Embed Size (px)
Citation preview

Between- and Within-Religion Differences in Hypertension Risks for Indonesian Women
Natalie Jansen*
University of Kansas
Hypertensive status, or high blood pressure, is an indicator of future cardiovascular disease
(CVD), heart attack, stroke, kidney disease, and premature mortality and disability. Using data
from Wave 5 of the Indonesian Family Life Survey, I explore religious differences in women’s
hypertensive risks. I find that Muslim women experience higher hypertension rates than
Christian and Hindu women. There are no within-religion differences in hypertension rates for
Muslim women when accounting for participation in daily salat prayer or when accounting for
adherence to different traditions. I also find that Hindu women have lower hypertension risks
than Christian and Muslim women, regardless of whether or not they eat beef. Finally, I find that
Hindu women who do yoga and/or meditate daily have the lowest risks of hypertension
compared to Muslims, Christians, and Hindu women who infrequently do yoga/meditate.
* Corresponding author: 1415 Jayhawk Boulevard, Fraser 716, Lawrence, KS, 66045;

Introduction
Hypertensive status, or high blood pressure, is an indicator of future cardiovascular
disease (CVD), heart attack, stroke, kidney disease, and premature mortality and disability (He &
Whelton, 1999; WHO, 2016). Furthermore, hypertension is responsible for at least 45 percent of
deaths as a result of heart disease and 51 percent of deaths caused by stroke globally (WHO,
2013). Past research demonstrates that hypertension and hypertension-related complications are
largely preventable, and making healthy lifestyle adjustments can lower blood pressure (Joffres
et al., 2013).
Concerted public health efforts are being made to alter individual behaviors largely by
striving to lower rates of alcohol consumption and tobacco intake– both previously-demonstrated
risk factors for hypertension (e.g., He & Whelton, 1999; Kayima et al., 2015; Khanam et al.,
2015; Abdul-Razak et al., 2016; Ibrahim, Hijazi, & Al-Bar, 2008). However, in Indonesia – a
low-middle income, Muslim-majority nation – fewer than three percent of women report tobacco
use (DHS, 2012), and fewer than five percent of women report drinking alcohol in the last 12
months (WHO, 2014). Despite the fact that only a small proportion of women in Indonesia
consume alcohol and/or tobacco products, rates of hypertension remain higher than the average
for women in Southeast Asia at 29.3 percent (WHO, 2016).
Low rates of tobacco use are attributed in part to cultural values which stigmatize women
as morally flawed (Barraclough, 1999) along with Islamic fatwas that encourage healthy living,
while low rates of alcohol consumption are attributed both to cultural stigmatization as well as
Islamic doctrine that prohibits alcohol intake. In addition to encouraging healthy living and
discouraging alcohol consumption, religion, and particularly Islam, plays a critical role in

women’s lives in Indonesia; Indonesian citizens must legally identify with a monotheistic
religion, although the overwhelming majority of Indonesians identify as Muslim.
Given the potential role religion has to provide structure to women’s daily lives, offer
social and spiritual support, and encourage healthy behaviors, understanding the role religion
plays on hypertension rates could offer additional insight into disparities in hypertension rates.
Religious involvement as measured by prayer participation, adherence to tradition, and selection
into different faiths, particularly in non-Christian-majority countries, is largely overlooked in
hypertension literature. In this study, I use Wave 5 of the Indonesian Family Life Survey to
examine differing risks in hypertensive status across and within religions.
The Role of Religion on Hypertensive Status
Many studies have found that religious involvement is associated with lower risks of
hypertension. The link between religion and hypertension has been attributed to a variety of
factors including encouragement toward healthy behaviors such as avoiding tobacco, exercising
regularly, and adhering to a particular diet (Koenig, 2012; Powell, Shahabi, & Thoresen, 2003),
strengthening social ties and fostering supportive environments (Krause, 2008; Bradley, 1995;
Holt et al., 2015) and providing a sense of security and self-control (Rounding, Lee, Jacobson, &
Ji, 2012). Koenig (2012) examined 63 studies and found that 36 reported lower blood pressures
for more religious individuals while seven reported significantly higher BP for more religious
individuals. Several studies have also found that religious attendance specifically is associated
with lower blood pressure (Banerjee, Boyle, Anand, Strachan, & Oremus, 2014; Bell, Bowie, &
Thorpe, 2012; Gillum & Ingram, 2006). Conversely, Buck, Williams, Musick, and Sternthal
(2009) found that attendance and public participation were not significantly related to
hypertensive status in a sample of adults from Chicago. Regarding the role of prayer, Buck et al.

also found that regular prayer was associated with a higher likelihood of hypertension. Similarly
Fitchett and Powell (2009) found in a study of middle-aged Protestant and Catholic American
women that daily spiritual experiences were not protective against hypertension.
Most research exploring hypertensive status relies on data from Christian and Catholic
respondents and does not explore between-religion variations in blood pressure. However,
research from rural India suggests that religious affiliation may differentially affect hypertensive
status; individuals belonging to minority religions have higher risks of hypertension compared to
Hindu individuals (Banerjee, Mukherjee, & Basu, 2016). In a country such as Indonesia, where
about 87 percent of the population practices Islam, understanding both the role that Islamic
practices play, as well as how Islam – as a majority religion – measures up to Christianity and
Hinduism, is an important next step in understanding the mechanisms through which religion
may affect hypertensive status.
Religions and Coexistence in Indonesia
In Indonesia, all citizens are declared religious through the Indonesian Constitution
(Gudorf, 2012). However, only six religions are legally recognized: Islam, Buddhism, Hinduism,
Catholicism, Protestantism, and Confucianism (An-Na-Im, 2008). Indonesia largely manages
religions through state administration of religious practices such as mandates to marry within an
individual’s religion, regulations on constructing houses of worship and performing mission
work, and requirements to claim a religion in order to acquire legal documents, obtain state-
administered identification, and travel outside of the country (Seo, 2012). Some argue that these
policies are discriminatory measures against minority religions in the country, particularly
Christianity (Jones, 2005) – due in part to hostility stemming from attempted evangelizing and
conversion (Hoon, 2013). Furthermore, Christianity is a product of Dutch colonialism, and the

legacy of Dutch origins has left Christians better-educated on average than Muslims and with
disproportionate control of the Indonesian economy (Jones, 2005), despite only comprising about
10 percent of the population (Hoon, 2016).
On the other hand, Hinduism and Islam coexist in several domains in Indonesia including
art, festivals, and religious gatherings and do not exhibit the same tensions as Christianity
(Suprato, 2016). In adhering to the legal recognition of monotheistic religions, many modern
Indonesian Hindus have adapted their practices to reflect a single Almighty God surrounded by
ancient gods who have been demoted to angels (McDaniel, 2010). Furthermore, the rich,
longstanding history of Hinduism in Indonesia dates back to the sixth century and has heavily
influenced Indonesian culture (Pringle, 2010).
As a result of the complex and hostile relationship between Christianity and Islam, as
well as the unique and coexistent relationship between Hinduism and Islam, and contrary to past
research demonstrating that minority religions experience higher rates of hypertension, I
hypothesize that:
1A. Christians will experience lower risks of hypertension than Muslim respondents.
1B. Hindu women will not experience significantly different risks of hypertension
compared to Muslim women.
Muslim Traditions in Indonesia
Indonesian Muslims primarily belong to one of two organizations: the Nahdlatul Ulama
(NU) and Muhammadiyah. NU is the largest traditionalist organization with 40 million members,
and Muhammadiyah is the leading modernist organization with 29 million members. Both
organizations are national and provide thousands of universities, schools, and medical facilities
(Pringle, 2010). Muhammadiyah is more stringently organized and is influenced heavily by

puritanical Middle Eastern trends (Pringle, 2010). Conversely, while NU is more accommodating
of local cultural norms within its definition of Islam (Pringle, 2010).
Given that members of NU experience may fewer internal conflicts between their
adherence to Islam and their cultural Indonesian traditions, I hypothesize that:
2. Women from the Nahdlatul Ulama tradition will experience lower risks of
hypertension than Muhammidiyah women, Muslim women without a tradition,
Christian women, and Hindu women.
Salat Prayer and Islam
Among the many religious practices performed by Muslims in Indonesia, one of the most
important is salat – the call to pray five times per day (Henkel, 2005). Salat includes recitations
and fixed sequences of physical movements (standing, prostrating, kneeling, sitting) in the
direction of Mecca. Most Muslims agree that regardless of one’s one level of conformity to
Islam, salat participation is required (Bowen, 1989). Past research has demonstrated that salat
movements can improve physical fitness (Ibrahim, Sian, Shanggar, & Razack, 2013; Reza,
Urakami, & Mano, 2001; Alabdulwahab, Kachanathu, & Oluseye, 2013), psychological well-
being due to its meditative nature (Doufesh et al., 2012), cognitive functioning (Bai, Ye, Zhu,
Zhao, & Zhang, 2012), and cardiac blood flow (Doufesh et al., 2013). Prayer enhances cardiac
autonomic control and increases bararoflex sensitivity (Bernardi, Sleight, Bandinelli, & Cencetti,
2001; Berntson, Norman, Hawkley, & Cacioppo, 2008). However, on the other hand, prayer
participation has been hypothesized to reflect mobilization of spiritual resources as a reaction to
poor health (Salmoirago-Blotcher et al., 2013). Given the meditative and physical nature of salat
prayer as well as its daily importance to Islam itself, I hypothesize that:

3. Muslim women who adhere to salat (by praying at least five times per day) will
have lower risks of hypertension than Muslim women who pray 0 times or 1-4
times per day and Christian women and Hindu women.
Setting
Indonesia is an archipelago nation located in Southeast Asia and is comprised of more
than 17,500 islands, 300 different ethnicities, and 580 different languages and dialects. Indonesia
is the fourth most populated country in the world following China, India, and the United States
with a population of approximately 255 million, although approximately 130 million of its
inhabitants reside on the Javanese cluster of islands (Indonesian Embassy, 2016). Despite ethnic
heterogeneity, 87 percent of Indonesia’s population identifies as Muslim.
Indonesia has long played an important role in global trade with a rich history dating
back to the 1500s when it was colonized by the Portuguese for its spices. Although the
Portuguese were largely unsuccessful, the Dutch established the Dutch East India Company in
1602 and maintained rule in Indonesia until the 1940s. Both the Dutch and Portuguese presence
heavily influenced the evangelization of Christianity across the nation, and the urge for Christian
movements to evangelize persists today. Following a brief interlude in which the Japanese ruled
during World War II, Indonesia formally established independence in 1949.
Since achieving independence, Indonesia has been ruled by two dictators, Sukarno
followed by Suharto. Suharto came to power after Sukarno in 1968 following an army-led anti-
communist purge in 1965 in which over 500,000 people were killed. However, Indonesia was
among the hardest hit by the Asian Financial Crisis in the late 1990s, and amidst the crisis
protests led to Suharto’s resignation in 1998. Following Suharto’s reign Indonesia has
increasingly democratized and has continued to operate under secular governance. For this

reason, Indonesia is seen as progressive with women’s rights relative to most Muslim-majority
countries (Pringle, 2010).
In recent years, Indonesia has been a site for six terrorist attacks by militant Islamic
organizations between 2002 and 2016. Indonesia was also devastated by an earthquake and
tsunami in 2004 that killed approximately 230 thousand people. A series of forest and plantation
fires due to slash and burn techniques has also led to dense hazes that have killed dozens of
people due to low visibility and respiratory illnesses.
Data
The data come from Wave 5 of the Indonesian Family Life Survey (IFLS5), a
longitudinal survey collected in 13 of Indonesia’s 27 provinces (Strauss, Witoelar, & Sikoki,
2016). The IFLS has been collected since 1993 and represents 83 percent of Indonesia’s
population with a sample size of more than 30,000. Individual surveys as well as data from
community leaders and social service centers such as schools, health clinics, and hospitals are
included.
The data for my analyses come from both the household- and community-level data.
Initially starting with a sample of 30,872, limiting the sample to women reduced the total to
16,706. I excluded women who moved outside of the surveyed communities, which further
restricted the sample size to 10,882. Some women had missing health data, and restricting these
women led to a sample size of 10,818 women. Finally, I restricted the sample to women who are
the household head or the household head’s spouse. After doing this, I excluded two households
for having two women who reported being spouses of the household head, presumably in
polygynous unions. Restricting the sample to household heads and household head spouses led to
a final sample size of 7,355 women nested within 310 communities.

Dependent Variable. In the IFLS5, regular interviewers were trained in collecting physical
measurements. Blood pressure was taken as the first anthropometric measure and was taken three
times on alternating arms. An Omron meter, HEM-7203, was used. (Strauss, Witoelar, & Sikoki,
2016). The Omron meter is fully automatic and operates on the oscillometric principle (Omron,
2016). That is, blood flowing through an artery between systolic and diastolic pressures produces
vibrations in the arterial wall that are translated to electric signals and provided as a digital
readout (Berger, 2001). Normal-sized cuffs were used in most circumstances, although large
cuffs were available if needed (Strauss, Witoelar, & Sikoki, 2016).
Importantly, past research has demonstrated the value of home blood pressure
measurements as opposed to measurements taken in a doctor’s office, as in-office measurements
are often higher than those taken at home (Bliziotis, Destounis, & Stergiou, 2012). At-home
measurements allow for more accurate readings due to the absence of the “white coat effect” –
having higher blood pressure during a doctor’s visit (Fuchs, de Mello, & Fuchs, 2013).
Furthermore, home blood pressure monitoring better predicts organ damage (Chobanian et al.,
2003) and hypertension (Pickering et al., 2008; Ward, Takahasi, Stevens, & Heneghan, 2012).
To account for differences in at-home blood pressure readings compared to a doctor’s office,
hypertension thresholds are adjusted accordingly and explained below.
Hypertension – Using the mean systolic and diastolic measurements for blood pressure, I
constructed a dichotomous measure of hypertension. In accordance with the Joint National
Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (2003),
individuals with a mean home-measured BP of more than 135/85 mm Hg are classified as
hypertensive. As supported by (Parati et al., 2008), this threshold is also the accepted indicator

for hypertension in older individuals and pregnant women. Women who do not fall above this
threshold but report taking hypertension medication are also classified as hypertensive.
Systolic Blood Pressure (SBP) – Systolic blood pressure refers to the amount of pressure
in the arteries during heart muscle contraction. I calculated SBP as a mean of three systolic
measurements taken. For those respondents missing measurements, the available measurements
were used to construct a systolic blood pressure value. For example, for women with two
readings, the mean of the two readings was used to create their SBP value.
Diastolic Blood Pressure (DBP) – Diastolic blood pressure refers to the amount of
pressure in the arteries when the heart is in-between beats. DBP was calculated as the mean of
three diastolic measurements. As with SBP, those women with fewer than three readings had
DBPs calculated using the available number of measurements.
Independent Variables. Religious affiliation was self-reported. Women reported affiliations
with Islam, Catholicism, Christianity, Hinduism, and Buddhism. Due to the low number of
Buddhist women in the sample (n=5), I exclude Buddhist respondents from analyses. Catholic
and Christian women are combined to form a “Christian” comparison group. To address
hypothesis 1, I disaggregate Muslim, Christian, and Hindu women with Muslim being the
reference. In order to address hypothesis 2, I disaggregate Muslim women by which Islamic
tradition they feel closest to. The tradition Nahdlatul Ulama (traditionalist) serves as the
reference category, and comparison groups are Muhamadiyah (modernist), not close to any
tradition, Christian, and Hindu. Finally, I disaggregate Muslim women by prayer frequency – 0
prayers per day, 1-4 prayers per day, 5 prayers per day, and 6 or more prayers per day – and
compare those groups to Christian and Hindu women in order to explore hypothesis 3.

Following initial findings, I also include additional variables to disaggregate Hindu
women by whether or not they eat beef as well as whether or not they participate in daily yoga or
meditation. I separate Hindu women into these categories because red meat consumption is
associated with higher risks of hypertension (Pan et al., 2012), while regular meditation and/or
yoga are associated with lower risks of hypertension (Wachholtz & Pargament, 2005). Using the
same reference groups and categories for Muslim and Christian women detailed above, I replace
the single aggregated Hindu group with Hindu women with and without dietary restrictions as
the independent variable for each model, followed by an independent variable with Hindu
women disaggregated by those who do and not participate in daily yoga or meditation.
Community-Level Controls. First, I separate each community into the major grouping of
islands it belongs to. The reference category is Sumatra, and the comparison groups are Java and
“other major islands.” This categorization of island groupings reflects the documentation
provided by the IFLS. Second, I include a dichotomous measure of urban/rural with urban
serving as the reference group. Proportion of community households with electricity is centered
at 35 percent – the minimum percent electricity in the sample. In order to control for health
center accessibility, I include a continuous variable for the number of health posts in the
community ranging from 1 to 38. Finally, I include a categorical variable for the level of
education of the community leader. The reference group is “junior high or less,” and comparison
groups are “high school” and “university/post-secondary.”
In order to accurately partition the variance accounted for as between-person variance
(individual-level) and between-community variance (community-level) to test for contextual-
level effects (Hox, Moerbeek, & van de Schoot, 2010), I also include community-level variables
corresponding with all individual-level characteristics. For continuous variables, I use the

community mean of the variable (e.g. the community’s mean number of household assets for a
given community). For categorical variables, I include a measure for the proportion of the
community reporting each response.
Individual-Level Controls. I included a continuous asset scale with scores ranging from 0-29.
The scale is weighted with more expensive items such as home ownership being worth more.
Possible assets are: house lived in, other house/building, land outside of farm land, livestock or
fish pond, poultry, hard crop trees (perennials), vehicle, household appliances such as a radio or
TV, savings/certificates of deposit/stocks, receivables, jewelry, household furniture and utensils,
and other assets.
Additionally, I include a continuous variable for age centered at the minimum age in the
sample of 15. Ages range from 15 to 101. Marital status is dichotomously coded with married
being the reference and single/divorced/separated/widowed being the comparison group. I also
include a binary measure of highest level of education attained. The reference group is
elementary school or less compared to junior high or more. Employment status is coded as
unemployed (reference) versus employed. A continuous measure for the number of community
programs the respondent has been involved with in the last 12 months ranges from 0 to 14. I also
dichotomously code for whether or not there are children under 15 years old residing in the
household with those women who answered “yes” being the reference group.
Self-reported childhood health status is a continuous Likert-type item ranging from
excellent (0) to poor (4). As many of the women in the sample are of childbearing age, I include
a dichotomous measure to account for whether a woman is pregnant and/or breastfeeding with
the reference being “neither pregnant nor breastfeeding.” As anemia, diabetes, and high
cholesterol are strong indicators of hypertension, I include a binary variable for those taking

medication for anemia, diabetes, and/or high cholesterol, with “no medication” being the
reference group. Smoking status is a dichotomous measure for whether the respondent has a
history of smoking (including those who quit and those who still smoke).
In order to account for healthcare quality, I include a categorical measure of healthcare
satisfaction. The reference category is women who reported less-than-adequate healthcare, and
the comparison groups are “adequate healthcare” and “more-than-adequate healthcare.” Women
were also asked about their food security; women with less-then-adequate food serve as the
reference, and comparison groups are women with “adequate food intake” and “more-than-
adequate food intake.” I also control for whether a woman was fasting at the time of the survey
with those who answered “no” being the reference group.
As regular physical activity has been shown to be a major predictor of hypertension, I
construct a binary variable for whether or not the respondent meets guidelines for adequate
physical activity, defined as participating in at least 25 minutes of vigorous activity 3 days a
week or 30 or more minutes of moderate activity 5 days a week (AHA, 2016). Women who fell
into one or both of these categories when reflecting on their weekly activity are categorized as
“physically active” (reference), while those who did not are categorized as “physically inactive.”
Finally, I construct a binary BMI variable calculated as: weight(in kg)/(height(in m)2). Per CDC
guidelines, those whose body mass index falls above the cut-off point of 25.0 are classified as
overweight or obese, with “not overweight” as the reference category. Because less than 5
percent of the sample are categorized “underweight,” they are included as “not overweight or
obese.”

Data Analysis
I estimate the relationship between the independent variables and their relationship with
hypertensive status, defined as having a home-based blood pressure greater than 135/85mm Hg,
using multilevel logistic regression models in Stata Statistical Software 14 (StataCorp, 2015).
Respondents are nested within communities, and all independent variables and controls are
included as fixed effects. Initially, I use three models to test hypotheses 1-3. However,
unanticipated findings regarding risks of hypertension in Hindu women resulted in 2 additional
models that disaggregate Hindu women by beef consumption and yoga/meditation practices.
In constructing the models, likelihood ratio tests for significant improvement in model fit
upon the inclusion of each independent variable are used. Variables that do not provide
significant improvement in model fit are trimmed and variables that significantly improve model
fit are retained. I perform pairwise comparisons to examine mean differences across comparison
groups for the independent variable in each model. Models are estimated using maximum
likelihood (ML) with unstructured covariances. Covariances are unstructured in order to allow
for unique variances and covariances without constraints. Because each variance and covariance
is estimated uniquely from the data, this structure results in the best possible model fit despite the
loss of degrees of freedom.
It is important to mention limitations. First, there is a possible issue of reverse causality
regarding religion and hypertensive status. However, most hypertensive individuals do not
experience symptoms (WHO, 2016). Furthermore, there is no reason to suspect that hypertensive
status would result in women differentially self-selecting into certain religions or Islamic
traditions. Even for Muslim women who may experience symptoms due to hypertension,
symptoms should not affect the number of daily prayers women report, as Muslim individuals

are expected to adapt prayer customs to physical abilities. Second, blood pressure measurements
are a mean of three measurements taken on a single day. A more accurate accounting of BP
would happen over a larger period of time. However, again there is no reason to believe that
more accurate BP readings would affect one religion or tradition over another.
Results
Descriptive statistics for the independent variables and individual-level controls by
hypertensive status are provided in Table 1. For continuous controls, I provide the percent
hypertensive for the mean response. Twenty seven percent of Muslim respondents, 27 percent of
Christian respondents, and 18 percent of Hindu respondents are categorized as hypertensive.
Within Muslim respondents, 26 percent of NU Muslim women, 26 percent of Muhammadiyah,
and 28 percent of Muslim women who do not identify with a tradition are hypertensive.
Nineteen percent of those who do not pray daily, 19 percent of those who pray 1-4 times per day,
27 percent of women who pray 5 times per day, and 32 percent of women who prayer six or
more times per day are categorized as hypertensive.
------------------------------------------------TABLE 1 ABOUT HERE ----------------------------------
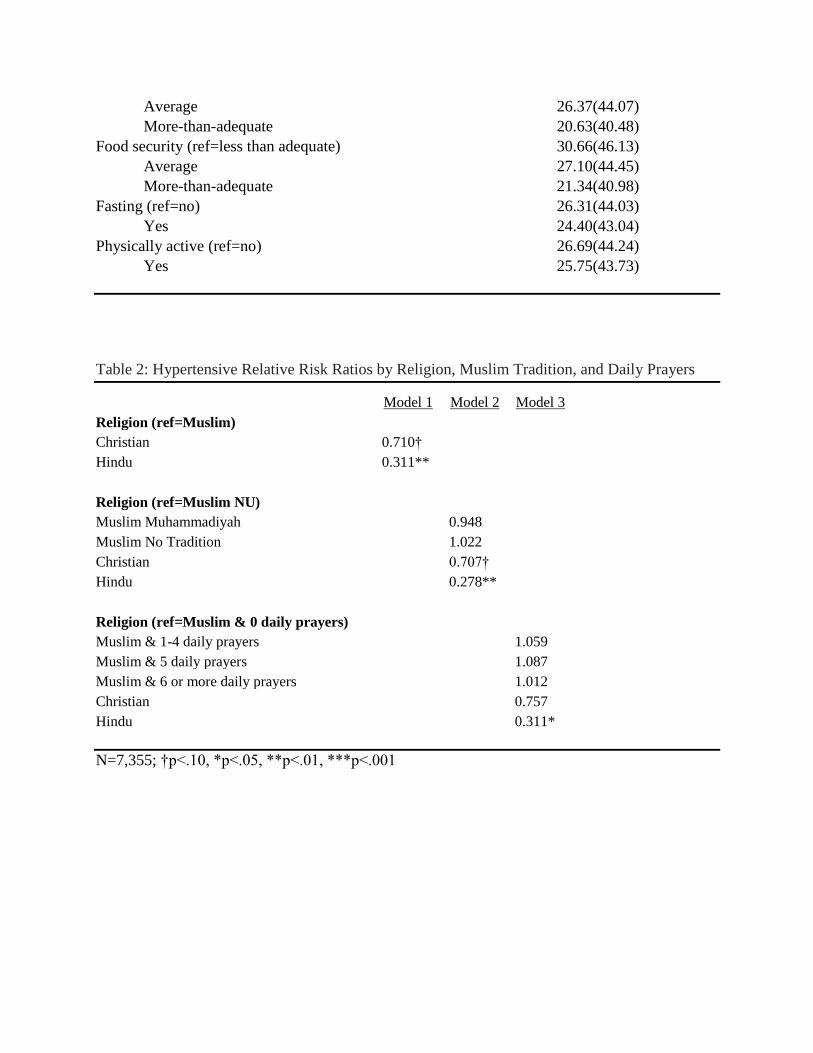
Table 2 provides multivariable results. These results are reported as relative risk ratios,
calculated by converting odds ratios as: RR=OR/[(1-P0)+(P0 x OR)] with P0 representing the
incidence for unexposed risk group (Zhang & Kai, 1998). In Model 1, I test hypotheses 1A and
1B by comparing relative risks of hypertension for Muslim, Christian, and Hindu women.
Inclusion of religion as fixed effects significantly improves model fit via a likelihood ratio test
relative to a model including all other fixed effects (χ2(2)=9.79, p=.008). Christian women have
marginally significantly lower risks of hypertension at 0.71 times the rate of Muslim women,
therefore lending some support to hypothesis 1A. Hindu women have significantly lower rates of

hypertension at less than one third the rate of Muslim women. As such, Model 1 does not
provide support for hypothesis 1B; that is, Hindu women and Muslim women do not experience
comparable risks of hypertension. Hindu women experience significantly lower rates of
hypertension than Muslim women. There are no statistically significant differences between
Christian and Hindu women.
-------------------------------------------TABLE 2 ABOUT HERE -----------------------------------------
In estimating Model 2, the disaggregation of Muslim women by tradition results in
significant improvement in model fit relative to a model including all other fixed effects
(χ2(4)=10.68, p=.03). However, relative to Model 1, there is no significant improvement in
model fit (χ2(2)=0.76, p=.684). Model 2 does not offer support to hypothesis 2 – there are no
significant differences in hypertension rates among Muslim women from different traditions.
Although Muhammidiyah women experience lower rates of hypertension than NU women, the
difference is nonsignificant. Compared to the other major religions, Christian women have
marginally significantly lower risks of hypertension when compared to NU Muslim women
(RR=0.71, p=.065), and Christian women have significantly lower risks compared to Muslim
women who do not adhere to a tradition (RR=0.60, p=.053) (not shown). Hindu women
experience significantly lower risks of hypertension compared to all Muslim women regardless
of tradition, although the largest difference in risk is between Hindu women and Muslim women
who do not adhere to a tradition at slightly above one quarter the rate (RR=0.269, p=.006).
Model 3 provides hypertension risks for Muslim women with differences in number of
reported daily prayers. Relative to Model 1, Model 3 does not provide significant improvement
in Model fit (χ2(3)=1.84, p=.606). Model 3 provides no evidence in support of hypothesis 3;
there are no significant differences in hypertension rates for Muslim women who pray different
amounts each day. However, pairwise comparisons show that Hindu women experienced
statistically significantly lower rates of hypertension when compared to Muslim women from
every category of prayer (p<.01). Additionally, Christian women experienced significantly lower
rates of prayer when compared to Muslim women who prayed 5 times per day (RR=.595,
p=.046).
Given the unanticipated findings in each of the models showing that Hindu women have
lower relative risks of hypertension than Muslim women of every tradition as well as Muslim
women of every category of prayer, I include additional models disaggregating Hindu women by
beef consumption followed by disaggregating Hindu women by daily yoga and meditation
(Table 3) and compare these models to Model 1 via likelihood ratio tests. Model 4 does not
significantly improve model fit relative to the religion model (χ2(1)=1.05, p=.306). In Model 4, I
disaggregate Hindu women by women who do and do not consume beef. Hindu women who eat
beef experience hypertension at one third the rate of Muslim women (p=.02), and Hindu women
who do not eat beef experience hypertension at approximately one fifth the rate of Muslim
women (p=.005). There are no significant differences in hypertension rates between Hindu
women who do and do not eat beef.
------------------------------------------TABLE 3 ABOUT HERE ------------------------------------------
In Model 5, I disaggregate Hindu women by women who do yoga/meditate infrequently
and those who do yoga/meditate every day. Model 5 provides significant improvement in model
fit relative to the aggregated religion model (Model 1) and therefore is the model of best fit
(χ2(1)=3.92, p=.048). Hindu women regardless of yoga/meditation experience statistically
significantly lower rates of hypertension than Muslim women. Those who do yoga/meditate
infrequently experience risks at 0.38 times the rate of Muslim women (p=.045), while those who

do yoga/meditate daily experience hypertension risks at one fifth the rate of Muslim women
(p=0.002). There was also a significant difference in rates of hypertension when comparing
Hindu women who do daily yoga/meditation versus those who do not; women who do
yoga/meditate experience risks of hypertension at 40 percent the rate of Hindu women who
infrequently do yoga/meditate.
Discussion
Although past findings from India suggest that minority religions experience lower rates
of hypertension than majority religions (Banerjee, Mukherjee, & Basu, 2016), my findings from
Indonesia show that Hindu women as well as Christian women fare better than Muslim women
with regard to hypertensive risks after controlling for key individual-level, community-level, and
contextual-level effects. The findings provide some support for hypothesis 1A – that is, Christian
women experience marginally significantly lower rates of hypertension than Muslim women in
four of the five models. This could be attributed in part to connections to the Western world that
provide benefits to Christians that Muslim women may not have access to (Jones, 2005).
Furthermore, there are not significant differences between Muslim women of different
traditions. Although I hypothesized that women who belong to the Nahdlatul Ulama tradition
would experience lower rates of hypertension than women who do not adhere to a tradition or
Muhammadiyah women, tradition does not result in significant differences in hypertension rates.
This finding could provide evidence for cohesion between the traditions; Muslim women in
Indonesia regardless of tradition adhere to the same core beliefs and participation in the salat as a
profession of faith (Pringle, 2010).
Additionally, despite past findings showing that women who participate in salat
experience better cognitive functioning attributed largely to the physical and meditative nature of

Islamic prayer (Doufesh et al., 2013), I estimate no significant differences in hypertensive rates
for Muslim women with varying degrees of daily prayer. Although salat prayer involves a series
of physical movements, the survey question used to gauge prayer participation for Muslim
women does not specify whether women are engaging with the physical aspects of prayer. Given
that Muslims are expected to adapt daily prayer to their physical limitations, salat prayer may not
provide meaningful physical activity for women who already have limitations. Furthermore,
women engaging in more prayer may be mobilizing spiritual resources as a reaction to poor
health (Salmoirago-Blotcher et al., 2013), and I cannot explore differences in possible reasons
women pray at higher rates due to limitations to the data.
Surprisingly, Hindu women have significantly lower risks of hypertension than Muslim
women in all five models presented, contrary to my hypothesis that Hindu and Muslim women
would have comparable hypertension risks (hypothesis 1B). Even after disaggregating Hindu
women by those who eat beef and those who do not, both Hindu groups experience lower
hypertension risks than Muslim women, although Hindu women with restricted diets experience
the lowest rates of hypertension relative to Muslim women. The nonsignificant difference in
women who eat and do not eat beef could reflect recent findings that unprocessed red meat is not
a significant predictor of hypertension (Lajous, 2015), although the survey questionnaire makes
no distinction between the type of meat consumed.
Disaggregating Hindu women by yoga and meditation practices may provide the most
insight into mechanisms through which religion may influence hypertensive risks; Hindu women
who meditate or practice yoga daily experience lower risks of hypertension than all other
religious groups including Hindu women who meditate or practice yoga infrequently.
Participation in daily yoga and meditation through Hinduism, which provides physical health
benefits, reflects past literature examining the role religion plays on encouraging healthy
behaviors and exercise (Koenig, 2012). Given past findings demonstrating the value of yoga for
cardiac health (Satin, Linden, & Millman, 2014; Rosenberg, 2015) as well as findings showing
that meditative practices infused with spirituality provide additional health benefits when
compared to secular meditation (Wachholtz & Pargament, 2005), intentional yoga and
meditation infused with Hindu beliefs may provide additional cardiac health benefits. Future
research may compare women who practice yoga for religious purposes versus women who
practice yoga secularly to examine possible differences in health benefits.
Next Steps
This study provides unique insight into the between-religion differences in hypertensive
rates in Muslim-majority setting. As I prepare the paper for presentation at PAA, I will take
advantage of the longitudinal nature of the data to explore possible differences in beef
consumption and yoga/meditation practices for Hindu women across the earlier waves to see if
changes in food consumption and physical activity behaviors over time reflect changes in
hypertensive risks. I will also expand my analyses to include models examining differences in
severity of isolated systolic hypertension (ISH) in Wave 5 as well as examining the relationship
between religions and hypertensive status in earlier waves of the IFLS as a predictor of mortality
in Wave 5.

References
Abdul-Razak, S., Daher, A. M., Ramli, A. S., Ariffin, F., Mazapuspavina, M. Y., Ambigga, K. S., ... &
Ng, K. K. (2016). Prevalence, awareness, treatment, control and socio demographic determinants
of hypertension in Malaysian adults. BMC public health, 16(1), 1.
Abdullahi Ahmed An-Na'im,. (2008). Islam and the Secular State.
AlAbdulwahab, S. S., Kachanathu, S. J., & Oluseye, K. (2013). Physical activity associated with prayer
regimes improves standing dynamic balance of healthy people. Journal of physical therapy
science, 25(12), 1565.
Bai, R., Ye, P., Zhu, C., Zhao, W., & Zhang, J. (2012). Effect of salat prayer and exercise on cognitive
functioning of Hui Muslims aged sixty and over.Social Behavior and Personality: an
international journal, 40(10), 1739-1747.
Banerjee, A. T., Boyle, M. H., Anand, S. S., Strachan, P. H., & Oremus, M. (2014). The relationship
between religious service attendance and coronary heart disease and related risk factors in
Saskatchewan, Canada.Journal of religion and health, 53(1), 141-156.
Banerjee, S., Mukherjee, T. K., & Basu, S. (2016). Prevalence, awareness, and control of hypertension
in the slums of Kolkata. Indian Heart Journal.
Barraclough, S. (1999). Women and tobacco in Indonesia. Tobacco Control,8(3), 327-332.
Bell, C. N., Bowie, J. V., & Thorpe Jr, R. J. (2012). The interrelationship between hypertension and
blood pressure, attendance at religious services, and race/ethnicity. Journal of religion and
health, 51(2), 310-322.
Bernardi, L., Sleight, P., Bandinelli, G., & Cencetti, S. (2001). Effect of rosary prayer and yoga mantras
on autonomic cardiovascular rhythms: comparative study. British Medical Journal, 323(7327),
1446.

Berntson, G. G., Norman, G. J., Hawkley, L. C., & Cacioppo, J. T. (2008). Spirituality and autonomic
cardiac control. Annals of Behavioral Medicine,35(2), 198-208.
Bliziotis, I. A., Destounis, A., & Stergiou, G. S. (2012). Home versus ambulatory and office blood
pressure in predicting target organ damage in hypertension: a systematic review and meta-
analysis. Journal of hypertension, 30(7), 1289-1299.
Bowen, J. (1989). Salat in Indonesia: The Social Meanings of an Islamic Ritual.Man, 24(4), 600-619.
Bradley, E. (1995). Religious Involvement and Social Resources: Evidence from the Data Set"
Americans' Changing Lives". Journal for the scientific study of Religion, 259-267.
Buck, A. C., Williams, D. R., Musick, M. A., & Sternthal, M. A. (2009). An Examination of Mediators
in the Relationship between Religiosity, Blood Pressure, and Hypertension. Social Science and
Medicine, 68(2).
Chobanian, A. V., Bakris, G. L., Black, H. R., Cushman, W. C., Green, L. A., Izzo Jr, J. L., ... &
Roccella, E. J. (2003). The seventh report of the joint national committee on prevention,
detection, evaluation, and treatment of high blood pressure: the JNC 7 report. Jama, 289(19),
2560-2571.
DHS (2012). Indonesia DHS, 2012 – Final report. http://dhsprogram.com/publications/publication-
fr275-dhs-final-reports.cfm.
Doufesh, H., Faisal, T., Lim, K. S., & Ibrahim, F. (2012). EEG spectral analysis on Muslim
prayers. Applied psychophysiology and biofeedback,37(1), 11-18.Fitchett, G., & Powell, L. H.
(2009). Daily spiritual experiences, systolic blood pressure, and hypertension among midlife
women in SWAN. Annals of Behavioral Medicine, 37(3), 257-267.
Doufesh, H., Ibrahim, F., Ismail, N. A., & Ahmad, W. A. W. (2013). Assessment of heart rates and
blood pressure in different salat positions.Journal of Physical Therapy Science, 25(2), 211-214.

Gillum, R. F., & Ingram, D. D. (2006). Frequency of attendance at religious services, hypertension, and
blood pressure: the Third National Health and Nutrition Examination Survey. Psychosomatic
Medicine, 68(3), 382-385.
Gudorf, C. E. (2012). Religion, Law, and Pentecostalism in Indonesia.Pneuma, 34(1), 57-74.
He, J., & Whelton, P. K. (1999). Elevated systolic blood pressure and risk of cardiovascular and renal
disease: overview of evidence from observational epidemiologic studies and randomized
controlled trials. American heart journal, 138(3), S211-S219.
Henkel, H. (2005). ‘BETWEEN BELIEF AND UNBELIEF LIES THE PERFORMANCE OF SALĀT
’: MEANING AND EFFICACY OF A MUSLIM RITUAL. Journal of the Royal
Anthropological Institute, 11(3), 487-507.
Holt, C. L., Clark, E. M., Wang, M. Q., Williams, B. R., & Schulz, E. (2015). The Religion–Health
Connection Among African Americans: What Is the Role of Social Capital?. Journal of
Community & Applied Social Psychology,25(1), 1-18.
Hoon, C. Y. (2013). Between evangelism and multiculturalism: The dynamics of Protestant Christianity
in Indonesia. Social Compass, 60(4), 457-470.
Hoon, C. Y. (2016). Religious aspirations among urban Christians in contemporary
Indonesia. International Sociology, 0268580916643853.
Hox, J. J., Moerbeek, M., & van de Schoot, R. (2010). Multilevel analysis: Techniques and applications.
Routledge.
Ibrahim, N. K., Hijazi, N. A., & Al-Bar, A. A. (2008). Prevalence and determinants of prehypertension
and hypertension among preparatory and secondary school teachers in Jeddah. J Egypt Public
Health Assoc, 83(14), 183-203.
Ibrahim, F., Sian, T. C., Shanggar, K., & Razack, A. H. (2013). Muslim Prayer Movements as an
Alternative Therapy in the Treatment of Erectile Dysfunction: A Preliminary Study. Journal of
physical therapy science,25(9), 1087.
Joffres, M., Falaschetti, E., Gillespie, C., Robitaille, C., Loustalot, F., Poulter, N., ... & Campbell, N.
(2013). Hypertension prevalence, awareness, treatment and control in national surveys from
England, the USA and Canada, and correlation with stroke and ischaemic heart disease
mortality: a cross-sectional study. BMJ open, 3(8), e003423.
Jones, N. (2005). REDISCOVERING PANCASILA: RELIGION IN INDONESIA'S PUBLIC
SQUARE. The Brandywine Review of Faith & International Affairs, 3(1), 23-30.
Kayima, J., Nankabirwa, J., Sinabulya, I., Nakibuuka, J., Zhu, X., Rahman, M., ... & Kamya, M. R.
(2015). Determinants of hypertension in a young adult Ugandan population in epidemiological
transition—the MEPI-CVD survey. BMC public health, 15(1), 830.
Khanam, M. A., Lindeboom, W., Razzaque, A., Niessen, L., & Milton, A. H. (2015). Prevalence and
determinants of pre-hypertension and hypertension among the adults in rural Bangladesh:
findings from a community-based study. BMC public health, 15(1), 1.
Koenig, H. G. (2012). Religion, spirituality, and health: The research and clinical implications. ISRN
psychiatry, 2012.
Krause, N. (2008). The social foundation of religious meaning in life.Research on Aging, 30(4), 395-
427.
Lajous, M., Bijon, A., Fagherazzi, G., Rossignol, E., Boutron-Ruault, M. C., & Clavel-Chapelon, F.
(2014). Processed and unprocessed red meat consumption and hypertension in women. The
American journal of clinical nutrition, 100(3), 948-952.

McDaniel, J. (2010). Agama Hindu dharma Indonesia as a new religious movement: Hinduism recreated
in the image of Islam. Nova Religio: The Journal of Alternative and Emergent Religions, 14(1),
93-111.
Pan, A., Sun, Q., Bernstein, A. M., Schulze, M. B., Manson, J. E., Stampfer, M. J., ... & Hu, F. B.
(2012). Red meat consumption and mortality: results from 2 prospective cohort studies. Archives
of internal medicine,172(7), 555-563.
Parati, G., Stergiou, G. S., Asmar, R., Bilo, G., de Leeuw, P., Imai, Y., ... & O'Brien, E. (2008).
European Society of Hypertension guidelines for blood pressure monitoring at home: a summary
report of the Second International Consensus Conference on Home Blood Pressure
Monitoring. Journal of hypertension, 26(8), 1505-1526.
Pickering, T. G., Miller, N. H., Ogedegbe, G., Krakoff, L. R., Artinian, N. T., & Goff, D. (2008). Call to
action on use and reimbursement for home blood pressure monitoring A joint scientific statement
from the American Heart Association, American Society of Hypertension, and Preventive
Cardiovascular Nurses Association. Hypertension, 52(1), 10-29. Powell, L. H., Shahabi, L., &
Thoresen, C. E. (2003). Religion and spirituality: Linkages to physical health. American
psychologist, 58(1), 36.
Pringle, R. (2010). Understanding Islam in Indonesia: Politics and diversity. Honolulu: University of
Hawaiʻi Press.
Reza, M. F., Urakami, Y., & Mano, Y. (2001). Evaluation of a new physical exercise taken from salat
(prayer) as a short-duration and frequent physical activity in the rehabilitation of geriatric and
disabled patients. Annals of Saudi medicine, 22(3-4), 177-180.Rosenberg, K. (2015). Yoga may
Improve Cardiac and Metabolic Risk Factors. AJN The American Journal of Nursing, 115(4), 60.

Salmoirago-Blotcher, E., Hunsinger, M., Morgan, L., Fischer, D., & Carmody, J. (2013). Mindfulness-
based stress reduction and change in health-related behaviors. Journal of Evidence-Based
Complementary & Alternative Medicine, 2156587213488600.
Satin, J. R., Linden, W., & Millman, R. D. (2014). Yoga and psychophysiological determinants of
cardiovascular health: comparing yoga practitioners, runners, and sedentary individuals. Annals
of Behavioral Medicine, 47(2), 231-241.
Seo, M. (2012). Defining ‘religious’ in Indonesia: toward neither an Islamic nor a secular
state. Citizenship Studies, 16(8), 1045-1058.
Strauss, J., Witoelar, F., & Sikoki, B. (2016). The fifth wave of the Indonesia Family Life Survey
(IFLS5): Overview and field report.
Suprapto, S. (2016). THE THEOLOGY OF TOLERANCE IN HINDU AND ISLAM: MAINTAINING
SOCIAL INTEGRATION IN LOMBOK-INDONESIA.ULUMUNA, 19(2), 329-352.
Wachholtz, A. B., & Pargament, K. I. (2005). Is spirituality a critical ingredient of meditation?
Comparing the effects of spiritual meditation, secular meditation, and relaxation on spiritual,
psychological, cardiac, and pain outcomes. Journal of behavioral medicine, 28(4), 369-384.
Ward, A. M., Takahashi, O., Stevens, R., & Heneghan, C. (2012). Home measurement of blood pressure
and cardiovascular disease: systematic review and meta-analysis of prospective studies. Journal
of hypertension,30(3), 449-456.
WHO (2013). Global health observatory data.
http://www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence/en/.
WHO (2014). Alcohol consumption: Levels and patterns. Retrieved 22 September 2016 from http://ww
w.who.int/substance_abuse/publications/global_alcohol_report/profiles/idn.pdf.

WHO (2016). A global brief on hypertension: silent killer, global public health crisis. World. Retrieved
from http://tinyurl.com/cywh2eh.

Table 1: Percent Hypertensive for Independent Variables and Individual-Level Controls
% Hypertensive (SD)
Independent Variables
Muslim Tradition
NU 26.33(44.04)
Muhammadiyah 26.08(43.94)
No Tradition 28.31(45.07)
Muslim Prayer
0 Prayers Per Day 18.94(39.27)
1-4 Prayers Per Day 19.13(39.36)
5 Prayers Per Day (salat) 26.88(44.34)
6 or More Prayers Per Day 31.97(46.65)
Christian 27.35(44.64)
Hindu Dietary Restrictions
No Dietary Restrictions 18.98(39.28)
Does Not Eat Beef 14.63(35.56)
Hindu Yoga/Meditation Participation
Daily Yoga/Meditation 12.43(33.09)
Infrequent Yoga/Meditation 23.46(42.50)
Individual-Level Controls
Age (mean age=43) 34.83(47.91)
Community Participation (mean=2) 28.17(44.99)
Education (ref=elementary or less) 33.72(47.28)
Junior High or More 18.12(38.53)
Employment (ref=unemployed) 27.81(44.81)
Employed 25.20(43.42)
Household Assets (mean=11) 24.63(43.12)
Kids Under 15 in Household (ref=yes) 38.53(48.68)
No 16.75(37.34)
Marital status (ref=married) 24.11(42.78)
Single/separated/widowed 39.05(48.81)
BMI (ref=not overweight or obese) 20.34(40.26)
Overweight or obese 33.13(47.07)
Childhood Health (mean=2) 26.99(44.40)
Tobacco use (ref=never tried) 25.92(43.82)
Formerly smoked, currently smokes 34.15(47.51)
Medication Use (ref=no medications) 25.82(43.77)
Takes medication 32.80(47.00)
Pregnant or Breastfeeding (ref=no) 28.60(45.19)
Yes 9.40(29.20)
Healthcare Quality (ref=less-than-adequate) 31.46(46.45)
Average 26.37(44.07)
More-than-adequate 20.63(40.48)
Food security (ref=less than adequate) 30.66(46.13)
Average 27.10(44.45)
More-than-adequate 21.34(40.98)
Fasting (ref=no) 26.31(44.03)
Yes 24.40(43.04)
Physically active (ref=no) 26.69(44.24)
Yes 25.75(43.73)
Table 2: Hypertensive Relative Risk Ratios by Religion, Muslim Tradition, and Daily Prayers
Model 1 Model 2 Model 3
Religion (ref=Muslim)
Christian 0.710†
Hindu 0.311**
Religion (ref=Muslim NU)
Muslim Muhammadiyah
0.948
Muslim No Tradition
1.022
Christian
0.707†
Hindu
0.278**
Religion (ref=Muslim & 0 daily prayers)
Muslim & 1-4 daily prayers
1.059
Muslim & 5 daily prayers
1.087
Muslim & 6 or more daily prayers
1.012
Christian
0.757
Hindu
0.311*
N=7,355; †p<.10, *p<.05, **p<.01, ***p<.001

Table 3: Hypertensive Relative Risk Ratios by Religion, Hindu Diet, and Hindu Yoga/Meditation
Model 4 Model 5
Religion (ref=Muslim)
Christian 0.712†
Hindu & No Dietary Restrictions 0.325*
Hindu & Does Not Eat Beef 0.219**
Religion (ref=Muslim)
Christian
0.709†
Hindu & Meditates/Does Yoga
Infrequently
0.395*
Hindu & Meditates/Does Yoga Daily
0.199**
N=7,355; †p<.10, *p<.05, **p<.01, ***p<.001





























