Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=iija20
International Journal of Audiology
ISSN: 1499-2027 (Print) 1708-8186 (Online) Journal homepage: https://www.tandfonline.com/loi/iija20
Beyond motivation: identifying targets forintervention to increase hearing aid use in adults
Chelsea S. Sawyer, Kevin J. Munro, Piers Dawes, Martin P. O'Driscoll &Christopher J. Armitage
To cite this article: Chelsea S. Sawyer, Kevin J. Munro, Piers Dawes, Martin P. O'Driscoll& Christopher J. Armitage (2019) Beyond motivation: identifying targets for intervention toincrease hearing aid use in adults, International Journal of Audiology, 58:1, 53-58, DOI:10.1080/14992027.2018.1534007
To link to this article: https://doi.org/10.1080/14992027.2018.1534007
© 2019 The Authors. Published byInforma UK Limited, trading as Taylor &Francis Group on behalf of British Societyof Audiology, International Society ofAudiology, and Nordic Audiological Society.
Published online: 28 Jan 2019.
Submit your article to this journal
Article views: 412
View related articles
View Crossmark data

ORIGINAL ARTICLE
Beyond motivation: identifying targets for intervention to increase hearing aiduse in adults
Chelsea S. Sawyera, Kevin J. Munroa,b , Piers Dawesa,b , Martin P. O’Driscolla,b andChristopher J. Armitageb,c
aManchester Centre for Audiology and Deafness, School of Health Sciences, Faculty of Biology, Medicine and Health, University of Manchester,UK; bNIHR Manchester Biomedical Research Centre, Manchester University Hospital NHS Foundation Trust, Manchester Academic HealthScience Centre, Manchester, UK; cManchester Centre for Health Psychology, Division of Psychology and Mental Health, School of HealthSciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester Academic Health Science Centre, UK
ABSTRACTObjective: The present study investigated: (a) how motivated patients are to use their hearing aid, and(b) whether post-motivational variables (e.g. action planning, coping planning) have anything to offer interms of developing interventions to boost hearing aid use.Design: participants completed a questionnaire designed to tap Health Action Process Approach con-structs prior to their hearing aid prescription and fitting. Study sample: Sixty-seven patients attendingNHS audiology clinics.Results: Participants reported very strong intentions to use hearing aids (Median¼ 7.00 Q1 and Q3¼ 6.67,7.00, on a þ1 to þ7 scale) and high self-efficacy (Median¼ 7.00, Q1 and Q3¼ 6.00, on a þ1 to þ7 scale)leaving little room for improvement. In contrast, participants reported moderate levels of post-motivationalvariables (action planning Median¼ 4.25, Q1 and Q3¼ 1.13, 7.00 and coping planning Median¼ 2.75, Q1and Q3¼ 1.00, both measured on þ1 to þ7 scales) thereby showing significant scope for change.Conclusions: Future interventions to increase hearing aid use should focus on ensuring that patients’motivation is translated into action, rather than further trying to boost motivation.
ARTICLE HISTORYReceived 25 January 2018Revised 3 September 2018Accepted 5 September 2018
KEYWORDSHearing aids; health actionprocess approach; hearingaid use; behaviour change
Introduction
The number of UK adults with hearing impairment is pre-dicted to rise from 10 million in 2011 to 14.5 million by 2031(Action on Hearing loss 2011a). Hearing impairment is associ-ated with negative outcomes including poor quality of life(Chia et al. 2007; RNID 2004); low self-rated health (Mulrowet al. 1990); cognitive decline (Lin et al. 2013); and feelings ofdepression, anxiety, frustration, loneliness and fatigue(Gopinath et al. 2009; Gopinath et al. 2012). Hearing impair-ment was ranked fifth for global disease burden in 2013 (Voset al. 2015).
The principal treatment for permanent hearing loss is hearingaids, but rates of non-use vary from 5% to 40% (Ferguson et al.2017). Research attention has been drawn to developing inter-ventions that will address sub-optimal use of hearing aids.However, Barker, Mackenzie, Elliott, Jones, and de Lusignan’ssystematic review showed that interventions designed to boosthearing aid use had limited success. Studies included in theirreview suffered poor methodological quality, with the majorityhaving potential biases in performance (participants were notblinded), detection (outcomes were not blinded) and/or selection(no details about randomisation). Moreover, all 31 of the inter-ventions that were targeted at the individual were designed toenhance motivation only for example, by providing informationabout the psychosocial impacts of hearing loss, the benefits of
using hearing aids, or demonstrating how to use a hearing aid,to boost intention and self-efficacy (Barker et al. 2014).
Theories of motivation, such as self-determination theory(Deci and Ryan 1985), the health belief model (Becker 1974) andtheory of planned behaviour (Ajzen 1991) have been applied tohearing aid use (Meister et al. 2014; Ridgway et al. 2015;Saunders et al. 2013). According to these theories, increases inmotivation (or “behavioural intention”) are sufficient to bringabout change behaviour (Armitage and Conner 2000), but theo-ries of motivation have been criticised due to the weak correl-ation between motivation and subsequent behaviour (Armitageand Conner 2001).
Stage models such as the Transtheoretical Model (TTM;Prochaska and Diclemente 1983) try to identify groups of peoplewho may be motivated to engage in a particular behaviour andconsiders people who are motivated but have not yet changedtheir behaviour. Stage models have been applied to hearing aiduptake (Laplante-L�evesque et al. 2013), but have been criticisedfor making arbitrary distinctions between the five different stagesof change and for a lack of information about how people maketransitions between stages (e.g. Armitage 2009; Sutton 2005).
However, the focus on motivation to promote hearing aid usemay have been misguided. The evidence increasingly shows thatpeople who have been prescribed a hearing aid are close to themaximum on measures of motivation, including behaviouralintention (Armitage et al. 2017; Meister, Grugel, and Meis 2014),
CONTACT Christopher J. Armitage [email protected] Manchester Centre for Health Psychology, Division of Psychology and Mental Health,Faculty of Biology, Medicine and Health, School of Health Sciences, University of Manchester, Manchester Academic Health Science Centre, Manchester, UK� 2019 The Authors. Published by Informa UK Limited, trading as Taylor & Francis Group on behalf of British Society of Audiology, International Society of Audiology, and NordicAudiological Society.This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License (http://creativecommons.org/licenses/by-nc-nd/4.0/), whichpermits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon in any way.
INTERNATIONAL JOURNAL OF AUDIOLOGY2019, VOL. 58, NO. 1, 53–58https://doi.org/10.1080/14992027.2018.1534007

self-efficacy (Armitage et al. 2017) and positive outcome expect-ancies (Meister et al. 2008), with respect to using a hearing aid.
One model that provides an alternative to an approachfocussed on motivation is the Health Action Process Approach(HAPA, Schwarzer 2008). The HAPA model provides a theoret-ical framework for the adoption and maintenance of behaviours(Schwarzer 2008). The HAPA model posits two phases. The firstphase is the motivational phase where the individual forms anintention to change their behaviour and is characterised by varia-bles such as behavioural intention and self-efficacy. The secondphase is the volitional phase, which is characterised by variablessuch as action planning (planning when to perform the behav-iour) and coping planning (planning how to deal with barriers).
The principal tenets of the HAPA, and in particular the dis-tinction between motivation and volition, have been supportedacross a variety of health behaviours, including physical activity(Perrier et al. 2012; Hattar, Pal, and Hagger 2016), healthy eating(Radtke et al. 2014), smoking cessation (Radtke et al. 2012), alco-hol consumption (Murgraff et al. 2003) and in chronic illnessand disability (Schwarzer et al. 2011). To date, however, theHAPA model has not been applied in the domain of hearinghealth care. For the first time, the present study used compo-nents of the HAPA model to inform future intervention develop-ment. It was hypothesised that adult hearing aid patients wouldbe highly motivated to wear hearing aids, but would report adeficit in volitional variables that have shown to be important intranslating that motivation into action.
Method
Participants
Sixty-seven participants were recruited from three NHS audi-ology clinics in England. Patients who met the inclusion criteria(>18 years of age, reporting hearing difficulties and audiometri-cally eligible for a hearing aid) were able to take part and nofinancial incentive to participate was offered. Written consentwas obtained from participants by the research team prior toparticipation. Ethical approval was gained from the London –City and East Research Ethics Committee (reference number 15/LO/0367) and local NHS Trust approval.
Participants’ ages ranged from 32 to 90 years old with amedian of 72 years old (Q1¼ 61.3, Q3¼ 78.0 years old). Thirty-six (53.7%) were male and fifty-four (91.5%) were white British.The duration for which participants had experienced hearing dif-ficulties ranged from 3months to 60 years with a median of8.5 years (Q1¼ 2 years, Q3¼ 12 years).Twenty-five (37.9%) par-ticipants had regularly worn a hearing aid in the past but hadstopped using it and forty-one (62.1%) had never owned or regu-larly worn a hearing aid before.
Study design
The study had a cross-sectional design. Data were obtainedthrough a questionnaire administered before participants’ hearingaids were prescribed and fitted. The questionnaire was completedin the clinic immediately after the initial assessment or later athome (to be returned by post).
Measures
The questionnaire operationalised the two phases from theHAPA model. The motivational phase was operationalised
through questionnaire items of behavioural intention and actionself-efficacy; the volitional phase was operationalised throughquestionnaire items of action planning and coping planning. Allfourteen items were answered on seven-point (þ1 to þ7) Likert-scales and were adapted for hearing aid use from the originalscales (Armitage et al. 2017; Sniehotta et al. 2005).
The questionnaire items of behavioural intention was adaptedfrom Armitage et al. (2017) using participants’ responses to threeitems: “I intend to wear a hearing aid as advised definitely donot-definitely do”, “I want to wear a hearing aid as advised def-initely do not-definitely do” and “How likely is it that you willwear a hearing aid as advised? not likely-very likely”.
Action self-efficacy was adapted from Armitage et al. (2017)and was assessed using responses to three items: “My wearing ahearing aid as advised would be difficult-easy”, “I believe I havethe ability to wear a hearing aid as advised definitely do not-def-initely do” and “How confident are you that you will be able towear a hearing aid as advised? not at all-very much so”.
The measure of action planning was adapted from Sniehottaet al. (2005). The four items were answered on 7-point scalesranging from strongly disagree to strongly agree. The item stem“I have made a plan regarding…” was followed by “…when towear my hearing aid”, “…where to wear my hearing aid”,“… how often to wear my hearing aid,” and “… in which situa-tions to wear my hearing aid.”
Coping planning was similarly adapted from Sniehotta et al.(2005). Participants responded to the four items on 7-pointscales ranging from strongly disagree to strongly agree. The itemstem “I have made a plan…” was followed by “… regardingwhat to do if something interferes with my plans to wear myhearing aid”, “… regarding how to cope with possible setbacksto wearing my hearing aid”, “… regarding how to wear my hear-ing aid in difficult situations” and “… to prevent lapses in wear-ing my hearing aid”.
Hearing sensitivity (i.e. pure tone hearing threshold level) wasobtained from the medical records and was the mean of 500,1000, 2000, and 4000Hz for the better ear.
Procedure
Patients who had been referred for a hearing assessment by theirgeneral practitioner were invited to take part in the study via aletter and an information sheet posted to them prior to theirhearing assessment appointment. Audiologists screened patientsfor their eligibility to be included in the study during their hear-ing assessment appointment. If patients were eligible the audiolo-gist introduced the patient to the researcher. Once patients hadconsented they completed the questionnaire alone. Patients com-pleted the questionnaire between May 2015 and September 2015.Recruitment rates and reasons for refusal and withdrawalwere recorded.
Data analysis
Descriptive statistics on participant characteristics, mean,Standard Deviations (SDs), median and interquartile range werecomputed. The data were ordinal and skewed and so a Friedmantest was used to compare scores on all the variables. WilcoxonSigned-Rank Tests were used to compare each motivational vari-able with each volitional variable. The effect sizes (r) for differen-ces between the motivational and volitional phases werecomputed. Zou’s (2007) procedures were used to assess whetherthe differences in effect sizes were statistically significant.
54 C. S. SAWYER ET AL.

Results
Recruitment and retention
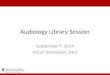
Recruitment and follow-up rates were lower than expected.Figure 1 presents a diagram of the study flow. Of the 253 peoplewho were screened and invited to take part in the study, 204participants were assessed for eligibility. Forty-nine participantswere not assessed for eligibility was due to the participants can-celling, rescheduling or not attending their appointment. Ofthose eligible to take part in the study, 57 were excluded as theydid not meet the audiometric criteria to be eligible for a hearingaid, 33 declined to participate (45.5% due to lack of interest,15.2% due to lack of time, and 21.2% due to ill health). Sixty-seven (53.6%) of 125 eligible participants who consented to takepart in the study completed and returned the questionnaire.
Reliability of measures
The Cronbach’s a for the three intention items in this studyindicated good internal reliability (a¼ 0.77). Cronbach’s a for
the three action self-efficacy items in this study was low(a¼ 0.50). Removal of the item: “My wearing a hearing aid asadvised would be difficult-easy”, increased the internal reliabilityto a¼ 0.77, and so this item was removed from subsequent dataanalysis. The Cronbach’s a for the three action planning items inthis study indicated that internal consistency of the action plan-ning scale was high (a¼ 0.95). The Cronbach’s a for the threecoping planning items in this study indicated that the internalconsistency of the coping planning scale was high (a¼ 0.96).
Participant characteristics
Table 1 summarises the characteristics of participants who wereincluded in the study. The mean hearing sensitivity for the betterear was 48 dB HL (SD¼ 19 dB). 54.6% and 30.3% had a mildloss (26–40 dB HL in the better ear) and moderate hearing loss(41–55 dB HL in the better ear), respectively. 12.1% had a mod-erately severe loss (56–70 dB HL in the better ear) and 3% had asevere loss (71–90 dB HL in the better ear).
Figure 1. Flow diagram of patients through the study.
INTERNATIONAL JOURNAL OF AUDIOLOGY 55

Motivational and volitional constructs
Participants reported being very highly motivated to use theirhearing aids, with 71.9% and 40.0% of people scoring at themaximums of the intention and self-efficacy scales, respectively(Medianintention¼ 7.00 Q1 and Q3¼ 6.67, 7.00; Medianaction self-
efficacy¼ 7.00, Q1 and Q3¼ 6.00, 7.00) and the median scoreswere at the maximums of the scales. In contrast, mean scores forvolitional variables were lower (Medianaction planning¼ 4.25, Q1and Q3¼ 1.13, 7.00; Mediancoping planning¼ 2.75, Q1 andQ3¼ 1.00, 5.56), with just 27.7% and 16.7% of participants scor-ing the maximum possible values for action planning and copingplanning, respectively. Thus, consistent with predictions, partic-ipants’ motivation was higher than their volition.
A Friedman test was conducted, to compare scores on all thevariables. This analysis revealed significant differences between thescores on all variables F (3, 58)¼ 40.47, p< 0.001. Both the vol-itional constructs (action and coping planning) scored significantlylower than the motivational constructs (intention and action self-efficacy). The Wilcoxon Signed-Rank Tests showed that actionplanning (volitional phase) scores were significantly lower thaneither intention (motivation phase), Z¼ �5.87, p< 0.001, or actionself-efficacy (motivation phase), Z¼�5.61, p< 0.001. Coping plan-ning scores (volitional phase) were significantly lower than eitherintention (motivation phase), Z¼�6.38, p< 0.001, or action self-efficacy (motivation phase), Z¼�6.34, p< 0.001 (see Table 2).
The effect size for the differences between intention and self-efficacy (motivational phase) were small to medium (r¼ 0.20) aswere the differences between action planning and coping planning(volitional phase; r¼ 0.27). In contrast, the differences betweenmotivation and volitional variables were large (rs> 0.50). Zou’s(2007) procedures were used to assess whether these differences ineffect sizes were statistically significant (Table 2). These analysesrevealed that the differences between the motivational andvolitional phases were significantly stronger (ps< 0.05) than thedifferences between variables within the phases.
Discussion
This is the first study to have applied the HAPA in the domainof hearing health care. The principal findings are: (a) adultpatients attending an NHS audiology clinic were highly moti-vated in terms of the HAPA model (intention and action self-
efficacy) to use a hearing aid, and (b) there is evidence for a dis-tinction between the motivational and volitional phases. The fol-lowing discussion focuses on the implications of the findings fortheory and practice.
Distinction between the motivational and volitional phase
Participants reported being highly motivated and confident theycould use a hearing aid as advised, consistent with Armitageet al. (2017). This high level of motivation in participants wasexpected because, by definition, the participants had bothacknowledged the possibility of a hearing loss and attended thehearing assessment appointment (Armitage et al. 2017). Thehigh level of motivation in adult participants attending an audi-ology clinic may go some way towards explaining why previousinterventions reviewed by Barker et al. (2014), which largelyfocussed on boosting motivation, were ineffective. In contrast,participants were relatively low in volition and did not reportmaking plans to use their hearing aid or to overcome potentialbarriers to using their hearing aids. For the first time, this pro-vides evidence for a distinction between the motivational andvolitional phases in relation to hearing aid use. Lower scores onthe volitional variables compared to motivational variables areunlikely to be due to lack of knowledge of using a hearing aidin difficult situations, as possible setbacks and potentially diffi-cult situations are highlighted during routine consultations.Thus, interventions may need to focus on increasing patients’use of volitional processes to help translate high motivation intobehaviour. One possible approach would be to encourage peopleto form implementation intentions (“if-then plans”), which areknown to help people translate motivation into action (seeGollwitzer 1999) in a range of behaviours from reducing suicidalideation and behaviour (Armitage et al. 2016) to increasingphysical activity (e.g. Epton and Armitage 2017), but not yet inrelation to hearing aid use.
Limitations
The major limitation associated with the present study was thatrecruitment proved challenging, with many potential partici-pants reporting that a lack of interest in the research was theirmain reason for declining. Future studies would need to addressthis issue and one approach would be to spend more time withpatients to improve recruitment materials, such as patient infor-mation sheets and advertising. Moreover, it is notable that wedid not offer incentives for participation, which would likelyhave boosted the recruitment rate (McDonald et al. 2006).Nevertheless, it is valuable to know likely recruitment rates forfuture research with this population, and potential strategies forovercoming the barriers. The study looked at the motivationaland volitional variables pre-fitting future studies should investi-gate the longer-term trajectories of motivation and volition
Table 2. The Wilcoxon Signed-Rank Tests for the motivational and volitional constructs.
Action planning Coping planning Intention Action self-efficacy
Action planning Median¼ 1.13 Q1¼ 4.25, Q3¼ 7.00 z¼ 3.17� r¼ 0.39a z¼ 5.87�� r¼ 0.72b z¼ 5.61�� r¼ 0.69bCoping planning – Median¼ 1.00 Q1¼ 2.75, Q3¼ 5.56 z¼ 6.38�� r¼ 0.78b z¼ 6.33�� r¼ 0.77bIntention – – Median¼ 6.67 Q1¼ 6, Q3¼ 6 z¼ 2.24� r¼ 0.27aAction self-efficacy – – – Median¼ 6.00 Q1¼ 6, Q3¼ 6
Note. Descriptive statistics are presented along the diagonal. Where effect sizes (r) have different subscripts they differ significantly (ps< .05) from one anotheraccording to Zou’s (2007) test.�p<.01.��p<.001.
Table 1. Characteristics of participants (Means and Standard Deviations) andmedians and interquartile ranges of the HAPA component.
N Mean, Standard Deviations (SDs)/Q1, Median, Q3
PTA better ear 66 47.98 (SD 18.91)Intention 64 6.67, 7.00, 7.00Action Self-Efficacy 65 6.00, 7.00, 7.00Action Planning 65 1.13, 4.25, 7.00Coping Planning 66 1.00, 2.75, 5.56
56 C. S. SAWYER ET AL.

post-hearing aid fitting. Another limitation is potential biasesfrom individuals who declined due to lack of interest, these indi-viduals may also have been less motivated to use hearing aid andmay have scored lower on the motivational variables compared tothe people who participated in the present study. These individu-als who declined due to lack of interest may be the ones whorequire further intervention to promote sustained hearing aid use.Further research is required to determine whether interventionsfor these groups of disinterested participants should target motiv-ation or volition. However, it is worth noting that these disinter-ested participants were sufficiently motivated, whether intrinsicallyor extrinsically by significant others, to seek help for their hearingand attend a hearing assessment appointment, we would expectissues in hearing aid use to also be related to volition.
The construct validity for the questionnaire items for the con-structs from the health action process approach model was notassessed prior to the study; therefore, it is possible the items mayhave low construct validity and may not have measured the con-structs adequately. However previous studies have demonstratedempirical evidence for the validity of the items measuring thehealth action process approach for a variety of different healthbehaviours in diverse settings (Schwarzer 2008).
Conclusions
This is the first study to have applied the HAPA model to thedomain of hearing healthcare. Participants attending a hearingassessment were already highly motivated to use a hearing aid butlow on volition. There seems to be little scope for boosting motiv-ation further but plenty of scope for changing the volitional varia-bles. Further research is needed to specify the role of volitionalvariables measured pre and post-hearing aid fitting in predictinghearing aid use and using behaviour change techniques to buildinterventions around volitional variables to boost hearing aid use.
Acknowledgements
The author would like to thank the audiology team at CentralManchester University Hospitals NHS Foundation Trust for theirhelp in recruiting participants.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
This research was funded by Central Manchester UniversityHospitals NHS Foundation Trust, Trust Charitable Funds (CentralManchester University Hospitals NHS Foundation Trust Charity),and supported by the NIHR Manchester Biomedical ResearchCentre, the NIHR Greater Manchester Patient Safety TranslationalResearch Centre, and the NIHR Greater Manchester: ClinicalResearch Network.
ORCID
Kevin J. Munro https://orcid.org/0000-0001-6543-9098Piers Dawes http://orcid.org/0000-0003-3180-9884Christopher J. Armitage https://orcid.org/0000-0003-2365-1765
References
Action on Hearing Loss 2011a. Facts and Figures on Hearing Loss andTinnitus. http://www.actiononhearingloss.org.uk/hearing-health/hearing-loss-and-deafness/ Accessed November 1, 2018.
Ajzen, I. 1991. The theory of planned behavior. Organizational Behavior andHuman Decision Processes 50:179–211. doi:https://doi.org/10.1016/0749-5978(91)90020-T
Armitage, C. J. 2009. “Is There Utility in the Transtheoretical Model?” BritishJournal of Health Psychology 14 (Pt 2):195–210. doi:10.1348/135910708X368991
Armitage, C. J., and M. Conner. 2000. “Social Cognition Models and HealthBehaviour: A Structured Review.” Psychology and Health 15 (2):173–189.doi:10.1080/08870440008400299
Armitage, C. J., and M. Conner. 2001. “Efficacy of the Theory of PlannedBehaviour: A Meta-Analytic Review.” British Journal of Social Psychology40 (4):471–499. doi:10.1348/014466601164939
Armitage, C. J., D. Lees, K. Lewis, and K. J. Munro. 2017. “PreliminarySupport for a Brief Psychological Intervention to Improve First-TimeHearing Aid Use among Adults.” British Journal of Health Psychology 22(4):976–983. doi:10.1111/bjhp.12244
Armitage, C. J., W. A. Rahim, R. Rowe, and R. C. O’Connor. 2016. “AnExploratory Randomised Trial of a Simple, Brief PsychologicalIntervention to Reduce Subsequent Suicidal Ideation and Behaviour inPatients Admitted to Hospital for Self-Harm.” British Journal of Psychiatry208 (05):470–476. doi:10.1192/bjp.bp.114.162495
Barker, F., E. Mackenzie, L. Elliott, S. Jones, and S. de lusignan. 2014.“Interventions to Improve Hearing Aid Use in Adult AuditoryRehabilitation.” The Cochrane Library doi:10.1002/14651858.CD010342
Becker, M. H. 1974. The Health Belief Model and Personal Health Behavior.:Slack, University of Michigan, USA.
Chia, E. M., J. J. Wang, E. Rochtchina, R. R. Cumming, P. Newall, and P.Mitchell. 2007. “Hearing Impairment and Health-Related Quality of Life:The Blue Mountains Hearing Study.” Ear and Hearing 28 (2):187–195.doi:10.1097/AUD.0b013e31803126b6
Deci, E., and R. M. Ryan. 1985. Intrinsic motivation and self-determination inhuman behavior. Springer Science and Business Media, New York, USA.doi:10.1007/978-1-4899-2271-7
Epton, T., and C. J. Armitage. 2017. “Does Situation-Specificity Affect theOperation of Implementation Intentions?” Behavior Therapy 48 (6):860–869. doi:10.1016/j.beth.2017.08.003
Ferguson, M., P. Kitterick, L. Chong, M. Edmondson-Jones, F. Barker, andD. Hoare. 2017. “Hearing Aids for Mild to Moderate Hearing Loss inAdults.” The Cochrane Database of Systematic Reviews 9:CD012023.
Gollwitzer, P. M. 1999. “Implementation intentions - Strong Effects ofSimple Plans.” American Psychologist 54 (7):493–503. doi:10.1037//0003-066X.54.7.493
Gopinath, B., J. Schneider, C. M. McMahon, E. Teber, S. R. Leeder, and P.Mitchell. 2012. “Severity of Age-Related Hearing Loss Is Associated withImpaired Activities of Daily Living.” Age and Ageing 41 (2):195–200. doi:10.1093/ageing/afr155
Gopinath, B., J. J. Wang, J. Schneider, G. Burlutsky, J. Snowdon, C. M.McMahon, S. R. Leeder, and P. Mitchell. 2009. “Depressive Symptoms inOlder Adults with Hearing Impairments: The Blue Mountains Study.”Journal of the American Geriatrics Society 57 (7):1306–1308. doi:10.1111/j.1532-5415.2009.02317.x
Hattar, A., S. Pal, and M. S. Hagger. 2016. “Predicting Physical Activity-Related Outcomes in Overweight and Obese Adults: A Health ActionProcess Approach.” Applied Psychology: Health and Well-Being 8 (1):127–151. doi:10.1111/aphw.12065
Laplante-L�evesque, A., K. J. Br€annstr€om, E. Ingo, G. Andersson, and T.Lunner. 2015. “Stages of Change in Adults Who Have Failed an OnlineHearing Screening.” Ear and Hearing 36 (1):92–101. doi:10.1097/AUD.0000000000000085.
Laplante-L�evesque, A., L. Hickson, and L. Worrall. 2013. “Stages of Changein Adults with Acquired Hearing Impairment Seeking Help for the FirstTime: application of the Transtheoretical Model in AudiologicRehabilitation.” Ear and Hearing 34 (4):447–457. doi:10.1097/AUD.0b013e3182772c49.
Lin, F. R., K. Yaffe, J. Xia, Q.-L. Xue, T. B. Harris, E. Purchase-Helzner, S.Satterfield., et al. 2013. “Hearing Loss and Cognitive Decline in OlderAdults.” JAMA Internal Medicine 173 (4):293–299. doi:10.1001/jamainternmed.2013.1868
McDonald, A. M., R. C. Knight, M. K. Campbell, V. A. Entwistle, A. M.Grant, J. A. Cook, Elbourne D. R., et al. 2006. “What Influences
INTERNATIONAL JOURNAL OF AUDIOLOGY 57

Recruitment to Randomised Controlled Trials? A Review of Trials Fundedby Two UK Funding Agencies.” Trials 7 (1):1. doi:10.1186/1745-6215-7-9
Meister, H., L. Grugel, and M. Meis. 2014. “Intention to Use Hearing Aids:A Survey Based on the Theory of Planned Behavior.” Patient Preferenceand Adherence 8:1265. doi:10.2147/PPA.S65008
Meister, H., M. Walger, D. Brehmer, U.-C. von Wedel, and H. von Wedel.2008. “The Relationship between Pre-Fitting Expectations and Willingnessto Use Hearing Aids.” International Journal of Audiology 47 (4):153–159.doi:10.1080/14992020701843111
Mulrow, C. D., C. Aguilar, J. E. Endicott, M. R. Tuley, R. Velez, W. S.Charlip, M. C. Rhodes, J. A. Hill, L. A. DeNino. 1990. “Quality-of-LifeChanges and Hearing Impairment: A Randomized Trial.” Annals ofInternal Medicine 113 (3):188–194. doi:10.7326/0003-4819-113-3-188
Murgraff, V., M. R. McDermott, and J. Walsh. 2003. “Self-Efficacy andBehavioral Enactment: The Application of Schwarzer’s Health ActionProcess Approach to the Prediction of Low-Risk, Single-OccasionDrinking.” Journal of Applied Social Psychology 33 (2):339–361. doi:10.1111/j.1559-1816.2003.tb01900.x
Perrier, M. J., S. N. Sweet, S. M. Strachan, and A. E. Latimer-Cheung. 2012.“I Act, Therefore I Am: Athletic Identity and the Health Action ProcessApproach Predict Sport Participation among Individuals with AcquiredPhysical Disabilities.” Psychology of Sport and Exercise 13 (6):713–720. doi:10.1016/j.psychsport.2012.04.011
Prochaska, J., and C. Diclemente. 1983. “Stages and Processes of Self-Changeof Smoking: Towards the Integrative Model of Change.” Journal ofConsulting and Clinical Psychology 51 (3):390–395. doi:10.1037/0022-006X.51.3.390
Radtke, T., D. Kaklamanou, U. Scholz, R. Hornung, and C. J. Armitage.2014. “Are Diet-Specific Compensatory Health Beliefs Predictive ofDieting Intentions and Behaviour?.” Appetite 76:36–43. doi:10.1016/j.appet.2014.01.014
Radtke, T., U. Scholz, R. Keller, and R. Hornung. 2012. “Smoking Is Ok asLong as I Eat Healthily: Compensatory Health Beliefs and Their Role forIntentions and Smoking within the Health Action Process Approach.”Psychology and Health 27 (sup2):91–107. doi:10.1080/08870446.2011.603422.
Ridgway, J., L. Hickson, and C. Lind. 2015. “Autonomous Motivation IsAssociated with Hearing Aid Adoption.” International Journal ofAudiology 54 (7):476–484. doi:10.3109/14992027.2015.1007213
RNID 2004. A Simple Cure. https://www.scie-socialcareonline.org.uk/a-sim-ple-cure-a-national-report-into-deaf-and-hard-of-hearing-peoples-experien-ces-of-the-national-health-service/r/a11G00000017vcpIAA. AccesedNovember 1, 2018.
Saunders, G. H., M. T. Frederick, S. Silverman, and M. Papesh. 2013.“Application of the Health Belief Model: Development of the HearingBeliefs Questionnaire (HBQ) and Its Associations with Hearing HealthBehaviors.” International Journal of Audiology 52 (8):558–567. doi:10.3109/14992027.2013.791030.
Schwarzer, R. 2008. “Modeling Health Behavior Change: How to Predict andModify the Adoption and Maintenance of Health Behaviors.” AppliedPsychology 57 (1):1–29. doi:10.1111/j.1464-0597.2007.00325.x
Schwarzer, R., S. Lippke, and A. Luszczynska. 2011. “Mechanisms of HealthBehavior Change in Persons with Chronic Illness or Disability: TheHealth Action Process Approach (HAPA).” Rehabilitation Psychology56 (3):161. doi:10.1037/a0024509
Sniehotta, F. F., R. Schwarzer, U. Scholz, and B. Sch€uz. 2005. “ActionPlanning and Coping Planning for Long-Term Lifestyle Change: theoryand Assessment.” European Journal of Social Psychology 35 (4):565–576.doi:10.1002/ejsp.258
Sutton, S. 2005. “Stage Theories of Health Behaviour.” Predicting HealthBehaviour: Research and Practice with Social Cognition Models 2:223–275.
Vos, T., R. M. Barber, B. Bell, A. Bertozzi-Villa, S. Biryukov, I. Bolliger, F.Charlson., et al. 2015. “Global, Regional, and National Incidence,Prevalence, and Years Lived with Disability for 301 Acute and ChronicDiseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysisfor the Global Burden of Disease Study 2013.” The Lancet 386 (9995):743–800. doi:10.1016/S0140-6736(15)60692-4.
Zou, G. Y. 2007. “Toward Using Confidence Intervals to CompareCorrelations.” Psychological Methods 12 (4):399. doi:10.1037/1082-989X.12.4.399
58 C. S. SAWYER ET AL.