. Use whatever it takes, for at least 3 days,
• Mild ORAL LAXATIVE AT H.S., SUPPOSITORY IN
A.M. AFTER BREAKFAST MAG,NOLAX orally, glycerin suppository
• Brisk GLYSSENID CASCARA PHENOLPHTHALEIN DULCOLAX SUPPOSITORY
• Thermonuclear CITRO-MAG LACTULOSE in increasing doses with suppository
C ESTABLISH ROUTINE 1. Demonstrate that you can maintain regularity EVERY 2
DAYS, OR EVERY 3 DAYS, with an ORAL LAXATIVE at H.S. and SUPPOSITORY in A.M. after breakfast.
2. Withdraw, slowly and steadily, down to the least aggressive regime that will maintain regularity (e.g., only a glycerine suppository after breakfast Q3 days), preferably down to nothing but regularizing measures.

176 Protocols in Primary Care Geriatrics
3. DON'T QUIT This regime has conquered some very hysterical drugstore laxative manipulators, and some very concrete extended care bed cases, but it takes a huge helping of firm friendly persistence.
Notes on Geriatrics 177
Chapter 10 - Pressure Sores
I GENERAL WISDOM A These are infarcts of skin, of intiltifactorial etiology. B There are hundreds of "cures" which attests to the lack of a
consistently superior one. C Decubiti are massively expensive of nursing time, both in pre
vention and healing.
II ETIOLOGY
THE BLOOD Nutrition Hemoglobin Oxygen
THE CIRCULATION Atherosclerosis Vasculitis Diabetes Hypotension CHF
THE SKIN Edema Infection Moisture Local pressure Shearing force
Pressure, over time, produces a bed sore by occluding blood flow to a local tissue area. How long it takes depends on all the other factors. It can occur in an hour in an unrecognized hypotensive or arrhythmic episode, but may take 24 hours or more in a healthy person.
III CLASSIFICATION (SHEA) GRADE I - erythema and warmth for 24 hours GRADE II-Through dermis into subcutaneous fat GRADE III-undermined into subcutaneous fat GRADE IV-to fat deep fascia, muscle, bone
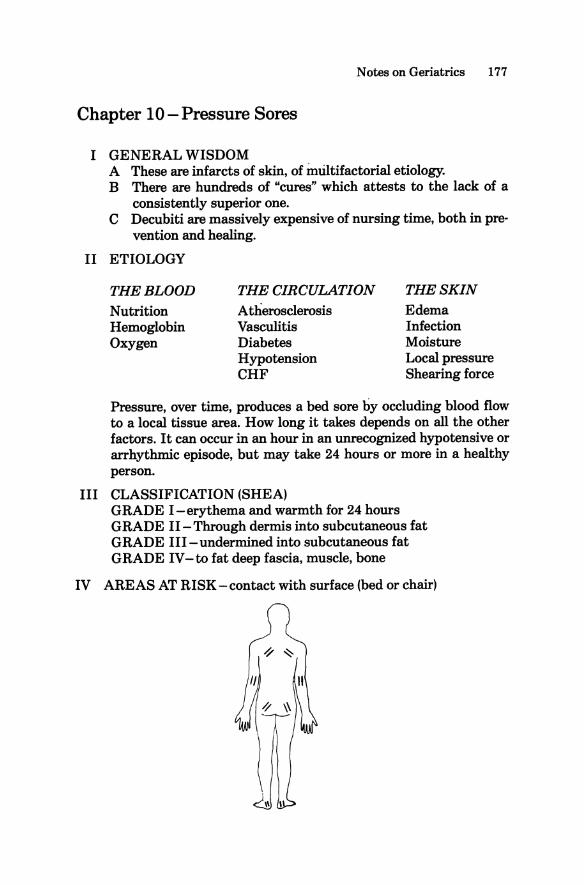
IV AREAS AT RISK - contact with surface (bed or chair)
178 Protocols in Primary Care Geriatrics
V MANAGEMENT (mnemonic "POINTS") Pressure - relieve it
-turning - special beds - cushions, etc.
Operate to debride necrotic tissue - most-of ten-overlooked step - get a scalpel and forceps and cut to fresh (bleeding)
tissue Infection - treat systemically only if delocalized as cellulitis or
speticemia -DON'T CULTURE (you'll always grow the same
cocktail party - every bug you can think of) -treat anaerobes, G-, staph. if you treat systemically -topically mupirocin (Bactroban), metronidozole
(Flagyl)-soaked dressings, sulfa cream useful Nursing care
- cover the wound with saline-soaked gauze - occlude it, but watch for anaerobic infection under-
neath
Treat general condition _ anemia, malnutrition, hypoxia, CHF, etc. may be
USEFULLY TREATED in this setting, where you would otherwise leave them alone
Surgeon - call the plastics person for a flap when all else fails
Notes on Geriatrics 179
Chapter 11-Agitation
I GENERAL WISDOM A Generally defined as inappropriate, negative behavior, usually
in very brain-failed patients: shouting, wandering, fighting during care, throwing food, etc.
B Research is just getting started and so far is mainly descriptive.
C Drug treatment involves important trade-offs: 1. Quality of life: the patient vs everyone else. 2. Economics: is it cheaper/easier to care for a more mobile,
noisy patient, or a more obtunded, quiet one (often about even)?
II CORRECTING REVERSIBLE CAUSES (consider "PRISM") Pain - a careful hands-on physical helps. Retention of urine - you may need a postvoid residual catheteriza
tion. Impaction - rectal examination. Staff or caregiver stress, or other causes of anger, including
abuse. Metabolic-T4, glucose, uremia, others.
III PATTERNS OF AGITATED BEHAVIOR A KIND OF ACTIVITY
1. VERBAL -noise only 2. PHYSICAL-may include simply wandering, or more dif
ficult sexual, combative, destructive behavior B ANCILUS AUTOMOTIVE CLASSIFICATION OF WAN
DERERS 1. SAAB (syndrome of aggressive ambulatory behavior): pa
tient covers great distances, and is undeterred by doors, fire escapes, fences, roadways. Risk of injury.
2. BMW (benign meaningless wandering): less pressured, slower movement; tends to careen passively off barriers, walls, other patients. Easier to settle.
IV BEHAVIORAL APPROACHES TO AG ITATION A These must be used continuously; this population doesn't
learn well. B Move slowly, approach from in front. C Explain gently what's going on; it's the tone of voice, not the
content. Reassure, reassure, reassure. D Try various staff: vary sex, size, age, race.
180 Protocols in Primary Care Geriatrics
E Ocassionally positive and negative reinforcement will work in the more cognitively intact group.
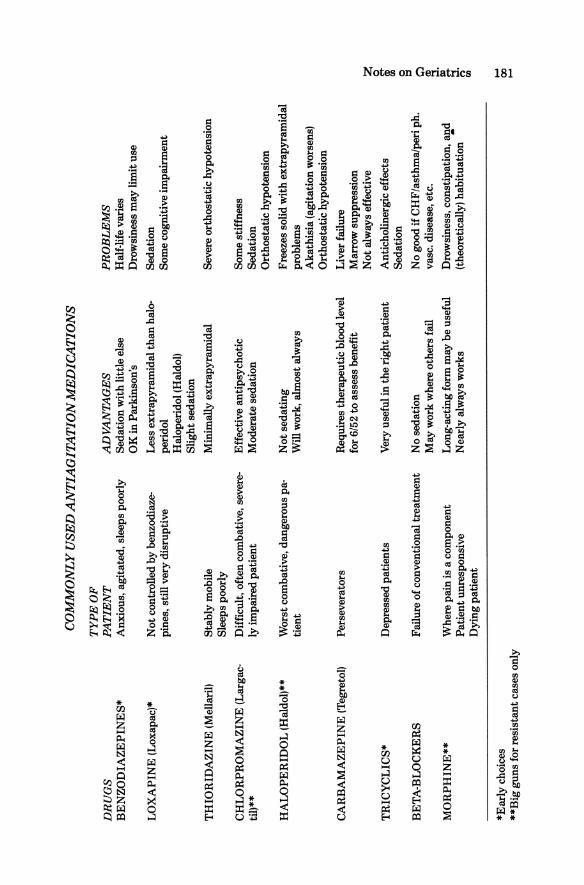
F Lighting, music, animals, plants, may all be of value. V DRUG THERAPY
A Although the risks of medication are serious, we often are left with no choice.
B The key is to titrate carefully, and remember the rules of drugs in the elderly (see chapter on Drugs).
DR
UG
S B
EN
ZO
DIA
ZE
PIN
ES
*
LO
XA
PIN
E (
Lox
apac
)*
TH
IOR
IDA
ZIN
E (
Mel
lari
l)
CH
LO
RP
RO
MA
ZIN
E (
Lar
gac
til)*
*
HA
LO
PE
RID
OL
(Hal
dol)
**
CA
RB
AM
AZ
EP
INE
(T
egre
tol)
TR
ICY
CL
ICS
*
BE
TA
-BL
OC
KE
RS
MO
RP
HIN
E**
*Ear
ly c
hoic
es
**B
ig g
uns
for
resi
stan
t cas
es o
nly
CO
MM
ON
LY
USE
D A
NT
IAG
ITA
TIO
N M
ED
ICA
TIO
NS
TY
PE
OF
P
AT
IEN
T
Anx
ious
, ag
itat
ed, s
leep
s po
orly
Not
con
trol
led
by b
enzo
diaz
epi
nes,
sti
ll v
ery
disr
upti
ve
Sta
bly
mob
ile
Slee
ps p
oorl
y
Dif
ficu
lt, o
ften
com
bati
ve, s
ever
ely
impa
ired
pat
ient
Wor
st c
omba
tive
, dan
gero
us p
ati
ent
Per
seve
rato
rs
Dep
ress
ed p
atie
nts
Fai
lure
of c
onve
ntio
nal t
reat
men
t
Whe
re p
ain
is a
com
pone
nt
Pat
ient
unr
espo
nsiv
e D
ying
pat
ient
AD
VA
NT
AG
ES
Sed
atio
n w
ith
litt
le e
lse
OK
in P
arki
nson
's
Les
s ex
trap
yram
idal
than
hal
ope
rido
l H
alop
erid
ol (H
aldo
l)
Sli
ght s
edat
ion
Min
imal
ly e
xtra
pyra
mid
al
Eff
ecti
ve a
ntip
sych
otic
M
oder
ate
seda
tion
Not
sed
atin
g W
ill w
ork,
alm
ost a
lway
s
Req
uire
s th
erap
euti
c bl
ood
leve
l fo
r 6/
52 t
o as
sess
ben
efit
Ver
y us
eful
in th
e ri
ght p
atie
nt
No
seda
tion
M
ay w
ork
whe
re o
ther
s fa
il
Lon
g-ac
ting
form
may
be
usef
ul
Nea
rly
alw
ays
wor
ks
PR
OB
LE
MS
Hal
f-lif
e va
ries
D
row
sine
ss m
ay li
mit
use
Sed
atio
n So
me
cogn
itiv
e im
pair
men
t
Seve
re o
rtho
stat
ic h
ypot
ensi
on
Som
e st
iffn
ess
Sed
atio
n O
rtho
stat
ic h
ypot
ensi
on
Free
zes
solid
wit
h ex
trap
yram
idal
pr
oble
ms
Aka
this
ia (
agit
atio
n w
orse
ns)
Ort
host
atic
hyp
oten
sion
Liv
er f
ailu
re
Mar
row
sup
pres
sion
N
ot a
lway
s ef
fect
ive
Ant
icho
line
rgic
eff
ects
S
edat
ion
No
good
if C
HF
/ast
hma/
peri
ph.
va
sco
dise
ase,
etc
.
Dro
wsi
ness
, con
stip
atio
n, a
nd
(the
oret
ical
ly)
habi
tuat
ion
•
i g o (I) :::t ~
~.
......
00
......
182 Protocols in Primary Care Geriatrics
Chapter 12 - Theory of Drug Therapy and Aging
I GENERAL WISDOM A WHY ARE DRUGS A PROBLEM IN THE ELDERLY?
1. MULTIPLE PATHOLOGY leads to MULTIPLE PRESCRIPTIONS (often unavoidably).
2. AGING CHANGES make drug behavior unpredictable.
~ AGINGSs '"
DRUGSs ~ PATHOLOGICALSs
3. The elderly operate with little cognitive and ADL reserve, and so are supersusceptible to adverse drug reactions.
B THEREFORE: 1. Once on more than three drugs, the situation becomes un
predictable. 2. Drugs are likelier to be part of the PROBLEM than part of
the SOLUTION. 3. When something goes wrong, think drugs first. 4. An unnecessary drug is defined as one which, when discon
tinued, involves no adverse consequence. 5. Although risks of untreated illness (NIDDM or hyperten
sion, e.g.) may be as serious in the elderly, the risks of drugs are greater than in young adults. Thus, the risk: benefit balance often tips toward not treating.
6. SMALL DOSES, LONG INTERVALS is the rule: b.i.d. is all you need for most drugs.
II FOLLOWING THE DRUG FROM PRESCRIPTION 1'0 RECEP1'ORSITE A COMPLIANCE
1. In the community, compliance runs at an average of 50%. 2. Use "brown bagging," large labels, no childproof tops, clear
explanation, dosettes or blister packs, but above all, MINIMIZE MEDICINES; SIMPLIFY REGIMENS.
3. BEWARE OF NURSING HOME OR ACUTE CARE ADMISSIONS from the community: compliance instantly becomes 100%. Sudden deterioration may occur.
B ABSORPTION - about the same as young adults. C DISTRIBUTION
1. Elderly have MORE FAT PER BODY WEIGHT LESS WATER VOLUME LESS PROTEIN
2. Fat-soluble drugs (e.g., haloperidol) eliminated slowly.
Notes on Geriatrics 183
3. Water-soluble and protein-bound drugs concentration increased.
D ELIMINATION 1. Renal function less
[NOTE: little old lady] ! ! !
CREAT.CLEAR.= (WT.) (140-age) (0.85 for 9 ) 0.8 SERUM CREATININE
This equation may still overestimate renal function. 2. Hepatic enzyme systems impaired. 3. Generally elimination/detoxification is VARIABLE and
SLOW. E PHARMACODYNAMICS-drug-receptor interaction in the
elderly is still not well understood: TIGER COUNTRY.
184 Protocols in Primary Care Geriatrics
Chapter 13 - Practical Prescribing to the Elderly
You can't be as confident giving drugs to old people as you can with young adults. These ten rules are a rudimentary guide to the challenging juggling act of geriatric pharmacotherapeutics:
1. TREAT ONLY WHEN LIFE, FUNCTION, OR COMFORT ARE THREATENED • If a local treatment exists, use it (e.g., steroid injections vs
NSAIDS). • The fact that a system subspecialist uses a drug routinely for a
condition is not necessarily sufficient reason to risk it in your elderly patient: e.g., triple angina therapy for chest pain, or an H2-receptor antagonist for dyspepsia.
2. STARTLOW • Half doses of most drugs are good starting doses. • Rarely, benefit may occur with minute doses. • Much more commonly, side effects/interactions occur with
minute doses.
3. GOSLOW • A LESS FREQUENT DOSING SCHEDULE is important
(e.g., RANITIDINE O.D., CAPTOPRIL B.I.D.) • Also increase doses only after a long wait for steady state (e.g.,
once a week)
4. BEGIN THERAPY WITH CLEAR ENDPOINTS IN MIND • . A drug may either do benefit, do harm, do both, or do neither. • Know how to MEASURE which of these outcomes has oc
curred at each given dose, and decide WHAT will make you stop, increase, continue the drug, BEFORE you start it.
• Often the endpoint is ADL and cognitive function. You need a baseline before starting meds.
• You also must KNOW YOUR DRUGS, to anticipate side effects.
5. ORGANIZE FOLLOW-UP • Strange to say, you won't know what the outcome was if you
don't go back and LOOK. • Old people, especially in nursing homes, don't always return
and tell you what has happened.
6. RISK REDUCING DRUGS REGULARLY • An unnecessary drug is identified when, after stopping it, no
adverse consequence occurs. • The conditions you were treating may have changed/gone
away, or you may have been wrong in the first place.
Notes on Geriatrics 185
• ENDPOINT has the same significance here, in reverse, as when starting a drug. The patient may benefit or suffer from your action: how will you decide? '
7. LIMIT ORDERS • Write the order only for the amount of time until your next
visit. • There's more risk from a continued medication than from a
stopped one.
8. REVIEW THE DRUG PROFILE AT EVERY VISIT-you can't assess ANY problem without a look at what the patient is on. The sheer amount will surprise you.
9. DO ONE THING AT A TIME If two or more medication changes are made at once, the benefit or (more likely) problems which occur may be due to two or more things. Which is it? You end up doing them separately anyway.
10. KEEP IT SIMPLE-The more the medicine the more likely is trouble, and the less likely that the patient will take the medicine.
186 Protocols in Primary Care Geriatrics
Chapter 14-Selected Therapeutic Problems
I CONGESTIVE HEART FAILURE (see also "CVS" in ATYPICAL PRESENTATION OF DISEASE) A The diagnosis and clinical follow-up of CHF can be very diffi
cult in the elderly. B DIGOXIN
1. Risk > benefit, nearly always, for CHF. 2. Can usually be safely discontinued if no CHF clinically;
sinus rhythm. C DIURETICS
1. Tend to be overprescribed and continued after the problem is LONG GONE.
2. Thiazides are long-acting and have numerous metabolic side effects.
3. Furosemide in low doses is our first choice. D ACE INHIBITORS
1. Small doses (6.25 mg b.Ld., e.g.) 2. Often best-tolerated, or only-tolerated, CHF treatment.
II SLEEP DISORDERS A The elderly sleep less for more time in bed and wake more
during the night. B Every benzodiazepine accumulates. C Rule out treatable sleep-loss causes (CHF, depression, pain). D Then try "natural" sleep (a quiet, secure evening, warm milk,
boring book, sleep-producing routine, exercise, go to bed later).
E When all else fails, validate lack of sleep and encourage night productivity (read, knit, write letters).
F When THAT fails, consider a benzodiazepine; but NEVER MORE THAN 3 NIGHTS • Triazolam (HALCION), fastest onset for initial insomnia;
habituating • Temazepam (RESTORIL), comes in capsule so can be
minititrated • Alprazolam (XANAX), probably the simplest (fewest me
tabolites) G AVOID
• Long-acting benzodiazepines • Diphenhydramine (except occasional nights) • All other hypnotics, neuroleptics, etc.
III BRONCHOSPASM A The drugs are toxic, so PROVE BENEFIT either with spiro
metry or with repeated auscultation.
Notes on Geriatrics 187
B SALBUTAMOL is best delivered IN A ROTAHALER, AEROCHAMBER, OR NEBULIZER: the puffer requires coordination.
C STEROIDS may be worth the risk in very elderly people who are miserable and resistant to treatment.
IV DYSPEPSIA A Discontinue offending NSAIDS; (unless they're necessary)
limit caffeine and alcohol B RULE OUT ULCER, then C See if ANTACIDS
SUCRALFATE WATER, etc, will work
D IF NOT, give a trial of RANITIDINE but limit the order, and don't use it p.r.n.
E AVOID CIMETIDINE (confusogenic and interactive)
V MUSCULOSKELETAL PAIN A MAKE THE DIAGNOSIS (R/O PMR, e.g.). B Treat locally
INJECTION (local anesthetic-corticosteroid) T.E.N.S. ICE/HEAT MASSAGE.
C ACETAMINOPHEN regularly may be effective, especially for activity related pain.
D NSAIDS as last resort, but ALWAYS WITH GASTRIC PROTECTION.
E When the third NSAID fails, consider atypical depression.
VI HYPERTENSION A Weigh the risk of the condition against the risk of treatment. B Beta-blockers are multiply-disabling. C Thiazide diuretics cause too many problems. D A single agent will minimize noncompliance. E In CHF patients, enalapril is our choice; in angina patients,
nifedipine. Start low, go slow.
188 Protocols in Primary Care Geriatrics
Chapter I5-Nursing Home Care
I GENERAL WISDOM A In our society, people unable to care for themselves (do ADLI
IADL) are helped by family, by help from professionals, or are given help by government.
B At some point it becomes easier or beneficial for some of the parties involved if the help is provided in a facility: a nursing home.
C Nursing homes may become "dependence traps:' There is a tendency for people, once in, to stay in, even if physical capability improves.
II LEVELS OF CARE
LEVEL
ACUTE EXTENDED CARE (Skilled Nursing Facility) INTERMEDIATE CARE (Sometimes divided into three sublevels)
IC-3
IC-2
IC-I
PERSONAL CARE SENIOR CITIZEN'S
HOUSING COMMUNITY
FUNCTION
VARIES NOT independently mobile
Difficult, very confused, requires extensive supervision Moderate confusion ± or mobility impaired Mild impairment, requires daily care Independent except for meals Lives in community with some added amenities and safety aids All ADLs; most IADLs
III STANDARDS OF MEDICAL CARE IN NURSING HOMES A In most settings, these are not finalized. B Areas of interest and need for standards, in our view:
1. DOCUMENTATION, including provision for transfer of information
2. PHYSICIAN AVAILABILITY and VISITS 3. MEDICATION, including review 4. MEDICAL ADMINISTRATION and MEDICAL
STAFF 5. PERIODIC REVIEW OF CARE 6. CARE PLAN ... please see Part One for a discussion of each of these.
Notes on Geriatrics 189
IV ADDITIONAL COMMUNITY RESOURCES A COMPREHENSIVE GERIATRIC ASSESSMENT UNITS
Assess people in ADL crisis; expensive; probably cost-effective.
B ADULT DAY CARE Cognitively impaired people attend activities, socialization.
C PHARMACIES Some take an interest and are helpful.
D CHURCH, SENIORS' NETWORK, OTHER COMMUNITYBASED GROUPS
190 Protocols in Primary Care Geriatrics
Chapter 16-Terminal or Palliative Care
I GENERAL WISDOM A Palliative care (PC) is care directed at comfort, rather than
cure. It is appropriate for all patients in whom cure is out of the question, but remember our duty "to comfort always"; it is a basic part of all medical care.
B When confronted with an elderly, dying patient, you must decide: do good PC yourself, or find someone who can. There is no other acceptable choice.
C Oncologists are not always good at PC. D You must be prepared to be personally involved, to confront
and discuss unpleasant issues, and to work with family and other professionals. This is not an area for technocrats.
II PAIN A Identify each pain source meticulously, by hands-on physical
examination. B Treat all pain, especially mild pain. C Achieve CONTINUOUS pain relief, and prevention, by round
the-clock dosing. D Use whichever route is effective: oral, rectal, i.m., continuous
i. v. Consider subcutaneous or i. v. minipumps, if available. E Acetaminophen/ ASA, codeine/oxycodone; morphine/hydro
morphone are the drugs of choice. Meperidine (DEMEROL) is nearly worthless for real pain.
FUse coanalgesics or adjuvants with analgesics
l. Bone pain NSAID 2. Intracranial pres-
sure Dexamethasone (Decadron) 3. Radicular pain Prednisone 4. Postzoster Tricyclic 5. Dysesthesia Carbamazepine (Tegretol) 6. Intermittent stab-
bing pain Valproate (Depakene) 7. Gastric distention Simethicone (Ovol)
Metoclopramide (Maxeran) 8. Muscle spasm Diazepam (Valium)
Baclofen (Lioresal) 9. Skin ulcer N 20 for dressing change
NSAID, metronidazole 10. Stomatitis Nystatin (Mycostatin), viscous
Lidocaine (Xylocaine)
Notes on Geriatrics 191
G TOTALPAIN 1. Enlist the power of the patient's own cortical suppression
of pain. 2. Finances, guilt, odor, self-loathing, sexual issues, cultural
issues, family stress, and caregiver conflict are among potent contributors to pain on which a sensitive palliative team may have an influence.
III OTHER SYMPTOMS A ANOREXIA-adjust diet, try prednisone or megestranol B DEHYDRATION -treat thirst and treat it PO C MOUTH DRY-DC drugs; use sour candies D DYSPHAGIA - change tablets to liquid, use liquid nourish
ments E HICCUP-CPZ, CO2, simethicone (Ovol), methylphenidate
(Ritalin), valproic acid (Depakene) F NAUSEA and VOMITING-phenothiazines, antihistamines,
metoclopromide (Maxeran), haloperidol (Haldol). G ASCITES-drain when tense H DYSPNEA-reassurance important; treat cause, including
thoracentesis I COUGH-codeine J SECRETIONS (near death)-hyoscine K INSOMNIA-treat cause; this is the one and only use of
triazolam, in our opinion L DELIRIUM - haloperidol is the best one here
M PRURITUS-terfenadine (Seldane) N BLADDER SPASM - Belladonna + opium o TENESMUS - steroid suppository
192 Protocols in Primary Care Geriatrics
Chapter 17 - Ethical Issues in Geriatrics
I GENERAL WISDOM A Biomedical Ethics is a branch of applied philosophy designed
to respond to questions of moral duty in medicine. These questions tend to arise at both ends of life and involve the consideration of important human values like: • Autonomy (a person's right to self-determination) • Beneficence (the principle of doing good for/to others; pre-
sumably the basis of medicine) • Allocation of resources (money, in essence) • Rights of the fetus • Paternalism • Truth-telling
B There is no doubt that we health-care providers find ourselves in difficult dilemmas which our training does not address. We often need guidance from principles, colleagues, committees, etc. in dealing with these.
C We see however, a few potential problems if consideration of ethical issues becomes as popular as sports medicine: 1. 1iivialization of important personal and life values 2. The tendency to find and dwell on heavy PHILOSOPHI
CAL issues in routine patient encounters 3. Ethical behavior "on paper" vs ethical behavior in fact.
Does an algorithm really get us off the hook? D Still, applied ethics is philosophy in action, and we believe in
tackling problems head on. If we don't, this new wave of bureaucrats will. Remember you are never under an obligation to do anything medically futile.
II A MODEL FOR ADVANCE DECISION - MAKING IN THE ELDERLY A DETERMINE COMPETENCE
Can the person understand, discuss, and appreciate the significance of the question?
B IF COMPETENT, then the patient (NOT the relatives or the doctor) decides.
C THEN, (IF COMPETENT), ask the patient to designate a substitute decision-maker for unforseen questions, should the patient become incompetent. Make it clear that this person's judgement would be followed even if it conflicted with medical judgement.
D IF INCOMPETENT, SEEK A PREVIOUS JUDGEMENT on the same question. A written statement, or a reliable report
Notes on Geriatrics 193
of a strong verbal statement (e.g., while watching TV "for God's sake don't ever let them do that to me ... ").
E IF NO PREVIOUS JUDGEMENT, seek a PREVIOUS SUBSTITUTED JUDGEMENT. Rarely, there will be a nonfinancial power of attorney or a reliable verbal delegation.
F IF NO SUBSTITUTED JUDGEMENT, make a BESTINTEREST JUDGEMENT. Do what you would do for your mother, your spouse, yourself.
Index
Acebutolol (Monitan, Sectral), for agitation, 74
ACE inhibitors, for congestive heart failure, 90, 186
Acetaminophen (Tylenol) for musculoskeletal pain, 93, 187 for pain control, 106
Activities of daily living (ADLs), 11, 102,155-156
assessing, 15-16 definition of, 15, 156 measurement of, 156
Acute, as term, 9 Acute, reversible syndrome, 168 Acute abdomen, 26, 160 Acute organic brain syndrome,
49-50 ADLs. See Activities of daily living Adrenocorticosteroids, for
depression, 172 Adult day care, 189 Advance decision-making, 8
model for, 112-113 Aging
causes of, 9-10,153 depression and, 153 loss and, 10 personality and, 153 psychological downside of, 10-11,
153 Agitation, 69-75, 179-181
behavioural approaches to, 71-72, 179
clinical exercise, 74-75 correcting reversible causes of,
70,179 description of, 69 drug therapy for, 72-73,181 general wisdom, 179 patterns of agitated behaviour,
70-71,179 Akathisia, 73 Albuterol (salbutamol in Canada;
Ventolin), for bronchospasm, 92
Alcohol, depression and, 172 Alphamethyldopa (Aldomet), for
hypertension, 94 Alprazolam (Xanax), for sleep
disorders, 91, 186 Alzheimer's disease, 51 Amphetamines, for depression, 59,
174 Analgesics, for pain control, 106 Ancill, Ray, Dr., 71 Ancill's Automotive Classification of
Wanderers, 179 Anhedonia, 56
depression and, 172 Anorexia, in end-stage patients, 108
treatment for, 191 Anticholinergics, for incontinence, 44 Antidepressants, in agitation, 73 Antihistamines, for nausea and
vomiting, 108 Antihypertensives, for depression,
172 Antiinflammatories, depression and,
172 Arrhythmia, 160
195
196 Index
ASA, for pain control, 106 Ascites, treatment for, 191 Assessment, process of, 157 Atypical presentation of depression,
172-173 Atypical presentation of disease,
25-31,160-161 acute abdomen, 26 adverse drug reactions, 27 cardiovascular disease, 28-29 clinical exercise, 29 - 31 examples, 160-161 general wisdom, 160 infections, 28 malignant neoplasm, 29 pulmonary embolism, 27-28 thyroid disease, 26 -27
Autoimmunity, 9 Autotoxicity, 61, 175
Baclofen (Lioresal), for pain control, 107
Barbiturates, for sleeplessness, 91 Benign Meaningless Wandering
(BMW), 71, 180 Benzodiazepines
for agitation, 72, 181 for depression, 172 for sleep disorders, 91-92, 108, 186
Beta-blockers for agitation, 74, 181 for coronary insufficiency, 84 for hypertension, 94
Biomedical ethics, 111-115, 192-193 clinical exercise, 113-115 general wisdom, 192 model for advanced
decision-making in elderly, 112-,.113, 192
public and popularization of, 111 Bladder physiology, 41-42 Bladder spasm
controlling, 108 treatment for, 191
BMW. See Benign Meaningless Wandering
Brain failure, as term, 50 Bronchodilators, 92 Bronchospasm, 93, 186-187
"CAMP,- as mnemonic, 168-169 Cancer, as silent mass, 161 Captopril (Capoten), for congestive
heart failure, 90 Carbamazepine (Tegretol)
for agitation, 73, 181 for pain control, 107
Cardiovascular disease, 28 -29, 160 Catheterization, for incontinence,
43-44 Cell-doublings,9-10 Chlordiazepoxide, for sleep
disorders, 91 Chlorpromazine (Largactil)
for agitation, 72-73 for hiccups, 108 for nausea and vomiting, 108
Chronic, as term, 9 Chronic irreversible syndrome, 168 Chronic organic brain syndrome,
49-50 Cimetidine (Tagamet), for dyspepsia,
93 Cisapride (Propulsid), for pain
control, 107 Clinical exercise answers, 117-143 Clouding of the state of
consciousness, 50, 52 Codeine
for cough, 108 for pain control, 106
Cognition measurement, 53 Cognitive function
assessment of, 14-15 tools for measurement, 155
Cognitive impairment as term, 49, 168 testing for, 52
Collagen protein, 9 Comprehensive geriatric assessment.
See Geriatric assessment Confusion, 49 - 54, 168 -171
clinical exercise, 53 - 54 cognition measurement, 53,
170-171 confusion triage, 52- 53, 170 delirium, 50-51, 168-169 dementia, 51-52,169-171 general wisdom, 168
"JAMAL," as mnemonic, 169 from medication, 27 as term, 168 terminology, 49-50,168
Congestive heart failure (CHF), 28-29,89-90,186
clinical exercise, 94 -95 Constipation, 61-64,108,175-176
approach to functional bowel movement problems in elderly, 61-63
clinical exercise, 63 - 64 gen~al wisdom, 175 laxatives for, 61, 62 treatment of, 175 -176
Continuous incontinence, 42 Coping mechanisms, 10 Corticosteroids, for musculoskeletal
pain, 93 Cough, controlling, 108, 191 "CRASHED," mnemonic for cause of
falling, 36-37, 162-163
"DARTS," as mnemonic, 159 "DATE," mnemonic for cause of
falling, 37, 163 "DEATH," as mnemonic, 156 Decision-making in elderly, model
for, 112-113 Dehydration, 191 Delirium, 50-51, 168-169
causes of, 51,168-169 distinguishing feature of, 168 as term, 50 testing for, 52 treatment for, 191
Dementia, 169-171 agitation in, 69 -70 causes of, 51 defInition of, 50 depression and, 57, 173 diagnosed as depression, 55 as mnemonic, 169 reversibility of, 169 tests for, 169 as treatable illness, 55
Demography, geriatric knowledge and, 153
Index 197
Depression, 55-60, 172-174 aging and, 153 atypical presentation of, 56-57,
172-173 clinical exercises, 59 - 60 dementia and, 57, 173 DSM-III(R) definition of, 56-57 in elderly, 173 general wisdom, 172 medication for, 85 secondary, 56, 172 as treatable illness, 55 treatment of, 57-59
Despiramine (Norpramine, Pertofrane), for depression, 58,173
Dexamethasone (Decadron), for pain control, 107
Diagnostic and Statistical Manual of Psychiatry (DSM-II, DSM-III), 49-50
dementia as defIned in DSM-III(R), 51
Diazepam (Valium) for pain control, 107 for sleep disorders, 91
Digoxin for congestive heart failure (CHF),
89-90,186 initial dosage for elderly, 84
Diltiazem (Cardizem) for hypertension, 94 initial dosage for elderly, 84
Dimenhydranate (Gravol), for nausea and vomiting, 108
Diphenhydramine (Benadryl), for sleep disorders,·91
Disability, 153 "DISASTERS," as mnemonic, 158 Disease, atypical presentation of.
See Atypical presentation of disease
Diuretics, for congestive heart failure (CHF), 90, 186
Domperidone (Motilium) for nausea and vomiting, 108 for pain control, 107
Drug reactions, 27, 160 from anticholinergics, 44
198 Index
Drug therapy and elderly, 79 -82 clinical exercise, 82 compliance, SO, 182 distribution, 81 drug absorption, 81 elimination, 81 pharmacodynamics, 81-82 practical prescribing to elderly,
184-185 as problem for elderly, 182 for secondary depression, 172
Dyspepsia, 92-93, 187 Dysphagia, 191 Dysphoria, 56, 172 Dyspnea, 108, 191
ECT. See Electroconvulsive therapy Elderly
activities of daily living (ADLs) and, 11
assessment of chances for and by, 20
demographics of, 2, 8 depression in, 173 heterogeneity among, 8, 79 limited cognitive and functional
reserve in, 79 medication for, unpredictability of,
79 multiple symptoms of, 158 practical prescribing to, 184 -185 rehabilitation of, 158 -159
Elderly hologram, illness in, 153 Electroconvulsive therapy (ECT)
for agitation, 74 for depression, 58 - 59, 174
Enalapril (Vasotec) for congestive heart failure (CHF),
90 for hypertension, 94 initial dosage for elderly, 84
Endocrine system, 10 Ethical issues in geriatrics. See
Biomedical ethics Exercise capacity, in elderly, 8 Extrapyramidal, as term, 157
Falls and instability, 35-39,162-163 algorithm for assessment, 162
"Bolt Out of the Blue" falling causes ("DATE"), 163
clinical exercise, 38 - 39 general falling causes
("CRASHED,,), 162 general wisdom, 162 practical approach to assessment
of falls, 36 - 38 Family physicians, as heterogeneous
group, 2 Famotidine (pepsid), for dyspepsia,
92 Fecal incontinence, 45, 167 Fluoxetine (Prozac), for depression,
58 Flurazepam (Dalmane), for sleep
disorders, 91 FolsteinM.,14 Force, as term, 157 Furosemide (Lasix)
for congestive heart failure, 90 initial dosage for elderly, 84
Gait, as term, 157 Geriatric assessment, 155-157
ADl/IADL(function),15-16 clinical exercise, 17-18 cognitive function, 14-15, 155 definition of, 13 generalvnsdom,155 process of assessment and
intervention, 17 Geriatric diagnosis and care, concept
of, 8-9 "Geriatric failure to thrive"
syndrome, 9, 57 Geriatric hospital admission, 11,
153-154 clinical exercise, 11-12
Geriatrics, interest in, 2 demography and, 153 interest in, 2
"GET PAST," as mnemonic, 172
Haloperidol (Haldol) for agitation, 73,181 for delirium, 108 initial dosage for elderly, 84 for nausea and vomiting, 108
Hayflick L., 9 Heterogeneity, 153 Hiccups, controlling, 108, 191 Homeostenosis, 20 H2-receptor antagonists, for
dyspepsia, 92-93 Huntington's disease, 52 Hydrochlorothiazide (Hydrodiuril)
initial dosage for elderly, 84 Hydromorphone (Dilaudid), for pain
control, 106 Hyoscine, 108 Hypertension, 94, 187 Hyperthyroidism, 26-27 Hypothyroidism, 26 -27
dementia in, 52
IADLs. See Instrumental activities of daily living
Illness-in-the-elderly hologram, 8 -9, 153
Immobility advanced, 159 causes and consequences, 158 falls and, 162-163
Immune system, 9 Incontinence, 41-47,164-167
algorithm for management, 42- 44 bladder physiology, 41-42 catheterization for, 43 - 44 causes of, 43 clinical classification of, 42 clinical exercises, 46-47 fecal, 167 psychological effects of, 41 urinary, 164 -166
Independence ADLs as, 15 deterioration of, 13 loss of, 7-8 as measure of success in elderly,
11,156 Infections, 28, 160 Insomnia, 91, 108,191 Instability. See Falls and instability Instrumental activities of daily
living, 15-16, 102, 156 Intervention, process of, 157 Ipratropium (Atrovent), for
bronchospasm, 92 Itching, controlling, 108
Laxatives, 61, 62
Index 199
Lidocaine (Xylocaine), in pain control, 107
Lithium, for depression, 173 "Long-term care facility relocation
stress," 80 Lorazepam (Ativan), for agitation, 72 Loss
aging and, 10 of independence, 7-8
Loxapine (Loxapac) for agitation, 72, 181 for delirium, 108 initial dosage for elderly, 84
Malignant neoplasm, 29 MAOI. See Monoamine oxidase
inhibitors Medical assessment, 16-17, 156-157 Medications
depression caused by, 56, 85 disability in elderly caused by, 9 in geriatric care, 7 incontinence caused by, 43 in nursing homes, 101 swallowing problems and, 108
Megestranol (Megace), for anorexia, 108
Meperidine (Demerol), for pain control, 106
Methylphenidate (Ritalin) for depression, 59, 174 for hiccups, 108
Metoclopramide (Maxeran,lReglan) for nausea and vomiting, 108 for pain control, 107
Metronidazole (Flagyl), for pain control, 107
Mini Mental Status Exam (MMSE), 14,52,53,155
Misoprostol (Cytotec), for gastric cytoprotection, 93
Monoamine oxidase inhibitors (MAOI), 58, 173
200 Index
Morphine for agitation, 74,181 for pain control, 106
Mouth dry, 191 Multiple pathology, of elderly, 7 Musculoskeletal pain, 93, 187 Myocardial infarct, 28 -29
Nausea, 191 Neuroleptics
for depression, 172 for sleeplessness, 91
Neuropsychological testing, 155 Nifedipine (Adalat), for
hypertension, 94 Nonsteroidal Anti-inflammatory
drugs (NSAIDS), 93, 107, 187 Nortriptyline (Aventyl)
for depression, 58, 173 initial dosage for elderly, 84
NSAIDS. See nonsteroidal anti-inflammatory drugs
Nursing home care, 99-103,188-189 additional community resources,
102,189 care plan, 102 clinical exercise, 102-103 documentation, 100 general wisdom, 188 level of care, 99, 188 medication, 101 periodic review of care, 101 physician availability, 100-101 restraining patients, 35 - 36 standards of medical care, 188
Nystatin (Mycostatin), for ulcer pain control, 107
"Old folks' homes," 2 Omiprazole (Losee), for dyspepsia,
92-93 Orientation, 3, 155 Orthostatic hypotension, 27 Overflow incontinence, 42 Overpresentation,l60-161 Oxycodone (percodan), for pain
control, 106
Pain, 21 control of, 106-107, 190-191 psychological worsening of, 107
Parkinson's disease, 17, 73 Pathogenesis of personality
disorders, theory of, 10 Patient
medical history of, 156 physical assessment of, 156 -157
Pediatric assessment, 13 Pentazocine (Talwin), for pain
control, 106 Personality, aging and, 153 Personality disorders, pathogenesis
of, 10 Pfeiffer E., 14 Pharmacies, 189 Physicians
active participation of, 158 demographics of, 2 as philosophers, 111 role of, in nursing home, 3
"PLAID," as mnemonic, 166 "POINTS," mnemonic for pressure
sore management, 66 -67, 178-179
Postvoid residual bladder volume, 43,166
Practical prescribing to elderly, 83-88, 184-185
begin therapy with clear endpoint in mind, 85
clinical exercise, 87 - 88 do one thing at a time, 87 go slow, 84-85 keep it simple, 87 limit orders, 86 organize follow-up, 85 review drug profile at every visit,
86 risk reducing drugs regularly,
85-86 start low, 84 treat only when life, function, or
comfort are threatened, 83-84
Pratt dilators, 166 Prednisone
for anorexia, 108
for pain control, 107 Pressure sores, 65 -68, 177-179
areas at risk, 178 classification (Shea), 177 clinical exercise, 67 etiology, 65 - 67, 177 general wisdom, 177 management, 66 - 68, 178 -179
"PRISM," as mnemonic for agitation, 70,180
Prochlorperazine (Stemetil), for nausea and vomiting, 108
Progressive senile dementia. See Alzheimer's disease
Propoxyphene (Darvon), for pain control, 106
Pruritus, 191 Pulmonary embolism, 27-28, 160
Ranitidine (Zantac), for dyspepsia, 92
Rehabilitation diagnosis, 158 Rehabilitation of elderly patients,
19-23,158-159 clinical exercise, 22-23 general wisdom, 158 immobility trap, 20 rehabilitation process, 21-22,159
Rehabilitation process, 21-22, 159 "Relocation stress," 101
SAAB. See Syndrome of Aggressive Ambulatory Behaviour
Salbutamol, 186-187 Secondary depression, 56, 172 Senile dementia of the Alzheimer's
type. See Alzheimer's disease Sensorium, as term, 49 Serotonin antagonists, for
depression, 58,174 Sexual behaviour, as agitation, 70-71 "SHAFf," as mnemonic, 156 Short Portable Mental Status
Questionnaire (SPMSQ), 14, 52,53
Simethicone (Ovol) for hiccups, 108
Index 201
for pain control, 107 Skin failure, 65. See also Pressure
sores Sleep disorders, 91-92,186 Steroids, 187 Stress incontinence
definition of, 42 management of, 44
Suppositories, 108 for constipation, 62
Swallowing problems, 108 "Sway," in elderly, 35 "Sway diagram," 162 Syndrome of Aggressive Ambulatory
Behavior (SAAB), 71, 180
Temazepam (Restoril), for sleep disorders, 91,186
Tenesmus, 191 TENS, in musculoskeletal pain, 93 Terfenadine (Seldane), for itching,
108 Terminal or palliative care, 105 -109,
190-191 clinical exercise, 109 control of other symptoms, 108 -109 general wisdom, 190 other symptoms, 191 pain control, 106-107, 190-191 total pain, 107
T4 screening, 26 -27 Theophylline (Theo-Dur), 92 Theory of drug therapy and aging,
182-183 Thiazide diuretics
for congestive heart failure, 90 for hypertension, 94
Thioridazine (Mellaril), for agitation, 72,181
Thiothixine (Navane), 73 Thoracentesis, 108 Thyroid disease, 26-27, 160 Timolol (Blocarden), for agitation, 74 Transient incontinence, 42 Transient ischemic attack (TIA), 51 Trazadone, 173 Triazolam (Halcion), for insomnia,
108,186
202 Index
Tricyclic antidepressants for agitation, 181 for depression, 58, 173 for pain control, 107 for sleeplessness, 91
Tryptophan, for sleep disorders, 91
Underpresentation,l60 Urge incontinence, 42 Urinary incontinence, 164 -166
algorithm. for management, 165, 166
clinical classification, 164 general wisdom, 164 poor man's bladder physiology, 164
Valproic acid (Depakene) for hiccups, 108 for pain control, 107
Vomiting, 191



























