Embed Size (px)
Citation preview

Bexar County
Healthcare Summit

Texas Healthcare Financing
Anne Dunkelberg, MPA Associate Director, Health and WellnessCenter for Public Policy Prioritieswww.cppp.org
Bexar County
Healthcare Summit

Title
Bexar County
Healthcare Summit

US Health Spending (CBO, The 2014 Long Term Budget Outlook , July 2014).
Bexar County
Healthcare Summit

Total health expenditure per capita, public and private, 2009
U.S. spends far more per capita on health care than all other developed countries.
Bexar County
Healthcare Summit
Total expenditure excluding investments.Source: OECD Health Data 2011; WHO Global Health Expenditure Database.

Center on Budget and Policy Priorities
cbpp.org6
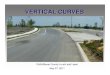
Medicare and Medicaid Controlled Costs Better than Private Insurance Over the Last Decade
Average Annual Growth Rate, 2000-2009
4.6%5.1%
7.2%7.7%
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
Medicaid Per Beneficiary
Medicare Per Beneficiary
Private Per Capita,
Comparableto Medicare
Private EmployerInsurancePremiums
6

Title
Bexar County
Healthcare Summit

CPPP.org
8%9%

Title
Bexar County
Healthcare Summit

forabettertexas.org/investinkids+
Texas Medicaid spending per client is lower than a decade ago
Without DSH and UPL, adjusted for medical inflation
CPPP analysis of THHSC and LBB data

11

CPPP.org
Fast Facts: Texans & Health Insurance (2012)
• 6.4 million uninsured Texans, 24.6% of all ages– Highest rate in the nation
• Children’s coverage is stable at 1.2 million uninsured, 16.4% of all kids (ages 0 – 18).
– Texas now has the 2nd worst uninsured rate for kids after NV.
– More than half of these uninsured children are U.S. citizens who are eligible for Medicaid or CHIP, but are not enrolled.
– Stability protections for CHIP and children’s Medicaid have kept public coverage for kids stable, while private coverage for Texas children continues to decline.
• Texans remain less likely to get job-based health coverage than Americans, on average.
– 49.5% of Texans were insured through their job (or their spouse’s/parents’), compared to 54.9% of the U.S. as a whole.

CPPP.org
TX FLCA
MT
MS NC KY IL CO TN O
H IN MI
ND DEM
E VT0%
5%
10%
15%
20%
25%
Percent Uninsured
Per
cent
Uni
nsur
ed
24% Uninsured
Texas Continues to Top List for Highest Uninsured Rate
5 Most Populous States:
Uninsured Rate by State, 2010 – 2012 avg. Source: CPPP Analysis of U.S. Census Bureau, CPS Annual Social and Economic Supplement, 2011 – 2013.
FLCA
ILNY
TX

CPPP.org
Working-Age Texans Have A Higher Uninsured Rate
Under 19 19 to 64 65 and over0
5000000
10000000
15000000
16% are uninsured1.2 million
32% are uninsured
5.1 million
3% are uninsured
91,000
Uninsured
Medicaid
Medicare
Job-based
Age (Years)
Peo
ple
(Mill
ions
)
Sources of Coverage in Texas by Age, 2012. Analysis excludes additional sources of coverage such as military care and direct purchase; adjusts for major (but not all) sources of dual coverage. Source: CPPP Analysis of U.S. Census Bureau, CPS Annual Social and Economic Supplement, 2013
Texans age 19 – 64 have lower access to public insurance, and are twice as likely to be uninsured as kids.

CPPP.org
Immigrants Not Primary Cause of Texas’ National Uninsured RankingRemove all non-citizens from the data and TX still tops list for highest uninsured rate.
TX LA FLM
SW
Y ID KYOR TN CO M
INE ND NY
ME
MN VT
0%
5%
10%
15%
20%
25%
Percent Uninsured
Pe
rce
nt
Un
insu
red
19.8% Citizen Uninsured Rate
5 Most Populous States:
Citizen Uninsured Rate by State, 2010 – 2012 avg. Source: CPPP Analysis of U.S. Census Bureau, CPS Annual Social and Economic Supplement, 2011 - 2013
TX
FL
CA
ILNY

27%
15%
10%
11%
24% 13%
Cost-Sharing Reductions PLUS Subsidies Subsidies Only
Marketplace Subsidies & Cost-Sharing Reductions
Kids’ Medicaid/CHIP (eligible today but not
enrolled)
Marketplace, No Assistance
Coverage Gap:TX State Policy Decision
Non-Citizens(some may be eligible for
assistance)
ACA: Over 1/3 Texas Uninsured May Get HelpACA Income Eligibility for Uninsured Texans, 2011-2012 avg.
6.4 million uninsured , 24.6% of all ages
Note: Authorized non-citizens may also eligible for financial assistance under a separate set of state and ACA eligibility rules; this analysis does not take into account uninsured families who may have an affordable offer of job-based coverage and who would therefore be ineligible for Marketplace subsidies.Source: CPPP Analysis of U.S. Census Bureau, CPS Annual Social and Economic Supplement, 2011 – 2013
Uninsured Texans (Millions)

Texas Marketplace Eligible
2,049,000Texans eligible for premium subsidies in the Texas Marketplace. (Includes both uninsured and people with individual market coverage today)
3,143,000Potential Marketplace size
Estimates of total eligible,
NOT projections of
who will actually enroll
Kaiser Family Foundation, State-by-State Estimates of the Number of People Eligible for Premium Tax Credits Under the Affordable Care Act, November 5, 2013

Late Surge in Texas EnrollmentMore Texans selected plans in the last 6 weeks than the first 5 months
U.S. Department of Health and Human Services, Health Insurance Marketplace Enrollment Report
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
438,732Mar -Apr
U.S. Texas0%
20%
40%
60%
80%
100%
120%
140%
160%
89%
148%
Total Texas enrollment through mid-April: 733,757
Increase in enrollment in the last 6 weeks of open enrollment
295,025Oct - Feb
18

Texas Marketplace Plan SelectionFrom October 1, 2013 – April 19, 2014
Selected a Marketplace Plan
As % of Marketplace-eligible Population
Texas 734,000 23%
United States 8.02 million 28%
Sources: U.S. Department of Health and Human Services, Health Insurance Marketplace Enrollment Report; and Kaiser Family Foundation, State-by-State Estimates of the Number of People Eligible for Premium Tax Credits Under the Affordable Care Act,, November 5, 2013.
Texas About in the Middle of the Pack When Looking at Eligible Enrolled
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
TexasU.S.
MedianU.S.
Average
Perc
ent o
f Pot
entia
l Mar
ketp
lace
Po
pula
tion
With
Pla
n Se
lecti
on
19

20
Texas Medicaid/CHIP: Who is Helped Today
Medicaid Children, 2,871,447
Maternity 138,060
Poor Parents, 147,013
Elderly, 373,835
Disabled, 426,267
CHIP, 405,654
August 2014, HHSC data
Total enrolled 8/2014:
3.97 million Medicaid;
(44% of Texas kids)
20

Income Caps for Texas Medicaid and CHIP, 2014Shows ACA “MAGI” changes, effective 1/2014
0%
50%
100%
150%
200%
250%
PregnantWomen
Newborns Age 1-5 Age 6-18 Parent of 2 SSI (agedor
disabled)
Long TermCare
CHIP
21
$29,487
$40,174 $40,174
203% 203%149%
$27,310
138%$3,760/yr
19% 76%
$8,892
222%
$25,956 $40,767
206%
• Long Term Care consumers above SSI income limit• Annual Income is for a family of 3, except Individual
Incomes shown for SSI and Long Term Care
Income Limit as Percentage
of Federal Poverty Income

Texas Coverage Gap: Medicaid Hole in the ACA Coverage System
Marketplace with
Subsidies
Marketplace with
Subsidies
Coverage Gap
Coverage Gap
Medicaid
Childless* Adults Working Parents
133% FPL
$25,975 for family of 3
19% FPL
$3,696 for family of 3
100% FPL
$19,530 for family of 3
State With Medicaid Expansion
Texas - Without Medicaid Expansion
Marketplace with Subsidies
Medicaid
Parents and Childless* AdultsFa
mily
Inco
me
$0
vs.
22“Childless” includes parents with grown children.

NOTES: Data are as of August 28, 2014. *AR, IA, MI, and PA have approved Section 1115 waivers for Medicaid expansion. In PA, coverage will begin in January 2015. NH is implementing the Medicaid expansion, but the state plans to seek a waiver at a later date. IN has a pending waiver to implement the Medicaid expansion. WI amended its Medicaid state plan and existing Section 1115 waiver to cover adults up to 100% FPL in Medicaid, but did not adopt the expansion.SOURCES: Current status for each state is based on data from the Centers for Medicare and Medicaid Services, available here, and KCMU analysis of current state activity on Medicaid expansion.
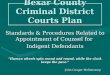
Current Status of State Medicaid Expansion Decisions
WY
WI*
WV
WA
VA
VT
UT
TX
TN
SD
SC
RI PA*
OR
OK
OH
ND
NC
NY
NM
NJ
NH*
NV NE
MT
MO
MS
MN
MI*MA
MD
ME
LA
KY KS
IA*
IN* IL
ID
HI
GA
FL
DC
DE
CT
CO CA
AR*AZ
AK
AL
Implementing the Medicaid Expansion (28 States including DC)Open Debate (2 States)Not Moving Forward at this Time (21 States)

24

SOURCE: Kaiser Family Foundation NOTE: Ten states (CT, IL, ME, MA, MN, NJ, NY, RI, VT, WI) and DC already offer coverage to parents at or above 133% FPL; under the ACA an income disregard of 5 percentage points will be applied to this limit increasing the effective income limit to 138% FPL .SOURCE: Based on the results of a national survey conducted by the Kaiser Commission on Medicaid and the Uninsured and the Georgetown University Center for Children and Families, 2013.
Coverage Gap is Not Just “Childless Adults,” Would significantly Increase Eligibility for Parents in TX, Other States
Medicaid Eligibility Levels for Parents, January 2013:
133%

The Coverage Gap
About 1 million U.S. citizen adults are uninsured in Texas and will have no affordable coverage options.
We have the opportunity at any time to accept federal dollars to expand coverage to low-income adults.
1,000,000

Red State AlternativesConservative States, Republican Governors have Negotiated Coverage
Ex: Arizona, Indiana, Iowa, Michigan, Nevada, New Jersey, New Mexico, North Dakota, Ohio, and Pennsylvania.
Benefits for the newly-covered adults are based on commercial and small business plan standards; – States must screen for “medically frail” persons in the newly-covered adult population, to make sure
they retain access to traditional Medicaid benefits.
– Iowa and PA’s waivers allow the state to experiment for one year with whether/how non-emergency medical transportation is provided to the newly-covered adults.
– IN proposal would give vision and dental care to adults who pay into their HSA-like “POWER account. “
– Reasonable policies ensure ongoing access to community safety net health care providers such as Community Health Centers (FQHCs) and family planning providers.
Personal Responsibility Provisions: Cost-Sharing for the newly-covered adults is allowed. – Waivers experiment with new approaches outside of the basic federal rules, including modest
premiums, and co-pays for non-emergency ER visits, mostly targeted to the new adults who are above the poverty line.
– MI, IA and PA will reduce out-of-pocket costs for enrollees who get check-ups or meet other wellness goals. IN proposal would use an HSA-like structure.
– Affordable cost-sharing (e.g., co-payments and premiums for newly-covered adults), but with protections to ensure coverage remains affordable for family members with serious or chronic health condition.
Bexar County
Healthcare Summit

Red State Alternatives, cont’d.
Financial incentives for wellness behaviors – such as check-ups, immunizations, and participation in chronic condition management programs,
with protections to ensure they are based on medical research and are not harmful to persons who are ill;
Integration with Marketplace – Maximizing the use of private insurers through HMO-style managed care. Like Texas, most states
now have “mature” Medicaid Managed Care sectors with the capacity to serve more adults.
– Arkansas got permission to use Marketplace coverage for all of its adult expansion group, but only because managed care markets were not established for either Medicaid or commercial insurance.
– Some states are seeking a combination of Medicaid Managed Care and Marketplace coverage, e.g., Medicaid Managed Care below poverty, and Marketplace for adults 100-138% of the federal poverty line (FPL).
Flexibility—Within Limits. There is flexibility available to state and federal Medicaid officials, but it is not unlimited. Under federal law, 1115 waivers allowed only to “further purposes of Medicaid.”
Bexar County
Healthcare Summit

Red State AlternativesConservative States, Republican Governors have Negotiated Coverage
Examples: Arizona, Indiana, Iowa, Michigan, Nevada, New Jersey, New Mexico, North Dakota, Ohio, and Pennsylvania
Benefits for the newly-covered adults are based on commercial and small business plan standards;
– States must screen for “medically frail” persons in the newly-covered adult population, to make sure they retain access to traditional Medicaid benefits.
– Iowa and PA’s waivers allow the state to experiment for one year with whether/how non-emergency medical transportation is provided to the newly-covered adults.
– IN proposal would give vision and dental care to adults who pay into their HAS-like POWER account.
– Reasonable policies ensure ongoing access to community safety net health care providers such as Community Health Centers (FQHCs) and family planning providers.
Personal Responsibility Provisions: Cost-Sharing for the newly-covered adults is allowed. – Waivers experiment with new approaches outside of the basic federal rules, including modest
premiums, and co-pays for non-emergency ER visits, mostly targeted to the new adults who are above the poverty line.
– MI, IA and PA will reduce out-of-pocket costs for enrollees who get check-ups or meet other wellness goals. IN proposal would use an HSA-like structure.
– Affordable cost-sharing (e.g., co-payments and premiums for newly-covered adults), but with protections to ensure coverage remains affordable for family members with serious or chronic health condition.

Red State Alternatives, cont’d.Conservative States, Republican Governors have Negotiated Coverage
Financial incentives for wellness behaviors – such as check-ups, immunizations, and participation in chronic condition management
programs, with protections to ensure they are based on medical research and are not harmful to persons who are ill;
Integration with Marketplace – Maximizing the use of private insurers through HMO-style managed care. Like Texas, most
states now have “mature” Medicaid Managed Care sectors with the capacity to serve more adults.
– Arkansas got permission to use Marketplace coverage for all of its adult expansion group, but only because managed care markets were not established for either Medicaid or commercial insurance.
– Some states are seeking a combination of Medicaid Managed Care and Marketplace coverage, e.g., Medicaid Managed Care below poverty, and Marketplace for adults 100-138% of the federal poverty line (FPL).
Flexibility—Within Limits. There is flexibility available to state and federal Medicaid officials, but it is not unlimited. Under federal law, 1115 waivers allowed only to “further purposes of Medicaid.”

31
Dollars, People, Jobs, Taxes: Get the County- and State-level Impact of the Coverage Gap at
www.CPPP.org

Research: Benefits for Taxpayers, HospitalsNon-Expansion states Paying Billions to Support Expansion States
• McClatchy Newspapers analysis of Urban Institute data: • 23 states that have not expanded Medicaid will pay (next eight years) $152 billion to extend
the program in other states. Nearly $88 billion from taxpayers in Texas, Florida, North Carolina, Georgia, and Virginia: 37 percent of the cost to expand Medicaid in the 27 remaining states.
Charity Care and ER visits dropping in Expansion States, Not in non-expansion• New from PWC (PricewaterhouseCoopers): New earnings and patient volume data (538
hospitals in 35 states) “reveal a distinct financial split between healthcare providers in states that have expanded their Medicaid programs and those that have not.”
– Example: Tenet hospitals saw uninsured, charity care admissions decline 46%, and 20.5% increase in Medicaid admissions in expansion states. In the second quarter alone, Tenet saw a $78 million reduction in unpaid care.
• Arkansas Hospital Association: “We expected our emergency rooms to uptick,” she said. “They didn’t.” In a statewide survey of 42 hospitals, the association found a 2% decline in emergency department visits., and about a 30% decline in uninsured patients.
• Colorado Hospital Association: Analysis of data from 30 states (15 with Medicaid expansion, 15 without). Uninsured and Charity care dropped in Medicaid expansion states, but not in non-ME states. AZ hospitals reported 31% drop in uncompensated care in the first 4 months of 2014.
• Oregon's Medicaid population saw a 9 percent reduction in emergency-department visits in the first year of new coordinated care organizations. ER spending dropped 18 percent in Oregon Medicaid from 2011-2013. 32

• Use of This Presentation
The Center for Public Policy Priorities encourages you to reproduce and distribute these slides, which were developed for use in making public presentations. If you reproduce these slides, please give appropriate credit to CPPP.
The data presented here may become outdated. For the most recent information or to sign up for our email updates, visit our website www.cppp.org.
© CPPP
Center for Public Policy Priorities 7020 Easy Wind Drive, Suite 200 Austin, TX 78752 P 512.320.0222 F 512.320.0227
Bexar County
Healthcare Summit